
Abstract
Purpose:
To evaluate differences in knee kinematic outcomes of patellar-lowering surgery, specifically patellar tendon advancement or patellar tendon shortening, compared with no-patellar-lowering surgery in multilevel surgery for children with cerebral palsy and crouch gait.
Methods:
Four databases were searched to retrieve studies published from inception until 2023. Three reviewers independently screened for studies with observational or randomized control designs, comparing two groups of patients with cerebral palsy and crouch gait who underwent multilevel surgery (with patellar-lowering surgery versus no-patellar-lowering surgery), where various gait analysis outcomes were reported (CRD42023450692). The risk of bias was assessed with the Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) tool.
Results:
Seven studies (249 patients and 368 limbs) met the eligibility criteria. Patients undergoing patellar-lowering surgery demonstrated statistically significant improvements in knee flexion at initial contact (mean difference = −6.39; 95% confidence interval = [−10.4, −2.75]; p = 0.0006; I2 = 84%), minimum knee flexion in stance (mean difference = −14.27; 95% confidence interval = [−18.31, −10.23]; p < 0.00001; I2 = 89%), and clinical knee flexion contracture (mean difference = −5.6; 95% confidence interval = [−9.59, −1.6]; p = 0.006; I2 = 95%), with a significant increase in anterior pelvic tilt (mean difference = 2.97; 95% confidence interval = [0.58, 5.36]; p = 0.01; I2 = 15%). However, improvements in gait deviation index and decrease in peak knee flexion in swing did not reach statistical significance. Subgroup analysis reduced heterogeneity and revealed (1) greater improvement using patellar tendon shortening versus patellar tendon advancement techniques; (2) lack of knee flexion contracture improvement in high-quality or longer-term studies; (3) longer-term improvement only in minimum knee flexion in stance, with a decrease in peak knee flexion in swing; and (4) an inability to assess the potential benefit of rectus femoris procedure and hamstring preservation.
Conclusions:
Overall, the combination of patellar-lowering surgery with multilevel surgery demonstrated superior improvements in stance-phase knee kinematics compared with multilevel surgery alone, despite an increase in anterior pelvic tilt and a longer-term knee flexion reduction during the swing phase.
Level of evidence:
Level III, Systematic review of level III studies.
Keywords
Introduction
Crouch gait is considered the most common gait pattern among the preadolescent population with bilateral spastic cerebral palsy (CP),1,2 which progressively challenges their autonomy.3 –5 This type of gait is characterized by persistent, excessive hip and knee flexion in the stance phase, often coupled with ankle dorsiflexion,3,6 and inability to fully extend the knee during terminal swing. Individuals with crouch gait also exhibit a steady increase in the internal knee extensor moment. 7
Multiple factors explain the onset and progression of crouch gait, 8 the most widely recognized causes being loss of adequate plantar flexion/knee extension (PF/KE) couple;9 –12 short and/or spastic hamstrings 13 and hip flexor muscles; 14 extensor mechanism insufficiency; 15 and lever arm dysfunction.11,16 Additional factors include muscle weakness17,18 and neurological, proprioceptive, and sensory impairments,10,19 among others. KE during gait depends primarily on functional hamstring length, knee extensor strength, passive ability to extend the knee, and a functional PF/KE couple. 20 The quadriceps muscle group, crucial for KE strength, plays a pivotal role during the early stance phase of normal gait. It resists the initial flexion force during weight acceptance, thus maintaining stability. 21 As the body’s momentum propels it forward over the stabilized tibia, the center of gravity shifts anteriorly to the knee joint, resulting in a passive extension of the knee. Notably, the quadriceps become relatively inactive by the midpoint of the stance phase. 21 When functioning optimally, the patella acts as a fulcrum, allowing the quadriceps tendon to exert force more efficiently when the knee extends. Patients who present crouch gait, in contrast, patellar tendon elongation, high-riding patella, and quadriceps insufficiency develop over time, hindering efficient KE during gait. In addition, patella alta increases patellofemoral joint stress 22 and produces pain. 23
While acknowledging the complex, multifactorial nature of crouch gait pathogenesis, an attempt should be made to treat as many of the existing causes as possible as part of a tailored approach. 20 Even for reducible deformities and in the absence of transverse or frontal plane abnormalities, nonsurgical treatments, such as physiotherapy and antigravity muscle strengthening,24,25 together with spasticity management and orthotic adjustment 26 seem insufficient.27,28 Among the surgical procedures used to correct crouch gait, distal hamstring lengthening (HSL) has traditionally been used to improve KE. Although the short-term results are acceptable,29 –31 the longer-term outcomes of this approach are compromised due to the lengthening of an already weak musculature, which also acts as a powerful hip extensor. 32 Moreover, hamstrings in crouch gait are often long or have adequate length, 33 even though functionally short and slow; therefore, HSL may be detrimental. 34 Aiming to achieve an upright posture, procedures such as distal femur extension osteotomy (DFEO) with or without shortening to correct the static knee flexion deformity,16,31,35 –37 combined with patellar-lowering surgery (PLS), whether using patellar tendon advancement (PTA)16,35 or patellar tendon shortening (PTS) techniques20,36,38 to improve dynamic quadriceps function and enhance KE, are solutions that preserve the power and propulsive function of biarticular muscles.39,40 These procedures should be performed in the context of multilevel surgery (MLS),40,41 with concomitant correction of alterations at other levels,16,42 to optimize muscle performance and restore the ground reaction forces in front of the knee, and thus reduce the demands on the quadriceps muscle and knee extensor mechanism. 20
Patellar lowering seeks to optimize patellar position within the trochlea and improve quadriceps leverage in an upright posture, thereby enabling the quadriceps to effectively extend the knee,43,44 (Figure 1), reducing the knee extensor lag. However, evidence on MLS outcome with PLS versus no-PLS in patients with bilateral spastic CP exhibiting crouch gait is limited,43,45 and the effect of these interventions on knee kinematics in stance and swing phase is unclear. In light of this gap in the knowledge base, we performed a systematic review and meta-analysis to quantitatively compare the knee kinematics during gait in patients with CP and crouch gait undergoing MLS, with or without PLS.
