
Abstract
Purpose:
Foot deformities are prevalent in children with cerebral palsy, but there is limited research on the progression of foot posture during growth. Our study aimed to evaluate the change in dynamic foot posture in children with cerebral palsy.
Methods:
Children with cerebral palsy, aged 17–40 months, were recruited to participate in this Institutional Review Board–approved prospective longitudinal study by having serial foot posture evaluations. The coronal plane index and foot segmental impulses were measured with dynamic pedobarography. Data were compared between children stratified by Gross Motor Function Classification System level and typically developing children using serial Welch’s t-tests across time with Holm correction for multiple comparisons.
Results:
In total, 33 children (54 limbs) were included in the analysis (21 bilateral and 12 unilateral; Gross Motor Function Classification System: I-13, II-14, III-4, IV-2. Children completed 16.9 (± 4.4) evaluations (initial age 2.9 (± 0.7) and final age 18.6 (± 1.7) years)). Early valgus foot posture normalizes in children at Gross Motor Function Classification System levels I/II and persists in children at levels III/IV who do not have foot surgery. For most young children, foot posture development is variable.
Conclusion:
Foot posture in young children with cerebral palsy begins in valgus and tends to normalize in youth who walk without an assistive device. Conservative management of foot deformity is recommended in early childhood.
Level of evidence:
Level II, prognostic study.
Introduction
Children with cerebral palsy (CP) often have gait patterns that deviate from typical development. Foot deformities, such as equinus, varus, and valgus, are common in children with CP. Secondary impairments such as compensations at the knee and hip are often present. 1 Such musculoskeletal deformities are accompanied by abnormal weight distribution during walking, which can become severely abnormal with growth and weight gain. 2 Despite the high prevalence of foot deformities in children with CP, there is limited evidence on how foot deformities evolve and affect gait development.3,4
Previous research shows that plantar pressure is a reliable method of evaluating foot deformity 5 and is significantly different between children with CP and typically developing (TD) children.6,7 A study by Galli et al. 8 revealed an increase in midfoot pressure in children with diplegic CP. They documented patterns of reduced heel contact and valgus foot deformity in 74% of children with diplegia and 54% of children with hemiplegic CP.
The high prevalence and negative impact of foot deformities has motivated several authors to examine short-term treatment effectiveness. Physical therapy (PT) is initiated in the early development of children with CP, leading to improvement in gross motor function.9 –11 A study by Theis et al. 12 demonstrated improved passive ankle dorsiflexion following prolonged passive stretching. Ankle foot orthotics (AFO) are the most used lower limb orthoses among children with CP and are shown to improve gait function and facilitate ankle dorsiflexion. 13 As a consequence of growth, foot deformities may progress, and conservative methods may not be effective. Surgical intervention is often employed to reduce toe walking, 14 correct planovalgus deformity, 15 and correct varus foot deformity. 7 The timing of surgical treatment is inconsistent among studies.16 –19
Although reports demonstrate the frequency of foot deformity and short-term effects of treatment, there is limited evidence describing changes over the entire course of childhood. Longitudinal change in gross motor function, 20 gait, 21 and passive range of motion 22 has been evaluated in children with CP. A study by Hanna et al. 20 finds that gross motor function after peaking between ages 6 and 8 years and plateauing between ages 9 and 12 years tends to decline after age 13 years in youth at Gross Motor Function Classification system (GMFCS) levels III–V. With growth, decreases in hip, knee, and ankle sagittal plane ranges of motion during gait are observed in children with CP. 21 Longitudinal studies of passive range of motion in children with CP show progressive lower-extremity contracture development with age. 22 Previous reports on foot development demonstrate that valgus deformities may resolve in children with CP at GMFCS levels I/II during early childhood, whereas they may persist in children classified as GMFCS levels III/IV. 4
The purpose of our study was to prospectively evaluate the evolution of dynamic foot posture over the course of childhood growth in children with CP who followed the standard care at a single specialty center. Comprehensive knowledge of foot posture development in ambulatory youth with CP will help guide clinical care and inform families for shared decision-making.
Methods
In 2003, children aged 17–40 months with a diagnosis of CP were recruited from a children’s hospital setting to participate in an Institutional Review Board–approved prospective longitudinal observational study. For this analysis, a query of this larger cohort identified participants with a minimum of seven evaluations over the 18-year study, and a final evaluation at age ≥ 14 years. Sufficient gait function was required to collect dynamic foot pressure using dynamic pedobarography with external support when necessary. Children were assigned a GMFCS classification and limb involvement (unilateral or bilateral) between ages 5 and 8 years.4,23 Participants were treated at a single specialty center with conservative treatment using PT during early childhood. Orthotics were used alone for common foot and ankle deformities during walking or in conjunction with botulinum toxin for muscle spasticity. When foot deformities could no longer be managed by conservative treatment (progressive deformity, pain, and skin breakdown), surgery was performed. No participants were excluded based on conservative versus surgical intervention. Standing foot and ankle radiographs were obtained when a decision was made for complete surgical correction of varus or valgus deformity. 24 Since our primary goal was to have a functional foot for walking, we placed more emphasis on pedobarograph, but used radiographs for surgical planning.
Children with CP were evaluated every 6 months until age 5 years, and then yearly until age 21 years. At each visit, participants walked barefoot across a foot pressure mat at their preferred walking speed, either independently, with an assistive device, or while hand-holding. Three foot strikes were collected per limb and averaged for analysis (F-Scan Measurement System, Tekscan, Boston, MA, USA). While measurements were taken for both feet, only measurements of involved limbs were considered for data analysis in children with unilateral involvement. For age-matched cross-sectional comparisons, foot pressure in TD children was collected in 2- to 21-year olds.
The foot was divided into five sections: lateral forefoot, medial forefoot (MFF), lateral midfoot, medial midfoot (MMF), and the heel (Figure 1).4,7 The location-specific dynamic impulses from the forefoot and midfoot were used to calculate a coronal plane pressure index (CPPI). A high positive CPPI (maximum = 100) represents a severe valgus foot deformity in which all the pressure is in the medial segments. A high negative number (minimum = −100) represents a varus deformity in which all pressure is in the lateral segments.
