
Abstract
Background:
Congenital pseudarthrosis of the tibia is a limb deformity, which can be distressing for the affected patients and the pediatric orthopedic surgeons involved. We hypothesized that the modified McFarland procedure would avoid fractures and even have a corrective effect on the affected tibia in congenital pseudarthrosis of the tibia patients. Toward this end, we evaluated the midterm results of treating congenital pseudarthrosis of the tibia patients of Crawford Type I and II with allograft bypass combined with long-term bracing.
Methods:
This study retrospectively evaluated 7 patients with congenital pseudarthrosis of the tibia who were treated with allograft bypass combined with long-term bracing between 2009 and 2018. The median follow-up was 7.0 years (range 3.8–10.0 years). The medical records and radiographs were reviewed for demographic data, clinical characteristics, outcomes, and complications.
Results:
At the time of the last follow-up, all allografts revealed complete consolidation in the patients’ tibiae at both ends. All patients presented no functional restriction of the lower limbs and no amputation or non-union has occurred. Most of the obvious deformities of the tibia diaphysis or ankle joint were corrected. Two complications occurred that required successful revision surgery.
Conclusion:
In this series of seven congenital pseudarthrosis of the tibia patients, the allograft bypass technique showed satisfactory midterm results and validated our hypothesis. For congenital pseudarthrosis of the tibia patients of Crawford Type I and II, this procedure combined with long-term bracing, which involves the affected leg only, can delay or possibly prevent fractures, decrease tibial malalignment, and preserve leg length.
Level of evidence:
level IV.
Introduction
Congenital pseudarthrosis of the tibia (CPT), one of the most challenging diseases in pediatric orthopedics, is characterized by segmental osseous dysplasia and progression to fractures and pseudarthrosis at walking age with a substantial risk of non-union, leg-length discrepancy (LLD), and malalignment of the tibia. 1 CPT contains a continuum of disease beginning with an anterolateral bowing of the tibia, which progresses to pathological tibial fractures with subsequent pseudoarthrosis. 2
CPT always occurs congenitally and fails to heal after either a spontaneous stress fracture or a corrective osteotomy due to an impaired callus formation, eventually resulting in pseudarthrosis. 3 Some surgeons also use the terms “pre-pseudarthrosis stage,” “pre-fracture stage,” or “anterolateral bowing of the tibia” for this stage.4,5 The etiology for CPT is not completely clear at present, although, there is a strong association between CPT and neurofibromatosis type I (NF-I). 6 Some scholars speculate that the periosteum plays an important role in the development of this disease, as they found that, the periosteum of the affected tibia was thickened, relatively avascular, constrictive, and adherent to the tibia and fibula, which may lead to an attritional loss of bone and increase the risk of fracture.7,8 Histological studies also have revealed hyperplasia of fibroblasts 9 and increased osteoclastic activity 10 in the periosteum of children with CPT.
Generally, the tibias of CPT patients correspond to the Types I to III in the Crawford 11 classification or Types I to IV in the Paley 12 classification and have at birth the following characteristics: (1) Complete tibia with continuous cortex and obvious anterolateral bowing, without pseudarthrosis, with or without NF-1, with or without cystic lesions; (2) no fractures at birth; (3) the lower extremity’s function is normal without neurodevelopmental disorder.
Due to the natural history of the disease, the body mass or/and the axis deviation transcend the limit of mechanical stress the dysplastic tibia can take so that a fracture in childhood is unavoidable. 13 Thus, prevention of fractures and subsequent pseudarthrosis is a worthy management goal for children in this stage. Once diagnosed, bracing is the primary intervention of choice for most orthopedic surgeons in order to protect patients from or delay the onset of fractures. 1 However, bracing alone does not provide satisfactory results, and many children are still unable to avoid fractures while using an orthosis. 4
Surgical options for delaying or reducing the risk of fractures mainly include corrective osteotomy or curettage, 14 bypass bone-grafting,4,15 and guided growth. 16 Among them is bypass bone-grafting, which was first reported by McFarland 15 in the 1950s, as a treatment option before fractures in order to obtain a normal mechanical axis and relieve the apex of the abnormal tibia, therefore, reducing tensile loads on the convexity and protecting the tibia from a fracture. More recently, in 2008, Ofluoglu et al. 4 performed the modified McFarland procedure (MMP) of placing an allograft fibula at the site of the concavity in the tibia in combination with long-term bracing to treat CPT and achieved favorable results. Our site also started to use the allograft bypass technique combined with long-term bracing to treat CPT children in 2009. Based on these, we propose the hypotheses that the MMP can avoid fracture and even has the effect of correction to the involved tibia in CPT patients.
To verify our hypotheses, in this report, we analyzed the midterm results of using the MMP in treating CPT patients of Crawford Type I and II and compared it to the results in the literature.
Patients and methods
Study design
We retrospectively reviewed seven CPT patients of Crawford Type I and II, who were treated with the allograft bypass technique (i.e. the MMP) at our hospital’s pediatric orthopedic department between 2009 and 2018 (Figure 1). The same senior surgeon performed the operation on all seven patients.
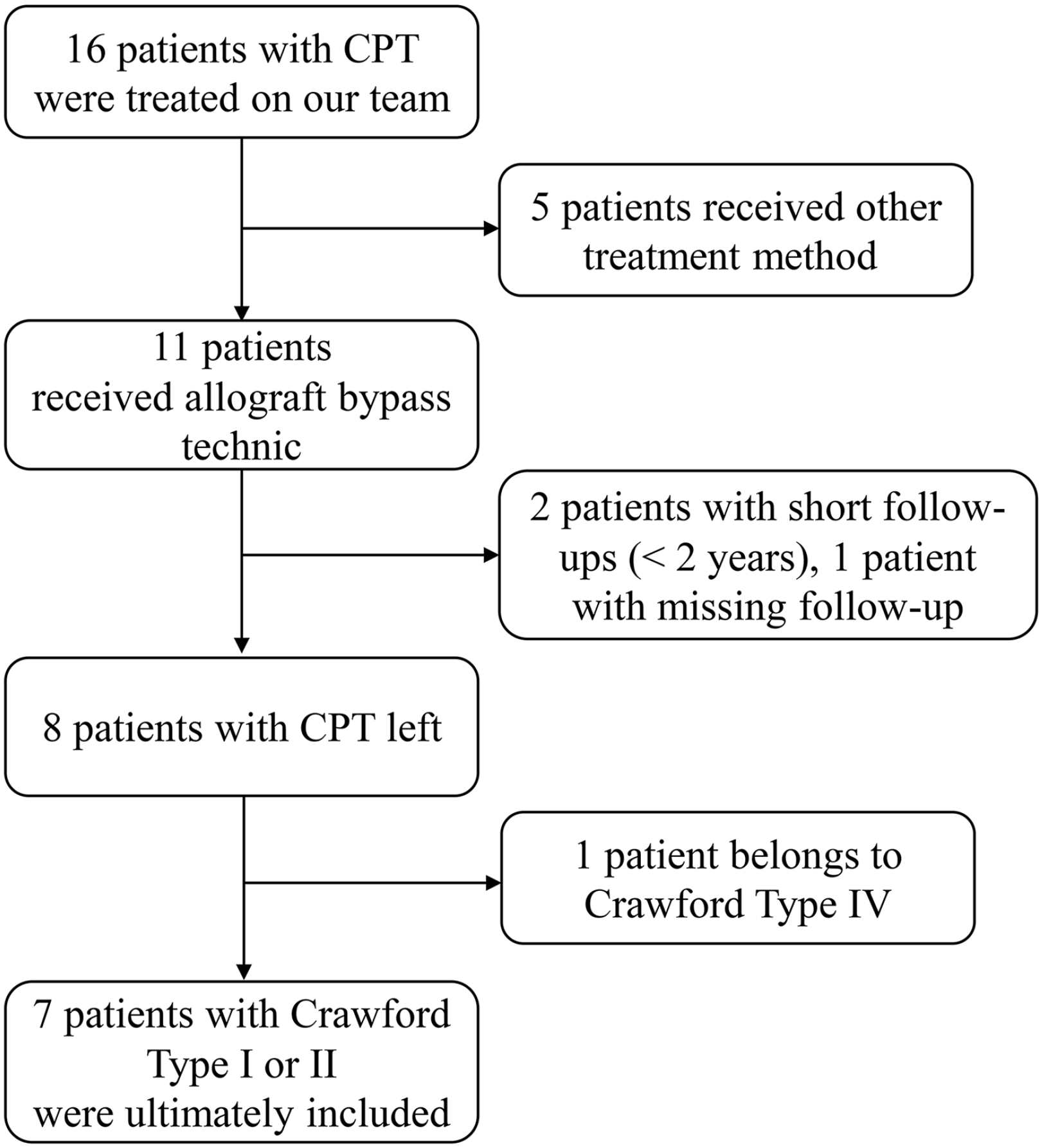
Patients flow chart.