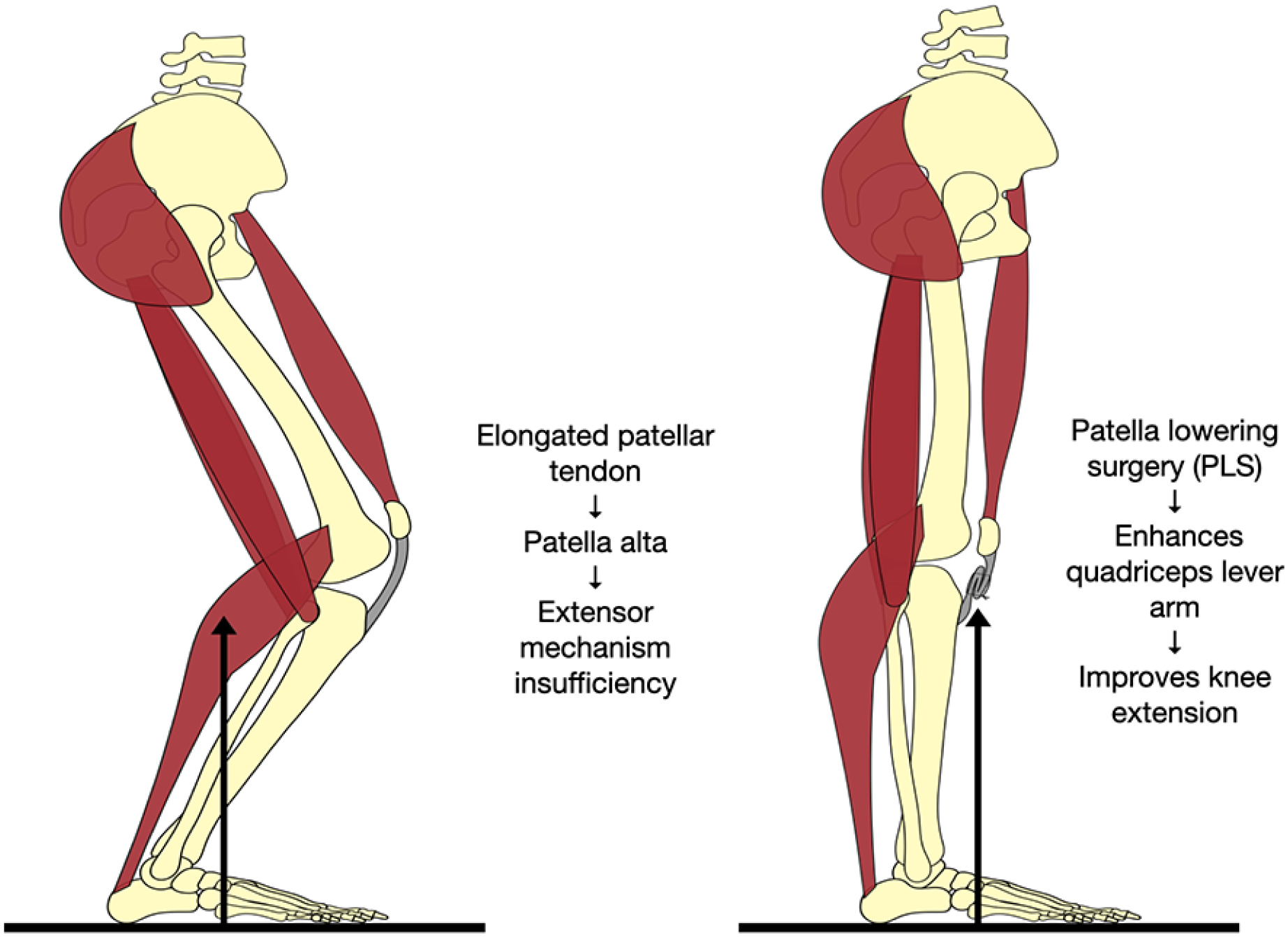
Graphical representation of the crouch gait pattern with extensor mechanism insufficiency due to an elongated patellar tendon and patella alta. In the context of multilevel surgery, this abnormality can be corrected with patellar-lowering surgery, which enhances quadriceps lever arm function and improves knee extension.
Methods
This systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines 46 and the latest Cochrane Handbook for Systematic Reviews of Interventions. 47 The PRISMA checklist can be found in Supplemental Table 1. The protocol followed was registered with and accepted by the International Prospective Register of Systematic Reviews (PROSPERO) on 1 August 2023 (CRD42023450692). Institutional review board approval and informed consent were not sought because the data were anonymous and publicly available.
Eligibility criteria
Inclusion in this meta-analysis was restricted to studies that met all the following criteria: (1) original studies with an observational or randomized control design; (2) enrolling patients with CP, as described by Bax et al., 48 and a crouch (flexed knee) gait; 6 (3) comparing PLS versus no-PLS in the setting of MLS; and (4) a mean follow-up of at least 1 year. In addition, studies were included only if they reported any of the outcomes of interest preoperatively and postoperatively for both groups. A minimum 1-year mean follow-up was chosen given the initial deterioration in function after MLS, followed by a return to baseline values 1 to 2 years later, with potential further improvements in the long term. 49
We excluded studies with (1) no control group and conference abstracts; (2) PLS surgery performed in both groups; (3) no evaluation of the outcomes of interest; and (4) a mean follow-up of less than 1 year. When studies with overlapping populations were identified, we planned to include the report with the largest sample size or the one that most closely matched the inclusion criteria of the present research.
Search strategy
A comprehensive search of the literature was performed of the PubMed, Embase, and Cochrane databases, and we selected original articles with an evidence level of IV or higher from the inception of each database to 2023. The search terms, including Boolean operators suitable for each database, were “patella alta” OR “patellar tendon” OR “patellar ligament” OR “patell*” OR “high riding knee cap” AND “knee flexion contracture” OR “flexed knee gait” OR “cerebral palsy” OR “crouch gait” OR “spastic diplegia.” We placed no restrictions on language or publication period. We manually examined all available reference lists of previously included studies to detect additional studies. The literature search was performed on 23 April 2023, and updated searches were run on 20 June 2023 and 23 July 2023.