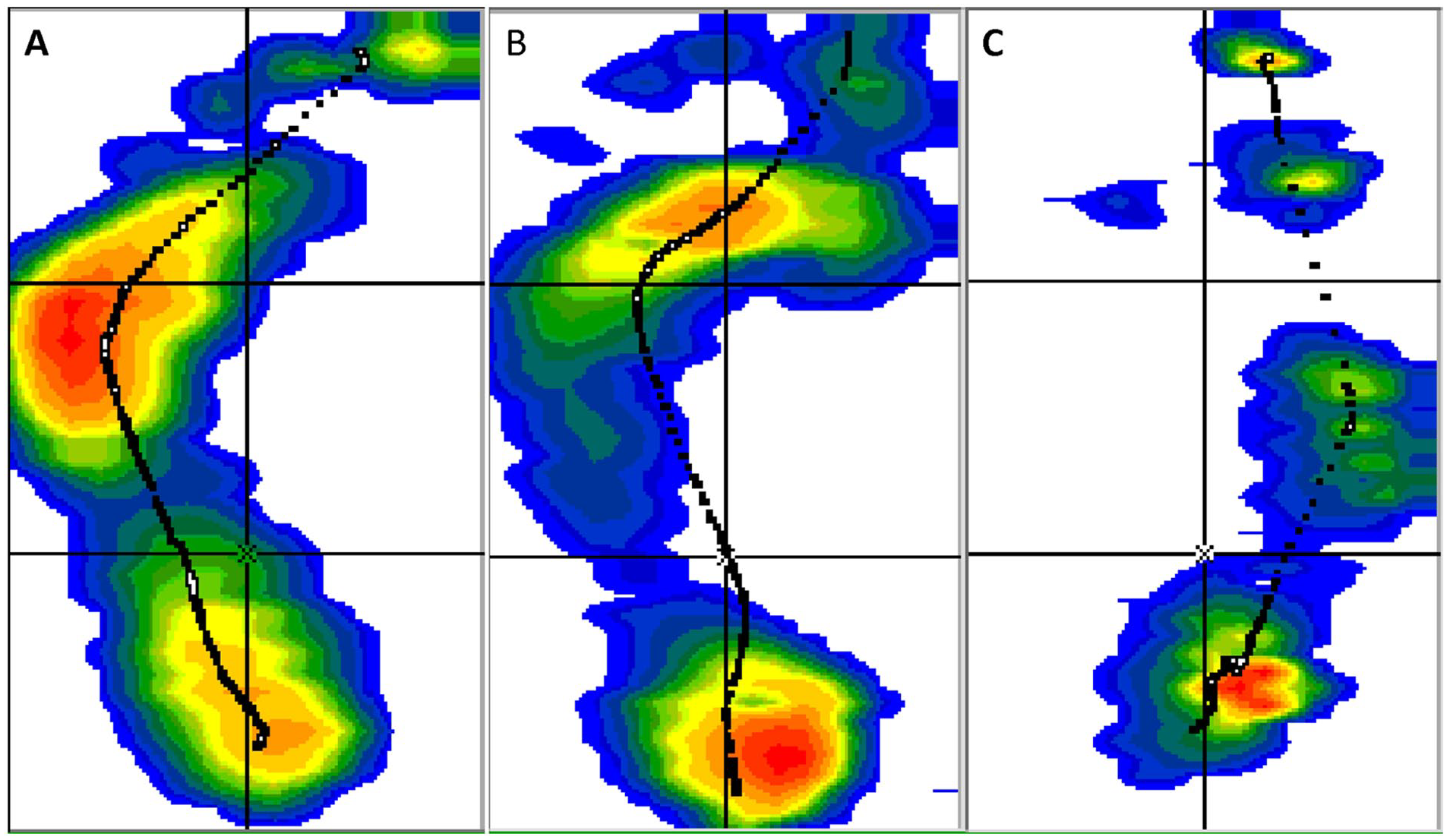
Dynamic pedobarographic results demonstrating (a) varus foot, (b) normal foot, and (c) valgus foot.
Foot pressure from the five segments and CPPI were compared between children with CP, stratified by GMFCS level, and TD children using locally weighted scatterplot smoothing (LOESS) averaging and serial Welch’s t-tests across time with Holm correction for multiple comparisons. 25 The group of children classified as GMFCS-IV was not statistically evaluated due to the small sample size. To understand the impact of orthopedic surgery on foot pressure, the change in CPPI pre-/post-surgery was compared with a paired t-test for children who underwent varus and valgus correction. A Fisher’s exact test was used to compare the relative frequency of no surgery/varus foot correction/valgus foot correction between children with unilateral and bilateral involvement. Variation in CPPI from each participant’s final visit stratified by GMFCS was evaluated by comparing with normative values to describe the frequency of normal (with 2 standard deviations (SD) of norm), varus (< 2 SD from norm), and valgus (> 2 SD from norm) feet.
Results
In 2003, 96 children with CP from our institution were enrolled in a broader long-term prospective study. However, 63 children from that cohort did not meet the inclusion criteria for the present analysis: 17 with involvement that was too severe to record reliable foot pressure data and 46 who did not reach participation targets, namely seven serial foot examinations over time. Meanwhile, 33 children met the inclusion criteria for this analysis. Of these, 13 children were GMFCS level I, 14 were II, 4 were III, and 2 were IV (Figure 2). However, 21 children had bilateral and 12 had unilateral involvement. In addition, 54 involved limbs were included in the analysis. Children were 2.9 (± 0.7) years old at baseline and 18.6 (± 1.7) years old at final evaluation. There were 525 total foot evaluations recorded with an average of 16.9 (± 4.4) evaluations per person and an average time between visits of 1.1 (± 0.4) years. The data of children with CP were compared with cross-sectional data from age-matched TD children (862 evaluations).
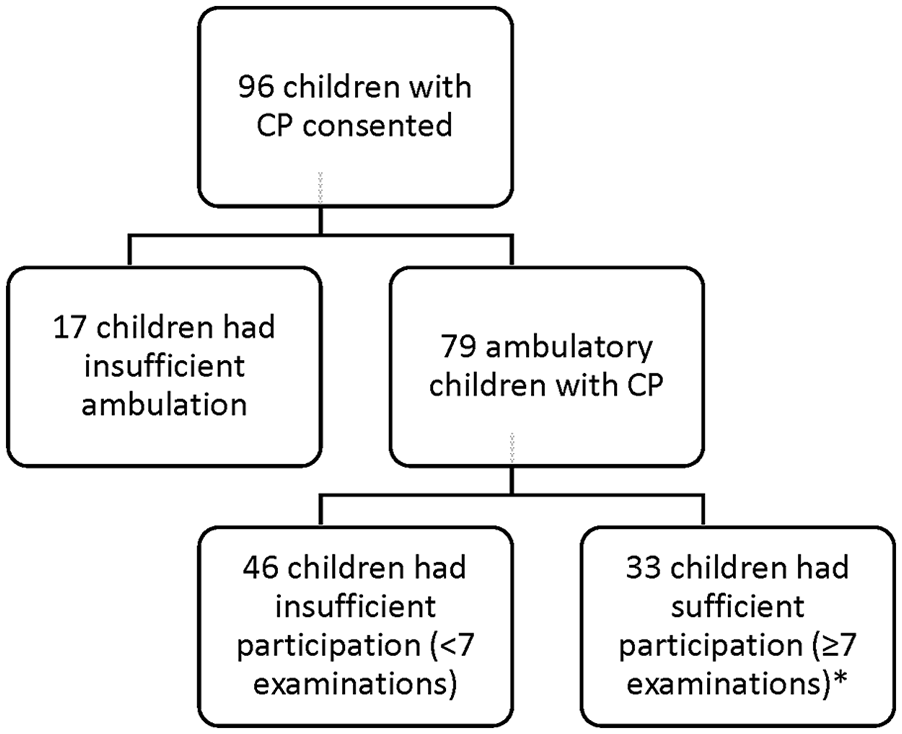
Flowchart showing the relationship between the study population and the initial study group. *GMFCS I: 13, II: 14, III: 4, and IV: 2 children. CP, cerebral palsy; GMFCS, Gross Motor Function Classification System.