The charts were reviewed according to following demographic information: age at the time of the first operation in our institute, diagnosis of NF-1, surgical procedure, adjuvant therapy, follow-up time, clinical findings, other procedures and complications. Anteroposterior and lateral radiographs of the tibia at the time of preoperative, postoperative, and last follow-up were reviewed as well, to evaluate the outcome.
The Crawford 11 classification, which is the one most frequently consulted, was used in this study to describe the type of tibial pseudarthrosis. It consists of four types: Type I: anterolateral bowing with an increase in cortical density, Type II: anterolateral bowing with sclerotic narrow medulla, Type III: anterolateral bowing with cysts or signs of a pre-fracture, and Type IV: anterolateral bowing with full-blown pseudoarthrosis.
Surgical technique and postoperative management
All operations were performed without the use of a tourniquet, taking the anteromedial approach, incising the skin and subcutaneous tissues.4,15 The periosteum was incised at the medial border and striped along the whole tibia, ending 1 cm from the proximal and distal physis. The abnormal periosteum and fibrous hamartoma were removed and only the normal periosteum was preserved. At approximately 2-cm distance from each physis, a 1-cm notch was created in the metaphysis. The fresh fibular allograft (obtained from the bone bank) was formed by the saw, approximately 2-cm longer than the length between the notches, to be able to insert a regular press fit and “bypassing” the dysplastic tibia. Then, the proximal end of the allograft was shaped into a spike in order to make a deep impact on the proximal tibial metaphyseal notch. Furthermore, the allograft was punched in preparation for the subsequent fixation. Finally, the tibia was stretched to obtain a satisfactory position and heavy sutures fixed both sides of the allograft. In our study, due to case 1 suffered a secondary fracture with tibial instability before treated in our institution, we replaced the heavy sutures with screws for fixation.
After the surgery, the operated limb was supported with an above-the-knee plaster, with the knee joint in an approximately 20–30° flexion, to avoid weight bearing until bone graft-tibia junctions showed consolidation on the X-ray. The median duration of plaster use was 10 weeks (8–12 weeks). After that, the patient changed to a patellar tendon-bearing brace until skeletal maturity. All patients were allowed to participate in regular exercise under the protection of the brace. The whole treatment algorithm of our cases was presented in Figure 2.
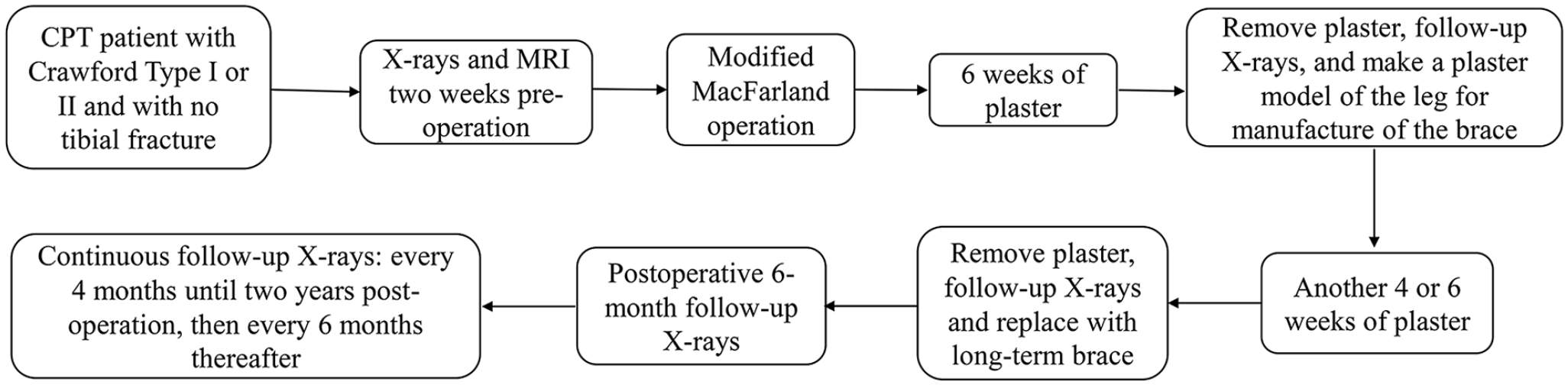
Treatment algorithm.
Radiographic measurements
According to standard deformity analysis, the medial proximal tibial angle (MPTA), lateral distal tibia angle (LDTA), anterior distal tibia angle (ADTA), and posterior proximal tibial angle (PPTA) were measured on preoperative and last follow-up X-rays (Figure 3(a)). Meanwhile, the anatomic tibia diaphyseal alignment was measured on anteroposterior and lateral views to evaluate the angulation and direction of the coronal and sagittal tibia diaphyseal. In addition, bilateral leg lengths were physically examined by measuring from the anterior superior iliac spine (ASIS) to the medial malleolus at the time of the last follow-up to calculate LLD. 17
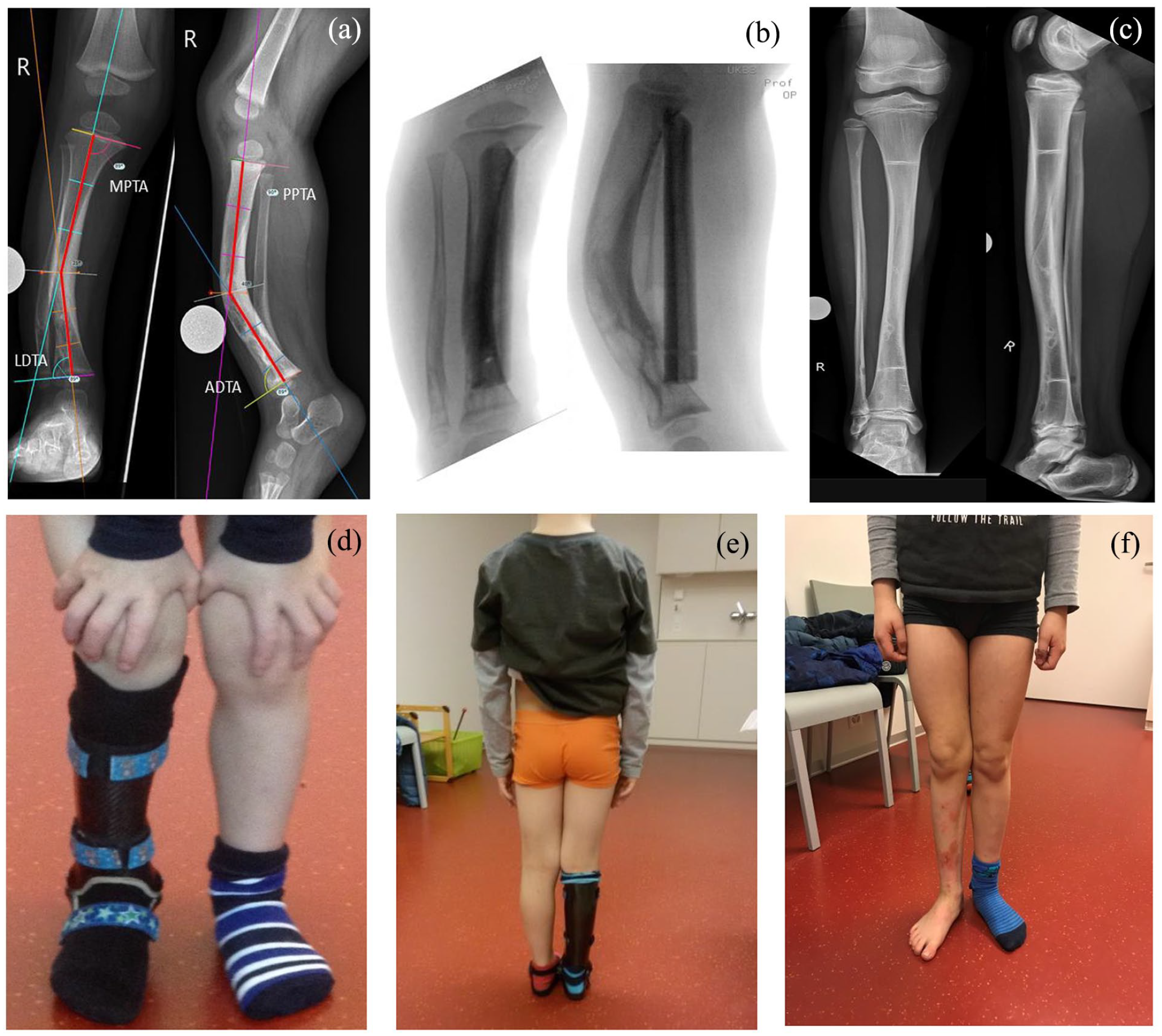
Illustrations of deformities, alignment, MPTA, LDTA, PPTA, and ADTA on the coronal and sagittal plane (Case 2). (a) Preoperative coronal and sagittal planes, (b) intraoperative X-rays, (c) 10 years postoperative X-rays, (d) 2 years postoperative follow-up, (e) 6 years postoperative follow-up, and (f) 10 years postoperative follow-up.
