
Abstract
Purpose:
The aim of this study is to analyze the clinical reality of pediatric trigger thumb among members of the European Paediatric Orthopaedic Society.
Methods:
A 35-question survey was sent to all European Paediatric Orthopaedic Society members, focusing on surgeon’s profile and experience, trigger thumb diagnostic and trigger thumb treatment approach. Descriptive statistics were performed.
Results:
A total of 99 responses were analyzed. Most important factor considered in the therapeutic approach was the presence of a locked interphalangeal joint (52%). Regarding treatment, 41.4% opt for conservative approach as the first line of treatment, while 30.3% consider surgery and 28.3% just observe. Nevertheless, 76% mention to treat conservatively their patients and 99% to consider surgery at some stage. Regarding surgical technique, 96% do it open and 56% consider 2 years as the minimum age for procedure. Most surgeons perform this procedure in out-patient care (87%), don’t administer prophylactic antibiotherapy (80%), use a tourniquet (75%), don’t use any postoperative immobilization (64%), and report complications related to surgery (64%), mainly recurrence/incomplete division (59%) and superficial wound infection (30%).
Conclusion:
Our study shows a significant variability in the initial management of pediatric trigger thumb with a predominance of conservative management, followed by surgery and observation without treatment. The disparity in treatment options and timing, or waiting times before moving on to different therapeutic options, shows us that this is a controversial issue and that the development of prospective randomized controlled studies is needed to analyze the different treatment methods and determine which ones give the best outcomes.
Keywords
Introduction
Trigger thumb is one of the most common pediatric hand conditions, and it is defined as a stenosing tenosynovitis of the flexor pollicis longus (FPL) with a characteristic flexion deformity of the interphalangeal (IP) joint. 1 Its incidence is of 1 to 3 per 1000 children2,3 and is far more frequent than triggering of other fingers. 4 The age of onset is variable, but usually occurs in the first 4 years of life. Regarding etiology, this is still controversial but it seems that is probably due to multifactorial etiology with a possible genetic predisposition.5 –7 There is no consensus on the therapeutic approach to this condition, and the literature often includes several different options and strategies with good outcomes, including mere observation without intervention, conservative treatment (exercises and/or splints), or surgical treatment (open or percutaneous).1,8 –17 The aim of this study is to analyze the clinical reality of trigger thumb treatment in the pediatric population among members of the European Paediatric Orthopaedic Society (EPOS), focusing on surgeon’s profile and experience and trigger thumb diagnostic and treatment approaches.
Material and methods
A survey was distributed to 642 EPOS members. The survey and study protocol were designed by four EPOS members, and subsequently approved by the EPOS Research and Scientific Committee and EPOS Board. An email with a link to the survey, hosted by https://forms.gle/ZfSTBMGZrzRiBFWx8, was sent to all EPOS members. At least one reminder email was sent for members who had not responded to the survey. The 35-question survey focused on surgeon’s profile and experience, trigger thumb diagnosis, and treatment approach. The survey consisted of three sections: (1) surgeon, (2) caseload and clinical approach, and (3) treatment option (divided into two subsections—conservative treatment and surgical treatment) (see supplemental material). The survey included binary questions, multiple choice, “select all that apply,” and open textbox question. Descriptive statistics were performed. Data analysis consisted of descriptive statistics.
Results
Surgeon
A total of 99 responses from 29 different countries and 4 continents were analyzed. The top responding countries were Spain (n = 19), Portugal (n = 14), and Italy (n = 9). Eighty-three percent of respondents considered themselves to be at least in level III of expertise according to Tang and Giddins. 18 They consider themselves to be surgeons with appreciable experience in the use of the relevant technique(s), having practiced as specialists over a longer period (typically >5 years). Other relevant data relating to the surgeon’s gender, age, working position, medical board certification, working department, type of institution, and expertise are detailed in Table 1.
Surgeon.
