
Abstract
Background:
Fracture separation of the distal humeral epiphysis in children is a relatively uncommon injury, predominantly occurring in children under 3 years. It has a high risk of treatment delays. This study aims to evaluate outcomes in the management of fracture separation of the distal humeral epiphysis treated seven or more days post-initial injury.
Methods:
A retrospective analysis was conducted on patients diagnosed with fracture separation of the distal humeral epiphysis between November 2016 and October 2023. Inclusion criteria encompassed patients with delayed presentation of fracture separation of the distal humeral epiphysis who underwent surgical intervention seven or more days following the initial injury. Demographic data were collected, and fractures were categorized using the modified DeLee classification. Plain radiographs facilitated the assessment of the carrying angle and postoperative Baumann angle. Clinical outcomes were evaluated using the Flynn criteria.
Results:
The study included 12 patients who met the inclusion criteria. The average age at the time of injury was 1.59 years. According to the modified DeLee system, fracture classification identified one type I fracture, eight type II fractures, and three type III fractures. The average duration from injury to surgery was 11.8 days. The mean surgical duration was 21.5 min. The average follow-up period was 40.7 months. One patient exhibited cubitus varus development. Based on the Flynn criteria, outcomes were as follows: seven patients had excellent outcomes, four had good outcomes, and one had a poor outcome.
Conclusion:
Closed reduction with percutaneous K-wire fixation represents a minimally invasive approach suitable for children diagnosed with fracture separation of the distal humeral epiphysis seven or more days post-initial injury. Most of these patients experienced favorable outcomes.
Level of evidence:
IV
Keywords
Introduction
Transphyseal fractures of the distal humerus, also referred to as fracture separation of the distal humerus epiphysis (FSDHE) or epiphysiolysis of the distal humerus, involve the separation of the growth plate at the lower end of the humerus. These fractures are primarily observed in children under 3 years 1 and account for 1.6% of all distal humerus fractures. 2 FSDHE can be radiographically misinterpreted as a lateral condyle fracture, traumatic elbow dislocation, or supracondylar humeral fracture. 3 Posteromedial displacement of the radius and ulna in young children is highly indicative of FSDHE, which can be definitively diagnosed via ultrasound. 4 Standard radiographs are frequently employed to guide FSDHE treatment, but they may not reveal the precise anatomy of the fracture ossified5,6 due to the lack of bone ossification. As a result, confirmation of adequate reduction during conservative treatment is difficult, and incomplete reduction can often result in cubitus varus.7,8 The preferred management approach for most FSDHE cases involves closed reduction and percutaneous K-wire fixation, aided by an elbow arthrogram. 5 Contrast administration enhances the visualization of the unossified epiphysis of the distal humerus, assisting in anatomical reduction. 7
Prompt diagnosis is essential for the effectively closed reduction of the fracture. Many experts advise against delaying fracture reduction more than 7 days post-injury due to concerns about avascular necrosis, growth plate trauma, and growth inhibition.2,6,9 However, some patients can be treated seven or more days after the initial injury.4,6,10 Although numerous studies have examined the outcomes of FSDHE,1,3,7,10 no prior investigation specifically evaluated closed reduction in cases presenting more than 7 days post-injury. This study aims to assess the outcomes following closed reduction and percutaneous Kirschner wire (K-wire) fixation, supplemented by an elbow arthrogram, for managing FSDHE cases treated seven or more days after the initial injury.
Materials and methods
Patient selection and data collection
This study received approval from the ethics committee of our institution (2024002). We conducted a retrospective analysis of data from children who experienced delayed treatment of FSDHE, occurring seven or more days post-injury, spanning from November 2016 to October 2023. Informed consent for surgical treatment was obtained from the patients’ legal guardians.
Inclusion criteria encompassed: (1) children presenting with delayed FSDHE, undergoing surgery seven or more days after the injury and (2) those with complete clinical and radiographic data. Exclusion criteria included patients with other types of injuries, congenital anomalies, and incomplete clinical and radiographic data. A total of 12 patients (9 males, 3 females, encompassing 12 elbows) met the criteria for inclusion in this study.
The collected clinical and radiographic data included age at the time of trauma, sex, affected side, fracture type as per the modified DeLee classification, 1 duration from injury to surgery, operative time, follow-up period, range of motion (ROM), changes in ROM, carrying angle, 11 changes in carrying angle, postoperative Baumann angle, 12 Flynn rating, 13 and reasons for delayed treatment.
Complications recorded included neurovascular injury, secondary displacement, refracture, infection, nonunion, and malunion.
All patients enrolled in the study underwent closed reduction and percutaneous K-wire internal fixation, assisted by an elbow arthrogram.
Surgical procedure
Patients underwent surgery in a supine position under general anesthesia. Before attempting closed reduction, an elbow arthrogram (using iodixanol contrast) was performed to assess fracture displacement and the reduction process.
The elbow was gradually subjected to axial traction at an angle between 60° and 90°. Under traction, lateral displacement correction was first addressed, followed by anterior–posterior displacement correction. Subsequently, the elbow was immobilized in flexion using an elastic bandage to maintain the reduction. If the reduction was deemed satisfactory, percutaneous K-wire fixation was then performed.
In cases where the initial reduction was unsatisfactory, the reduction maneuver was repeated, followed by a reassessment of the reduction. A 1.6 mm K-wire was then inserted through the lateral humeral condyle to partially stabilize the fracture (as illustrated in Figure 1). If the reduction remained unsatisfactory even after C-arm verification, the K-wire was retracted just below the fracture line. The reduction process was repeated, and the K-wire was advanced again into the proximal fragment. This maneuver could be repeated up to three times, depending on the quality of the reduction (see Figure 2). Once the reduction was considered satisfactory, the K-wire fixation was completed. Finally, a cast was applied to the elbow, maintaining it in 30° to 60° of flexion.