Literature review
A literature search was performed to detect studies on the surgical treatment of CPT using the McFarland bypass technique. Two reviewers searched the electronic PubMed and Web of Science databases using “pseudarthrosis” and “tibia” terms combined with the following terms: “Bypass” or “McFarland.” In addition, the two same reviewers conducted additional searches on Google Scholar using “pseudarthrosis,” “tibia,” “Bypass,” and “McFarland” terms. The bypass relative cases should count more than 2 if the study was a case series report containing multiple treatment modalities. Case reports, review articles, meta-analyses, articles not in English, articles without full-text, and books were excluded. The MINORS criteria were used to rate the included literature. The literature search flow chart was shown in Figure 4.
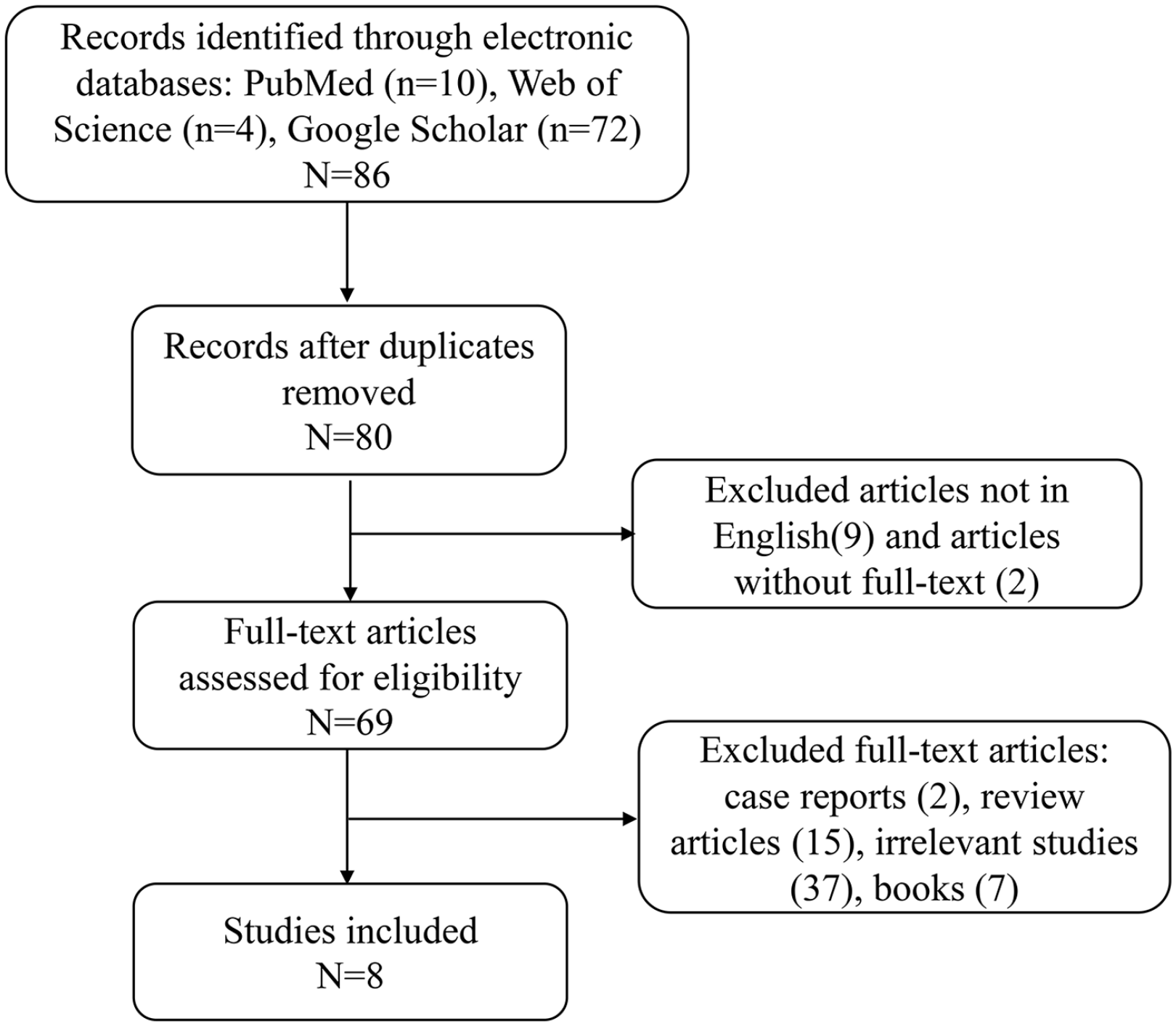
Literature research flow chart.
Statistical analysis
Demographic data and radiographic results were analyzed by descriptive statistics. The radiographic measurements were performed by TraumaCAD (BrainLAB, Munich, Germany). The graphs were created with GraphPad Prism (Version 9.0, San Diego, California, USA).
Results
A total of seven patients with CPT were treated with the allograft bypass technique at a median age of 2.2 years (range: 1.6–8.2 years). In this cohort, there were six boys and one girl, and three of them (cases 1, 3, and 7) had an underlying diagnosis of NF-1. Prior to the referral to our institution, one patient (case 1) with Crawford Type I tibia had undergone osteotomy, fixed by an intramedullary (IM) nail when she was 4 years old in another hospital. At the age of 5, she suffered a secondary fracture and gradually developed a tibial pseudarthrosis. The other six patients had not undergone surgery beforehand. At the initiation of treatment, five cases were Crawford Type I and two cases were Crawford Type II. The median follow-up period was 7.0 years (range 3.8–10.0 years). At the time of the last follow-up, none of them had reached skeletal maturity. The demographic data of all CPT patients are shown in Table 1.
Overall clinic demographic data of CPT patients.