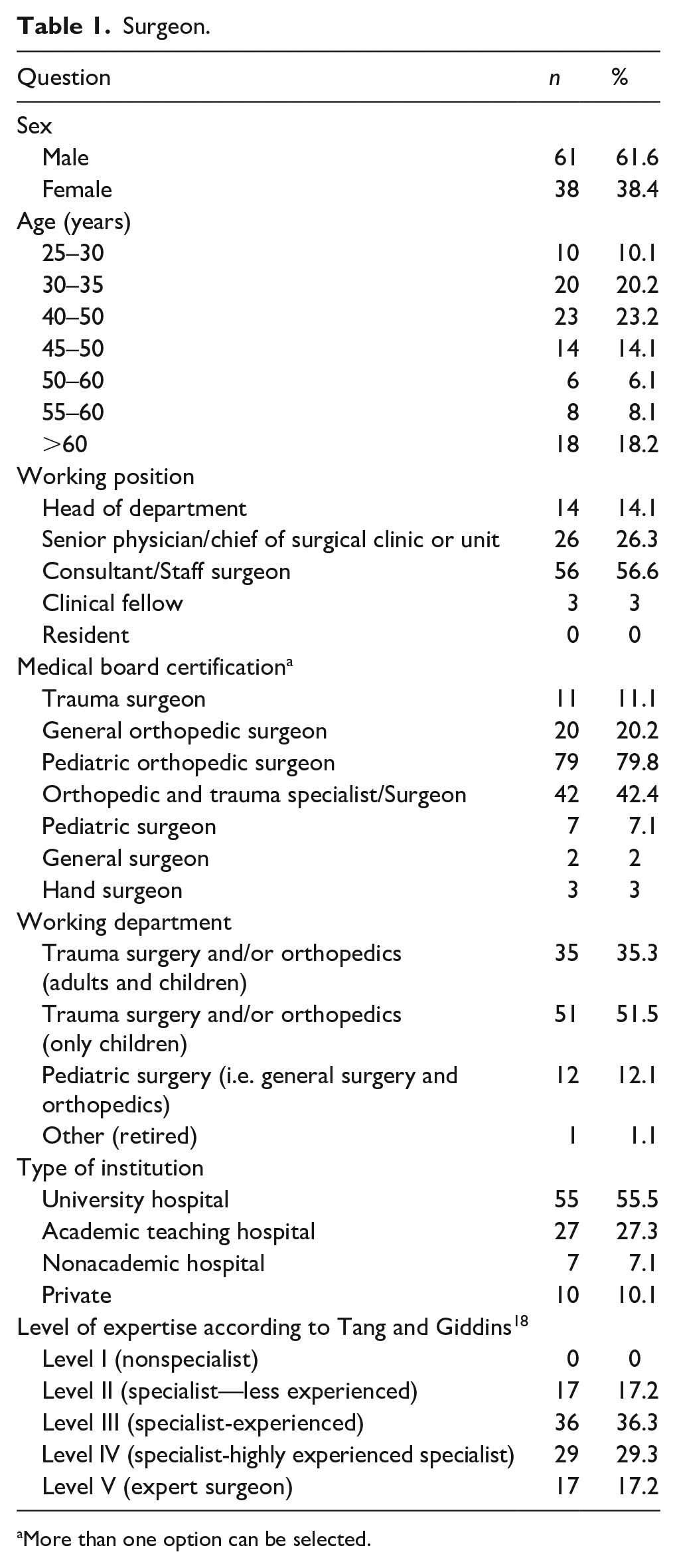
More than one option can be selected.
Caseload
Regarding caseload, 49.5% of respondents observe more than 10 trigger thumbs per year (of which only 4% observe more than 50/year). The most important factor considered in their therapeutic approach is the presence of a locked IP joint (51.5%), followed by the age of the patient (22.2%) (Table 2). The majority of respondents (82.8%) do no not use any classification to guide treatment and of the 17.2% who do, the majority (76%) use Watanabe et al.’s 19 classification while the others use Sugimoto’s 20 classification. Diagnosis is clinical for 83.8% of respondents, who do not request any imaging studies. However, 8% of respondents request an X-ray and 8% request an ultrasound in the diagnostic approach.
Caseload.
