
Abstract
Background:
The surgical treatment of moderate and severe slipped capital femoral epiphysis is controversial. Treatment ranges from pinning in situ to open dislocation and reduction of the slipped epiphysis. The modified Dunn procedure has been associated with variable avascular necrosis with rates, ranging between 0% and 67%. The aim of this study was to evaluate the outcomes and complications of patients who have undergone a subcapital realignment osteotomy (SCRO) in our center.
Methods:
A retrospective longitudinal study of the osteotomies performed between 2009 and 2019 in a tertiary referral center for Pediatric Orthopedics in Queensland, Australia. Patient demographics, stability, and severity of slip and surgical outcomes were collected.
Results:
A total of 123 procedures were performed on 116 patients. The mean age was 12.4 years, 65 (56%) patients were male and the mean posterior sloping angle was 60.10 with 93 (75%) being severe slips. There were 51 (41.5%) Loder’s stable and 72 (58%) unstable slipped capital femoral epiphysis. Our overall avascular necrosis rate following SCRO was 17.8%. Time between surgery and diagnosis did not have an effect on avascular necrosis.
Conclusion:
The subcapital realignment osteotomy remains a controversial and complex procedure for the management of moderate and severe slipped capital femoral epiphysis. We found that our cohort demonstrated an avascular necrosis rate in keeping with the existing literature. This indicates that when performed in a high-volume center with experienced surgical staff, it can be an effective treatment option for these patients.
Level of evidence:
Level IV
Introduction
Slipped capital femoral epiphysis (SCFE) is a common adolescent hip pathology in Australia and is on the rise in both Obese and Aboriginal patients. 1 Coupled with an establish increased incidence in the Polynesian population, this means that Queensland sees some of the highest rates of SCFE in the world. 2 Despite the increased incidence, surgical management of moderate and severe slips remains controversial.3 –6 The goals of surgery are to achieve stability, maintain function, and to avoid avascular necrosis (AVN) of the femoral head.
The most widely accepted treatment modality of pinning in situ (PIS) is designed to stabilize the SCFE but does not address deformity and can therefore impact range of motion and function. Impingement from the residual cam lesion occurs in even a mild SCFE and has led an increasing number of surgeons to consider correction of the acute SCFE via a corrective osteotomy procedure that addresses the deformity and cam impingement with a variety of techniques described.7,8 The safety of this procedure is still in question, and as a result of this controversy, studies have been conducted to see whether the rate of major complication, in particular AVN, is comparable to that of other treatment modalities.
Closed reduction and PIS can be associated with a high rate of osteonecrosis. Boero et al. 9 associated negative outcome with both degree of slip and the use of a reduction maneuver. However, some units do report reasonable outcomes of AVN and suggest that this remains a reasonable treatment option. 10 It is now accepted that there is a chronic component of the slip associated with remodeling of bone at the posterior aspect of the femoral metaphysis. When the epiphysis is reduced into its anatomical position, the posterior retinacular vessels are occluded when they stretch over the remodeling callus. 11 This will sometimes be absent or smaller in the acute slip and it may be responsible for the discrepancies in outcome reported with the technique of gentle reduction and pinning. PIS alone can reduce this risk of AVN, but it does not address cam type lesion causes femoroacetabular impingement and the development of degenerative osteoarthritis.12 –17
A number of corrective osteotomies have been described which attempt to minimize the long-term sequelae of the proximal femoral deformity; however, results have not always been encouraging. The incidence of osteonecrosis after subcapital wedge osteotomy has been reported from 20% to 30% in a series by Gage et al. 18 in 1978. The rate of chondrolysis was also high at 37%. The Southwick and Imhauser osteotomies have been more encouraging with only two cases of osteonecrosis in a series of 35 Intertrochanteric osteotomies by Kartenbender et al. 19 in 2000. Furthermore, 77% of these had good to excellent long-term outcomes at 23-year follow-up. Parsch et al. 20 reported a rate of osteonecrosis of 2% to 6% with good short term results; however, the incidence of osteoarthritis was reported at 55% after 20-year follow-up. The modified Dunn procedure aims to maintain epiphyseal vascularity through continuity of the epiphysis with the posterior periosteum and capsular retinacular vessels throughout the procedure address the cam deformity and reduced the risk of AVN. It is a technically challenging procedure that can be associated with complication but has been shown to have good functional outcomes in experienced hands.7,21 The senior author has adapted this further to perform a modified subcapital realignment osteotomy.