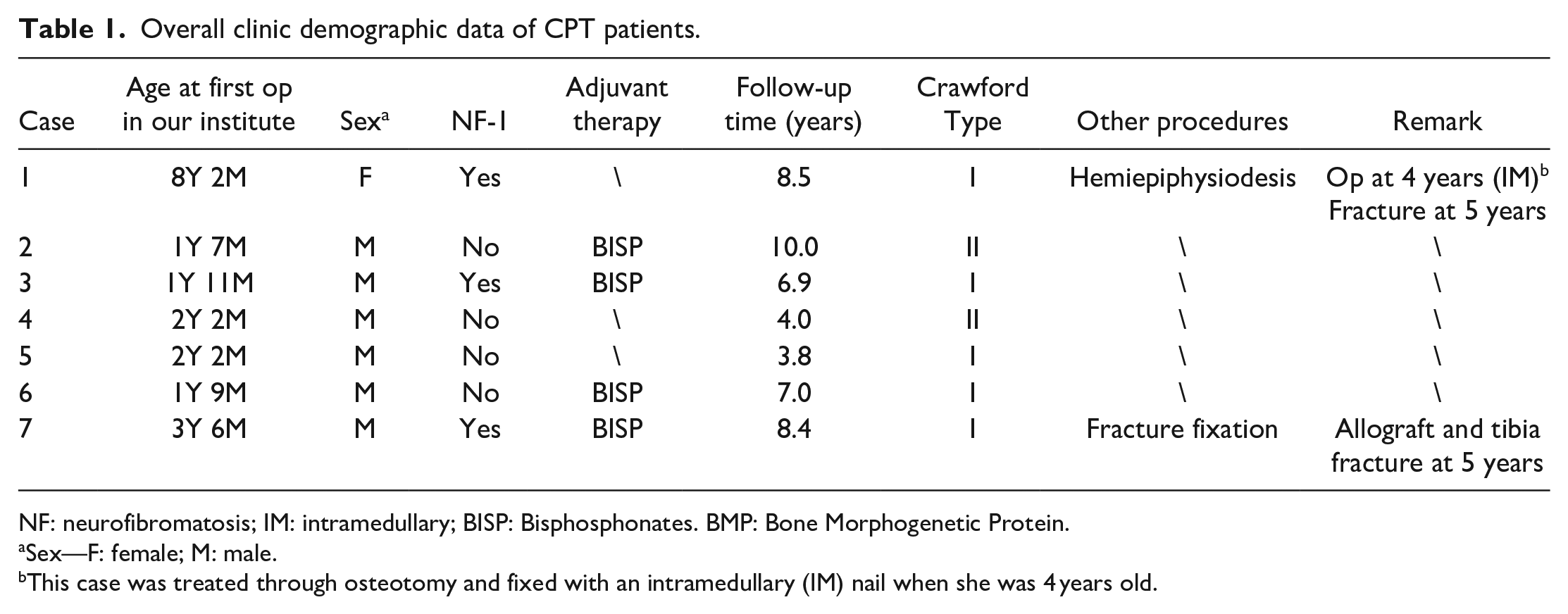
NF: neurofibromatosis; IM: intramedullary; BISP: Bisphosphonates. BMP: Bone Morphogenetic Protein.
Sex—F: female; M: male.
This case was treated through osteotomy and fixed with an intramedullary (IM) nail when she was 4 years old.
Consolidation and union
At the time of the last follow-up, all bypass allografts revealed union at both ends of the tibia. No pseudarthrosis developed in any of the patients. The median union initiated at 4 months (range: 2.5–6.8 months) after the surgery. Notably, case 7 suffered tibia and allograft fractures 1.5 years postoperatively. This patient then underwent a second operation totally resecting the fractured tibia and allograft to reconstruct the allograft and fix it with plates, which healed after 10 months. Three of our cases were shown in Figures 3, 5, and 6.
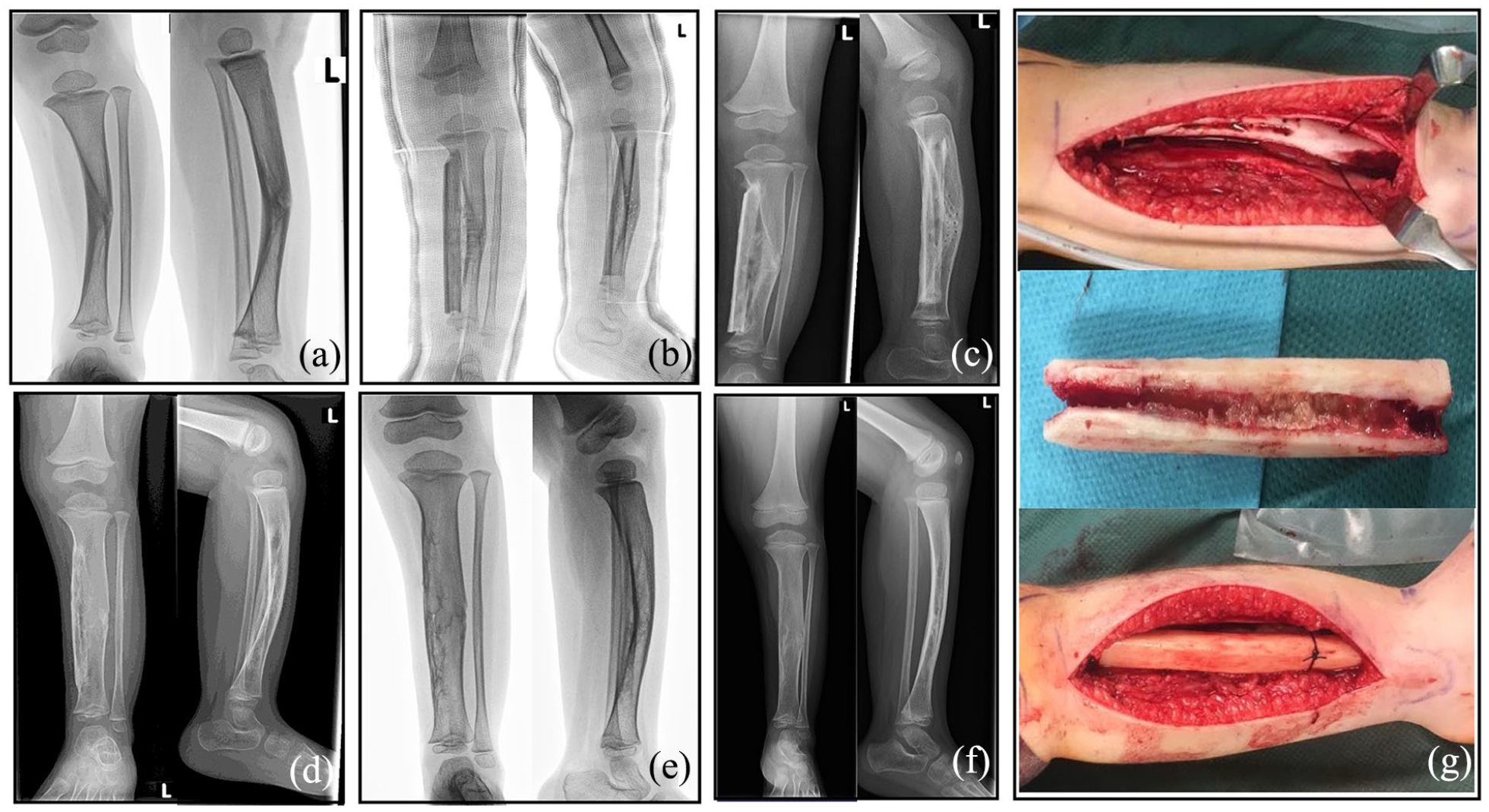
Serial radiographs and intraoperative images of case 5. (a) Preoperative X-rays, (b) 1 week postoperative X-rays (with the cast), (c) 3 months postoperative X-rays, (d) 1 year postoperative X-rays, (e) 2 years postoperative X-rays, (f) last follow-up (3.8 years postoperative) X-rays, and (g) intraoperative images.