The elbow is held in flexion, and pressure is applied from the medial condyle to the lateral condyle for optimal frontal plane reduction; then, the K-wire can be advanced to cross the fracture line and reach the opposite cortex.
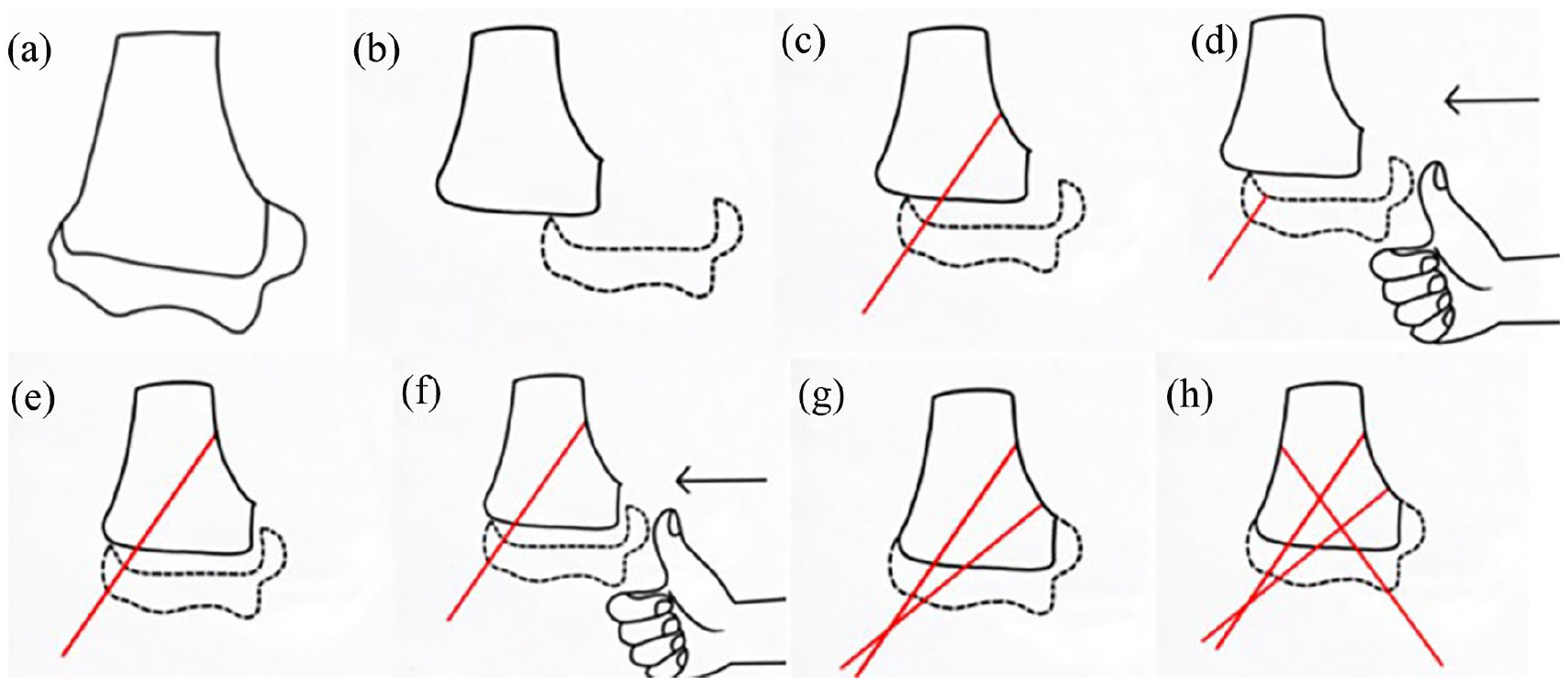
An anatomical diagram of the distal humerus is shown (a). The diagram illustrates the medial displacement of the distal humeral epiphysis (b). If the reduction remains unsatisfactory (c), the K-wire is retracted just below the fracture line and the reduction process is repeated (d), followed by advancing the K-wire into the proximal fragment again (e). To ensure stability, a second K-wire will be inserted to maintain reduction, and if necessary, a third K-wire will be inserted at the medial site (f-h).