The aim of this study was to evaluate the outcomes and complications of patients who have undergone our centers adaption of the modified Dunn subcapital realignment osteotomy, for the management of moderate and severe SCFE and compare it with the existing literature.
Materials and methods
Study design
Clinical and radiographic records of all patients who underwent a Subcapital osteotomy for SCFE were retrospectively reviewed between 2009 and 2019. Surgical treatment was provided by the senior author (G.D.). Inclusion criteria and exclusion criteria are shown in Table 1.
Inclusion and exclusion criteria.
SCFE: slipped capital femoral epiphysis; PSA: posterior sloping angle.
Collected records included patient demographics, slip severity, slip stability, type of fixation used, time to surgery, length of follow-up, and presence of AVN at final follow-up. Any complications or subsequent procedures were also recorded. Radiographic slip severity was graded using the posterior sloping angle (PSA) as measured on frog leg lateral of both hips. The PSA of the SCFE was graded accordingly. 22 Stability was graded according to Loder’s classification as stable or unstable. Patients with Loder’s unstable slips were treated as emergency admissions and confined to strict bed rest. Theater was planned on a semi urgent basis. Intraoperative slip stability was also recorded. The senior author (G.D.) assessed this by observing if the capital epiphysis remained attached to the neck during initiation of dislocation. AVN was assessed postoperatively by single-photon emission computed tomography (SPECT) bone scan. This allowed early recognition of AVN and ongoing management with bisphosphonate therapy. Postoperative radiographs were also taken at follow-up appointments to assess sphericity of the femoral head and presence of collapse.
Surgical technique and postoperative management
All operations were performed using the technique described by Ziebarth et al. 23 A lateral approach with trochanteric osteotomy was utilized. An in situ periosteal sleeve peel was carefully done on the exposed lateral femur. A “Z” shaped capsulotomy was then performed and labrum protected (Figure 1(b)). The periosteal sleeve surrounding the femoral neck was further peeled. The head was either not secured or secured with a wire prior to dislocation depending on perceived stability. After head delivery, the ligamentum teres was resected and acetabulum inspected. The femoral neck was reshaped with a combination of nibbler and rasp (Figure 1(c)). The epiphysis was curetted and drilled to assess for blood supply intraoperatively. The head was relocated on the femoral neck and an antegrade wire was passed (Figure 1(d)). After predrilling, the 7 mm headless compression screw (Charlotte Screw—Wright Medical, Memphis, Tennessee) was inserted retrograde (Figure 1(e)). The capsule was repaired and trochanter fixed with multiple 3.5 mm small fragment screws (Depuy Synthes, Raynham, MA, USA). The decision whether to pin the contralateral hip was made on a case by case basis and was not specifically addressed in this study.
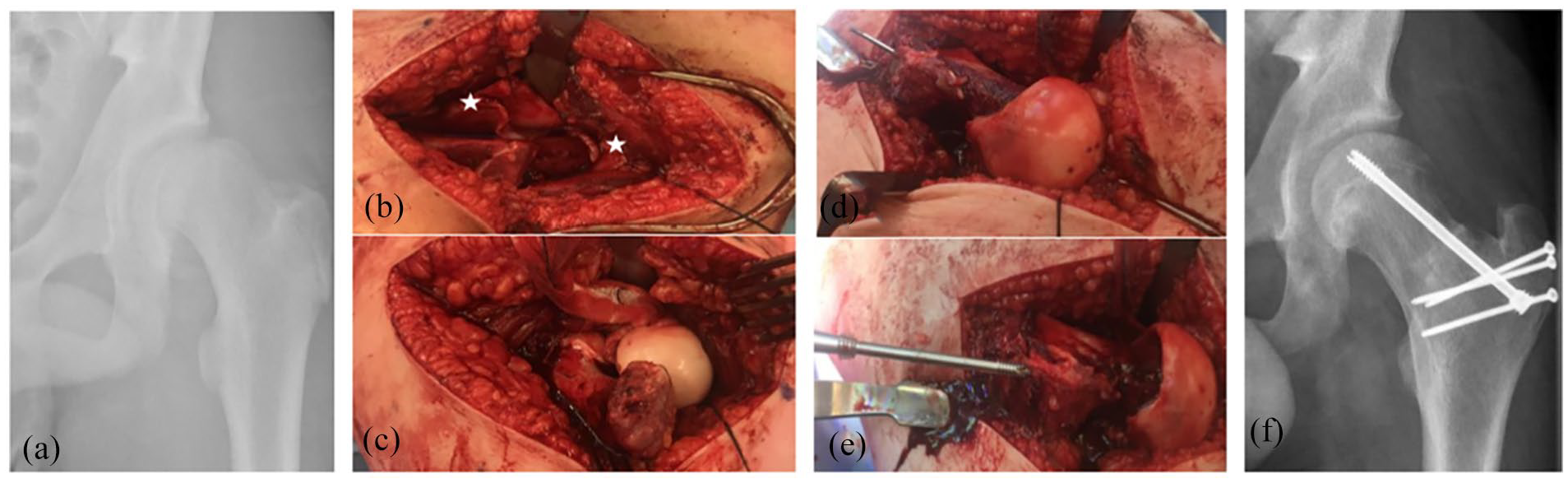
(a) Radiograph demonstrating a sever slip, (b) Z-capsulotomy and periosteal sleeve peel (*), (c) femoral metaphysis with evidence of remodeling requiring re-shaping, (d) epiphysis reduced onto metaphysis and held with an antegrade wire, (e) retrograde insertion of a Charlotte screw, and (f) postoperative radiograph demonstrating fixation of the greater trochanter osteotomy.
