
Abstract
Purpose:
The aim of this systematic review was to address the Ponseti method in arthrogrypotic clubfoot treatment and evaluate the success, complication, and recurrence rates.
Method:
A systematic review was performed in the PubMed, Scopus, Embase, and Web of Science databases on 9 January 2023, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Success, recurrence, and complication rates were evaluated and analyzed. Risks of bias and the quality of the studies were also evaluated.
Results:
Five case series, including 53 patients (102 feet), were identified. According to this model, the initial success rate was 91% (95% confidence interval = 0.79–0.96) with I2 = 43%, and the final success was 68% (at 5.8 years of follow-up). Recurrence rate was 30% (95% confidence interval = 0.14–0.52).
Conclusion:
Ponseti method is indicated in the initial treatment of arthrogrypotic clubfeet, as it is a minimally invasive method with a high correction rate (91%). However, a high recurrence rate (30%) requires early detection and adequate treatment.
Level of evidence:
Level III
PROSPERO Protocol:
CRD42020210373
Keywords
Introduction
Arthrogryposis multiplex congenita (AMC) is a clinical condition characterized by multiple non-progressive joints, normally detected at birth, and affects two or more joints. The frequency in the population is estimated at 1 case for every 3000 live births of either sex in the United States.1 –4
Foot deformities are very common in all types of arthrogryposis. The most common is severe clubfoot, with an incidence of up to 90%. 5
The purpose of arthrogrypotic feet treatment is the conversion into a plantigrade and painless foot that can be shoeable. Treatment should be started soon after the diagnosis to allow independent ambulation.
Management of foot deformities in arthrogryposis is difficult because some other joint deformities and contractures make it difficult to align the limb and use an orthosis. The main arthrogrypotic clubfoot treatment was surgical, and treatment with casts was contra-indicated. 4 Different surgeries, such as soft tissue and bony procedures, were proposed, including osteotomies, talectomies, and arthrodesis. Bone resection procedures were recommended for the primary foot treatment in arthrogrypotic patients. However, the results were unsatisfactory, with high recurrence rates and few functional results.6,7
The Ponseti method to treat these deformities was based on the high success rates in patients with idiopathic congenital clubfoot.8 –10
Ponseti developed his own treatment method in the 40s motivated by the poor results obtained with the available treatments. He studied the pathological and functional anatomy of clubfeet and established a protocol for manipulation of feet and plaster casting, as well as Achilles tendon tenotomy and recurrence prevention strategies with an abduction nighttime brace, based on the child’s age and parental cooperation. Ponseti method has become the preferred method for the treatment of idiopathic clubfeet in many countries. 10
The aim of this systematic review is to address the Ponseti method in arthrogrypotic clubfoot treatment and evaluate the success, complication, and recurrence rates.
Materials and methods
Search strategy
A systematic review was performed by two researchers (A.C.B. and G.F.F.) according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search was conducted on PubMed, Scopus, Embase, and Web of Science databases.
The search was performed on January 9, 2023, using the keywords “arthrogryposis” and “clubfoot” with a Boolean search AND without any language restriction.
The present systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) CRD42020210373. The researchers obtained the data and independently analyzed each study. Disagreements were resolved by the senior researcher (M.P.N.).
Inclusion and exclusion criteria
The inclusion criteria were (1) clinical diagnosis of arthrogryposis and clubfoot; (2) treatment by Ponseti method; (3) minor surgical procedure associated with Achilles tenotomy or anterior tibial transfer; and (4) no previous surgical treatment.
The exclusion criteria were (1) idiopathic clubfoot; (2) another neuromuscular disease or syndrome; (3) previous surgical treatment; and (4) case reports.
Data extraction
Two researchers extracted the data according to the following criteria: name of the first author, publication year, country, study design, type of study, number of patients, number of feet, age, and follow-up.
Quality assessment
The index for non-randomized studies (MINORS) was used to evaluate the methodological quality of the studies (observational).
Studies with scores ≤11 were classified as low quality, and those with scores ≥12 were classified as high quality.
Risk and publication bias
Each included study was analyzed using the ROBINS-I tool recommended by Cochrane, whose objective is to assist in the pre-intervention bias risks: confusion, selection, and classification; and post-intervention bias: intention-to-treat deviation, data loss, outcome measurement, and reported outcome selection; and the funnel plot was performed to evaluate the publication bias.