Clinical and radiographic evaluation
Patients underwent routine clinical and radiographic follow-up assessments. Anteroposterior (AP) and lateral elbow radiographs were taken at 2 and 4 weeks postoperatively, followed by additional assessments every 3–6 months (see Figure 3). Four weeks after the surgery, the K-wires and cast were removed, and patients commenced active functional elbow exercises. Throughout the follow-up period, the carrying angle 11 and ROM of the affected elbow were recorded and compared to those of the contralateral side. The postoperative Baumann angle 12 and configuration of the K-wires were evaluated using plain radiographs. Clinical functionality was assessed utilizing the Flynn rating system. 13
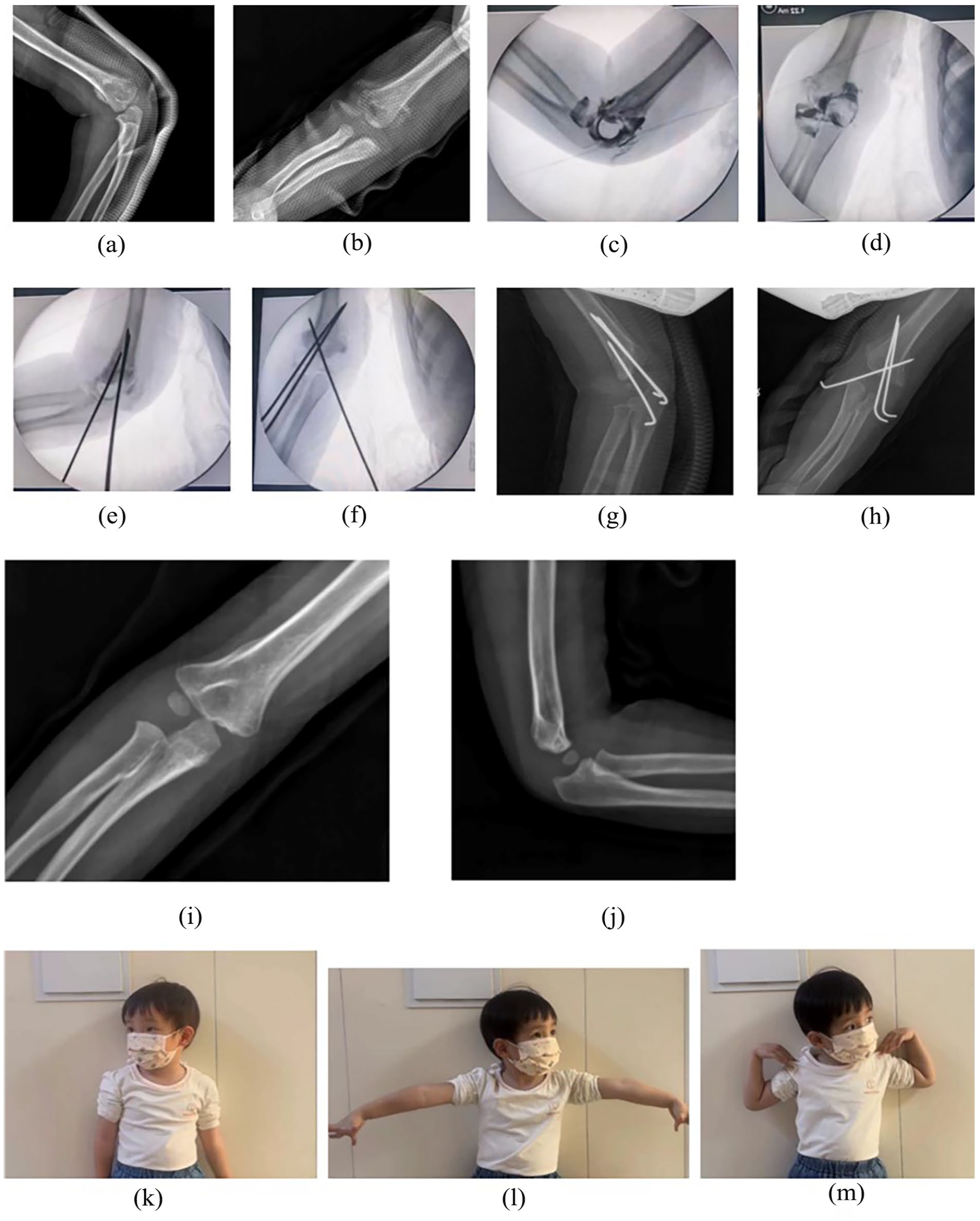
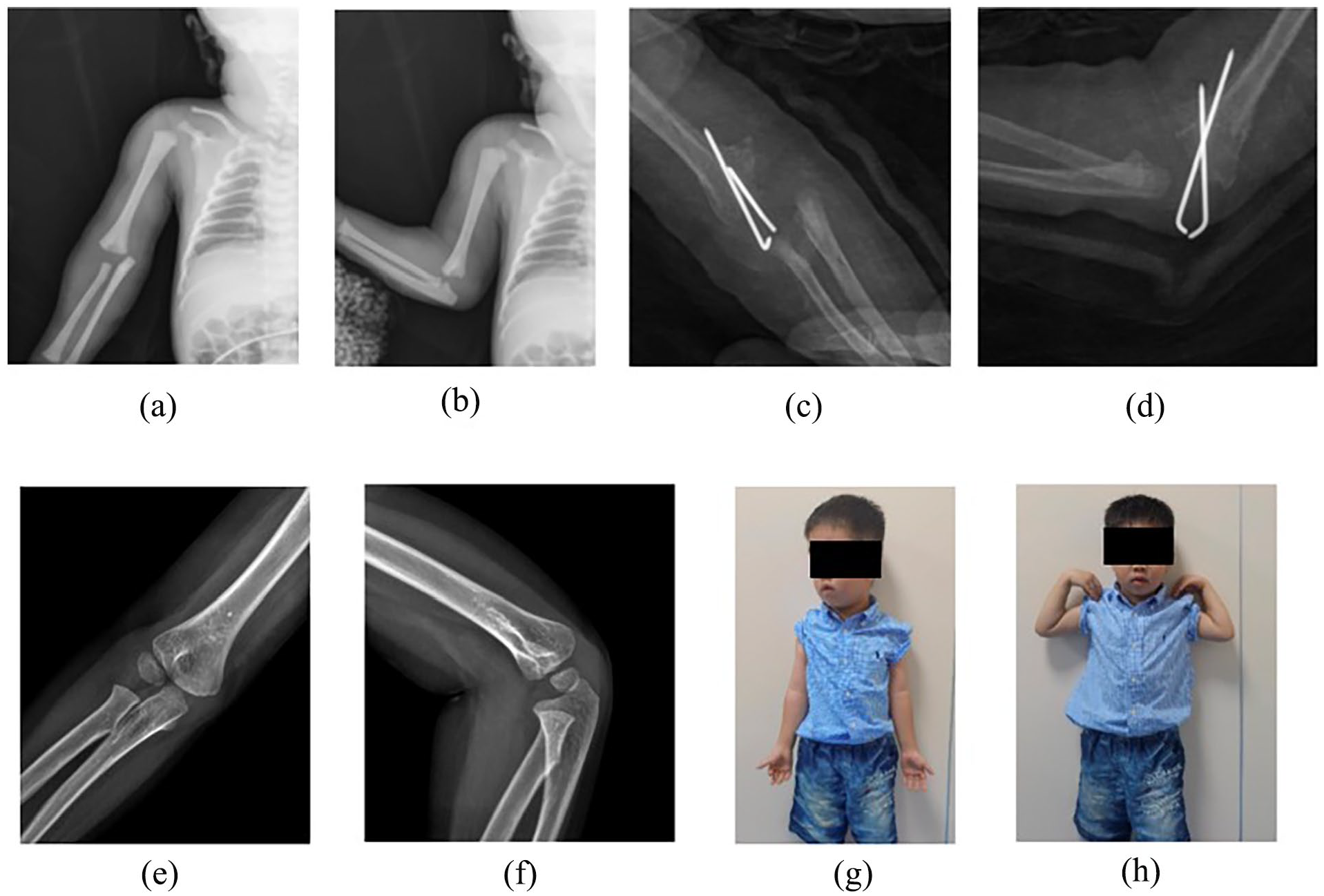
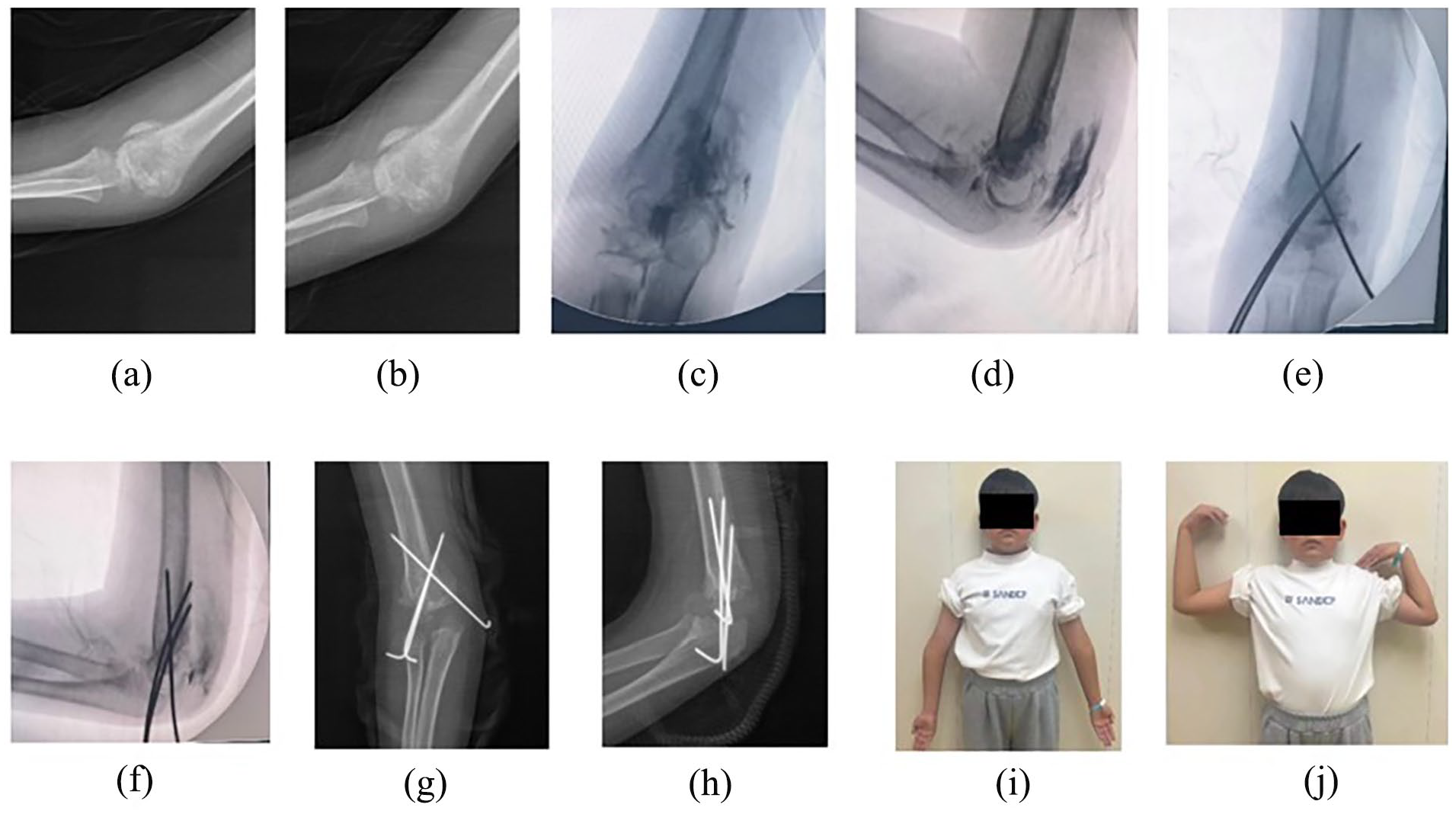
One year and 3-month-old female (case 12) with FSDHE, who underwent surgery 20 days after the initial injury. Preoperative radiographs showed callus (a, b); preoperative and postoperative arthrograms (c, d); postoperative radiographs (e, f); follow-up radiographs taken (g, h) 1 and (i, j) 14 months after surgery, respectively; photographs capturing the physical appearance at the final follow-up assessment (k, l, m).
Statistical analysis
The statistical analyses were conducted using IBM SPSS version 26.0. Spearman correlation coefficients were employed to explore the relationships between various variables. These variables included age at injury, follow-up duration, a modified version of DeLee’s classification, the interval between injury and surgery, operative time, Flynn rating, changes in ROM, and alterations in the carrying angle. Correlation coefficients below 0.4 indicated a weak correlation; coefficients ranging from 0.4 to 0.7 suggested a moderate correlation; and coefficients exceeding 0.7 denoted a strong correlation. The threshold for statistical significance was established at p < 0.05.