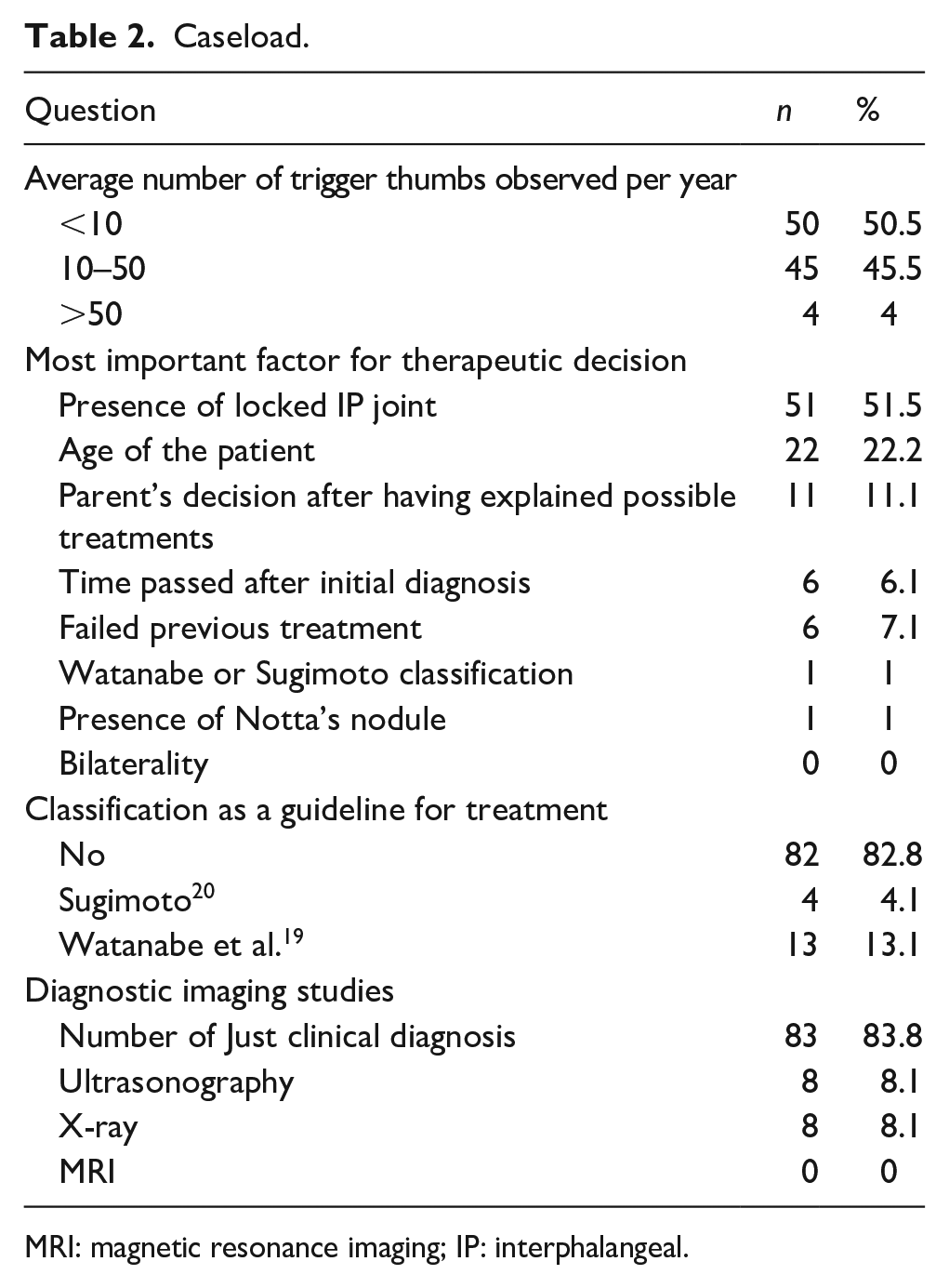
MRI: magnetic resonance imaging; IP: interphalangeal.
Treatment
Regarding treatment option, 41.4% prefer conservative approach as the first line of treatment, while 30.3% consider surgery and 28.3% don’t treat at first observation (maintaining regular observation in consultation) (Table 3). Nevertheless, 76% mention to treat conservatively and 99% to consider surgery at some stage. Of those who consider conservative treatment (n = 75), 85% treat between 1–10 trigger thumbs/year and 15% treat between 10–50 thumbs/year. Of those who opt for conservative, 74.7% do not use any kind of splint and/or orthotics and only recommend exercises. Of the remaining, 18.6% recommend static splints (splint without passive extension movements) and 6.7% dynamic splints (splint with passive extension movements). For those who use splints as part of the treatment, 84% mention complications including residual triggering (63%), dropout treatment (25%), and contact dermatitis (12%). Regarding exercises and/or splinting, 54% move on to a different option after 6 months and 21% after 1 year of no results.
