
Abstract
Purpose:
We compared the outcomes of arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in 31 adolescents with cerebral palsy, using three different methods of fixation: K-wires, non-locking plates, and locking plates.
Methods:
Clinical outcomes included time to weight-bearing, fusion rates and surgical complications. Radiographic assessment included comparing pre- and post-operative hallux valgus angles, intermetatarsal angles, interphalangeal angles, and lateral metatarsophalangeal angles. Patient-reported outcomes included pre- and post-operative visual analogue scales addressing bunion pain and concerns, difficulties with wearing shoes and braces, and difficulties with foot hygiene.
Results:
Of the 31 adolescents (16 male), 10 patients had K-wire fixation, 11 had a non-locking dorsal plate, and 10 had fixation with a dorsal locking plate. Mean age at surgery was 16 years (12–18 years) and mean follow-up was 4 years (2.7–6.5 years). Patients with K-wire fixation had delayed weight-bearing and had more complications than those managed by dorsal plating. There were significant improvements in radiographic parameters (except interphalangeal angle) and in patient-reported outcomes, in all groups (p < 0.001). However, radiographic and clinical outcomes were better in the dorsal plating groups compared to the K-wire group.
Conclusion:
Arthrodesis of the first metatarsophalangeal joint gave good correction of deformity with improvements in symptoms and radiographic parameters in adolescents with cerebral palsy. We recommend dorsal plating that allowed early weight-bearing and had fewer complications with better clinical and radiographic outcomes, than K-wire fixation.
Level of evidence:
IV: Retrospective case series.
Introduction
Deformities of the foot and ankle are common in children and adolescents with cerebral palsy (CP) and are acquired during growth and maturation. 1 The most common deformities associated with pes valgus are ankle valgus and hallux valgus (HV).1,2 HV is common in ambulant adolescents with CP who have bilateral involvement, a spastic, or mixed tone muscle disorder, equinus deformity, pes valgus, and disordered gait biomechanics. 3 Poor clearance during swing phase is associated with toe scuffing and laterally directed forces during walking. 3 Muscle imbalance and disordered gait biomechanics may predispose children with CP and pes valgus to develop HV at early age.1 –3
HV is the most common forefoot deformity in children with CP with onset at an earlier age than in the typically developing population.3,4 Symptoms are often mild in younger children but may increase around the time of the adolescent growth spurt, as the severity of the deformity increases.1 –4 Typical symptoms include pain and cosmetic concerns about the bunion, impaired gait and functional ambulation, problems maintaining foot hygiene and difficulty with shoe wear or using an orthosis.1 –4 Surgery may be indicated where there are significant symptoms, usually a combination of pain, cosmetic concerns, and impaired function. Joint sparing surgery, such as combinations of soft tissue balancing and corrective osteotomies, can be successful in the short term, in high-functioning adolescents with mild CP, Gross Motor Function Classification System (GMFCS) I and II.5 –7 Non-fusion surgery, especially soft tissue procedures or isolated bunionectomy, can be associated with high recurrence rates and lower patient satisfaction in this patient population.5 –7 Metatarsophalangeal joint (MTPJ) arthrodesis is an accepted method for the primary treatment of HV in adolescents and young adults with CP and severe, symptomatic deformities. 8 Prior studies have reported good outcomes in terms of pain relief, deformity correction, and patient satisfaction.8,9
The majority of studies have reported fixation techniques, similar to those used in the typically developing, adult population. These include K-wires, solid screws, cannulated screws, and dorsal plates.8,9 Historically, at our institution, first metatarsophalangeal (MTP) arthrodesis was performed using K-wire fixation followed by a 6 weeks in a cast and up to 12 weeks of non–weight-bearing, as previously described. 9 Over time, our technique has evolved from using K-wires to dorsal non-locking plates and then to locking plates. 10 When plate fixation was introduced, we also changed the method of joint preparation to include the use of hemispherical cup and cone reamers, as described by Coughlin and his colleague Grimes.11,12 These trends in fixation are similar to those reported in the typically developing adult population.13,14 The aim or this study was to compare patient-reported outcomes (PROMs), surgical complications, and radiological results of three types of fixations used at our institution for first MTP arthrodesis in adolescents with CP.