Results
This study enrolled 12 patients, comprising 9 males and 3 females. The mean age of the participants was 1.59 years, ranging from 0.02 to 6 years. Detailed clinical information about the patients is presented in Tables 1 and 2.
Patient demographics.
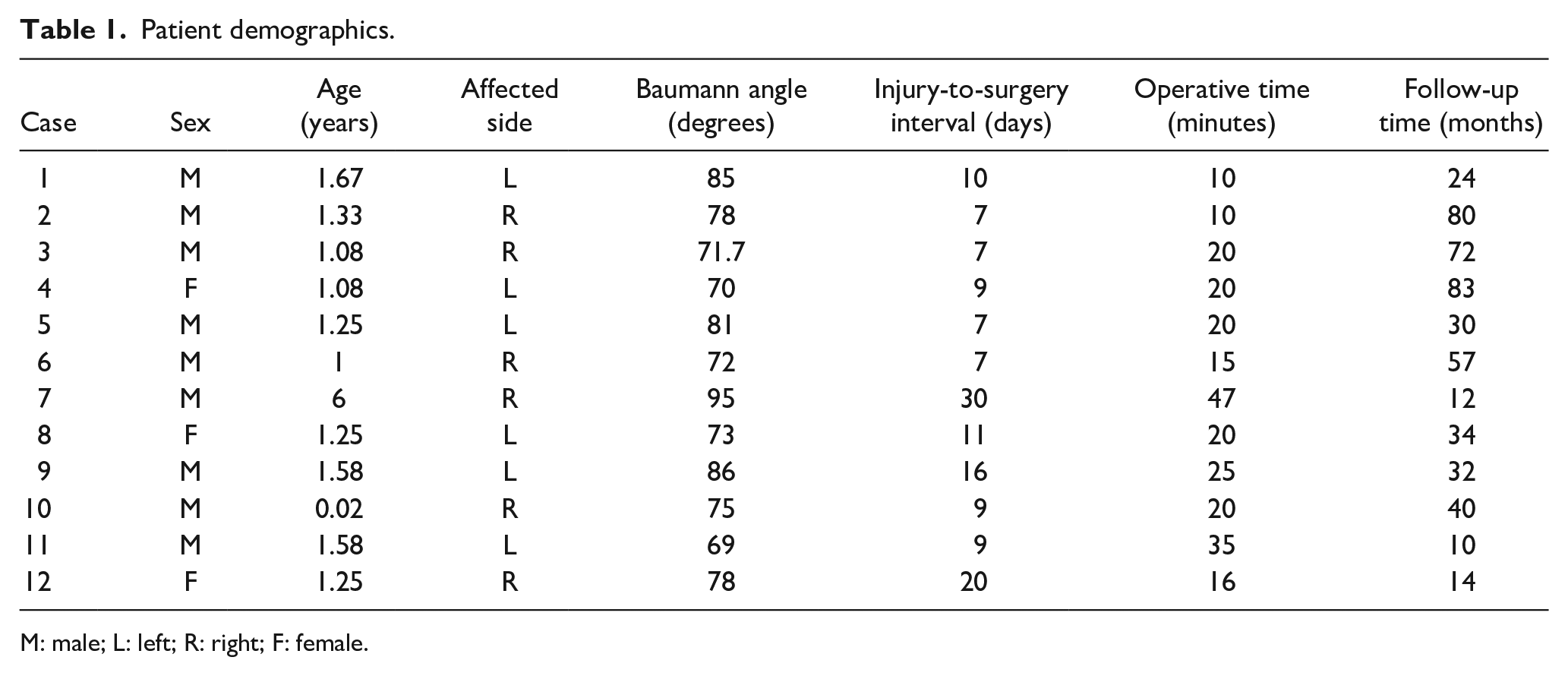
M: male; L: left; R: right; F: female.
Clinical data.