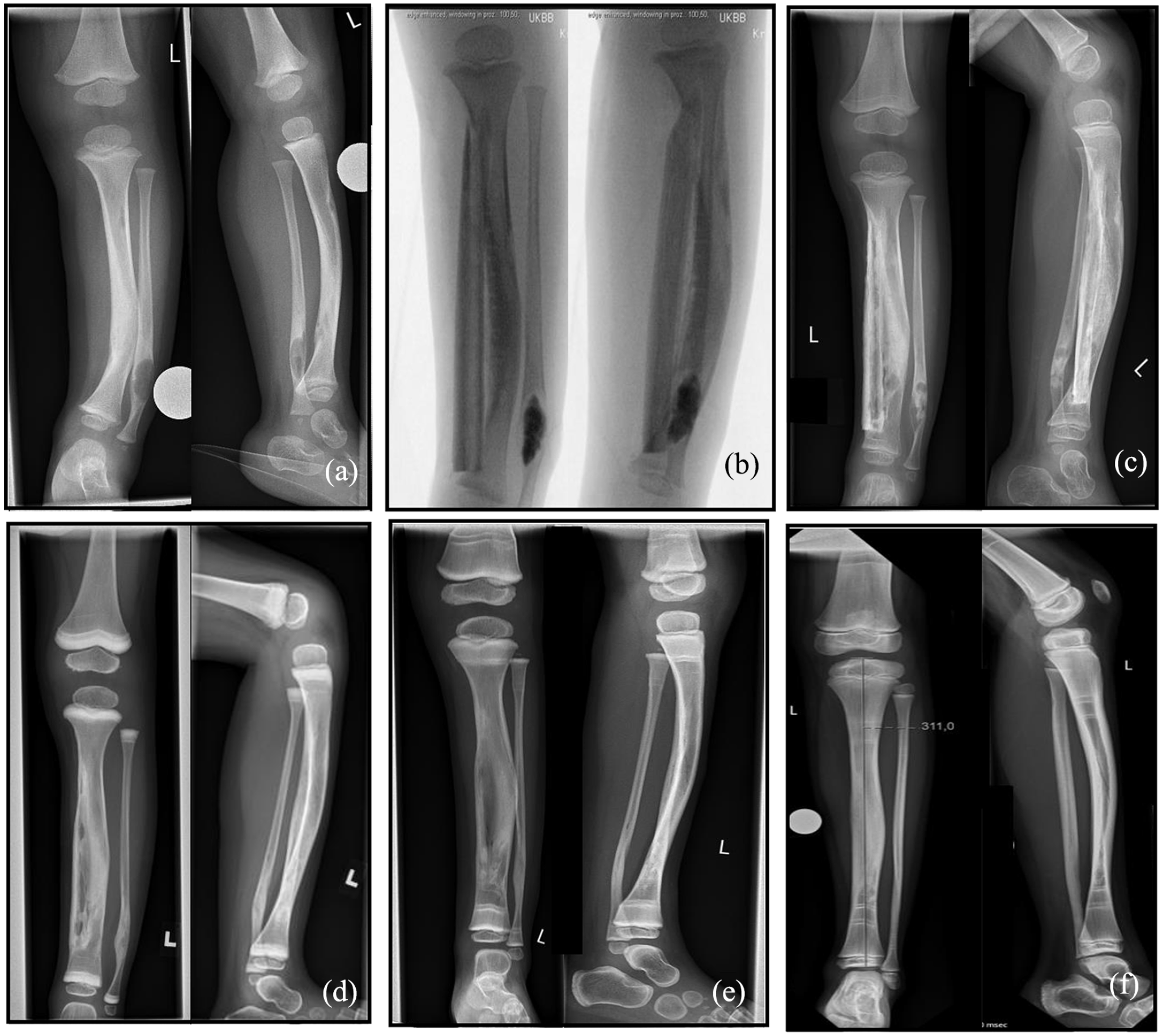
Serial radiographs of case 6. (a) Preoperative X-rays, (b) intraoperative X-rays, (c) 3 months postoperative X-rays, (d) 1 year postoperative X-rays, (e) 2 years postoperative X-rays, and (f) last follow-up (7 years postoperative) X-rays.
Radiographic outcomes of tibia deformity and alignment
Tibial deformity and alignment had improved in all patients at the time of the last follow-up. In the coronal plane, the angulation deformities were corrected in all but 1 patient, with a median of a 18.5° (range: 10°–23°) improvement (Table 2, Figure 7(a)). Case 1 had an increased valgus from 3° to 11° due to the intramedullary nail from the patient’s initial surgery, which was retained in the tibia to maintain the alignment before the bypass operation. Although a marked varus (>10°) was also observed in case 7 at the last follow-up, this was obtained by improvement of the preoperative 28° varus. In the sagittal plane, all patients had a median of a 24° (range: 12°–60°) procurvatum prior to the bypass operation, and all angulation deformities were corrected, with a median of 12° (range: 3°–50°) improvement (Table 2, Figure 7(b)).
Radiographic outcome of Tibia deformity at the last follow-up.
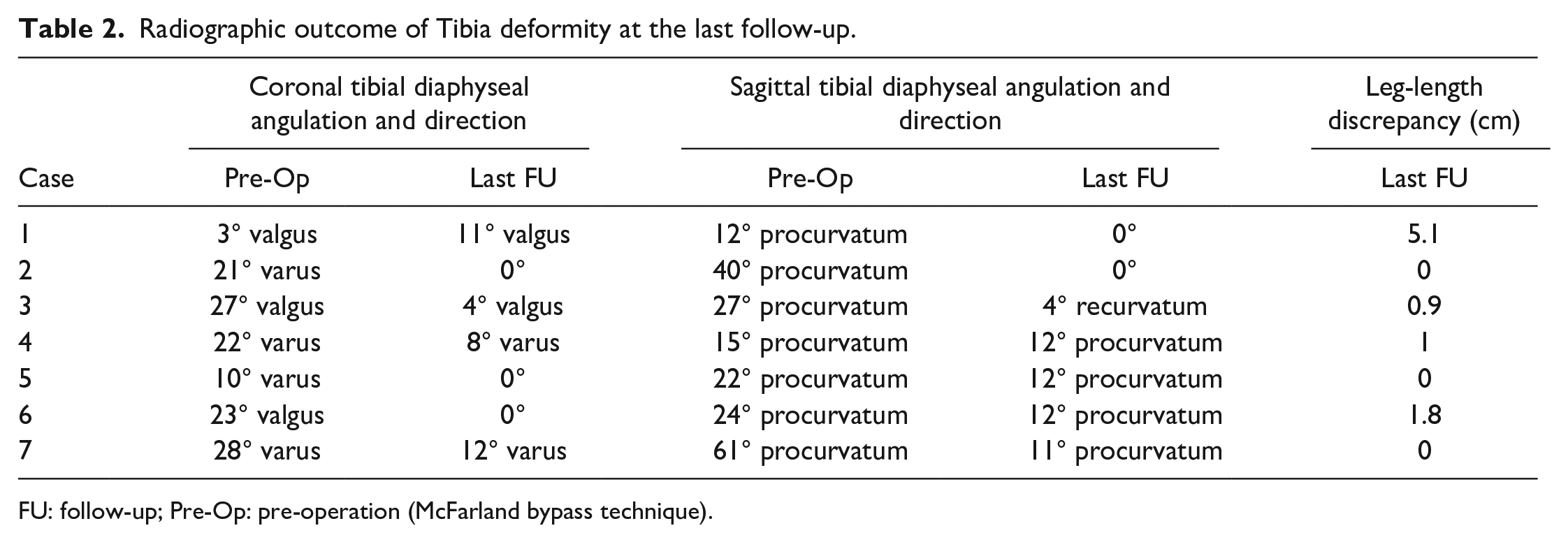
FU: follow-up; Pre-Op: pre-operation (McFarland bypass technique).