Data on conservative interventions reveal that PT and bracing were most common during younger ages with 94% receiving PT and 82% using orthotics between the ages of 2 and 5 years. Over time, children with CP tended to receive less conservative treatment (Table 1), which decreased across all treatment methods with time.
Conservative management in ambulatory children with CP.
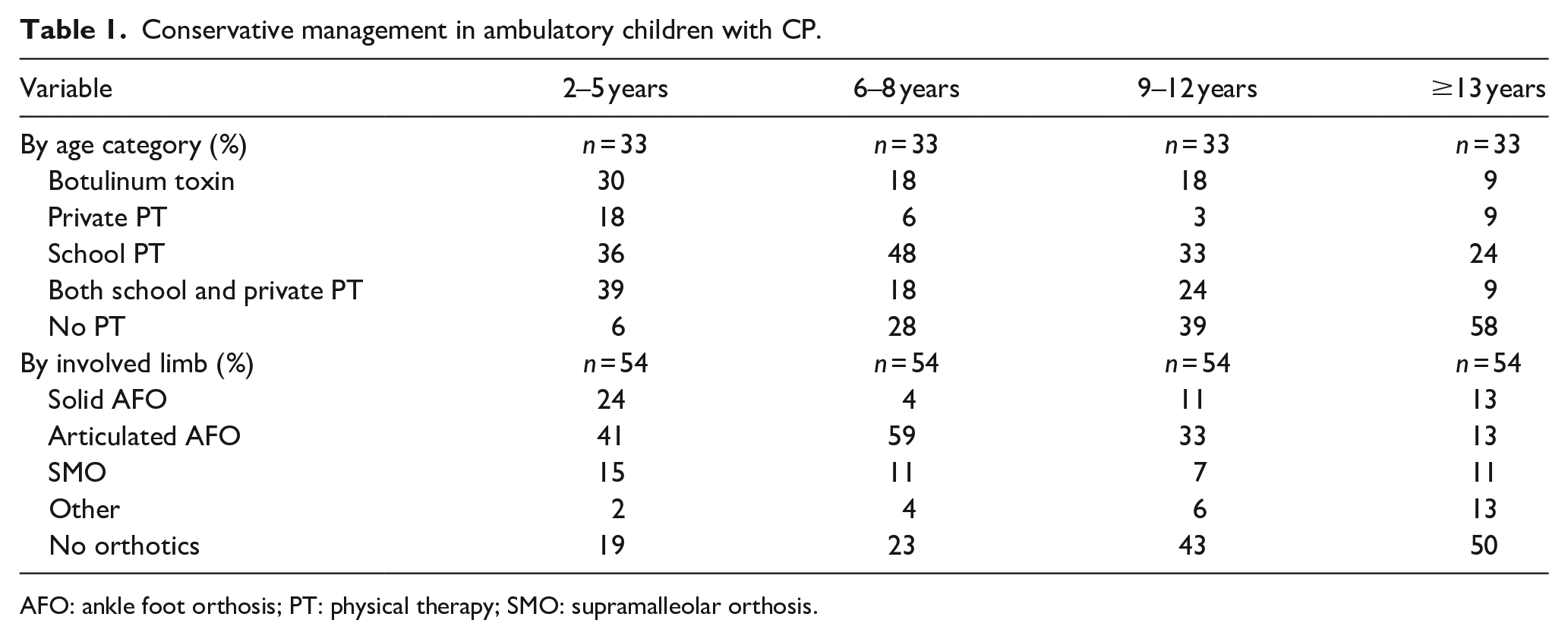
AFO: ankle foot orthosis; PT: physical therapy; SMO: supramalleolar orthosis.
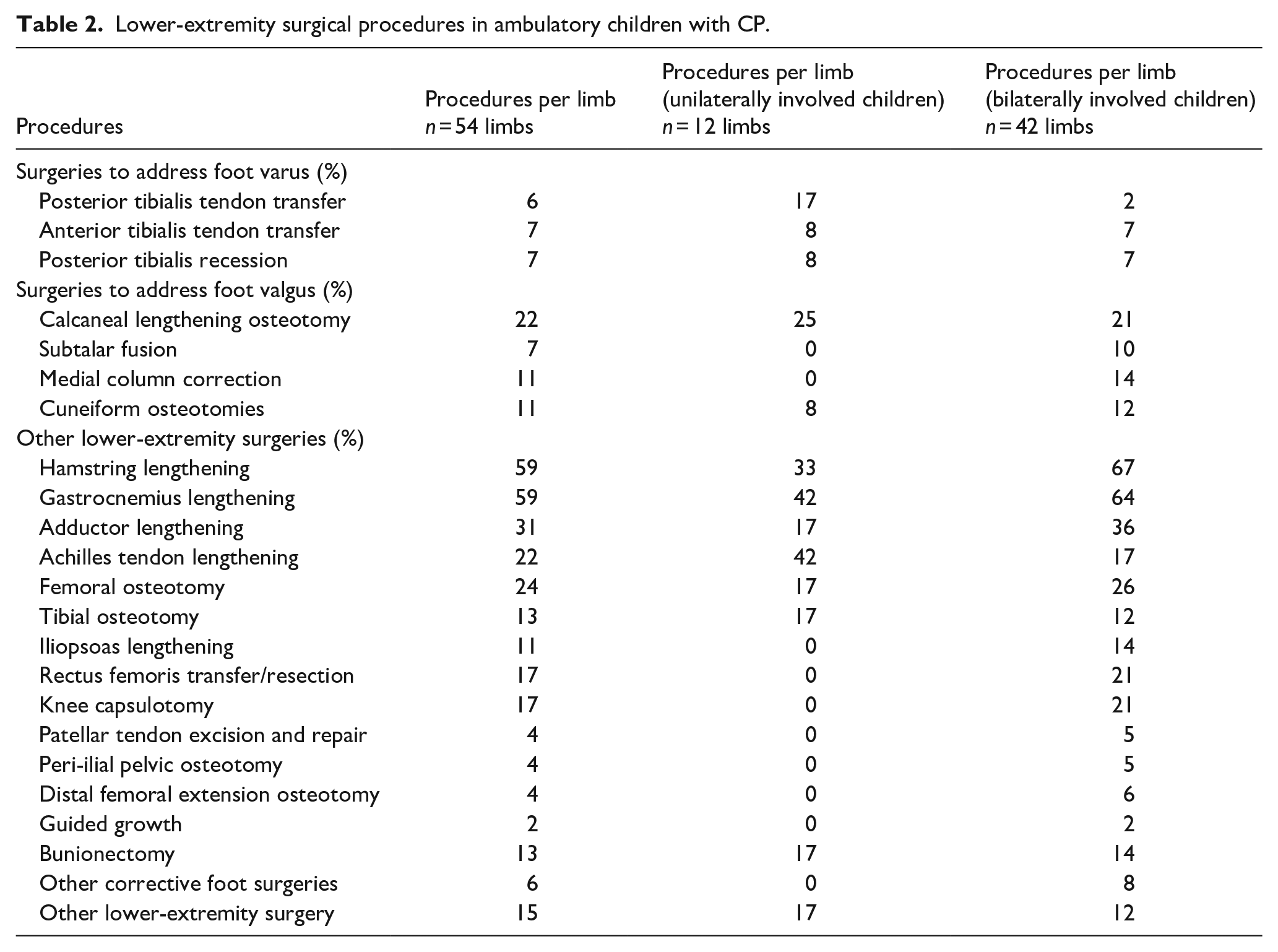
With respect to surgical outcomes, 82% of children underwent lower-extremity surgery (65 surgical events). Within the 65 events, 6 children had one surgical event, 12 had two, and 9 underwent three or more surgical events. Surgeries to address foot deformities specifically included 39 procedures on 17 children: 11 to address varus feet and 28 to address valgus feet (Table 2). However, 16 children did not receive varus or valgus foot corrective surgery, and 6 had no lower-extremity surgery. A variety of lower-extremity procedures were performed (Table 2). The CPPI improved from −64 (± 25.3) before to −16.5 (± 54.5) after varus corrective surgery (p = 0.05) and improved from 55.7 (± 23.7) before to 18.7 (± 44.7) after valgus corrective surgery (p < 0.05). However, 42% of unilaterally involved limbs received foot corrective surgery (17% varus, 25% valgus) and 43% of bilaterally involved limbs received foot surgery (10% varus, 33% valgus). No significant difference was found in frequency of varus and valgus procedures based on the pattern of involvement (p = 0.717).
Lower-extremity surgical procedures in ambulatory children with CP.