Statistical analysis
A meta-analysis of proportions with data normalized using the logit function based on the selected outcomes was performed. Heterogeneity was calculated using the I2. The random effects model was selected for the meta-analysis, and the calculations were performed through the software R.
Publication bias was analyzed using a funnel plot.
Data items
The results were categorized using Endnote, and duplicates were excluded.
Outcomes
The outcomes evaluated were the initial and final success and complication rates. The success rate was evaluated two times: at the final serial casts and Achilles tenotomy and at the last follow-up.
It was considered success a plantigrade foot and able to use orthosis, with no need for additional procedures.
Results
Eligible studies
The search included 1187 articles: PubMed (222), Embase (444), Scopus (414), and Web of Science (107). After the exclusion of duplicates and irrelevant articles, 30 studies were carefully analyzed by the authors. At last, five observational studies that met the established criteria were selected for the meta-analysis. The flowchart representing the study selection is shown in Figure 1.
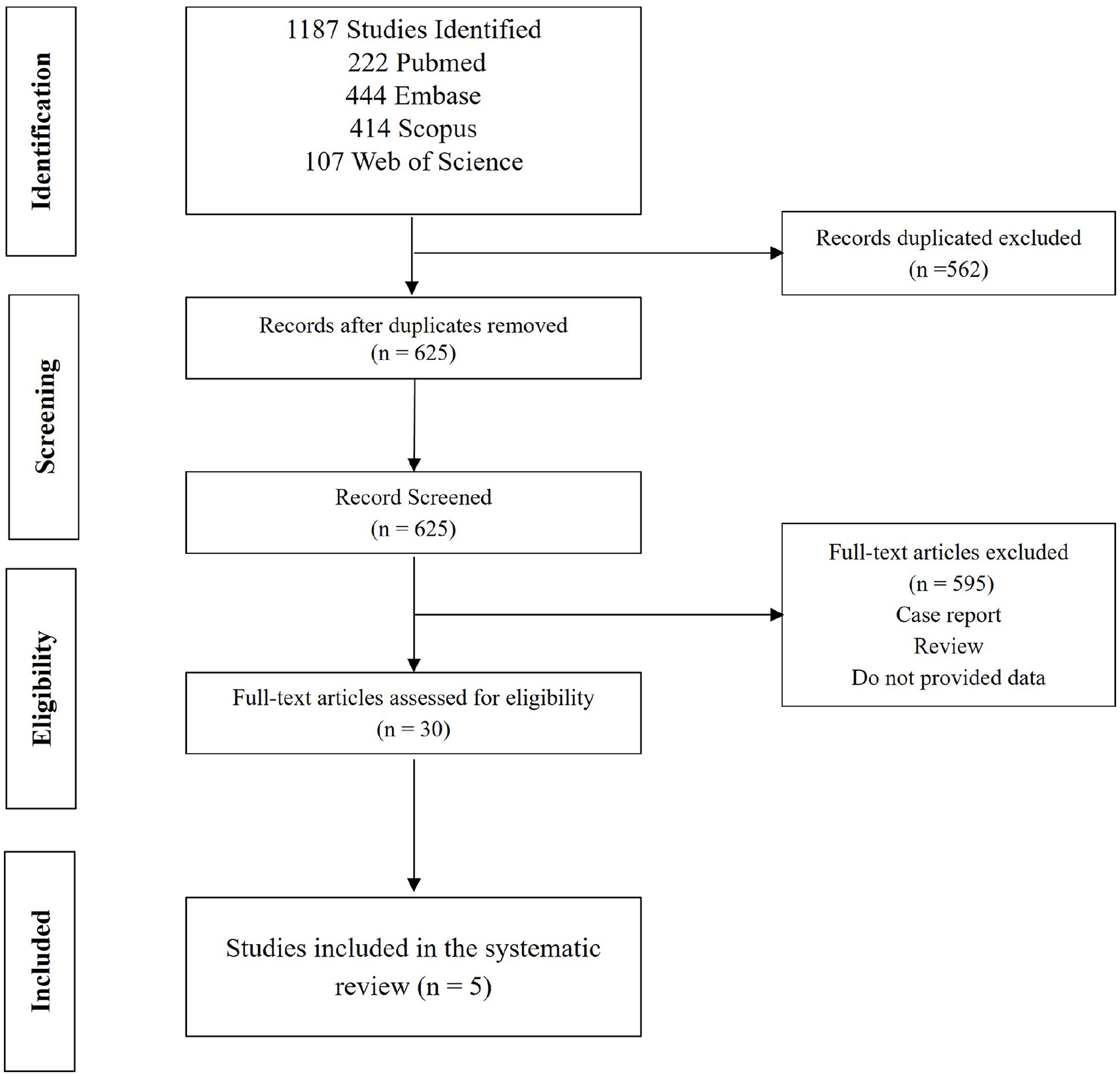
PRISMA flowchart of the literature search and study selection.