Treatment option.
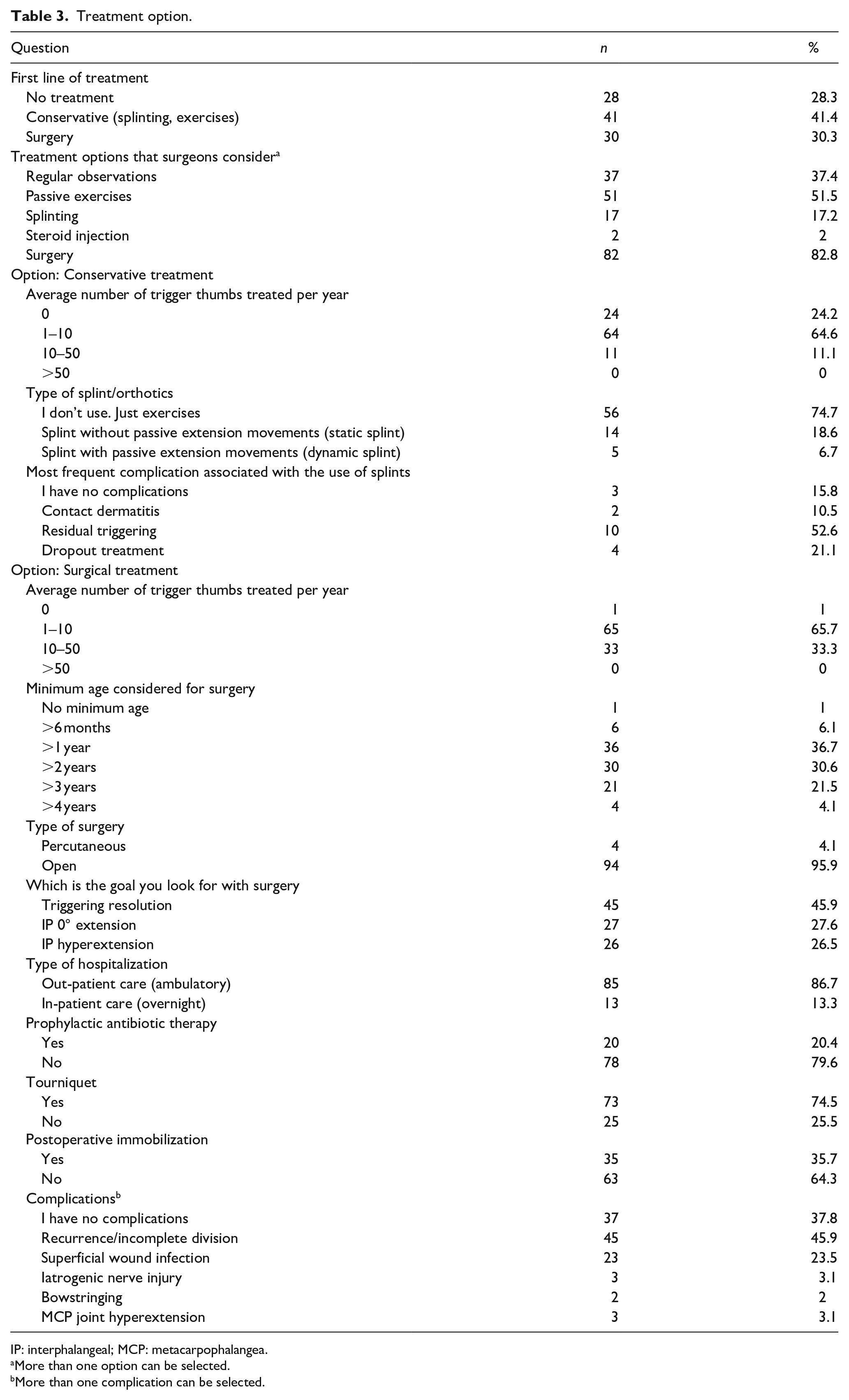
IP: interphalangeal; MCP: metacarpophalangea.