Regarding developmental trends, CPPI demonstrated abnormal pressure distribution in children with CP compared with TD children (Figure 3). Timing of varus (triangular tic marks) and valgus (circular tic marks) surgical correction is noted in Figure 3. With age, children classified as GMFCS levels II and III move toward a more normal foot posture. The GMFCS level I group showed no significant difference in CPPI over time compared with the TD group. The GMFCS levels II and III groups began in significant valgus but resolved to a foot posture not significantly different from normal CPPI (adjusted p < 0.05). Resolution of deformity and development of a more TD foot pressure took longer in children classified as GMFCS level III compared with GMFCS level II (level II approximate age 6 years, level III approximate age 10 years). Children classified as level IV followed a different trajectory, with progressive increase in valgus over time. There were no statistically significant differences in CPPI due to the small sample size (n = 2) in the level IV group, but both children had a persistent valgus tendency. No statistical difference in CPPI over time was shown between participants with unilateral and bilateral involvement (adjusted p > 0.05).
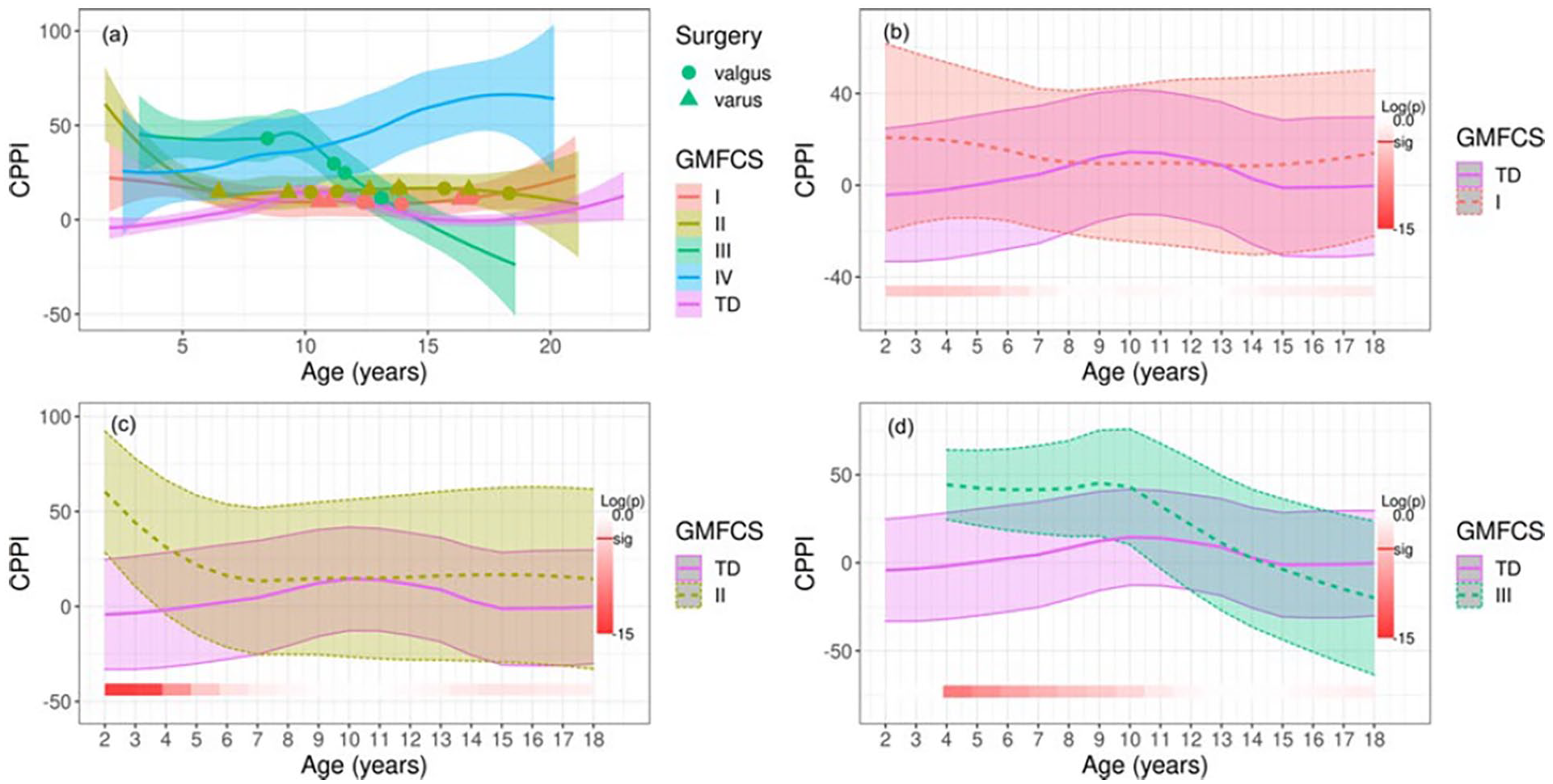
Longitudinal change in CPPI. Plot (a) demonstrates a comparison of mean CPPI over time with standard error among GMFCS levels with the TD group. The three remaining plots labeled (b–d) display each GMFCS level compared with the TD group with standard deviations. Standard errors are used for the first panel (a) rather than standard deviations to avoid excessive overlap of shading and to enhance clarity. The bottom bar highlights significance over time where a deeper red represents a higher level of significant difference. Log(p) is the logarithm of the p-value at each time interval.