Three independent reviewers (M.G.O., S.L.L., and B.T.I), working separately and blinded to each other, screened the search results against the inclusion/exclusion criteria based on the contents of the title, abstract, and keywords. Full texts of potentially relevant studies were independently appraised for eligibility by both authors. Disagreements between the two reviewers were resolved by discussion and consensus with two other authors with extensive experience in this field (I.M.C and P.H.).
Data extraction
Data extraction was done using a standardized form. Data were collected from the text, tables, and figures of the included studies. We extracted data on study characteristics (study title, author name, publication year, study design), patient characteristics (sample size, including number of patients and number of limbs, age at intervention, gross motor function classification system (GMFCS) level), data from interventions (indication, technique, concomitant procedures), and follow-up, where available. The primary outcomes were the mean differences (MDs) in preoperative and postoperative measurements for the following kinematic parameters: knee flexion at initial contact (KFIC), minimum knee flexion in stance (mKFSt), and peak knee flexion in swing (pKFSw), assessed by three-dimensional gait analysis (3DGA). Gait analysis was chosen as the primary outcome measure due to its superior accuracy in determining the effect of PLS surgery when compared with X-ray or clinical assessment, greater objectivity, 49 and availability in the studies reviewed. Secondary outcomes included MDs in preoperative and postoperative measurements for clinical knee flexion contracture (KFC), measured during supine physical examination as the angle formed between the thigh and the leg during maximum passive KE, mean anterior pelvic tilt (APT) obtained from 3DGA, and the gait deviation index (GDI). 50 Due to the infrequent reporting of complications and kinetic parameters in the included studies, these outcomes were not included in our final analysis. We contacted the principal investigators to collect any missing data, additional details, or unpublished data. Prespecified subgroup analyses included data restricted to (1) PTA versus PTS studies, (2) studies controlling for confounding factors, (3) studies associating rectus femoris (RF) procedures (recession or transfer), (4) studies not associating HSL procedures, (5) studies analyzing DFEO versus no-DFEO, and (6) studies with longer-term (≥2 years) follow-up.
Quality and bias assessment
Nonrandomized studies were appraised with the Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) assessment tool, 51 as recommended by the Cochrane Handbook for Systematic Reviews. When using the tool, studies are scored as having low, moderate, serious, or critical risk of bias in seven domains: confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result. 52 Publication bias was investigated by funnel-plot analysis of point estimates according to study weights.
Statistical analysis
Changes in preoperative and postoperative clinical and 3DGA parameters were evaluated by mean values and standard deviation. MD with 95% confidence intervals (CIs) was used to compare treatment effects for continuous endpoints. The Cochrane Q test and I2 statistics were used to assess heterogeneity; p < 0.10, and I2 > 25% were considered significant for heterogeneity. We used a fixed-effect model for outcomes with low heterogeneity (I2 < 25%). Otherwise, the DerSimonian and Laird random-effects model was used. Review Manager 5.3 (Cochrane Center, The Cochrane Collaboration, Denmark) was used for statistical analysis.
Results
Study selection and baseline characteristics
As detailed in the PRISMA flow chart (Figure 2), our literature search initially identified 411 studies. After removing duplicates (n = 93) and studies found to be ineligible based on their title, abstract, or keywords (n = 291), 27 were selected for full-text review in accordance with the inclusion criteria. Of these, 20 were excluded with reasons (Supplemental Table 2), and finally, 7 studies (249 patients and 368 limbs, Table 1) met our inclusion/exclusion criteria and were subsequently selected for quantitative analysis. These comprised five retrospective case–control or cohort studies, one prospective cohort study, and one randomized control trial (RCT). Three studies (58 patients and 71 limbs) used a PTA technique, three studies (36 patients and 58 limbs) used a PTS technique, and one used both techniques (18 patients and 29 limbs). Within the PLS group (110 patients and 158 limbs), there were a total of 48 bilateral procedures, 17 unilateral procedures, and 45 studies in which only one limb was included. Conversely, in the no-PLS group (139 patients and 210 limbs), there were 71 bilateral procedures, 40 unilateral procedures, and 28 studies in which only one limb was included. The detailed description of the procedures performed in the context of MLS in each group is summarized in Supplemental Table 3. There was significant interstudy variability in terms of patient age and length of follow-up.
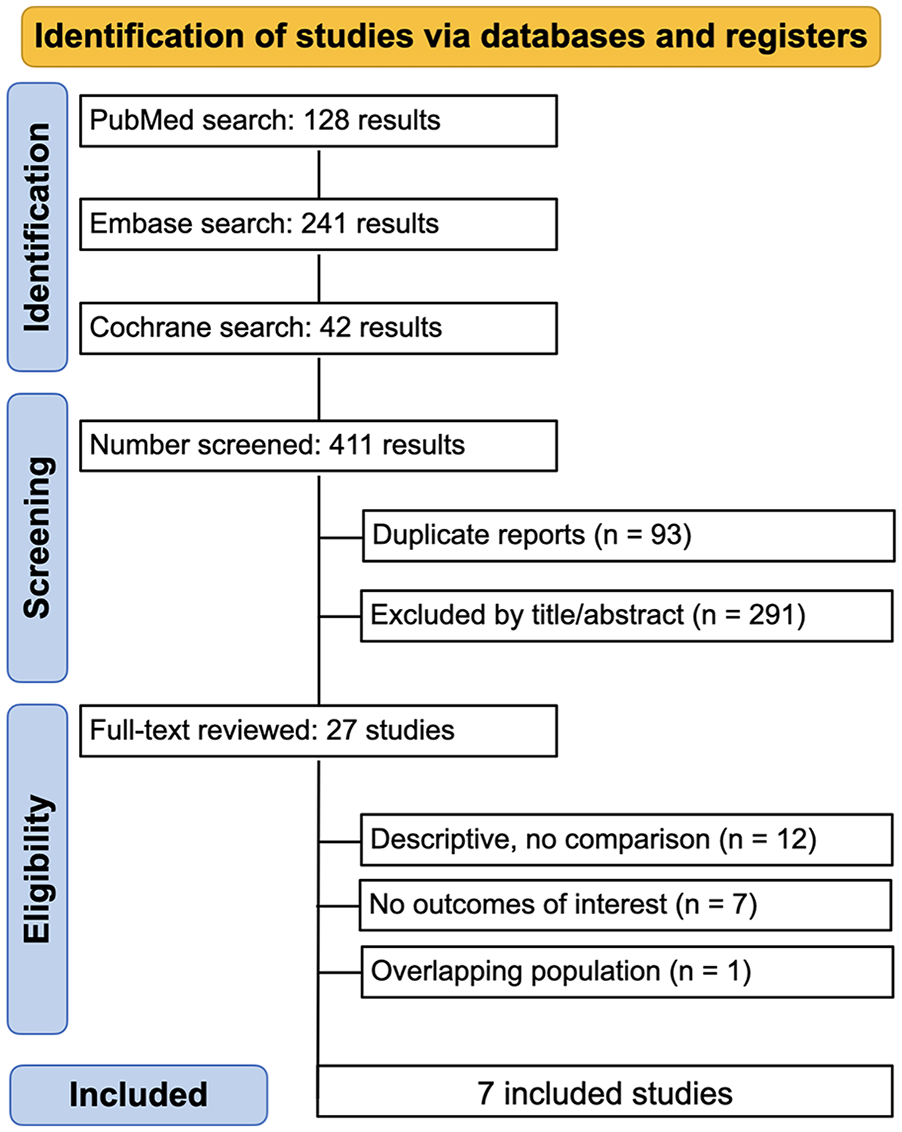
Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram of study screening and selection.