Material and methods
A retrospective analysis was performed on data, which had been collected prospectively, for adolescents with CP who had received first MTP arthrodesis surgery for HV between 2000 and 2019, at a single tertiary level, children’s hospital. Ethical approval for the study was given by the institution’s Ethics in Human Research Committee, approval number 29151. No external funding was received.
Inclusion criteria were a diagnosis of CP with registration on the state-wide CP register, arthrodesis of the first MTPJ in one or both feet and baseline, and follow-up radiology at a minimum follow-up of 30 months post-operatively. Exclusion criteria were absence of baseline or follow-up radiographs and patients lost to follow-up before 30 months.
Patients were classified according to their functional level using the GMFCS, as well as their movement disorder (spastic, dystonic, or mixed) and topographical distribution (hemiplegia, diplegia, triplegia, and quadriplegia). 15 Ten-point visual analogue scales (VASs) were used to record PROMs in three domains: pain and cosmetic concerns over the bunion/medial callosity, difficulties with shoe and brace wear, and problems with foot hygiene. 16 The three scales ranged from “None” to “Very Severe” and are shown in Supplemental Appendix 1. The content of the questions was derived from interviewing patients with severe HV about their concerns. A clinical example of a patient with severe HV deformity is shown in Figure 1, with post-operative photograph shown in Figure 2. Many adolescents found it difficult to distinguish concerns about bunion pain from deformity concerns, as described in a previous review. 2 For this reason, bunion pain and bunion concerns were posed as a single question. 2 PROMs were recorded prior to surgery and at final follow-up, at a transition clinic appointment. 17 PROMs data were recorded by telephone interview or email, when direct report from the outpatient clinic was missing.

Adolescent male, age 15 years, GMFCS Level IV. Severe bilateral hallux valgus with severe pes valgus. The hallux underlies the lesser toes and reaches as far laterally as the fourth toe. Hallux valgus angles were 64° and 72°, and VAS scores were 8, 9, and 6. The patient was unable to tolerate AFOs or regular shoes and was restricted to wearing slippers to school. Management was bilateral talonavicular fusion and bilateral first MTP fusion with dorsal locking plates.

Post-operative clinical photographs, of the same patient (Figure 1). The medial border of the first ray is corrected with good correction of hallux valgus and pes valgus. Post-operative hallux valgus angles were 7° and 6°. VAS scores were 1, 0, and 0.
A total of 31 patients were evaluated in this study including a total of 59 operations with most patients receiving bilateral surgery. Three groups were identified: planar joint preparation and K-wire fixation, cup and cone reaming for joint preparation, and either non-locking mini-fragment plate fixation (Luhr, Howmedica, Rutherford, NJ, USA), or locking low-profile, contoured plate fixation (Acumed®, Hillsboro, OR, USA). There were 10 patients in the K-wire group, 11 patients in the non-locking plate group, and 10 in the locking plate group.
Radiographic evaluation was based on weight bearing radiographs taken pre-operatively and at the latest follow-up. Parameters measured included hallux valgus angle (HVA), intermetatarsal angle (IMA), interphalangeal angle (IPA), and lateral metatarsophalangeal angle (LMTPA) using previously described methods.3,8 Measurements were made using tools in the picture archiving and communication system (PACS) and transferred to an Excel spreadsheet. Measurements were made by a research fellow and a senior surgeon, and the results averaged.
Prior and concomitant surgery to the foot and ankle were extracted from hospital records. Post-operative complications were noted and graded using a Modified Clavien–Dindo (MCD) system. The MCD system has defined grading criteria to enhance objectivity, reduce bias and has been shown to have good reliability. 18 Previous studies have shown that there is little change in radiological parameters between short and long-term follow-up, if the arthrodesis is sound. 8
Statistical analysis was performed using IBM SPSS statistics software (version 29.0.0.0) and results displayed as mean, median, standard deviation, or range. Statistical significance was analyzed using the Student’s t-test for unpaired data with a statistical significance assigned to p values < 0.05. Statistical comparison of data from more than two groups was completed using the Kruskal–Wallis test, with subsequent intergroup comparison using the Mann–Whitney test.