Routine postoperative management included touch weight bearing on the affected side. Early active range of motion of the hip was allowed, avoiding the extremes of range. After 6 weeks, the patients were permitted to begin weight bearing as tolerated. The postoperative follow-up included 6 weeks for wound review, then at 3, 6 and 12 months postprocedure then yearly until 5 years. This is our institutions standard follow-up for surveillance for osteonecrosis and complications. A bone scan was performed after 48 h postoperatively. Bisphosphonates were administered at 6 weeks postoperatively if indicated.
Statistical methods
Frequency data were reported as percentages of the overall cohort and/or subset, and demographic and radiological data were presented as the mean, range, and standard deviation. A forward stepwise binominal logistic regression analysis was undertaken to determine the variable(s) that best predicted the odds of 12-month postsurgery AVN. Predictor variables assessed were age at surgery, sex, time from first symptoms to surgery, PSA severity, Loder’s classification, intraoperative stability, and evidence of perfusion on postoperative SPECT-computed tomography (CT).
Results
In total, 123 osteotomies were performed on 116 patients (Figure 2). Overall, 65 patients were male (56.0%) and 72 left hips were affected (58.6%). The overall mean age was 12.4 years (range = 7–17 years), with a female mean of 11.5 (range = 7.9–14.4) and a male of 13.1 (range = 7.0–17.0). A total of 89 (76.7%) were referrals from other hospitals. Mean postoperative stay was 6.2 days (range = 1–20 days). Mean follow-up was 51.3 months (7–126).
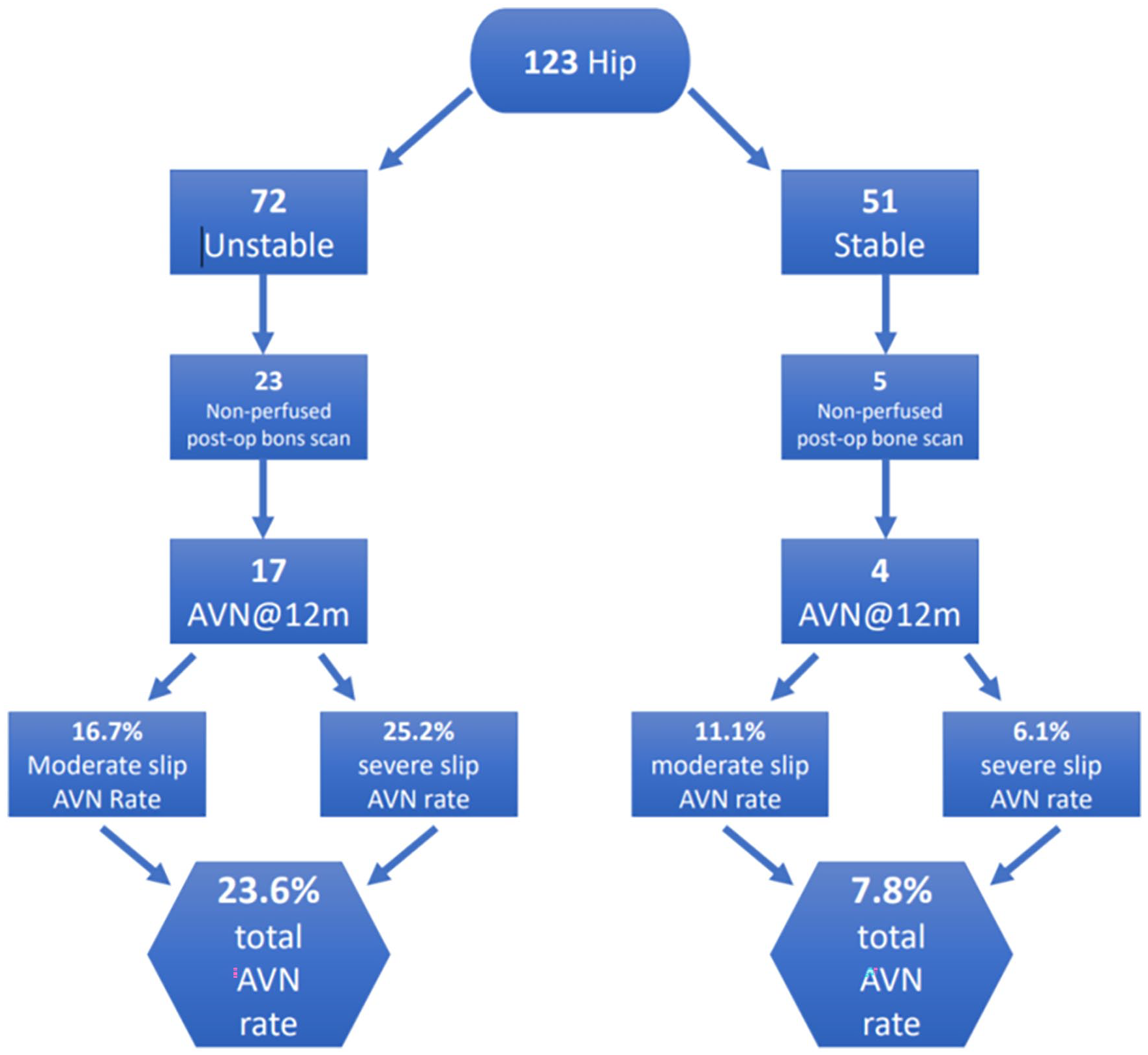
Summary of AVN rates.