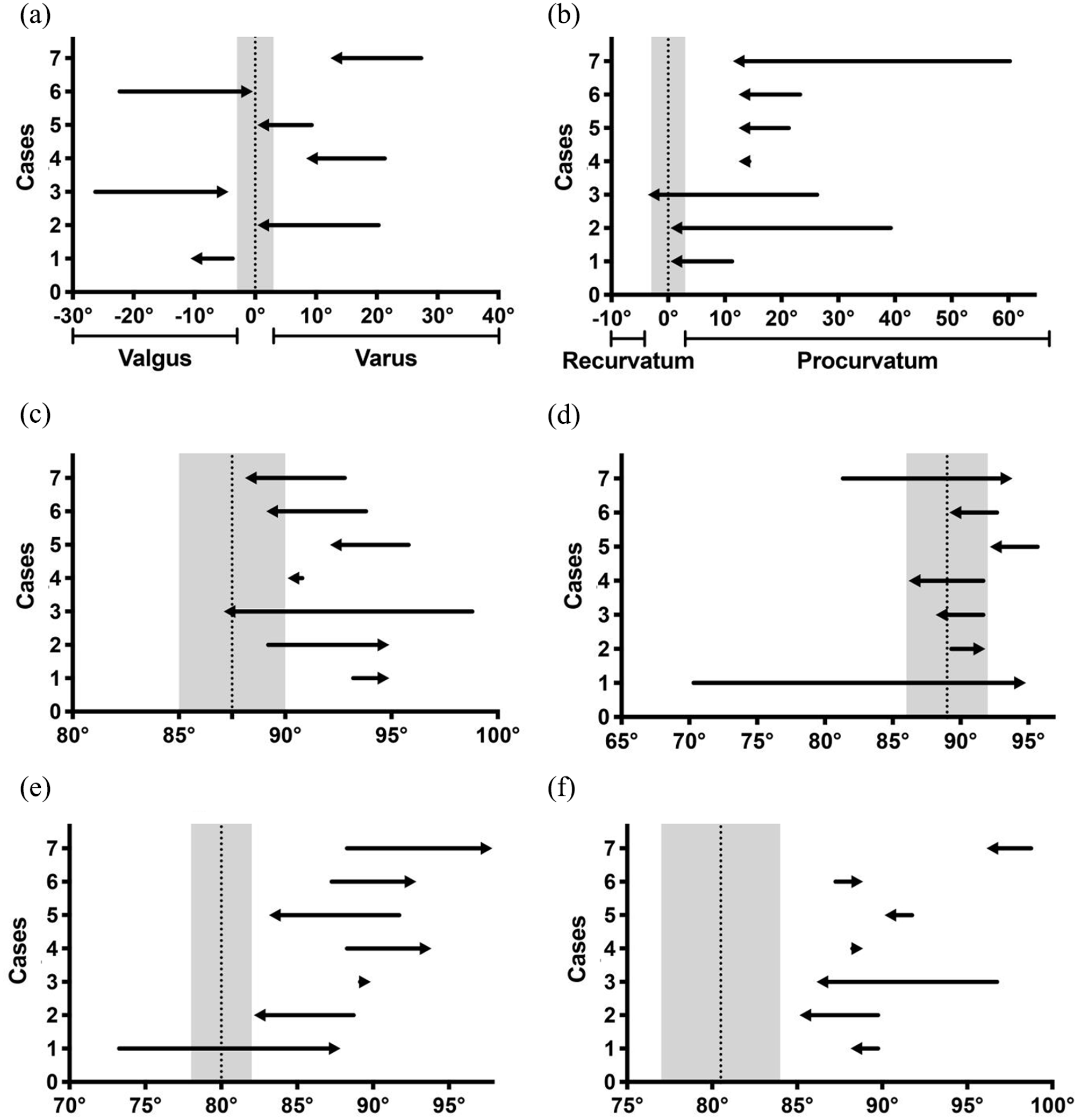
Changes in radiographic measurements of tibial deformity and alignment. (a) Coronal tibial diaphyseal angulation and direction, (b) sagittal tibial diaphyseal angulation and direction, (c) MPTA on coronal plane, (d) LDTA on coronal plane, (e) ADTA on sagittal plane, and (f) PPTA on sagittal plane.
In addition, the other two coronal indicators also improved in most cases. MPTA returned to the normal zone (gray zone in Figure 7) in three of the seven cases and converged to the normal zone in another two cases (Table 3, Figure 7(c)). LDTA returned to the normal range in four of the seven cases and approached normal values in the other three cases (Table 3, Figure 7(d)). However, individual changes were shown for the other two sagittal indicators (ADTA and PPTA), and both of them in all cases were still abnormal at the time of the last follow-up (Table 3, Figure 7(e) and (f)).
Radiographic outcome of MPTA, LDTA, ADTA, and PPTA at the last follow-up.
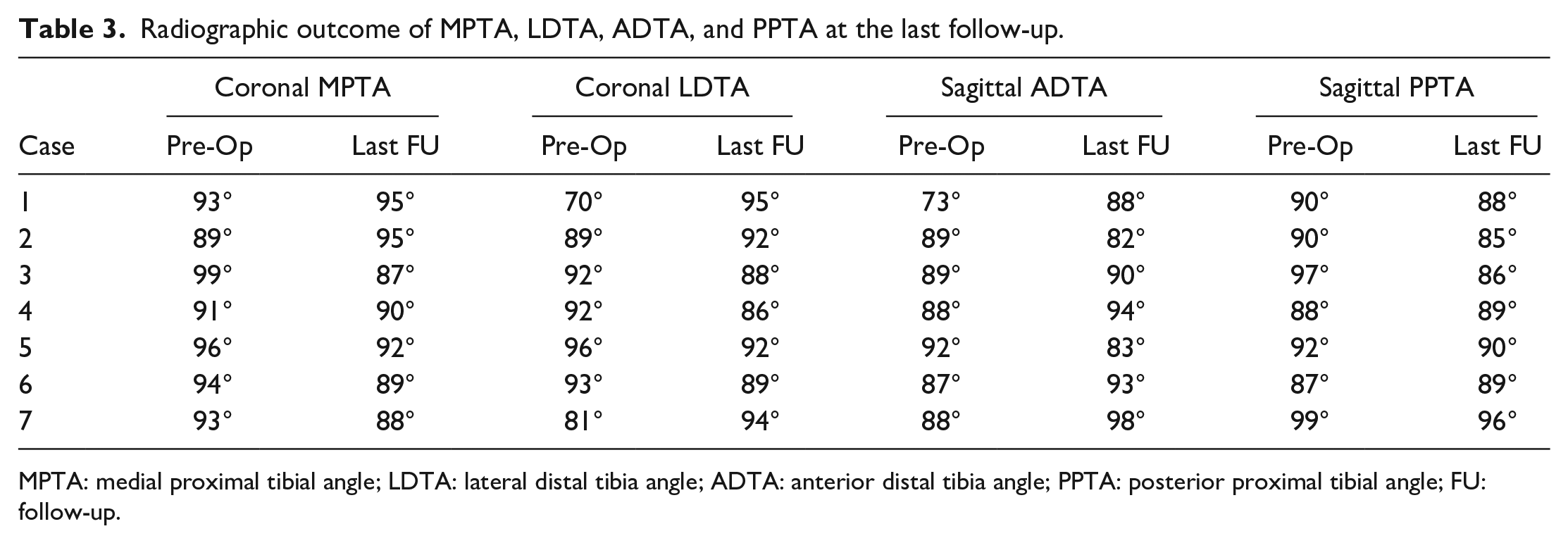
MPTA: medial proximal tibial angle; LDTA: lateral distal tibia angle; ADTA: anterior distal tibia angle; PPTA: posterior proximal tibial angle; FU: follow-up.
Moreover, at the time of the last follow-up, measurable LLD was found in four of the seven patients. Three patients had less than 2 cm of discrepancy, and only case 1 measured a 5.1-cm LLD (Table 2).
Functional outcomes and complications
All seven cases were asked to wear the patellar, tendon-bearing brace in daily life until they achieve skeletal maturity. Protected by the brace, all seven patients can fully bear weight, walk, jump, run, and regularly exercise without using any other aids such as crutches, canes, or wheelchairs. No patient reported any pain and restriction of the knee or ankle caused by tibial deformity.
One patient (case 7) suffered a traumatic, low-energy, non-displaced tibia and allograft fracture postoperatively, which healed after the second procedure we mentioned above. Another patient (case 1) with progressive knee valgus deformity and an obvious LLD after the operation was treated with a proximal tibia hemiepiphysiodesis. By the time of the last follow-up, case 1 still had an 11° valgus deformity and a 5.1-cm LLD.