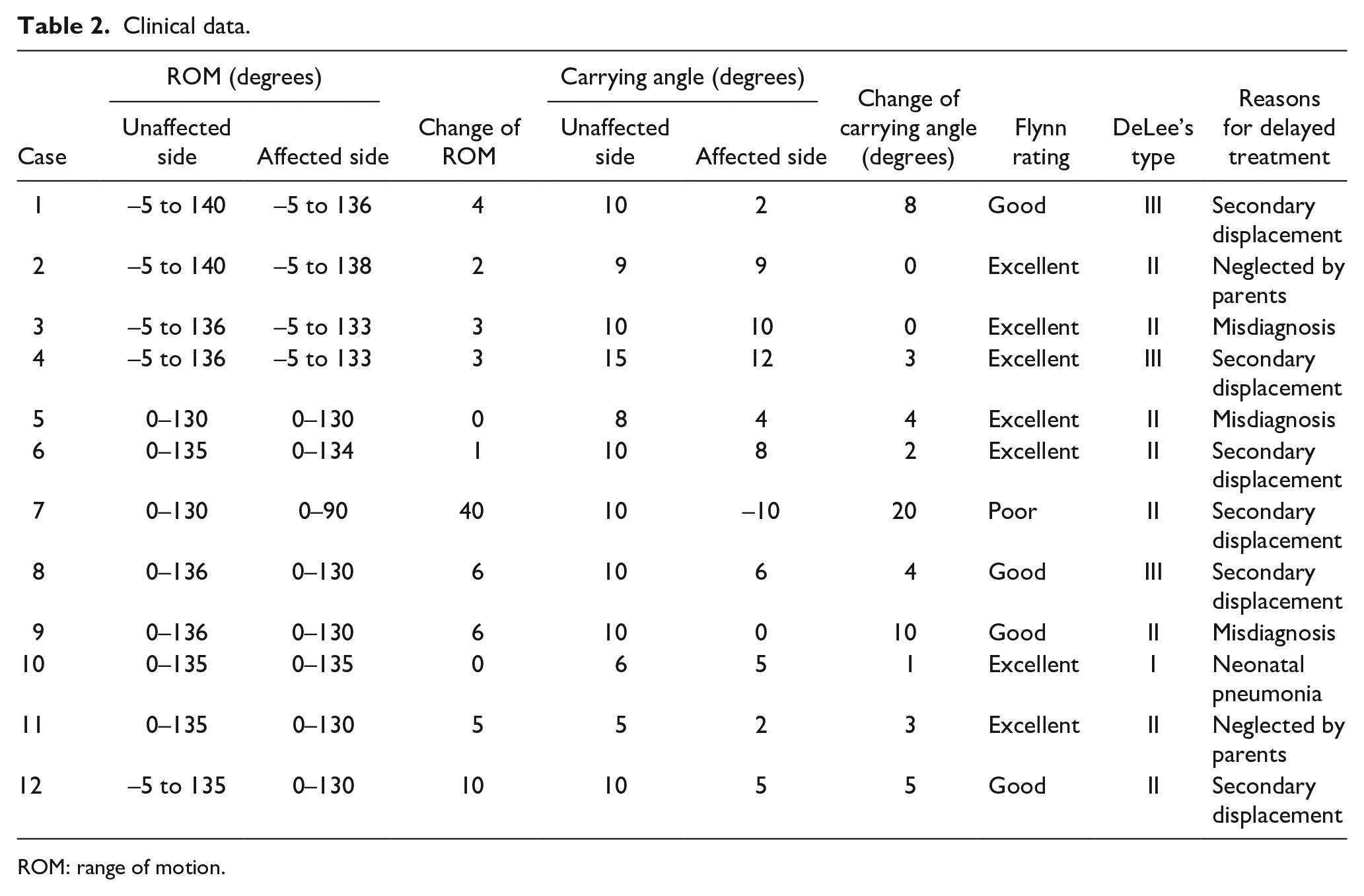
ROM: range of motion.
According to the modified DeLee classification, 1 the fracture distribution among the patients was as follows: one patient with a type I fracture, eight type II fractures, and three type III fractures. The average duration from injury to surgery was 11.8 days, ranging from 7 to 30 days. The mean operative time recorded was 21.5 min, varying from 10 to 47 min. The average follow-up period was 40.7 months, ranging from 10 to 83 months.
Only one patient had obvious cubitus varus and elbow stiffness, while two patients had only mild cubitus varus. Analysis using Spearman correlation coefficients revealed that the interval between injury and surgery strongly correlated with changes in the ROM, carrying angle, 11 and Flynn rating, as shown in Table 3. Furthermore, a moderate correlation was observed between age and changes in carrying angle, 11 Flynn rating, 13 and changes in ROM, detailed in Table 4. However, no significant correlation was found between operative time and variables such as age, changes in ROM, postoperative Baumann angle, 12 fracture type, and Flynn rating 13 (as indicated in Table 5).
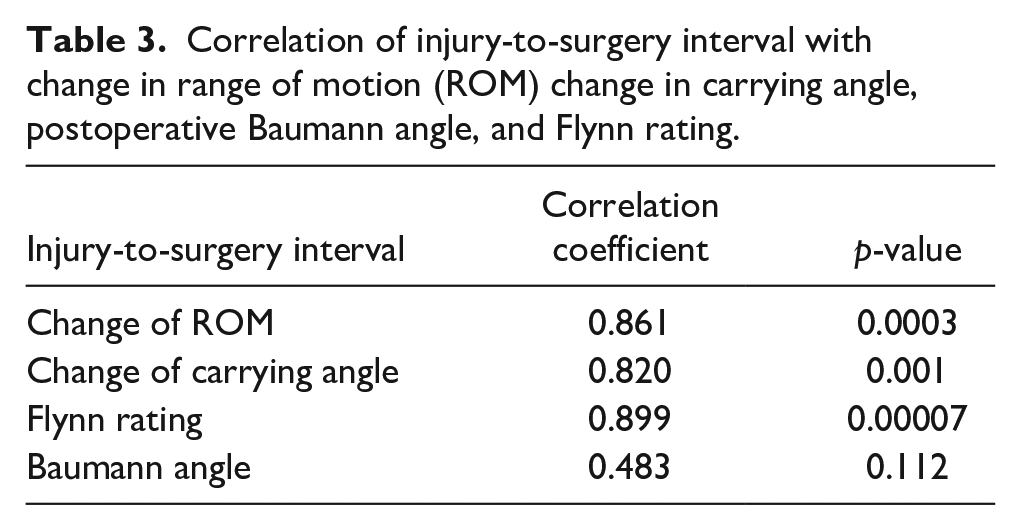
Correlation of injury-to-surgery interval with change in range of motion (ROM) change in carrying angle, postoperative Baumann angle, and Flynn rating.