Baseline characteristics of included studies.
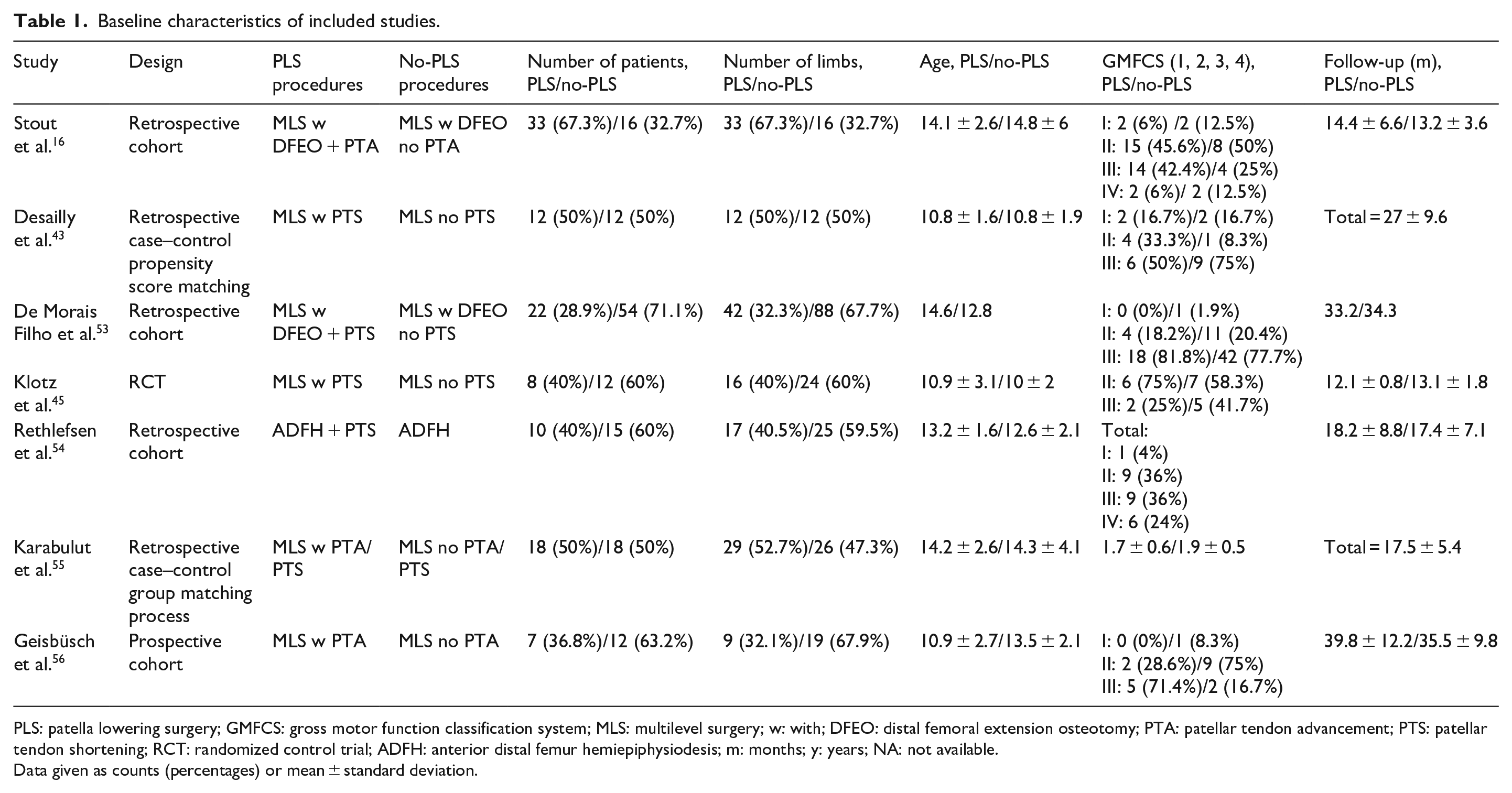
PLS: patella lowering surgery; GMFCS: gross motor function classification system; MLS: multilevel surgery; w: with; DFEO: distal femoral extension osteotomy; PTA: patellar tendon advancement; PTS: patellar tendon shortening; RCT: randomized control trial; ADFH: anterior distal femur hemiepiphysiodesis; m: months; y: years; NA: not available.
Data given as counts (percentages) or mean ± standard deviation.