Literature
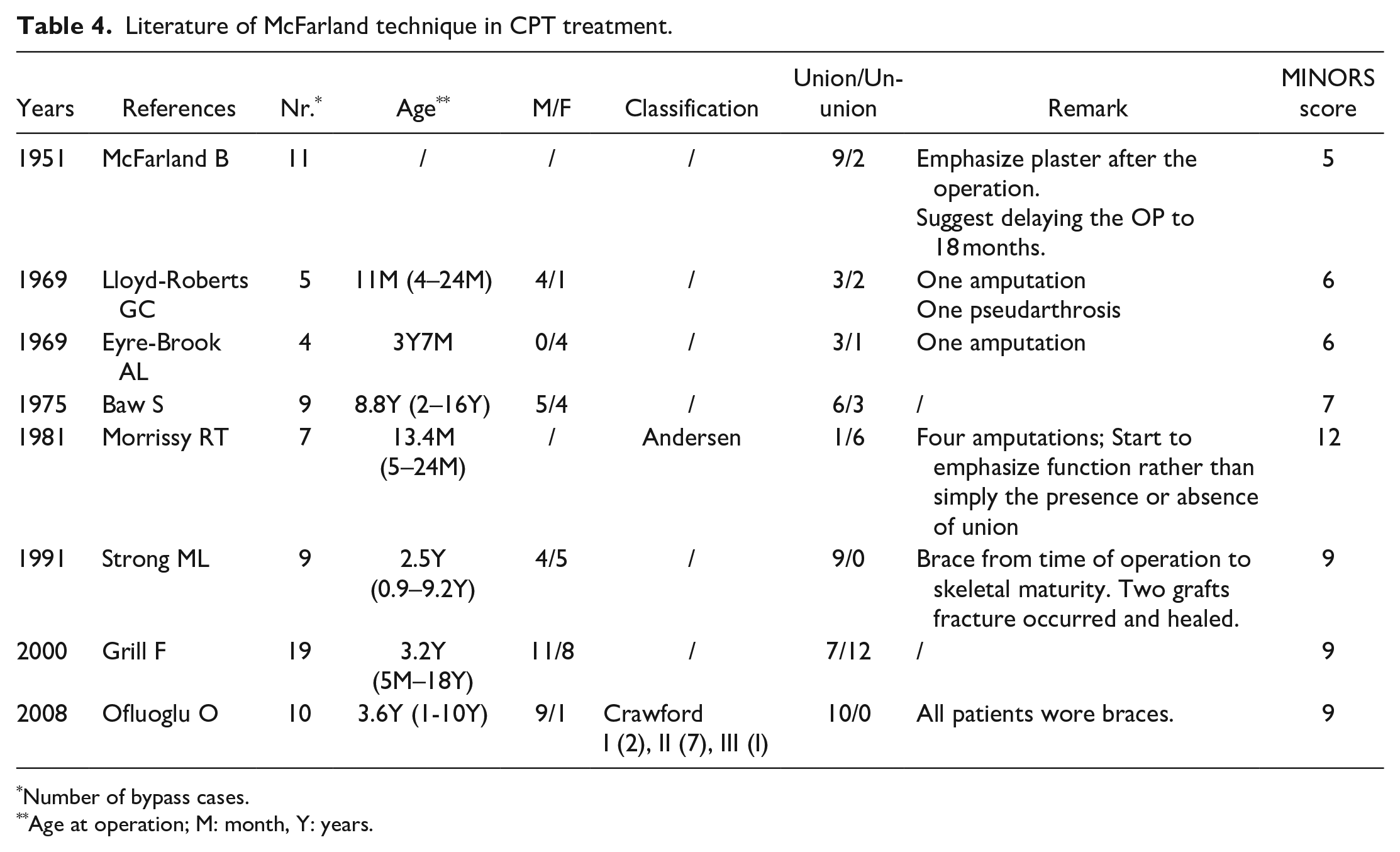
After screening out duplicates, a total of 80 papers have been retrieved, of which 61 were excluded because they were either unrelated to our study or article type did not meet the requirements. Nine were excluded as they were not available in English, and two were excluded without full-text. We ultimately included eight studies with a total of 81 CPT patients treated with the McFarland bypass method (Table 4). These studies reported varying rates of tibial union. The study of Morrissy et al. 18 reported the lowest union rate (14.3%). Only one of the seven patients had a healed tibia, and four patients eventually underwent amputation. However, studies conducted by Strong and Wong-Chung 19 and Ofluoglu et al., 4 respectively, achieved a 100% union rate (nine in nine and 10 in 10). Overall, 59.3% (48 in 81) cases were reported to have a healed tibia, and six cases were reported to have undergone amputation (Table 4).
Literature of McFarland technique in CPT treatment.
Number of bypass cases.
Age at operation; M: month, Y: years.
Discussion
CPT is a rare malformation and has a variety of clinical manifestations, ranging from simple anterolateral bowing to complete non-union with extensive bone defects of the tibia. The incidence of CPT is currently reported between 1:60,000 and 1:250,000. 2 Although several surgical approaches (e.g. cross-union, intramedullary fixation, external fixation, free vascularized fibular grafting, and amputation) are now available for the treatment of CPT and have shown significant improvements in treatment outcomes, many challenging problems remain, including non-union, re-fracture, LLD, and malalignment of the tibia and ankle.12,20 Moreover, an early fracture of the dysplastic tibia is one of the better-known risk factors for a poorer outcome in CPT patients. 21 Therefore, fracture prevention in the pre-fracture stage of CPT patients is important to avoid the occurrence of pseudarthrosis and obtain a better prognosis.
To our knowledge, there currently is no consensus on the optimal technique for the treatment of CPT. The most common treatment strategy used to date to prevent fracture and initiation of pseudoarthrosis has been the use of braces. However, as we mentioned above, the use of braces alone does not provide favorable outcomes. The McFarland procedure is an old surgical approach to prevent CPT from developing into pseudoarthrosis. However, there are only a few high-quality articles reporting the outcome of the McFarland technique (Table 4). McFarland performed his first graft to treat CPT in 1931 and first reported on it in 1951. In these 11 cases, 9 were thought to be successfully achieved unions. At the same time, he also clarified that the cause of CPT is a mechanical reason, emphasizing the use of plaster after the operation and suggesting delaying the operation to 18 months of age. 15 After that, Lloyd-Roberts and Shaw, 22 Eyre-Brook et al., 23 and Baw 24 respectively reported 18 cases treated with the McFarland method with a total of 12 unions in tibias and two amputations. In 1981, Morrissy et al. 18 reported a series of total 40 cases, of which 7 underwent prophylactic bypass grafting. Thereby, only one case yielded a good result and four resulted in amputation. In this study, the function rather than simply the presence or absence of union gained emphasis, nonetheless, there still was a lack of attention on bracing and casting. Since the 1990s, the union rate of the McFarland technique increased, especially in single-center reports. Strong and Wong-Chung 19 reported nine cases wearing braces from the time after the operation to skeletal maturity, and Ofluoglu et al. 4 presented 10 cases wearing braces as well, all of which healed well. In our center, we analyzed seven patients with CPT who were treated with bypass allograft stabilization, including an allogenic fibula grafting in combination with planned long-term bracing. All seven of our patients healed as well. When including our study, all 26 cases reported by single-center studies within the last 30 years healed without pseudarthrosis.
Although the bypass treatment demonstrated satisfactory healing rates in recent studies, residual deformities persisted. In our study, we measured the coronal tibial diaphyseal angulation, sagittal tibial diaphyseal angulation, MPTA, LDTA, ADTA, and PPTA (Tables 2 and 3, and Figure 7). All coronal plane measurements (angulation, MPTA, and LDTA) and sagittal tibial diaphyseal angulation are trending toward the normal range (gray zone in Figure 7). However, sagittal ADTA and PPTA showed no significant regular variation in measurements and were abnormal in all patients at the time of the last follow-up. The study by Ofluoglu et al. 4 also found that most patients had considerable residual deformity at the time of the last follow-up: the mean coronal diaphyseal angulation was 25.7° and sagittal diaphyseal angulation was 27.5°. Laine et al. 5 reported on the same observation, although, they used the guided growth method to treat CPT, they also found residual deformities with diaphyseal angulation of 4.1° in the coronal plane and 9.1° in the sagittal plane. Notably, it appears that the coronal deformity was more successfully corrected than the sagittal deformity, although, an improvement was seen in the alignment in all cases of these studies. Therefore, the improvement of the sagittal deformity in the treatment of CPT requires more attention from pediatric orthopedic surgeons.