Demographic characteristics of the included studies
The studies were published from 2008 to 2016. Among the five identified studies: three were from the United States,11 –13 one from the United Kingdom, 14 and one from Poland. 15 There were 53 patients (102 feet) aged 1 to 280 weeks.
The Ponseti method was applied to all patients. The cases casts were applied by the senior researcher. Moreover, the type of brace used after the casting phase is different.
Age at the beginning of treatment varied across studies, with studies starting treatment at birth and others later. The mean age was 1 year. The follow-up among the studies also varied, with a short follow-up study of 2 years and the longest follow-up time of 5.8 years (Table 1).
Demographic and treatment characteristics of the included studies.
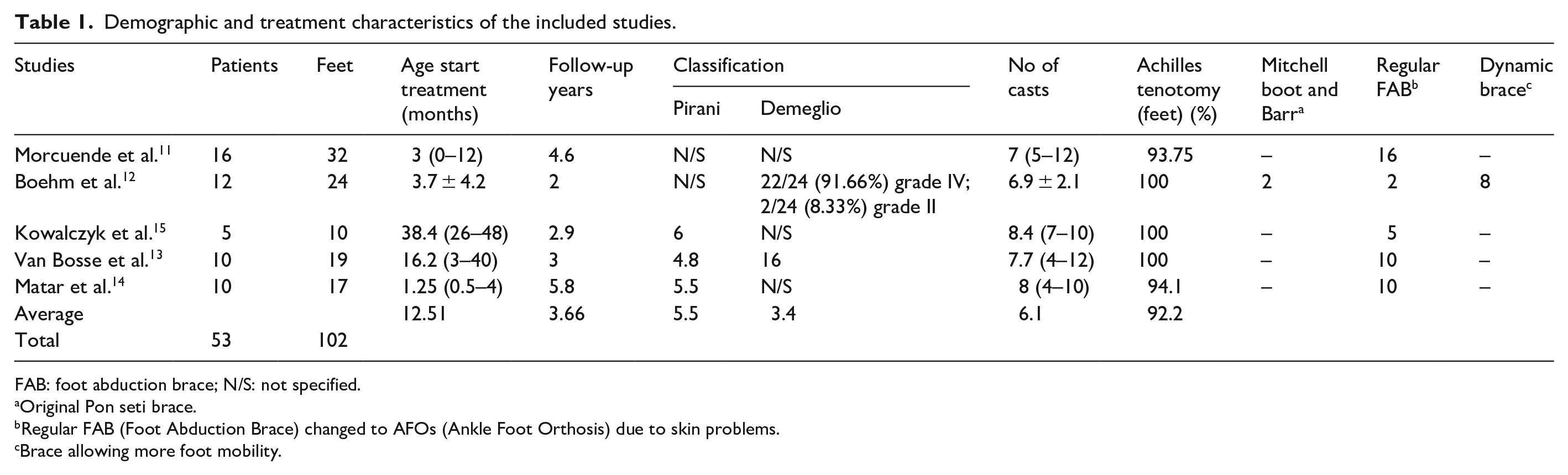
FAB: foot abduction brace; N/S: not specified.
Original Pon seti brace.
Regular FAB (Foot Abduction Brace) changed to AFOs (Ankle Foot Orthosis) due to skin problems.
Brace allowing more foot mobility.
Treatment failure was defined as a non-plantigrade foot and inability to use an orthosis, requiring additional procedures, including extensive posteromedial release. Recurrence was defined as the appearance of any deformity or dorsiflexion lower than 0°.