The mean PSA was 60.1° (range 36°–88°) with 93 (75%) being severe slips. There were 51 (41.5%) Loder’s stable and 72 (58%) unstable SCFE. Seven of the Loder’s stable hips were found to be unstable intraoperatively as determined by the lead surgeon and 1 unstable was found to be stable. The mean time between onset of symptoms and surgery was 113.1 days (range = 0–445).
In total, 28 of 122 (22.9%) hips had a non-perfused postoperative SPECT-CT bone scan. One patient did not have a postoperative scan and unfortunately went on to develop AVN and collapse. At the 12-month radiograph, 22 of 123 (17.8%) hips were found to have AVN, 3 of which had a perfused postoperative SPECT-CT bone scan. Therefore, 35.7% of the non-perfused SPECT did not develop AVN at 12 months and 3.2% of the perfused hips went on to develop AVN. The total number of hips developing AVN from the Loder’s stable group was 4 (7.8%), comprising of two moderate slips and two severe slips. Of the Loder’s unstable hips, 41.7% of the moderate slips had a non-perfused SPECT and 16.7% went onto develop AVN. Whereas 30.5% of the severe slips had non-perfused scans with 26.7% developing AVN (Table 2).The mean time from diagnosis to surgery overall was 8.9 days (0-96), stable slips was 11.8 days (0–96) and unstable slips was 6.8 days (0–61). Time from diagnostic X-ray to surgery did not appear to influence AVN rates; 25% of unstable hips operated on in <24 h developed AVN, versus 23.7% in 24 h to 7 days and 27.3 >7 days. In total, five hips had a differing intraoperative assessment of stability when compared to Loder’s classification; four were classified as Loder’s stable but intraoperatively unstable and 1 was Loder’s unstable but intraoperatively stable.
Demonstrating rates of non-perfused postoperative SPECT-CT bone scans and radiographic AVN at 1 year, divided by Loder’s classification and PSA.