More than one option can be selected.
More than one complication can be selected.
In these cases, where conservative treatment fails, open surgery (95.4%) is the most commonly chosen option, followed by percutaneous surgery (4.6%). Of the respondents who make just regular observations on their patients, all of them wait at least 6 months before moving on to a different option (62% move forward after 6 months and 38% wait more than 1 year). In these cases, they consider the following treatment options: open surgical treatment (79%), exercises (11%), percutaneous surgery (7%), and splinting (3%). Regarding surgical treatment, 99% (n = 98) refer to do it at some stage. Among respondents, 66% operate between 1–10 trigger thumbs/year and 33% between 10–50 thumbs/year. Regarding the minimum age for surgery, most surgeons (56.2%) only consider surgery after 2 years of age.
Considering the surgical technique, 96% perform open surgery. Of these, 58% mention they only section the A1 pulley and do not partially resect any A1 pulley fragment. On the contrary, 25% of the surgeons report that they systematically perform a partial resection of the A1 pulley, while 18% do it only in selected cases. As for the primary goal of surgery, 45.9% of surgeons intend to resolve the trigger, 27.6% want to achieve a 0° extension of the IP and 26.5% a hyperextension of the IP joint.
Regarding type of hospitalization, 87% of the surgeons perform this procedure in out-patient care (ambulatory), 80% don’t administer any kind of prophylactic antibiotic therapy, and 75% use a tourniquet to perform the procedure. Regarding the use of postoperative immobilization, 64% don’t use any. Of the 36% who use postop immobilization, 91% apply a soft bandage while the others use splints. With regard to immobilization time, the maximum time of immobilization is 3 weeks for all respondents, with 46% using it for just 1 week, 43% for a 2-week period, and 11% for a 3-week period.
As for complications related to the surgery, 35.7% reported having no complications. As for the 64.3% who reported complications, the most frequently mentioned was recurrence/incomplete division in 59%, followed by superficial wound infection in 30%, iatrogenic nerve injury in 4%, MCP joint hyperextension in 4%, and bowstringing in 3%. The perception of the approximate percentage of complications varied between 0.1% and 10%, with 88% reporting a range between 1% and 5%. When asked how often surgeons observed a tight IP volar plate after A1 division (likely due to long-standing flexion contracture), 45% answered yes but only rarely, while the remaining surgeons said they had never seen it. Of the surgeons who answered yes, they believe that the cause that most contributes to this situation is the older age of the child in general (43.2%). Other possible causes considered include fixed flexion contracture for more than 3 years (34.1%), more than 1 year (13.6%), or more than 5 years (2.3%). Of the 89% of surgeons who work with residents in their departments, 44% report that they frequently allow their residents to do the surgery, 40% allow them to do it but only rarely, and 16% report that they never allow their residents to do it.
Discussion
The aim of this study was to report the clinical reality of the diagnostic and treatment approach to the trigger thumb in the pediatric population among the members of the EPOS. To the best of our knowledge, this is the first survey study on pediatric trigger thumb, focusing on the surgeon’s profile, therapeutic approach and in the perception of their results. Among the active members of EPOS, the response rate was 15.4%, similar or slightly lower than the response rates from previous EPOS or Pediatric Orthopaedic Society of North America (POSNA) surveys.21 –26 It should be noted, however, that of the 642 members who received the email, only 379 members (59%) opened it, assuming that these are probably the ones who are most interested in the pathology or anatomical segment in question, and considering this sample, the response rate was 26.1%. Regarding caseload, 50% of those surveyed observe 1 to 10 trigger thumbs a year, which means that although it is a common pathology, there is a significant dispersion between different hospitals and surgeons, which means that there isn’t such a substantial concentration of cases per surgeon, with only 4% seeing more than 50 trigger thumbs a year. Another probable reason for this is that most surgeons who responded to the survey work in academic hospitals (83%), many of them with a high degree of differentiation, probably focusing their intervention on pathologies of greater complexity and functional or vital impact, making room for the treatment of pathologies of lesser technical complexity and less resource requirements, to be treated in other centers.