Cases included in the studies were evaluated based on clinical assessment. Success was defined as a plantigrade foot without residual deformity, with some dorsiflexion, and no need for additional surgical procedures.
The quality of the studies was evaluated using MINORS, 16 and the summarized study quality assessment is shown in Table 2.
Summary of the study quality assessment using the methodological index for non-randomized studies (MINORS). a
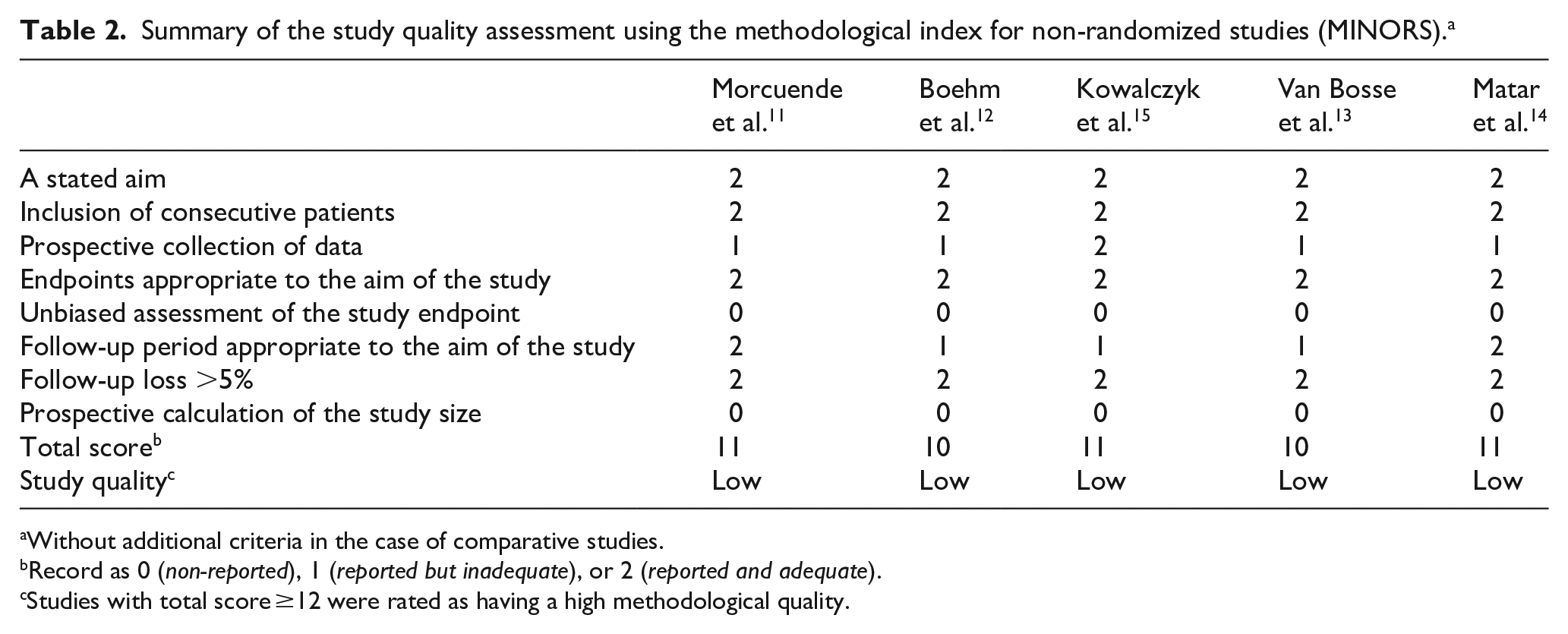
Without additional criteria in the case of comparative studies.
Record as 0 (non-reported), 1 (reported but inadequate), or 2 (reported and adequate).
Studies with total score ≥12 were rated as having a high methodological quality.
Pooled analysis
The success and recurrence rates outcomes show results that made a pooled analysis possible.