Guided growth, which was first reported by Kennedy et al. 16 in 2017 as a one case report, is another surgical approach to treatment options for CPT. And recently, Laine et al. 5 reported a 10-CPT-case series treating the disease with distal tibial growth modulation using an eight-Plate, to delay or prevent fractures. Although, residual deformities persisted as mentioned above, none of these 10 cases developed a tibial fracture or pseudarthrosis after the initiation of guided growth treatment. In addition, significant LLD was observed in only one case in our study, which is similar to the result of Laine et al., and contrary to the results observed with other treatment methods.1, 28 This supports the interpretation of Laine et al. 5 who contend that LLD is not an inherent risk of CPT but may be iatrogenic or secondary. All these results strengthen our confidence to manage CPT treatment by preventing fracture, decreasing tibial malalignment, improving radiographic appearance of bone quality, and preserving leg length.
Cross-union is also a surgical procedure that has developed in recent years. Choi et al. and Paley independently published their methods of treating patients with CPT in 2011 and 2012, respectively, with the intention of creating a cross-union between the tibia and fibula.25,26 Although there are some differences in their approaches, in a series of studies using the cross-union method, 100% union rates without refractures have been reported.12,26 This is an encouraging result. More importantly, the cross-union procedure proposed by Paley can be used for all types of CPT patients. In our study, although union was achieved in all cases and no pseudoarthrosis was formed, the MMP technique we used was limited to patients with Crawford Type I and II.
In addition to above, there are several other approaches for CPT that deserve to be mentioned. Intramedullary rod (IMR) fixation has been widely used. The advantage of IMR is that it can remain until bone maturity, maintain alignment and prevent re-fractures that may occur years after union. However, IMR is often associated with complications such as unstable fixation, ankle stiffness and LLD. 27 Furthermore, children with fixed nails (non-retractable) will need to undergo multiple surgeries as they grow. In terms of patient outcomes, a published systematic review concluded that the mean primary union rate in series using IMR was 67.7% and there was high non-union (17%) and refracture rate (48.1%). 28 The Ilizarov external fixator, which was proposed in the early 1970s, is capable of producing rigid and controlled fixation for compression, distraction, bone transport to the resection defect, lengthening, deformity correction, and union. 29 The overall union rate for the Ilizarov method in literature ranges from 60%–100%.1,30 Refractures rates have also been reported to be high (more than 32%), 31 even to the extent that in one study, refractures were inevitable in almost all patients. 32 Vascularized fibular graft (VFG), which uses either the contralateral or homolateral fibula, is similar to the MMP and has the advantage of a single-stage procedure and good patient compliance. Nevertheless, patients face complications, especially on the donor side, such as sensory or motor weakness and valgus ankle deformity. 33 Whereas, in our study, there was no need to worry about these risks because of the use of allograft and no donor area. Amputation is also still an option, but only for selected patients with failed reconstruction, severe LLD, severe leg and ankle deformities, and those who have a strong desire not to undergo reconstruction and voluntarily request amputation.
The timing of surgical treatment remains controversial. The European Paediatric Orthopaedic Society (EPOS) study recommended surgery after 3 years of age and believed that surgery after six years of age elicits better results. 30 However, some authors suggest operating before the age of 3 to achieve a stable and functional limb early and maintain maximal residual growth of the tibia. 34 In our cohort, five of the seven patients were under the age of 3 at the time of the bypass treatment. All of them achieved healing with improved deformity and alignment of the tibia. Two other patients in our cohort who were older than 3 years of age also healed, but one had a significant LLD and knee valgus deformity at the time of the last follow-up, and the other suffered a fracture and underwent a second surgery after the initial procedure. Our results suggest that prophylactic surgery treatment with the bypass allograft method in CPT patients under 3 years of age who are in the pre-fracture stage can achieve satisfactory midterm outcomes. However, due to the rarity of the disease and the small number of cases, we were unable to statistically analyze whether there was a significant difference in treatment outcome between children over or under 3 years of age.
In our study, we also administered bisphosphonate adjuvant therapy to four of these patients (cases 2, 3, 6, and 7). This is because compared to normal periosteum, CPT periosteum is characterized by an increased osteoclastic activity and decreased osteoblastic activity, which is associated with healing failure and bone graft resorption. 10 Bisphosphonate is recommended to supplement surgery for CPT because of its anti-osteoclastic activity, which may play a role in preventing bone resorption. 35 Schindeler et al. 36 also demonstrated in the mice model that the use of bisphosphonate led to a synergistic increase in the amount of heterotopic bone in both NF1+/+ and NF1+/− mice. Although, we attempted to use bisphosphonate adjuvantly in the treatment of bypass prophylactic surgery in CPT, we did not use it in all of our cases, which would have introduced bias, and due to the scarcity and heterogeneity of patients, we did not have an ideal control group for comparison, and therefore, we cannot confirm the exact role of bisphosphonate in our treatment.
In addition, we reiterate and support the view of Morrissy et al. 18 that the function rather than merely the presence or absence of union should be emphasized. The goal of the treatment is to obtain a straight, stable, healed, and unencumbered tibia by the time of skeletal maturity, with as few surgical procedures as possible. The function of the limb should not restrict patient activity in childhood or adolescence. Therefore, we must critically evaluate patient-related outcomes with CPT. The definition of a good outcome must include outcomes that are functionally relevant to the patient and not simply a radiological consolidation. In our study, all children wore braces before and after the CPT operation to prevent fractures, allowing them to engage in physical activities without restriction.
Furthermore, it should be clarified that the indication for this procedure at our center is for Crawford Type I and type II patients with intact tibia. Our results indicated that this procedure is most effective for the pre-fracture stage. Although we tried and succeeded with case 1, if a fracture has occurred or pseudoarthrosis has developed, it would be better to avoid this procedure.
There are several limitations in this study. First, none of our patients reached skeletal maturity at the last follow-up, so the clinical and radiographic outcomes were not collected up to the time of skeletal maturity. Furthermore, the small number and heterogeneity of the patients only allowed us to perform a descriptive analysis, without obtaining statistical results. Afterward, in our treatment, we used bisphosphonates in some cases and not in others, which increased the bias in our study. Finally, since we did not follow-up the contralateral limb with X-rays, we were unable to provide more detailed data on the contralateral limb.
Conclusions
The MMP technique in our series presented good midterm results in the pre-fracture stage CPT patients of Crawford Type I and II. Tibial deformity and alignment improved, and bypass allograft revealed union in all patients at the time of the last follow-up. No pseudarthrosis developed in any of the patients. All these results validated our hypothesis. This procedure combined with long-term bracing, which involves only the affected leg, can delay or possibly prevent fracture, decrease tibial malalignment, and preserve leg length with a low complication rate. A long-term follow-up until the time of skeletal maturity is necessary to further evaluate the results of this method.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241228168 – Supplemental material for Preventing of nonunion in congenital pseudarthrosis of the tibia cases of Crawford Type I and II through the use of allograft bypass and a brace: Midterm findings
Supplemental material, sj-pdf-1-cho-10.1177_18632521241228168 for Preventing of nonunion in congenital pseudarthrosis of the tibia cases of Crawford Type I and II through the use of allograft bypass and a brace: Midterm findings by Chao Dong, Chengxiang Li, Ute Brückner, Hermann Hellmich and Andreas H Krieg in Journal of Children’s Orthopaedics
Footnotes
Author contributions
A.H.K and C.D. have contributed to the study design and redacting of the manuscript. A.H.K., C.D., and C.L. have contributed to the data collection and manuscript preparation. C.L., U.B., and H.H. have contributed to the search for literature and data analysis. C.D. and C.L. are contributed equally to this work and should be considered co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the “Kiwani Club Klingenthal, Basel, Switzerland.” The sponsors neither had any influence on study design, the collection, analysis, and interpretation of data, the preparation of the manuscript, nor on the decision to submit the article for publication. The views expressed in this manuscript are exclusively those of the authors.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee Northwest and Central Switzerland (EKNZ Project ID. 2021-00186). As this was a retrospective review, no specific consent is needed for statistical analyses of aggregated deidentified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.