Regarding the treatment, there is not a real consensus on the best option or approach, as the literature shows us variable rates of spontaneous resolution and outcomes with conservative options (exercises and or splinting) or surgical procedure (open or percutaneous).1,8 –17 Regarding natural history of this condition, some cases resolve spontaneously without the need for any type of intervention. Baek and Lee, 1 in a study with 67 thumbs and a 5-year follow-up, obtained a complete resolution in 76% of the cases, while, Hutchinson et al., 8 with 93 thumbs and a similar follow-up, reported resolution rates around 32%. For this reason, many surgeons choose not only to intervene in the initial phase but also to keep regular observations in the hope that the trigger thumb will resolve spontaneously. In our study, 28.3% said they didn’t treat the patient at first consultation. In any case, most surgeons don’t wait as long as described in Baek’s or Hutchinson’s article, opting to move on to another therapeutic approach if they don’t reach spontaneous resolution (62% after 6 months and only 1% wait more than 4 years). In this case, the most widely considered following option is open surgery (79%). This decision also seems understandable, since after a long period of waiting without success, the surgeon will try to move on to the option that guarantees the best results. The majority of the studies 13 report success rates with surgical treatment around 95%–100%. Han et al. 14 reported full tendon relief with surgical treatment even after 5 years of age in 100% of the 31 operated thumbs he studied. Furthermore, Farr et al. 13 in his systematic review reported full IP joint motion in 95% of patients treated surgically, 67% treated with orthotics, and 55% treated with exercise, concluding that open surgery yields the most reliable outcomes. Regarding conservative treatment, this is the preferred first-line treatment option in our study (41%) with 76% of respondents considering it at some stage. Good results have been described in the literature, especially with the use of splints with or without passive mobilization, although it is known that success rates are lower than for surgical treatment.11,13,27,28 In our study, of all those who mention to treat conservatively their patients, only a fifth recommended the use of splints. These treatment failures with conservative method are associated not only with the specificity of the treatment method but also with the lack of co-operation and compliance from patients and families. This reality was also identified in our study with 84% of those who use splints, reporting complications, mainly treatment failure (63%) and dropout treatment of the patients and families (25%). It is also interesting to see that there are huge differences in the outcomes, fact that highlights the cultural differences of the families’ expectations and compliance with the treatment, with different nonoperative resolution rates according to geographical region.11,12,27 Regarding splinting with or without exercises, this option is very common in Asian countries and success rates vary from 39% to 92%.27,29 Koh et al. 11 published his results with a rate of resolution of 92% at 22 months in 36 locking thumbs (all Watanabe stage 3), while Yano et al. 12 reported a 54% success rate at 42 months. Dittmer et al., 9 in his article with 193 thumbs, reported a 54% success rate at 42 months and also note that the cases with rigid deformity (Sugimoto stage 4) did very poorly with only 14% resolving without surgery. Furthermore, Dittmer et al. 9 also stated that stage 4 thumbs are 4.6 times more likely to fail conservative treatment and go on to surgery when compared with stage 2 or 3 thumbs. Ogino, 10 on the contrary, suggests that passive exercises should be done while the child is sleeping and to consider surgery if there is no resolution by the age of 5. All respondents who treat their patients conservatively indicate that if this treatment fails, they move on to surgical treatment (95% open and 5% percutaneous). The majority of these surgeons (54%) consider conservative treatment to have failed if there is no result after 6 months from the start of the treatment and 11% after 1 year. Around one fifth of surgeons don’t necessarily value the time that has passed, considering going ahead with surgery if parents request, even if it hasn’t been 6 months since the start of the conservative treatment.