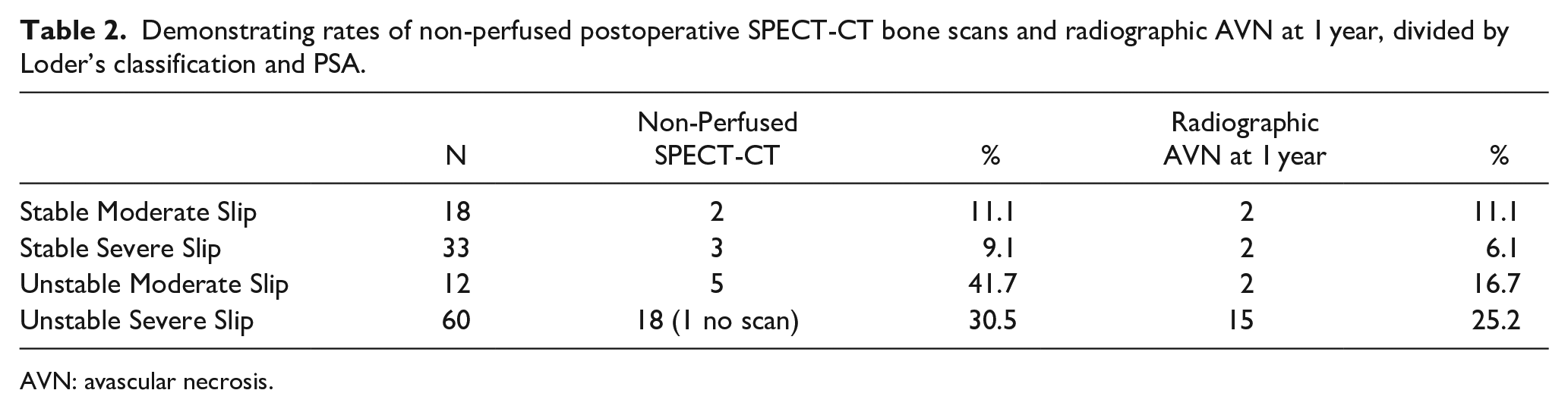
AVN: avascular necrosis.
The final logistic regression model was statistically significant, χ2(2) = 41.5, p < 0.001, explained 47.9% (Nagelkerke R 2 ) of the variance in 12-month postsurgery AVN rates and correctly classified 87.7% of cases. The only independent variables retained in the final model were evidence of perfusion on postoperative SPECT-CT whereby patients with a non-perfused SPECT-CT increased the odds of 12-month postsurgery AVN by a factor of 34.8.
Complications occurred in 32 (26%) procedures. Ten hips (8.1%) required repositioning of the cephalad screw for penetration. Six were identified on the SPECT-CT bone scan and returned to theater during the same admission, the remaining four were associated with collapse of the femoral head and eventually went on to require total hip replacement (THR). Four hips (3.3%) required elective screw removal due to irritation. Seven hips (5.7%) went on to have a THR all for AVN and seven hips (5.7%) required a fibular graft. Two patients (1.6%) had surgical site infection with one being superficial and treated with oral antibiotics. The second was a deep infection requiring three washout procedures and a prolonged course of antibiotics. Two patients had a symptomatic leg length discrepancy, one of which was treated with femoral lengthening. The rate of complication in the patients with AVN was 8.9%. There were no postoperative dislocations or loss of reduction.
Discussion
The management of moderate and severe SCFE remains controversial. The modified Dunn procedure subcapital realignment osteotomy is a technically challenging procedure which historically has been associated with a variable AVN rate with studies reporting AVN rates ranging from 2% to 34%.17,21,24 –32 It is important to note that the available literature consists predominately of small retrospective case series with few studies consisting of more than 50 patients. Birke et al. 33 recently published their experience in >200 patients and reported that 14.6% of their hips had AVN on the postoperative SPECT-CT bone scan. Their cohort, similar to our own, likely represents the rate of AVN of patients who are treated in high-volume centers. The Queensland Children’s Hospital provides tertiary cover to a large catchment area, consisting of the entirety of Queensland and parts of northern New South Wales. This combined with certain population demographics such as high numbers of Aboriginal and Pacific Islander patient groups contributes to over representation of SCFE in our center compared to other units around the world. Although some authors advocate avoiding the “unsafe window” of 1 to 7 days for surgery, like Birke et al. we also found that time of surgery did not influence AVN rates.34,35 We found a discrepancy between the initial findings on SPECT bone scan and the 12-month radiograph with eight of these patients not developing AVN. Although this may represent an element of misreporting of scans by our radiologists, it may also suggest that by restoring the anatomy and relieving the threatened blood supply of the femoral head, it allows re-perfusion that happens relatively soon after surgery but not immediately. Six of these eight hips underwent surgery <7 days after diagnosis which possibly suggested that early restoration of normal anatomy may facilitate re-perfusion to occur in a threatened head, although numbers are too small to make a firm conclusion.