Risk of bias and publication bias
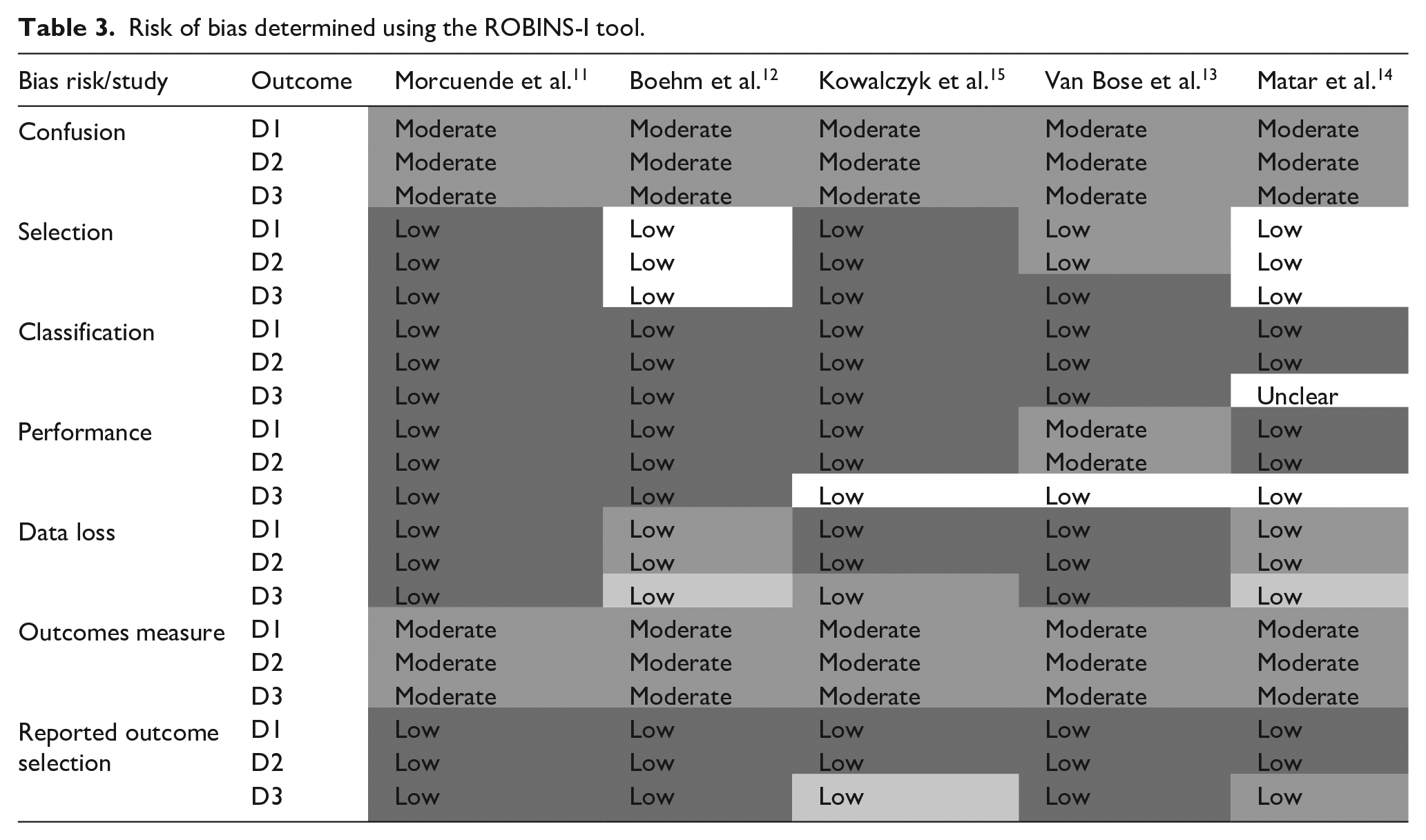
Risks of bias data were analyzed using the ROBINS-I tool and are summarized in Table 3. Those biases that could not be identified due to lack of information in the article are also marked. Summarized data allow us to observe that the greatest risks in these studies involve the pre-intervention phase with confusion bias. These are case series; therefore, no patient who received the intervention was randomized. Post-intervention bias occurs when measuring the results, mainly because there is no blinding.
Risk of bias determined using the ROBINS-I tool.

Publication bias was reduced for a large search in the database without language restriction and additional search in the gray literature; however, it is not possible to eliminate this bias. Figure 2 shows qualitative analysis by funnel plot. All five studies had a heterogeneity distribution.