Regarding surgical treatment, only 7% consider surgery before the first year of life, while the majority (56%) recommend it after the age of 2. There is no consensus in the literature on the age for surgery, with some articles arguing that it is possible to achieve complete correction even after the age of 3 or more, or even that the favorable outcome is independent of the age.14,30 Despite this, the likelihood of spontaneous resolution appears to be much lower in cases where the IP joint flexion contracture is greater than 30° on initial observation (only 2.5% are expected to resolve spontaneously after 3 years of follow up), 8 so the decision to proceed with early surgical treatment may be more justified in these cases. In patients where there isn’t such severe flexion of IP joint, it seems reasonable that there is no need for early intervention, considering the possibility of spontaneous resolution and the risk of operating on very young children, which also entails greater technical difficulties and surgical and anesthetic risks. As for the type of surgical technique, only 4% reported using a percutaneous technique. This low percentage is consistent with the tendency in the literature to favor open surgery since the open technique is significantly safer and more effective in resolving this pediatric condition. Sirithiantong et al. 16 in his article even stated that the risk of recurrence is 3.29 times higher with percutaneous release of the A1 pulley when compared with open surgery. In addition, Masquijo et al., 17 in his level II prospective study, do not recommend percutaneous release due to the risk of iatrogenic neurovascular and FPL injury or incomplete release of the A1 pulley. However, in our study, of the four surgeons who reported performing percutaneous surgery for trigger thumb, only one reported complications (incomplete division and recurrence).
Another surgical issue often debated is whether if complete A1 pulley division is enough for trigger thumb resolution. Some studies refer the importance of releasing 50% of oblique pulley31,32 to achieve full IP extension, while others also focus on the release of Av pulley (variable annular pulley) to achieve complete resolution of the triggering. 33 Nevertheless, it is widely agreed that complete division of both A1 and A2 pulleys simultaneously is not advisable, because this can result in bowstring. There is no consensus on the need to resect part of the A1 pulley. In our study, 58% reported that they only section A1 pulley without partial resection. Of these 58%, around 51% report recurrence as a postoperative complication in their clinical practice, while of the 24% who always perform partial resection of the A1 pulley, 43% report recurrence as a complication. Although associated with better results, open surgical treatment is not exempt from few complications such as incomplete release, wound complications, bowstringing, nerve injury, IP flexion deficit, and metacarpophalangeal joint hyperextension.13,34,35 Dittmer et al. 9 in his article reported a complication rate of 3.4% with a recurrence and superficial infection rate of 1.7% each while Linhua et al. 15 in his study analyzing 1930 operated thumbs reported a complication rate of 0.2% referring to 1 patient who needed to be re-operated on due to trigger recurrence. As in the literature, the most frequently reported complications in our study were recurrence/incomplete division (59%) and superficial wound infection (30%). Regarding infection, 20% of surgeons surveyed reported using prophylactic antibiotic therapy, and of these, 35% mentioned superficial infection as one of the postoperative complications in their clinical practice. Paradoxically, of the 80% who don’t administer prophylactic antibiotics, only 21% reported superficial infection as a complication.
Conclusion
Our study shows that there is significant variability in the initial management of pediatric trigger thumb between EPOS members, with a predominance of conservative management, followed by surgery and observation without treatment. However, conservative treatment is an option for 76% of respondents, and surgical treatment is an option for 99% at some stage. For the majority of respondents, conservative treatment consists only of recommending exercises (75%) (not using splints or orthotics), and surgical treatment is mostly performed using an open technique (96%). The disparity in treatment options and timing, or waiting times before moving on to different therapeutic options, shows us that this is a controversial issue and that clear guidelines are not yet well defined. In the future, we hope that this study will encourage the development of prospective randomized controlled studies that can effectively analyze the different treatment options and determine which ones give the best results.
Supplemental Material
sj-docx-1-cho-10.1177_18632521231214312 – Supplemental material for Trigger thumb treatment approach: Results of a survey of EPOS members
Supplemental material, sj-docx-1-cho-10.1177_18632521231214312 for Trigger thumb treatment approach: Results of a survey of EPOS members by Marcos Carvalho, Laura M Perez-Lopez, Sebastian Farr and Nunzio Catena in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-2-cho-10.1177_18632521231214312 – Supplemental material for Trigger thumb treatment approach: Results of a survey of EPOS members
Supplemental material, sj-pdf-2-cho-10.1177_18632521231214312 for Trigger thumb treatment approach: Results of a survey of EPOS members by Marcos Carvalho, Laura M Perez-Lopez, Sebastian Farr and Nunzio Catena in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors thank to all of the anonymous EPOS members who responded to this survey.
Author contributions
MC: Study design, data analysis, manuscript preparation.
LMP-L: Study design, manuscript revision.
SF: Study design, manuscript revision.
NC: Study design, manuscript revision.
All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent
The survey was anonymous and did not require informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.