Heel impulse was lower in children classified at all levels of GMFCS compared with TD children (Figure 4). As children aged, the difference in heel contact remained significantly different from TD children until around age 15 years in the level I group, around 18 years in the level II group, and around 9 years in the level III group (adjusted p < 0.05).
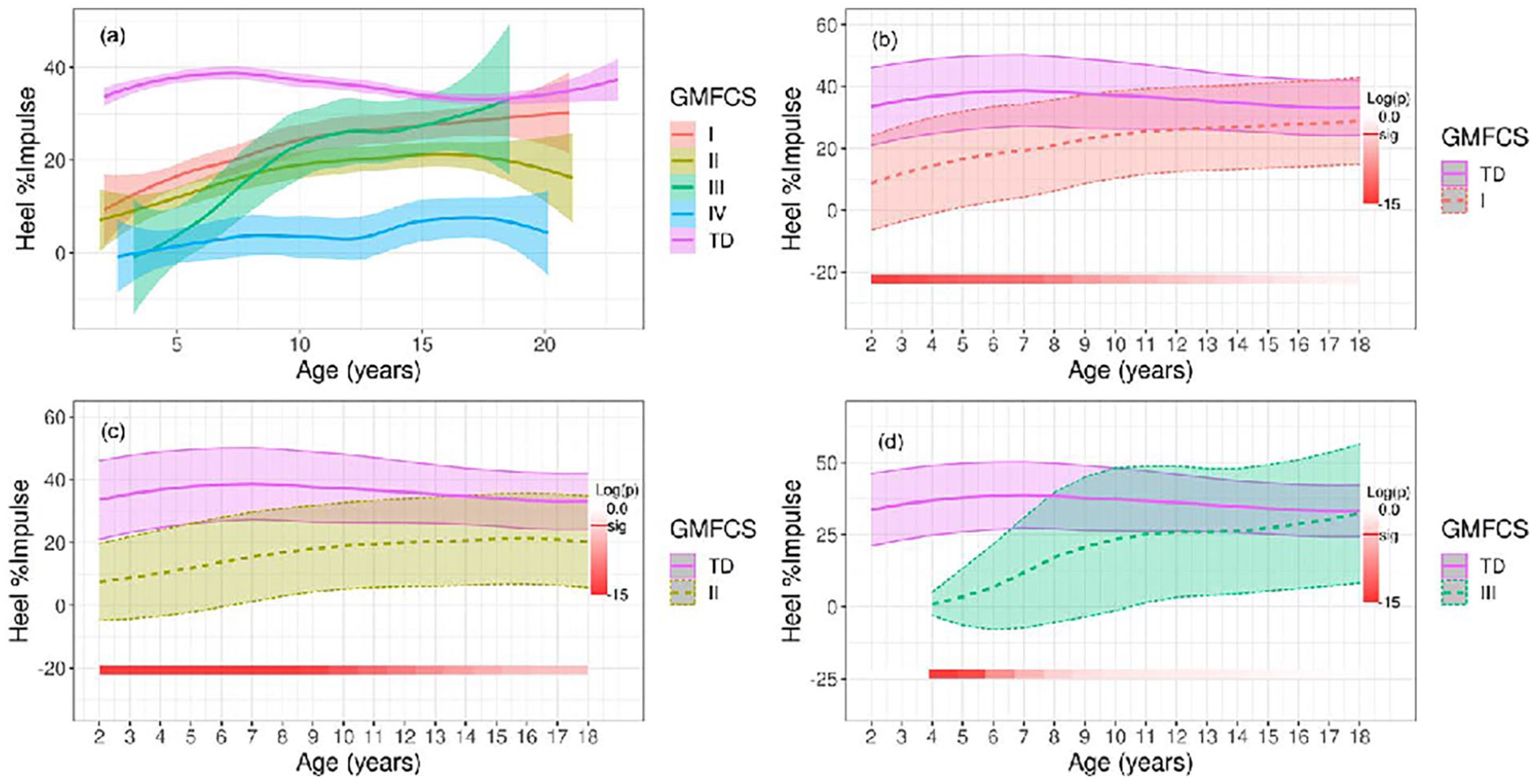
Longitudinal change in heel pressure in children with CP. Plot (a) demonstrates a comparison of mean heel impulse over time with standard error among GMFCS levels with the TD group. The three remaining plots labeled (b–d) display plots of heel impulse for each GMFCS level compared with the TD group with standard deviations. Standard errors are used for the first panel (a) rather than standard deviations to avoid excessive overlap of shading and to enhance clarity. The bottom bar highlights significance over time where a deeper red represents a higher level of significant difference. Log(p) is the logarithm of the p-value at each time interval.