Pooled analyses of all studies
At a mean follow-up of 22.9 ± 6.8 months (range 12.7 to 37.6), the PLS group had significantly higher improvement in terms of KFIC (MD = −6.39; 95% CI = [−10.4, −2.75]; p = 0.0006; I2 = 84%; Figure 3(a)), mKFSt (MD = −14.27; 95% CI = [−18.31, −10.23]; p < 0.00001; I2 = 89%; Figure 3(b)), and KFC (MD = −5.6; 95% CI = [−9.59, −1.6]; p = 0.006; I2 = 95%; Figure 3(d)) due to a decrease in knee flexion, compared with the no-PLS group. There was also a statistically significant increase in APT for the PLS group (MD = 3.05; 95% CI = [1.15, 4.96]; p = 0.002; I2 = 0%; Figure 3(e)) and an overall trend toward improvement in GDI (Figure 3(f)) and toward a reduction in pKFSw (Figure 3(c)), but these results did not reach statistical significance. The mean pre- and post-pKFSw for the PLS group was 65.53 ± 5.5° and 54.67 ± 3.76°, while for the no-PLS group was 61.98 ± 4.53° and 57.57 ± 2.94°, respectively. Hence, it can be deduced that this decrease in pKFSw is not clinically relevant either, observing how the preoperative values were slightly above the normal value of 60°, as patients with crouch gait have an abnormally elevated pKFSw, and postoperatively, they were slightly below normal. The indications for PLS surgery mentioned by the included studies are listed in Supplemental Table 4.
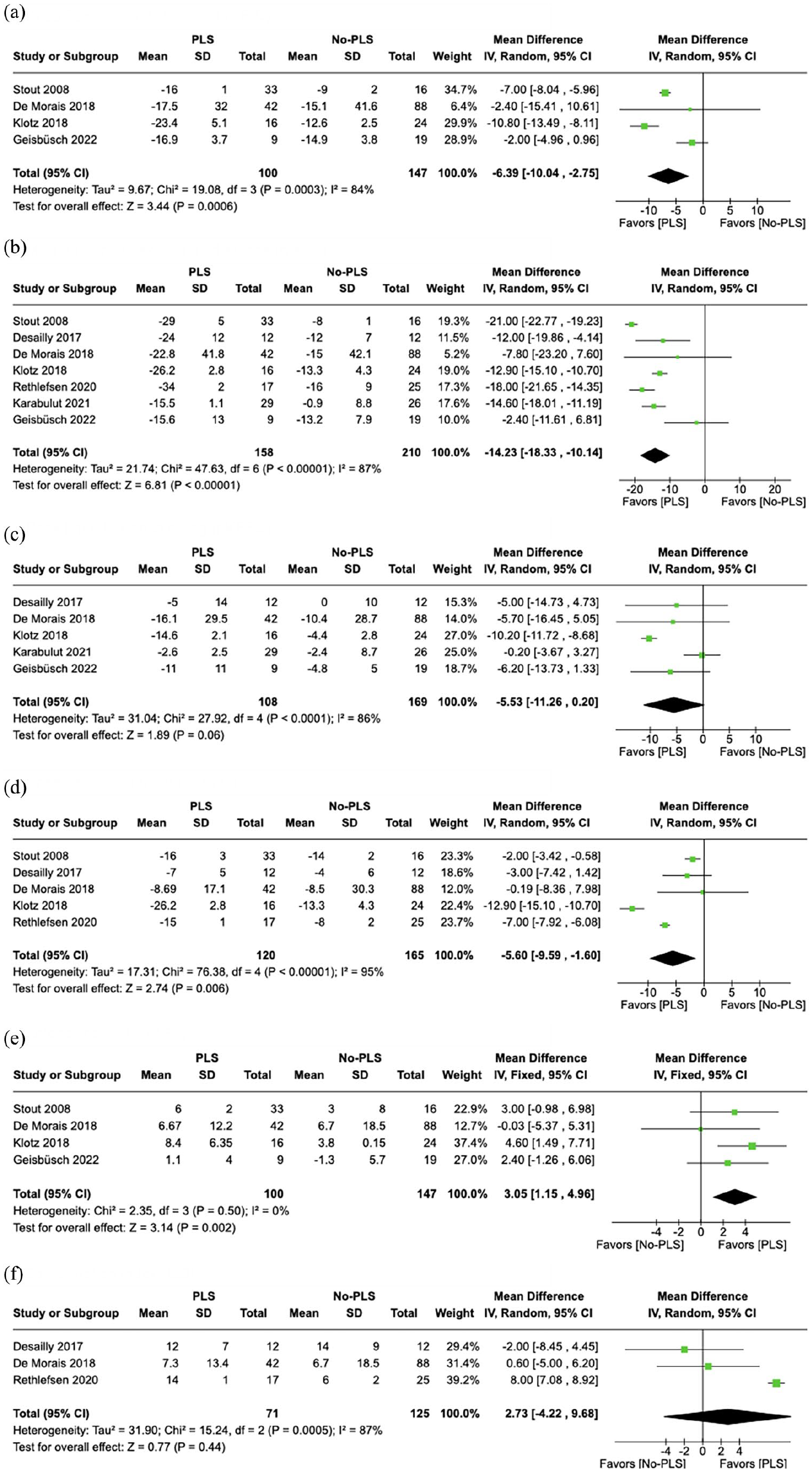
Forest plot of the main results of the meta-analysis. Data represent the MD between preoperative and postoperative values: (a) knee flexion at initial contact, (b) minimum knee flexion in mid-stance, (c) peak knee flexion in swing, (d) knee flexion contracture, (e) anterior pelvic tilt, and (f) gait deviation index.
Subgroup analyses
In a subanalysis of studies using PTA16,56 versus the PTS technique45,53 (Supplemental Figure 1), there was a significant higher improvement in KFIC (p = 0.007) and mKFSt (p < 0.001) and reduction in pKFSw (p < 0.001) in studies using PTS techniques, with reduced heterogeneity. There was a trend toward more improvement in studies using PTA techniques in these parameters, without being statistically significant (p = 0.06, p = 0.21, and p = 0.11 for KFIC, mKFSt, and pKFSw, respectively). KFC improved significantly more with both studies using PTA and PTS techniques versus the no-PLS group (p = 0.006 and p = 0.003, respectively). The higher increase in APT was statistically significant only for studies using PTA techniques, but likely clinically not very relevant due to implying 2.7°. GDI could not be evaluated in these subgroups of patients due to the absence of studies using PTA that included this parameter. The differences in kinematic parameters obtained between the studies using PTS or PTA are not necessarily implicit to the technique itself but rather to the rest of the procedures performed by each group, since the PTS technique has not been directly compared with the PTA technique in the same group subjected to the same associated procedures and treated by the same group of surgeons.