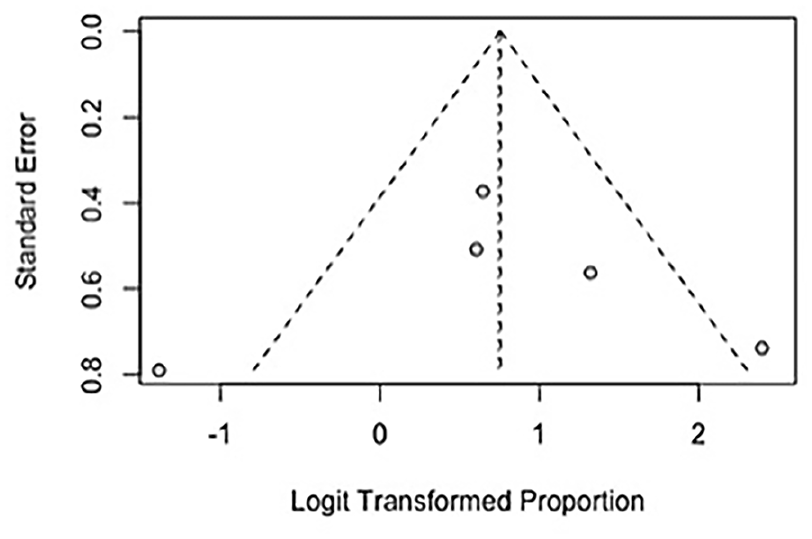
Funnel plot of the publication bias of included studies.
Outcomes
All studies included were accurately read, and the values of the outcomes are shown in Table 4.
Studies outcomes.
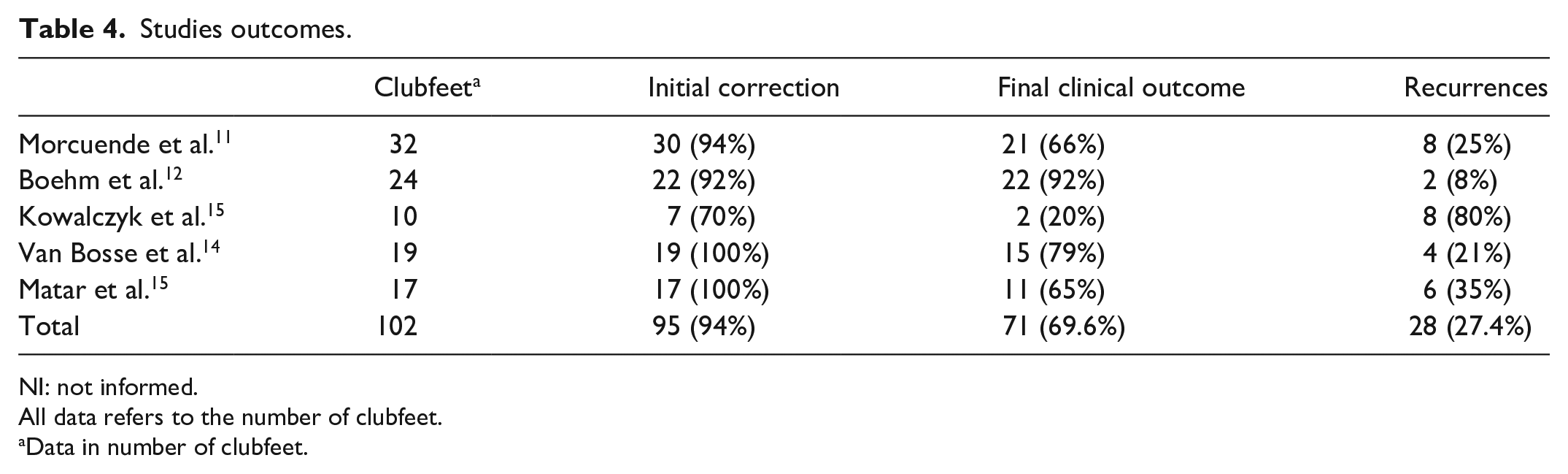
NI: not informed.
All data refers to the number of clubfeet.
Data in number of clubfeet.