Finally, abnormal foot posture in children with CP was also reflected in the segmental pressure allocation in the MFF (Figure 5) and MMF (Figure 6) (adjusted p < 0.05). Children in all GMFCS levels presented with high pressure in the MFF, which resolved over the course of growth, compared with the TD group. Children classified at levels I and II initially demonstrated high MMF pressure, which resolved. Children classified at levels III and IV began with normal MMF pressure due to toe walking patterns but had high MMF pressure, peaking around age 10 years. There were no significant differences between the groups in the lateral forefoot and lateral midfoot impulse (adjusted p > 0.05). The group differences tend to be most evident in the younger age groups, and with development, there was high variability in the evolution of foot posture. The trajectory of these changes could be very dramatic and we could not find predictive measures in the young children of 18–40 months old (Figure 7). At final visit, CPPI compared with normative data demonstrated in GMFCS I that 6% were varus, 72% normal, and 22% valgus; II that 8% were varus, 63% normal, and 29% valgus; III that 25% were varus, 63% normal, and 13% valgus; and IV that 0% were varus, 25% normal, and 75% valgus.
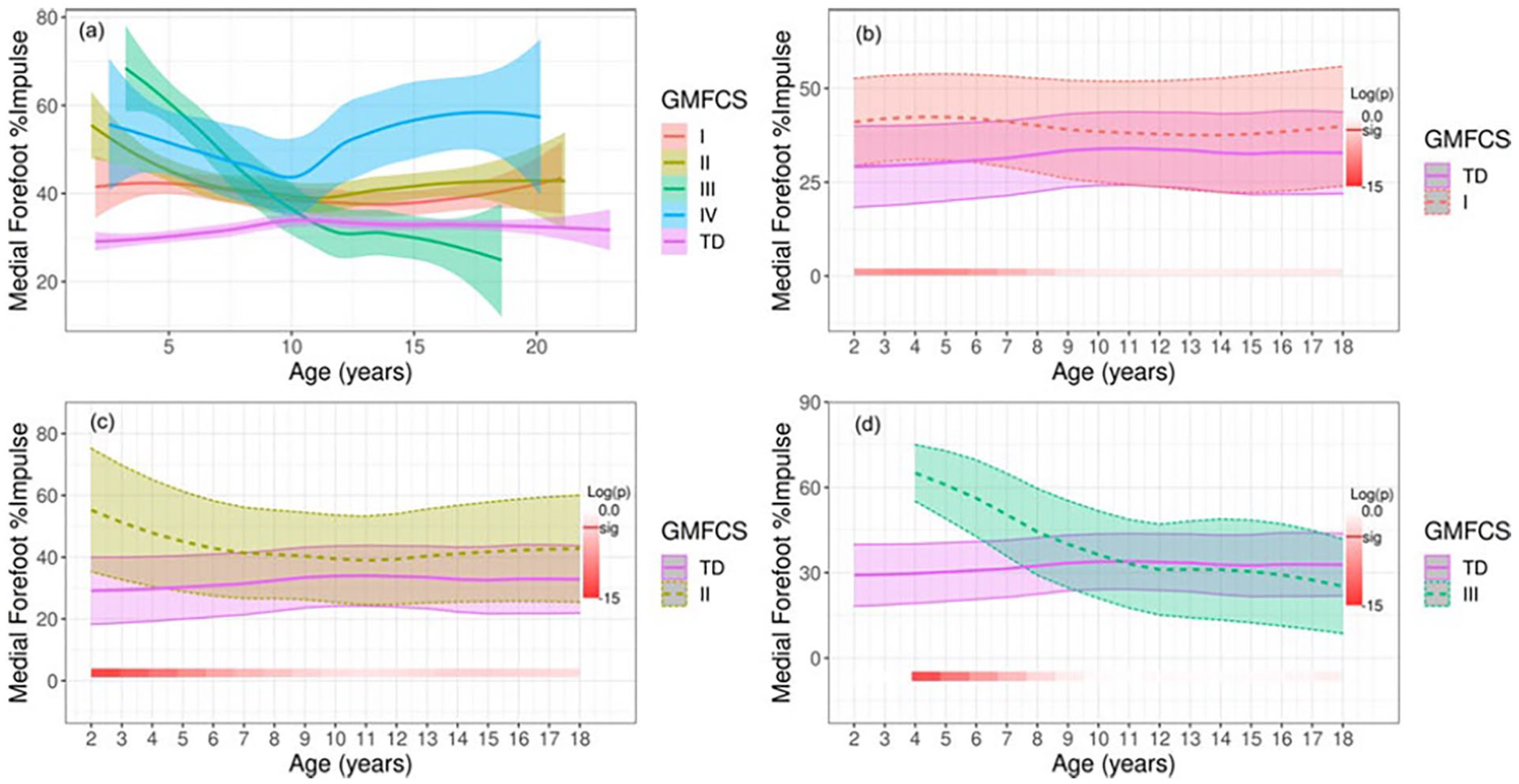
Longitudinal change in the MFF in children with CP. Plot (a) demonstrates a comparison of mean MFF impulse over time with standard error among GMFCS levels with the TD group. The three remaining plots labeled (b–d) display MFF impulse for each GMFCS level compared with the TD group with standard deviations. Standard errors are used for the first panel (a) rather than standard deviations to avoid excessive overlap of shadowing and to enhance clarity. The bottom bar highlights significance over time where a deeper red represents a higher level of significant difference. Log(p) is the logarithm of the p-value at each time interval.