In a subanalysis restricted to high-quality studies that controlled for confounding factors and had a low risk of bias43,45,55 (Supplemental Figure 2), both KFIC and mKFSt demonstrated a statistically significant greater improvement in the PLS group (p < 0.001). There were trends toward greater improvement for KFC (p = 0.1) and GDI (p = 0.54), and reduction in pKFSw (p = 0.19), although this did not reach statistical significance. APT could not be further subanalyzed for high-quality studies because this parameter was not documented in those studies.
Unfortunately, in the absence of patient-level data, the planned subanalysis separating studies associating RF procedures or HSL procedures and studies using DFEO versus no-DFEO was not possible due to the very limited number of studies that reported all patients who underwent these procedures or no patients receiving them, as most patients underwent a combination of the different techniques.
The pooled analysis of the three studies with longer-term follow-up (≥2 years)43,53,56 (Supplemental Figure 3) revealed highly decreased heterogeneity and resulted in no statistically significant differences between PLS and no-PLS groups concerning KFIC (p = 0.17), KFC (p = 0.23), APT (p = 0.29), and GDI (p = 0.29). However, there was a statistically significant higher improvement in mKFSt (p = 0.02) and reduction in pKFSw (p = 0.03) in the PLS group versus the no-PLS group.
In summary, the analysis of particular subgroups according to different criteria led to the conclusion that (1) studies using the PTS technique reported significant improvements in all 3DGA parameters compared with no-PLS, while studies using the PTA technique showed a trend toward improvement that was not statistically significant; (2) as in the overall analysis, high-quality studies showed more improvement in stance-phase gait parameters, but not in KFC; and (3) studies with longer follow-up revealed no significantly superior improvement in KFIC, KFC, and GDI, no significant increase in APT, but a significant improvement in mKFSt and reduction in pKFSw for in the PLS group. In addition, heterogeneity was significantly reduced in all subgroup analyses performed.
Quality assessment
The overall appraisal of individual studies is reported in Figure 4(a), and the combined evaluation in Figure 4(b), both indicating a serious overall risk of bias. All studies had important confounding domains, such as associated procedures performed within MLS, except for the RCT, in which the recruited patients were assigned to each group by balanced randomization. Only two of the remaining studies used an appropriate analytical method that controlled for biases (a propensity score match and a group matching process). The selection of study participants was based on the type of intervention; groups were clearly defined; and follow-up was initiated thereafter. Due to the MLS setting, all participants had undergone concomitant surgical procedures, which were similar between groups in three studies; in another study, an appropriate analysis was performed to estimate the effect of these interventions, and in the remaining three studies, there was no analysis of the effect of concurrent procedures, which may introduce significant bias. Because most studies were retrospective and the inclusion criteria called for preoperative and postoperative gait analysis, outcome data were available for almost all participants, and only two participants of the RCT were excluded because of missing outcome data. It is unlikely that knowledge of the intervention received by the participants influenced the outcome measure, even though the evaluators were aware of the intervention performed on each, given that the outcome assessment was based on 3DGA. This method of assessment was comparable between intervention groups and had a low risk of systematic error related to the intervention received. Selection of the overall effect estimate was based on results from the average of multiple measurements, thus providing greater precision. A detailed appraisal of each study is reported in Supplemental Table 5. As shown in Supplemental Figure 4, there was evidence suggestive of publication bias; the funnel plot showed an asymmetrical distribution of similar-weight studies, with divergence toward the pooled treatment effect size as weights increased for KFIC and pKFSw and greater convergence for mKFSt. There was also a lack of studies reporting worsening of kinematic parameters after PLS, which also suggests a bias against publishing less favorable results or a functional worsening with loss of ambulation and, therefore, impossibility to perform 3DGA.
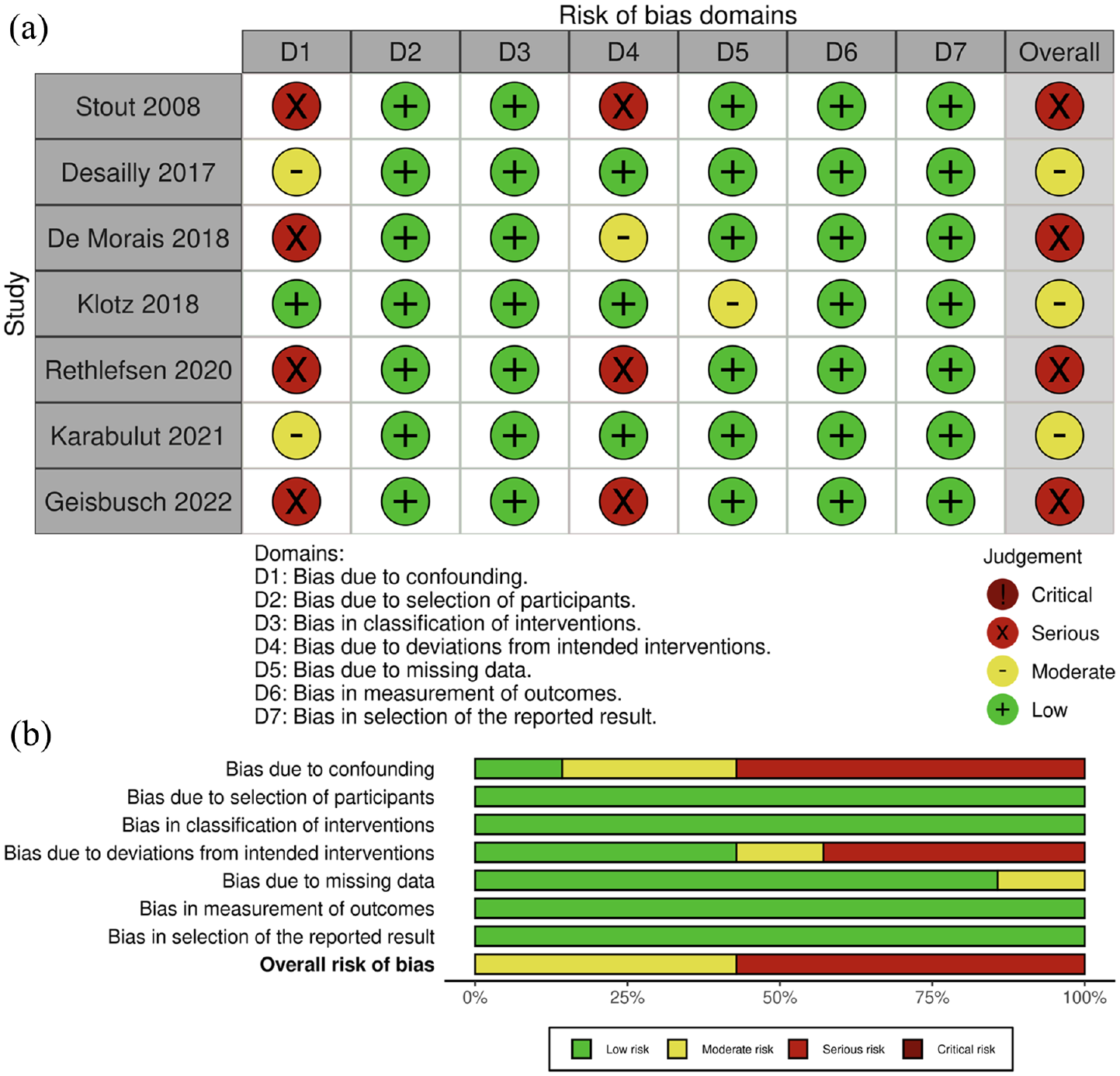
(a) Individual overall traffic light plot of the risk of bias of the studies and (b) summary plot of the combined risk of bias of the meta-analysis. 57
Discussion
In this systematic review and meta-analysis of seven studies, including 249 patients and 368 limbs, we mainly compared the knee kinematic results of PLS to no-PLS as part of MLS for CP patients with crouch gait. The main findings from the pooled and subgroup analyses are as follows: (1) KFIC and mKFST improved significantly more after PLS, especially in studies using a PTS technique, but long-term improvement was only maintained for mKFSt; (2) KFC improved more with PLS overall, but not in the subgroup analysis; (3) after PLS, APT significantly increased and there was a trend toward pKFSw reduction, the latter being significant in longer-term studies, but the potential benefit of hamstrings preservation and/or RF procedures could not be evaluated.