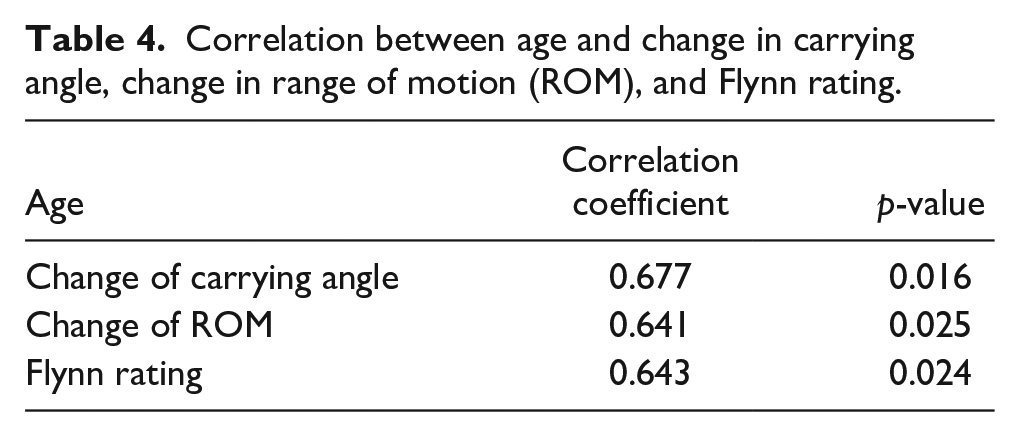
Correlation between age and change in carrying angle, change in range of motion (ROM), and Flynn rating.
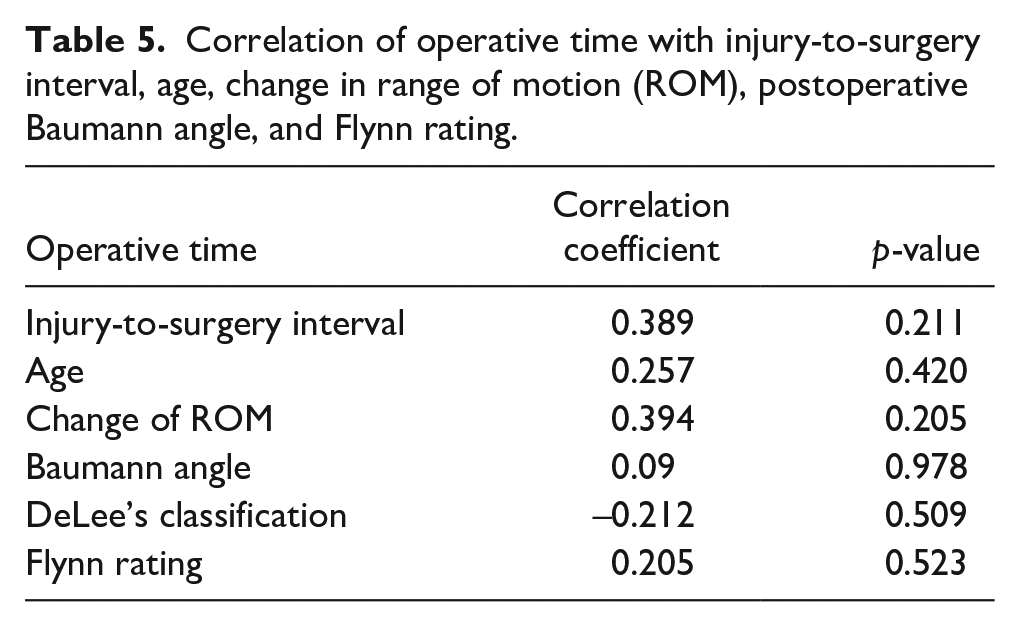
Correlation of operative time with injury-to-surgery interval, age, change in range of motion (ROM), postoperative Baumann angle, and Flynn rating.
Discussion
This study aimed to evaluate the clinical and radiographic outcomes of delayed treatment in cases of FSDHE. Delayed treatment can be attributed to various factors, including parental neglect, misdiagnosis, and secondary displacement following conservative treatment.4,5 Because FSDHEs are highly associated with child abuse,2,4,8 the clinician should be vigilant, especially in guardians who do not seek care immediately after the trauma and in patients with other associated injuries. None of the patients in our study had FSDHE secondary to child abuse. In children over 6 months of age, closed reduction and K-wire fixation are recommended as1,14 effective interventions, as conservative management in this age group carries a heightened risk of cubitus varus deformity 9 development, with secondary displacement occurring in approximately 50% of cases. 10
In our study, secondary displacement after conservative treatment is the main cause of delayed surgical treatment. The late presentation to our institution suggests that delayed treatment might have influenced the outcomes of closed reduction. Notably, Abe et al. 9 reported an association between delayed diagnosis and treatment and an increased prevalence of elbow deformity in children with FSDHE.
The predominantly cartilaginous composition of the distal humerus in FSDHE makes it invisible on plain radiographs. In one study, 56% of cases were initially missed on radiographs, with misinterpretations including normal findings, elbow dislocation, and supracondylar. 4 fractures. Elbow dislocations are exceptionally rare in children under 3 years old, rendering them more prone to physical fractures. 5 Specifically, when forearm misalignment with the humeral shaft is posteromedially displaced, FSDHE is more likely than an elbow dislocation, which4,5,15 typically presents with posterolateral displacement.
Diagnosis of FSDHE can be achieved through ultrasound, magnetic resonance imaging (MRI), and elbow arthrography. Ultrasound is advantageous due to its non-invasive nature, absence of radiation exposure or sedation requirements, and efficiency and cost-effectiveness. Conversely, MRI often necessitates sedation and may not be readily available. An elbow arthrogram, helpful in diagnosing epiphyseal separation fractures and evaluating reduction quality, involves invasive procedures under anesthesia.5,6,16 All patients in this study underwent elbow arthrography.
The prognosis is generally positive when the injury is promptly recognized and treated. Gilbert and Conklin 2 notably advise against late manipulation more than 4 to 7 days post-injury, citing concerns about growth disturbances in physical injuries at high risk for such complications. Avascular necrosis incidence has been reported to be significant in distal humeral epiphyseal separation following open reduction. 17 However, Galeotti et al. 10 documented favorable outcomes with closed reduction and percutaneous K-wire fixation in five neonates with birth trauma with a maximum delay of 10 days post-injury. In our study, treatment performed up to 20 days after the initial injury yielded promising results. However, it should be noted that our series included only one neonate with a cesarean section–related fracture (see Figure 4).