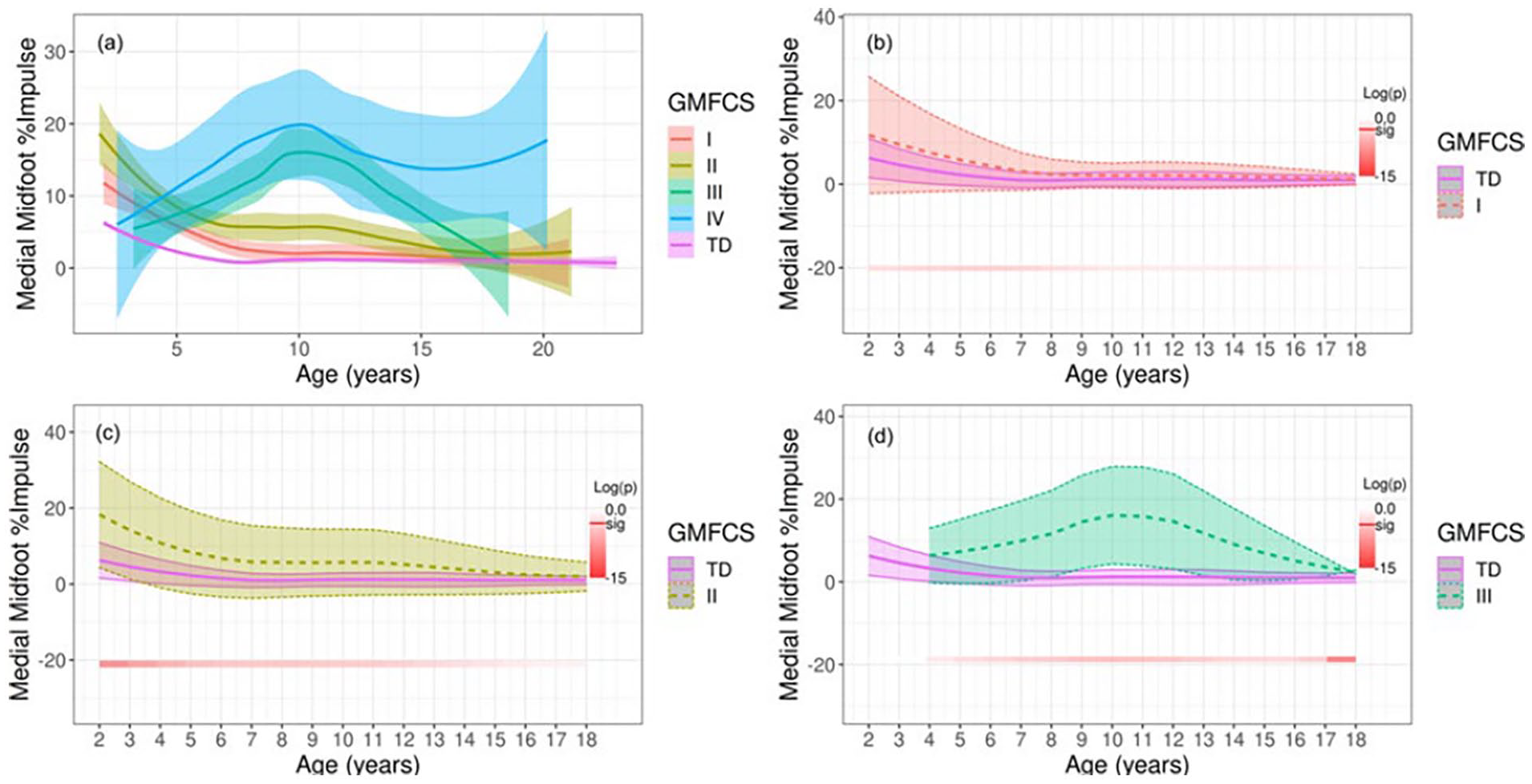
Longitudinal change in the MMF in children with CP. Plot (a) demonstrates a comparison of mean MMF impulse over time with standard error among GMFCS levels with the TD group. The three remaining plots labeled (b–d) display MMF impulse for each GMFCS level compared with the TD group with standard deviations. Standard errors are used for the first panel (a) rather than standard deviations to avoid excessive overlap of shading and to enhance clarity. The bottom bar highlights significance over time where a deeper red represents a higher level of significant difference. Log(p) is the logarithm of the p-value at each time interval.
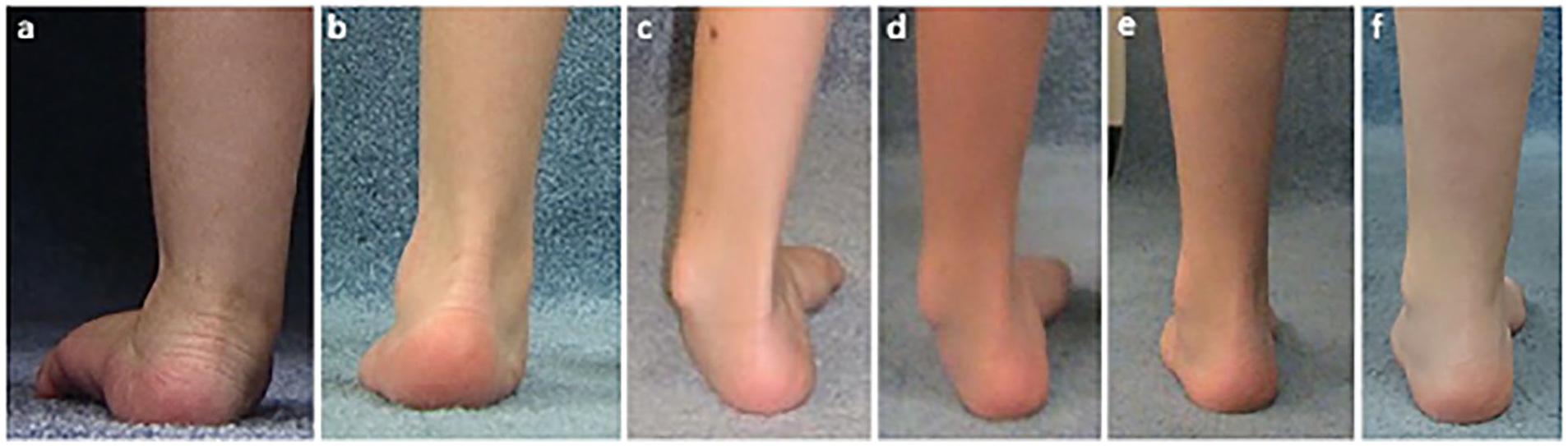
This girl presented at 2 years of age with a hemiplegic pattern, walking without external support. The main concern was (a) the severe left planovalgus foot, which was treated with a solid AFO. By age 4 years, the planovalgus was a (b) little better and the hinged AFO was continued. From age 4 to 6 years, her AFO was weaned as her foot improved, but then it continued into (c) varus. This required her to return to the AFO use until age 8 years when (d) the deformity was becoming more stiff with reduced AFO tolerance. At age 10 years, she had a gastrocnemius lengthening and a split tibialis posterior transfer. By age 14 years, she is brace-free with (e) improved foot posture, which continued to be (f) maintained with mild further improvement at age 21 years. This pattern of foot posture development from age 2 to 20 years is especially unpredictable in the younger ages.
Discussion
The progression or resolution of coronal plane foot deformities over time differs between children functioning at different GMFCS levels. TD children are born with flat feet and shift toward a neutral foot posture during early walking with medial arch development. 26 Children functioning at GMFCS level I follow a foot pressure trajectory similar to TD children, shifting from valgus to neutral at a young age. Children classified as GMFCS level II begin in a higher degree of valgus compared with TD children, and valgus resolution takes longer. Children classified at GMFCS levels III and IV tend to persist in valgus deformities that do not resolve until bony correction. Only one foot evaluated below the age of 3 years was determined to be in varus. Therefore, a young child presenting with varus foot deformity at this age should be considered to have another underlying pathologic etiology in addition to spastic CP.