PLS enabled a significantly greater reduction in knee flexion in the stance phase compared with no-PLS, a testament to its efficacy. By lowering the patella to its anatomically appropriate position, the quadriceps muscle regains its optimal angle of pull enhancing its mechanical advantage for KE in an upright posture.44,58 From a functional perspective, gait benefits have been identified, not only in terms of improved mechanical action of the quadriceps; rather, improvements in stance phase have been documented, with greater KE and thus improved stability.20,45 Our meta-analysis indicated a more substantial improvement in the mid-stance subphase (14.27°) than on initial contact (6.39°). This difference could be attributable to impaired selective motor control leading to failure to fully extend the knee during terminal swing and deficient initial contact. As noted in previous studies, we also found significantly higher improvement in mKFSt among patients with longer-term follow-up.59,60 This represents a success interrupting the progressive natural history of crouch gait. 61 While the initial clinical amelioration in KFC might be influenced by accompanying MLS procedures, the greater long-term improvement seen in the PLS group compared with the no-PLS group is likely due to the maintenance effect exerted by the tensioning of an elongated extensor mechanism. 45 Historically, the pivotal role of PLS in avoiding recurrences has been underscored. 62
The anticipated increase in APT following PLS aligns with previous observations in the literature.31,38,45,53,63 This can be attributed to the dual-joint nature of the RF muscle. Besides its role as a knee extensor, the RF functions as a hip flexor. When tightened, this muscle exerts an anterior pull on the pelvis. Moreover, if the knee is extended without attention to the flexion contracture at the hip, it will pull the pelvis anteriorly and exacerbate the APT. 16 Several studies within our review further lengthened the hamstrings, which are generally weak and elongated, thus impairing their function as hip extensors and further increasing the APT.32,34,53,63 –66 Preservation of the hamstrings as hip extensors and incorporating RF procedures likely mitigates APT after PLS.34,45,53,63,67 Unfortunately, data limitations prevented a subanalysis. Notably, an APT rise after extension or shortening osteotomy has been documented,31,68 although to a lesser extent, possibly due to hamstrings’ relative lengthening, making them insufficient for pelvic stabilization. Techniques such as psoas over-the-brim lengthening plus proximal RF lengthening aimed at correcting knee flexion by reducing APT have been previously described. 69 Yet is important to understand the clinical relevance of minor absolute increases in APT and continue exploring treatments to prevent APT worsening, since it may lead to a reciprocal rise in lumbar lordosis, a precursor to lower back pain.70,71
The reduction in pKFSw is an expected outcome when the procedure tightens the quadriceps muscle tendon to improve KE.20,31,38,45,53 However, this outcome did not reach statistical significance in the pooled analysis, and neither has clinical relevance, given that postoperative values were close to normal. In the longer-term subgroup analysis, a statistically significant reduction was observed, but again, it held little clinical meaning. RF procedures have demonstrated efficacy in improving swing phase and thus foot clearance.72,73 Some authors suggest that the addition of RF procedures to PLS would improve pKFSw phase and prevent a stiff knee.45,63 However, as mentioned earlier, our inability to evaluate the impact of RF procedures in a subgroup analysis limits conclusive statements. Besides, global tone management has not been considered in the studies evaluated. The spasticity-reducing effect of selective dorsal rhizotomy results in a improved knee flexion during the swing phase. 74
Gait kinematics assessed by GDI improved in both groups, with a trend toward greater improvement in the PLS group, although the difference was not statistically significant. This may be explained by the fact that GDI is an overall evaluation parameter, and as such is influenced by all surgical procedures performed in MLS. As a result, this parameter may explain the moderate effect of PLS in global terms. Another possibility is that PLS has a small net benefit on gait. Notably, our observation indicates an improvement in the stance phase, but not the swing phase, coupled with potential negative impact on pelvic dynamics. GDI, encompassing different aspects of the entire gait cycle, including pelvis and hip angulation in all three planes, the sagittal plane of the knee, and ankle–foot progression is sensitive to these intricacies. 75 The wide CIs reported by the studies and our evaluation limited to data from three studies might account for the lack of statistical significance. Sossai et al. 20 credited the significant improvement in global gait indices to PLS; however, the absence of a control group in their study prevents a direct attribution of these results to the effect of PLS within MLS. In addition, the possible benefits of PLS on kinetics could not be evaluated due to the lack of data in the included studies. However, the sole study evaluating kinetics reported a significant increase in peak KE moment arm in the PLS group compared with no-PLS, a noteworthy consideration. 55
In the studies analyzed, common indications for PLS, consisting of either PTA or PTS, included a high patella on a lateral knee X-ray or a knee extensor lag exceeding 10°. Treatment with DFEO is another indication for PLS due to the laxity generated at the extensor mechanism. Crouch gait (knee flexion >30° at mid-stance) alone was only acknowledged as an indication for PLS by one author. 42 These indications are in line with recent expert consensus. 76