Success rate
Success rate was analyzed twice during treatment, after the final cast (initial correction), and at the last follow-up (final clinical outcome). Forest plots summarized the results for initial correction among the five included studies. According to the random effect model, the initial success rate (initial correction) was 91% (95% confidence interval [CI] = 0.79–0.96) with heterogeneity among the results I2 = 37%, and the final success rate (final clinical outcome) was 68% (95% CI = 0.42–0.86) with heterogeneity among the results I2 = 70% (Figures 3 and 4).

Forest plot of the meta-analysis of studies examining initial success (initial correction).
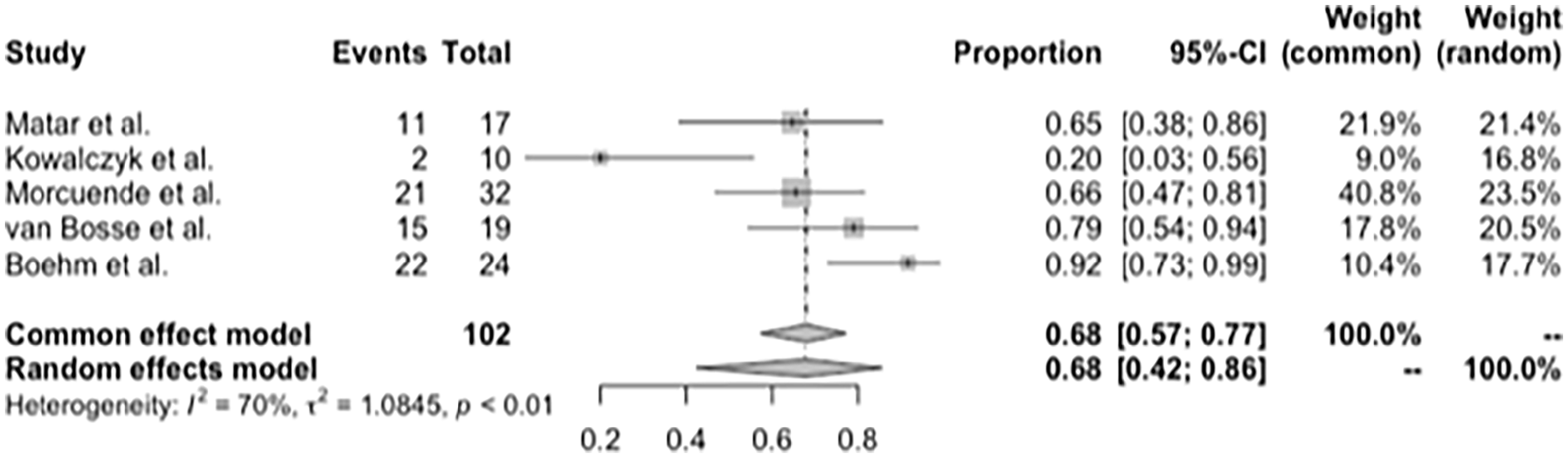
Forest plot of the meta-analysis of studies examining the final success (final clinical outcome).
Recurrence
Five studies evaluated the recurrence rate, which was found 30% (95% CI = 0.14–0.52) (Figure 5).
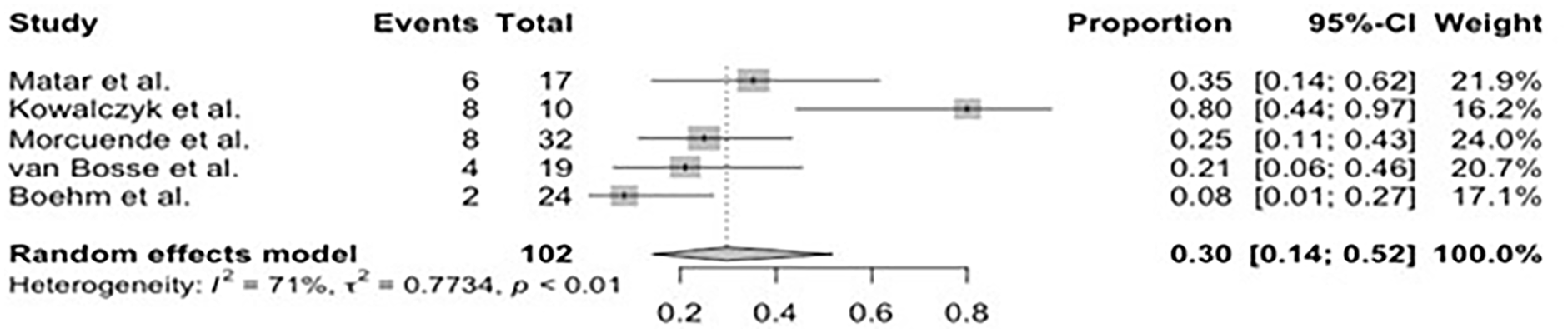
Forest plot of the meta-analysis of studies examining the effect of recurrence.