Seven-day-old male (case 10) with FSDHE who underwent surgery 9 days after the initial injury. (a, b) The secondary ossification center of the distal humerus was not visible on radiographs, and the forearm is displaced posteromedially with respect to the humeral shaft; only two K-wires were inserted due to the small size of the humerus. (c, d) Callus had formed 4 weeks after surgery; (e, f) follow-up radiographs taken 3 years after surgery; (g, h) photographs capturing the physical appearance at the final follow-up.
Our findings indicate a strong correlation between the time from injury to surgery and changes in ROM, changes in carrying angle, and Flynn rating. A longer interval post-injury was associated with more significant bony callus formation, complicating the achievement of satisfactory reduction.
Cubitus varus is a frequent complication of FSDHE.18 –20 The two primary factors leading to cubitus varus deformity are inadequate reduction and loss of reduction, 3 while growth plate injury is not a primary contributor to this deformity. 7 In our study, satisfactory reduction was not achieved in one patient (case 7), who was treated 30 days post-injury. This resulted in cubitus varus and elbow stiffness (see Figure 5).
Six-year-old male (case 7) with FSDHE who underwent surgery 30 days after the initial injury. Radiographs showed callus formation and standard anteroposterior and lateral elbow radiographs could not be obtained due to elbow stiffness and pain (a, b). After the elbow arthrogram was performed, a standard anteroposterior and lateral view was taken to assess fracture displacement (c, d). Despite our best efforts, the posteromedial displacement improved but remained (e, f). Four weeks after surgery, the fracture was healed and the K-wires were removed (g, h). At the last follow-up, an obvious cubitus varus and limited range of motion of the elbow were observed (i, j).
Distal humerus fractures are known for diminished remodeling capacity, especially in children over 5 years old. 21 One patient in our study exhibited a persistent loss in 40° of ROM and 20° in carrying angle over a 1-year follow-up period. In such cases, corrective osteotomy at a later stage might be more appropriate than closed reduction with percutaneous K-wire fixation. Age emerged as a significant prognostic factor in this study, showing a moderate correlation with changes in carrying angle, change in ROM, and Flynn rating. The favorable outcomes in neonatal FSDHE cases reinforce this observation.6,15,22
The duration of the surgical procedure did not correlate with outcomes or the injury-to-surgery interval. Reduction was attempted a maximum of three times to avoid epiphyseal plate injury. In instances where sufficient reduction was not achieved after three attempts, open reduction was not considered due to the potential risk of avascular necrosis.9,14,17,20 Therefore, the duration of the operation likely did not influence the results.
Overall, closed reduction with percutaneous K-wire fixation is viable for patients with FSDHE treated between 7 and 20 days post-injury. However, it is not advisable for patients injured more than 20 days before intervention, as achieving adequate reduction becomes challenging due to bony callus formation.23,24 In these scenarios, mobilization, follow-up, and corrective osteotomy for secondary cubitus varus are recommended.
This study does have limitations. First, its retrospective nature may introduce typical biases of such reviews. Second, the sample size was limited, and there was no control group. Despite these constraints, the number of patients included is significant, given the rarity of the injury. Furthermore, our analysis included a homogeneous group of patients diagnosed with FSDHE more than 7 days post-injury. Third, some clinical signs and symptoms of cubitus varus may only become apparent during adolescence or adulthood, whereas the mean follow-up period in this study was 40.7 months.
Conclusion
In conclusion, closed reduction with percutaneous K-wire fixation represents a minimally invasive approach suitable for children diagnosed with FSDHE seven or more days following the initial injury. Our findings suggest that the treatment window could be extended to 20 days, within which favorable outcomes are achievable. Beyond this period, observation is advised, and the consideration of the treatment for secondary cubitus varus at a later stage may be necessary if complications arise.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241246142 – Supplemental material for Closed reduction with percutaneous Kirschner wire fixation for delayed treatment of distal humeral epiphyseal fracture separation
Supplemental material, sj-pdf-1-cho-10.1177_18632521241246142 for Closed reduction with percutaneous Kirschner wire fixation for delayed treatment of distal humeral epiphyseal fracture separation by Xinwu Wu, Linkun Wu, Federico Canavese, Dianhua Huang and Shunyou Chen in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors thank Chenyan Lin in Medical Record Department for data collection.
Availability of data and material (data transparency)
All authors made sure that all data and materials support their published claims and comply with field standards.
Author contributions
X.W. and L.W. contributed equally toward design of the study, article preparation, statistical analysis, revision, and drafted the article. D.H. was involved in statistical analysis and revision of the article. F.C. was involved in article preparation, statistical analysis, and revision. S.C. contributed toward design of the study, surgery and general supervision of the research group. All authors read and approved the final article.
Code availability (software application or custom code)
All authors made sure that all software applications support their published claims and comply with field standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Project of Fuzhou Science and Technology (2022 S-057); Key Clinical Specialty Discipline Construction Program of Fuzhou, Fujian, P.R. China (20220104); Fujian Provincial Clinical Medical Research Center for First Aid and Rehabilitation in Orthopedics Trauma (2020Y2014); Fuzhou Trauma Medical Center Project (2018080303).
Ethical statement
All procedures in the study involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This was a retrospective study and approved by the Medical Ethics Committee of Fuzhou Second Hosptial (2024002).
Informed consent
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. Written informed consent to participate in this study was provided by the participants’ legal guardians/next of kin.
Consent for publication
All authors agreed with the content and gave explicit consent to submit the work after obtaining consent from the responsible authorities at the organization where the work had been carried out.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.