This study has certain limitations that should be noted. In the first place, despite an exhaustive review of the literature published to date, the analysis was confined to only seven studies comparing MLS with PLS and no-PLS. Of these, few were properly controlled and there was significant heterogeneity in the pooled analysis. Nonetheless, the inclusion of a substantial number of patients (n = 249) and limbs (n = 368) from these reports provides a substantial basis for drawing conclusions. Furthermore, subgroups analysis of higher quality offered more robust data, enhancing the reliability of results. Second, as is typical in orthopedic studies focusing on deformity management in CP patients, PLS is often combined with other procedures to correct crouch gait, making it difficult to objectively evaluate the isolated effect of a single procedure. Therefore, we focused on comparative studies between two groups of patients undergoing MLS with the main difference being the PLS procedure, to draw conclusions about its true effect on gait. Although the concomitant procedures were consistent with the general principles in CP, correcting muscle imbalance and restoring bony lever arm dysfunction, the variability in these procedures across patients may contribute to differential improvements in gait. Moreover, the asymmetry in spastic diplegia, leading to unilateral PLS in some cases, and the analysis of only one limb in bilaterally performed PLS, further complicates the interpretation of results. Third, although we attempted to obtain some results in subgroup analysis, we are aware that in certain subgroups, limitations in the number of studies may lead to insufficient power to draw solid conclusions. Future research should consider the impact of distal lever arm deformities in crouch gait treatment. Furthermore, in theory, the reduction of knee flexion in swing phase can be minimized by associating RF recession, and the increased APT by avoiding HSL, but there is no evidence for this and deserve to be further investigated. Fourth, among the primary outcomes assessed, only mKFSt, the most relevant kinematic parameter, was reported in all the studies included, whereas KFIC and pKFSw were only reported in four and five studies, respectively. In addition, the absence of information on maximum ankle dorsiflexion in stance, not documented in the reviewed studies, might impact the precision in distinguishing true crouch from jump or apparent equinus gait patterns. Moreover, details on presurgical or postsurgical orthotic treatment and postoperative physical therapy programs were not included, constituting a potential gap in understanding the comprehensive care context. It is crucial to acknowledge that orthotic use is vital for controlling residual excessive ankle dorsiflexion, leading to a reduction in ground reaction force. Optimizing the biomechanics of the knee joint aims to achieve more normal gait mechanics, enhanced mobility, and functional outcomes, with the ultimate goal of improving participation in daily activities and quality of life of CP patients, which should also be addressed when evaluating the results of surgical procedures, as part of the comprehensive care of individuals with CP. 59
To conclude, this meta-analysis shows improved overall results of PLS in combination with MLS for children with CP and crouch gait in stance-phase knee kinematics parameters compared with MLS alone. APT is increased, and the statistically significant reduction in knee flexion in swing phase in the long term seems clinically negligible. However, the potential benefit of RF procedures and hamstrings preservation could not be evaluated and merit further research. Surgery should be customized according to individual patient needs, the most common indications for PLS being knee extensor lag over 10° or a high patella on a lateral knee X-ray, as well as if DFEO is performed and extensor mechanism laxity is generated.
Supplemental Material
sj-docx-2-cho-10.1177_18632521231217542 – Supplemental material for Does patella lowering as part of multilevel surgery improve knee kinematics in children with cerebral palsy and crouch gait? A meta-analysis of comparative studies
Supplemental material, sj-docx-2-cho-10.1177_18632521231217542 for Does patella lowering as part of multilevel surgery improve knee kinematics in children with cerebral palsy and crouch gait? A meta-analysis of comparative studies by María Galán-Olleros, Sergio Lerma-Lara, Beltran Torres-Izquierdo, Ana Ramírez-Barragán, Rosa M Egea-Gámez, Pooya Hosseinzadeh and Ignacio Martínez-Caballero in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231217542 – Supplemental material for Does patella lowering as part of multilevel surgery improve knee kinematics in children with cerebral palsy and crouch gait? A meta-analysis of comparative studies
Supplemental material, sj-pdf-1-cho-10.1177_18632521231217542 for Does patella lowering as part of multilevel surgery improve knee kinematics in children with cerebral palsy and crouch gait? A meta-analysis of comparative studies by María Galán-Olleros, Sergio Lerma-Lara, Beltran Torres-Izquierdo, Ana Ramírez-Barragán, Rosa M Egea-Gámez, Pooya Hosseinzadeh and Ignacio Martínez-Caballero in Journal of Children’s Orthopaedics
Footnotes
Author contributions
M.G.-O., S.L.-L., B.T.-I., A.R.-B, R.M.E.-G., P.H., and I.M.-C. all made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent
Institutional review board approval and informed consent were not sought because the data were anonymous and publicly available.
Protocol
This systematic review and meta-analysis were conducted following the PRISMA statement and the most recent methodological guidance from the Cochrane Handbook for Systematic Reviews of Interventions.
Quality assessment
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.