Sagittal plane assessment reveals lower heel pressure in children with CP classified as GMFCS levels I–IV compared with TD children in early childhood. This is confirmed in previous reports, which found equinus as one of the most recognized foot deformities in children with CP leading directly to limited heel pressure.19,27 In addition to equinus, excessive knee flexion as seen in jump gait and apparent equinus gait could also contribute to low heel impulse.7,8 Lower heel pressure is present among all GMFCS levels but typically improves in GMFCS levels I–III with treatment. Surgical lengthening of plantar flexors14,28 and correction of flexed knee gait 29 contribute to increases in heel impulse.
Conservative treatment is the standard early management of foot deformities at our specialty center. Early PT is recommended to promote strength, limit contractures, and facilitate motor coordination, 30 which could contribute to arch development and improved heel pressure. An AFO is commonly used in combination with PT to support a neutral foot posture and provide a stable plantigrade foot-to-floor contact. 1 While AFO have proven benefits, the goal at our center is to wean children from braces with time (82% in orthotics at age 2–5 years, 50% in orthotics at age ≥ 13 years) when the potential for strengthening is present to allow opportunities for functional activities, such as stair climbing and transitions. 31 Conservative management of foot deformities is definitive in some children (typically GMFCS I and II, where 52% received no foot surgery), but in others, it serves to extend the time until surgical intervention when, with deformity progression and weight gain, the child is no longer able to tolerate orthotic support.
Surgical intervention can have a dramatic impact on foot deformities in children with CP.15,32 Telléus et al. 18 describe foot and ankle surgeries as the most common procedures in people with CP between the ages of 2 and 25 years, accounting for 49% of procedures in those classified as GMFCS level I, 54% of people classified as level II, and 40% in those classified as level III. Our study shows comparable results where 35% of surgeries in children classified as level I, 29% classified as level II, and 40% as level III included foot correction procedures. In this study, participants classified as GMFCS level IV had not yet undergone foot corrective surgery due to limited functional demand and braceable deformities. Planovalgus correction is common for youth at GMFCS level IV at our institution, with goals of maintaining braceable feet for pain-free standing and transfer function.
Traditionally, valgus deformities are associated with bilateral CP and varus deformities are associated with unilateral CP.6,15,19 A foot pressure study by Galli et al, which looked at foot pressure in children with CP between the ages of 5 and 13 years, showed more frequent varus presentations in hemiplegic children compared with diplegic children; however, valgus was the most common deformity in both groups. 8
In the current study, the frequency of valgus and varus correction in children with unilateral involvement (17% varus, 25% valgus) compared with bilateral involvement (10% varus, 33% valgus) was not different, but when the pattern of involvement and GMFCS level were considered in combination, significant trends emerged. Children classified as GMFCS level III were all bilaterally involved and 100% of these children underwent valgus correction. In children classified as GMFCS levels I and II with bilateral involvement, 27% underwent varus correction. Of those who underwent varus correction, all but one presented with asymmetric lower-extremity involvement, which may predispose the development of varus deformity.
The optimal timing of surgical intervention in children with CP is difficult to determine.16 –19 With a lack of knowledge on the evolution of foot posture during childhood, it is a challenge to predict improvement or progression of deformity. Poorly timed surgery poses a threat of deformity recurrence or overcorrection with the potential need for revision surgery. 27 At our center, surgical foot deformity correction is performed only after bracing becomes intolerable due to progressive deformity, which in children at GMFCS level I–II was age 13.0 (± 3) years (tendon lengthening /transfer or bony correction), and at level III, it was age 11.8 (± 2.4) years (bony correction). Only two varus corrections were completed below age 10 years and only one valgus correction occurred in a child below age 10 years (Figure 1(a)). Development of foot deformity in early childhood is very variable and hard to predict as demonstrated by a typical case from this study. The young child went from early severe planovalgus to a varus foot in late childhood (Figure 5). Many of these children need plantar flexor lengthening in middle childhood, and the response to the foot posture is unpredictable; sometimes planovalgus gets worse, sometimes it gets better, and sometimes it can convert to varus as noted in the example in Figure 5. Surgical decision-making should be made based on longitudinal data in collaboration with the child and family. While early surgery should be avoided when possible, it is important to avoid the development of severe fixed deformity or functional loss due to foot position.
While children in this study were stratified according to pattern of involvement and GMFCS classification, both are continuous and neither can solely predict progression of deformities. Variation in functionality presents within GMFCS levels and in some cases, classification is difficult, particularly in young children. 23 Uncertainty in early classification provides additional justification to employ conservative management and delay surgical intervention.
Limitations exist within this prospective longitudinal study. The small sample size is largely due to the long participation required by children and families. Trends may not be applicable to children receiving care at other institutions or children who do not have access to specialized pediatric orthopedic care. However, the data provide comparable information for future studies. Quantitative measures in this study were restricted to foot pressure data, which may be affected by foot, ankle, knee, hip, pelvis, and trunk, but do offer a functional assessment of how the foot interacts with the ground, leading to functional stability. Multiplanar proximal malalignment (i.e., crouched gait and rotational malalignment) will have impact on foot posture and future studies should include a full-body segmental three-dimensional dynamic analysis. Participants in the study received individualized, conservative, and invasive treatment as determined by expert clinicians and are, therefore, not a natural history. Obtaining natural history data through the completion of growth would be ideal; however, in setting up this study, we realized that it would both be unethical to withhold treatment that we felt was medically indicated and that parents would not consent to such a study.
In conclusion, this study represents the longest-term prospective report of foot posture development in youth with CP. Youth with CP present with abnormal foot pressure compared with youth with typical development. Children classified as GMFCS levels I–IV begin walking in valgus foot posture; those at levels I and II tend to normalize throughout development while those at levels III and IV persist in valgus until surgical intervention. Conservative management starting at an early age is recommended with surgical intervention at later ages for persisting deformities that resist conservative management. The description of foot deformity management foot posture and progression over the course of growth can be used to guide treatment and educate families on expected outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231208746 – Supplemental material for Changes in foot posture evaluated with dynamic pedobarography over the course of childhood in ambulatory youth with cerebral palsy
Supplemental material, sj-pdf-1-cho-10.1177_18632521231208746 for Changes in foot posture evaluated with dynamic pedobarography over the course of childhood in ambulatory youth with cerebral palsy by Chris Church, Nancy Lennon, Madison Lennon, John D Henley, Thomas Shields, Tim Niiler, Daveda A Taylor, M Wade Shrader and Freeman Miller in Journal of Children’s Orthopaedics
Footnotes
Author contributions
C.C., N.L., M.W.S., and F.M. made substantial contributions to conception or design of the work. All authors participated in acquisition, analysis, or interpretation of data for the work. C.C., N.L., and M.L. involved in drafting the work. All authors participated in revising the work critically for important intellectual content; approved the final version to be published; and investigated and resolved the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriate.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication made possible in part by support from the Nemours Grants for Open Access from Library Services.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.