Discussion
Ponseti method was originally described for idiopathic clubfoot with excellent results and has become an option for children with non-idiopathic clubfoot, with a high initial correction rate and a promised long-term result. 11
The review demonstrated treatment of arthrogrypotic feet using the Ponseti method, a success rate of 91% (initial correction) and 68% at the final follow-up. That decrease is due to the high recurrence rate, dependent on the time of follow-up (long follow-up, more recurrences).
Despite the variations, all studies demonstrated a high success rate in initial correction. However, it is difficult to maintain the initial correction because arthrogrypotic clubfeet are more rigid and present other lower extremity deformities than idiopathic; they are also more difficult to brace. 17 The muscle imbalance is responsible for more recurrences, and retreatment with more casts and foot abduction brace is the way to avoid surgical interventions. To avoid treatment failure, managing these patients starts with an explanation and family assistance. We believe that the recurrence rate and the final success are related to the intrinsic characteristics of these feet due to muscular imbalance, rigid deformity, and impaired proprioception.11 –15
The initial correction was high, and as shown in the idiopathic clubfoot, the maintenance of this correction was difficult. The fact that these feet have more rigidity is known, but it does not reflect in the correction capacity. Recurrence rate reflects the difficulty of maintaining the initial correction. Although there is strong evidence that the classic form recurs more, a comparative study using the Ponseti technique between the different forms would be necessary to confirm this hypothesis. It is also important to consider that posteromedial release is one modality of treatment that Kowalczyk and Lejman 15 had chosen to treat his recurrences. This is still a surgeon’s choice—they could have treated also with a new series of casts and tenotomy.
A foot abduction brace is essential to maintain the correction, sometimes up to pre-teenage years. Children must be followed until maturity, when the bones and muscles/tendons are more stable, not suffering the stretching of the bone spurts. Then, those children will finally be able to maintain the correction, with a functional foot.
This systematic review has limitations. The studies included were series cases (observational studies) with low methodological quality, 80% were retrospective with risk of bias of information and records, and were studies that used data obtained without a proposal for the study. The arthrogryposis type is also not reported in detail as its outcome. In addition, most studies have limited follow-up time, which may have altered the recurrence rate. However, this evidence is important in the lack of higher quality studies to propose to change and improve how children with arthrogrypotic feet are treated.
Conclusion
Ponseti method is indicated in the initial treatment of arthrogrypotic clubfeet, as it is a minimally invasive method with a high correction rate (91%). However, a high recurrence rate (30%) requires early detection and adequate treatment.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231214778 – Supplemental material for Effectiveness of the Ponseti method for congenital clubfoot in patients with arthrogryposis: A systematic review and meta-analysis of observational studies
Supplemental material, sj-pdf-1-cho-10.1177_18632521231214778 for Effectiveness of the Ponseti method for congenital clubfoot in patients with arthrogryposis: A systematic review and meta-analysis of observational studies by Augusto Cesar Bravin, Gabriel Ferraz Ferreira and Monica Paschoal Nogueira in Journal of Children’s Orthopaedics
Footnotes
Author’s note
Augusto Cesar Bravin is also affiliated to Hospital do Servidor Público Estadual de Sao Paulo, Sao Paulo, SP, Brazil.
Author contributions
A.C.B., MD, MSc, contributed to conceptualization, data curation, investigation, methodology, visualization, writing—original draft preparation, and writing—review & editing. G.F.F., MD, MSc, contributed to data curation and investigation. M.P.N., MD, PhD, contributed to conceptualization, formal analysis, methodology, validation, and writing—review & editing.
Declaration of conflicts of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article. Furthermore, the data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.