When comparing the modified Dunn osteotomy with PIS, a recent systematic review and meta-analysis by Cheok et al. 36 reported that there was an improvement in the Alpha and Southwick angles, but no difference in postoperative AVN rates. While we acknowledge that PIS followed by corrective osteotomy, such as a Southwick or Imhauser osteotomies are valuable treatment options, our preference is for a subcapital realignment osteotomy which we feel addresses the need for deformity correction and slip stability with favorable long-term outcomes. Severity and stability of slip remain some of the best predictors of AVN and long-term complications with an increasing volume of literature supporting a realignment osteotomy in the unstable group.37,38
Complications are frequently underdiscussed in the orthopedic literature. 39 SCFE patients are usually independently functioning prior to onset of pathology and there can be significant impact from the condition on their quality of life and education as well as financial implications.40 –42 The complications of the modified Dunn can be considerable in their own right, and therefore, surgery should not be undertaken lightly and preferably by experienced clinicians in high-volume centers. We had six patients who required a return to theater due to penetration of the screw as identified on postoperative CT. More recently, we have implemented intraoperative isocentric C-arm imaging to achieve a three-dimensional (3D) image in theater to address this. AVN can lead to poor outcomes in the patients who develop it and which can necessitate further intervention. Seven patients (5%) went on to require a THR, and while implant survivorship has improved greatly, this still has an important impact on the patient. All patients undergoing a subcapital realignment osteotomy should be thoroughly counseled as to the potential long-term complications of pathology and its surgical treatment.
Limitations
This study was limited by being a retrospective analysis of a single center’s experience. No formal patient outcome measures were collected at the time of surgery or during follow-up meaning we rely on radiographic outcomes and complications alone. There were also no comparative data collected for patients undergoing pinning in situ from our center. One potential limitation is the use of a single screw to maintain the femoral head reduction; however, we did not experience any loss of position in our patient cohort. Three patients had a final follow-up radiograph taken at less than 12-month following surgery. These were taken at 7 and 8 months and showed no evidence of AVN, although we acknowledge that this could possibly develop at a later date.Some follow-up was performed remotely due to our large geographic area, and this contributed to difficultly to locating some radiographs.
Further studies to assess both our long-term AVN rates but also patient reported outcome measures would be of huge benefit and are already underway in our unit. This will enable us to accurately target which patients would benefit most from an SCRO and further reduce our complication rate.
Conclusion
We present our results of treating the moderate and severe slipped subcapital femoral epiphysis using the subcapital realignment osteotomy. We recommend its use in both the moderate and severe slips to restore normal hip anatomy in patient cohorts such as ours. This is one of the largest reported studies in the literature and supports its use in a tertiary center with experienced staff to reduce the risk of AVN and other associated complications.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241246144 – Supplemental material for Subcapital realignment osteotomy for the treatment of moderate and severe slipped upper femoral epiphysis: A retrospective study of 123 hips in a tertiary center
Supplemental material, sj-pdf-1-cho-10.1177_18632521241246144 for Subcapital realignment osteotomy for the treatment of moderate and severe slipped upper femoral epiphysis: A retrospective study of 123 hips in a tertiary center by Daniel MG Winson, William J Cundy, Megan JN Roser, Christopher P Carty, Sheanna Maine and Geoffrey Donald in Journal of Children’s Orthopaedics
Footnotes
Author contributions
D.M.G.W. contributed to data acquisition, analysis, and interpretation and manuscript drafting, critical revision, and final approval. W.J.C. contributed to data acquisition, analysis, and interpretation and manuscript drafting, critical revision, and final approval. M.J.N.R. contributed to study design, data acquisition, analysis, and interpretation and manuscript final approval. C.P.C. contributed to data analysis and interpretation and manuscript final approval. S.M. contributed to manuscript final approval. G.D. contributed to study design, data acquisition, analysis, and interpretation and manuscript final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This project was approved by the Royal Children’s Hospital Human Research Ethics Committee (HREC/45968/RCHM-2019-173470) with retrospective data access for the purpose of research being subsequently approved by the Queensland Government Department of Health (PHA 173470). The study was conducted in accordance with the Declaration of Helsinki and was approved by the Royal Children’s Hospital Human Research Ethics Committee (HREC/45968/RCHM-2019-173470) with retrospective data access for the purpose of research being subsequently approved by the Queensland Government Department of Health (PHA 173470) on 19 June 2019, with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated de-identified data. For this study, the raw data were first extracted from the hospital database, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified. The authors declare that they did not receive funding for this project.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.