This study has been assessed for accuracy and completeness using the Equator STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guideline criteria (see Supplemental Appendix 2).
Surgical techniques
The surgical indication for correction of HV deformity included HVA greater than 30 degrees, with symptoms referable to the bunion, present for at least 12 months and refractory to non-operative measures, such as brace or shoe wear modification. Equinus and valgus deformities were evaluated and corrected prior to first MTP fusion in 27 patients, usually as part of multilevel surgery.1 –3,8 Equinus correction was dose-based depending on patient condition, with diplegic patients receiving gastrocnemius recession with or without soleal fascia lengthening. Of the three patients with hemiplegia, two had modified Vulpius lengthening and one had Achilles tendon lengthening. Of the 25 patients with diplegia, 16 had calcaneal lengthening osteotomies (CLOs), 3 had subtalar fusion, and 2 had talonavicular fusions. Two patients with hemiplegia had CLO. The patient with triplegia had talonavicular fusions and one patient with quadriplegia had subtalar fusion and talonavicular fusions.
Four patients had correction of severe pes valgus by subtalar fusion or talonavicular fusion, at the same time as bilateral first MTP fusion. Two were functioning at GMFCS Level III and two at GMFCS Level IV. 15
Surgery was performed under general anesthesia, supplemented by local nerve blocks. Perioperative intravenous antibiotics were given and a sterile tourniquet was used to achieve a bloodless field. The incision and surgical approach were similar in all three groups. A dorsal, curvilinear skin incision was used extending from the level of the interphalangeal joint distally and extending proximally for a distance of 6 cm along the dorsum of the first metatarsal. The incision was deepened along the medial border of the extensor hallucis longus (EHL) tendon, with identification and protection of cutaneous nerves, and mobilization and retraction of the EHL tendon. 9 The first MTPJ was mobilized by incision of the joint capsule and the collateral ligaments, so that, the joint could be dislocated to prepare the articular surfaces for fusion. In all groups, the medial exostosis was reduced in size using rongeurs and in the plating groups, with a hole saw matching in size, the selected cup and cone reamers11,12 (Figure 3). In the K-wire group, the joint was prepared for fusion using rongeurs and small osteotomes to remove articular cartilage, as previously described. 9 The goal was to produce matching planar surfaces maintaining the length and shape of the metatarsal head and the base of the proximal phalanx. The joint was reduced manually and stabilized with two 1.8 mm crossed K-wires (Figure 4). The position of the wires was checked using fluoroscopy and the wire tips were bent close to the exit point and protected by gauze padding. In both dorsal plating groups, appropriately sized, cup and cone reamers were used to remove articular cartilage and to produce matching convex and concave surfaces. Care was taken to limit the amount of subchondral bone removal, especially in patients with osteopenia. In the Luhr (Vitallium) plate group, a four-hole plate was pre-bent by approximately 10–15 degrees (provides extension) and applied to the dorsal surface of the first MTPJ with an assistant holding the joint reduced under compression, as previously described11,12 (Figure 5). The Luhr plates are 2.7 mm mini-fragment Vitallium plates, originally designed and used in maxillofacial surgery.11,12 In the locking plate group, six-hole low-profile plates were used with a preset dorsiflexion angle of 9 degrees and a HVA of 10 degrees, as previously described 10 (Figure 6). In all three groups, fluoroscopy was used to check the position of the implants and the radiographic alignment of the first MTPJ after fixation. Alignment was checked clinically and fluoroscopically aiming for 5–10 degrees of valgus, 5–10 mm of clearance of the tip of the hallux with the foot plantigrade, equating to an LMTPA of approximately 20 degrees with neutral rotation, in all cases. Hallux clearance was checked using a sterile metal plate applied to the plantar surface of the foot and dorsiflexing the ankle to 90 degrees dorsiflexion. 8 The aims were to provide sufficient dorsiflexion to permit clearance in gait, with the foot and ankle plantigrade, allowing for the fact that many adolescents with CP have a degree of drop foot in swing. 15 In both plating groups, temporary fixation was achieved with a percutaneous K-wire before definitive fixation with screws inserted through the plate holes. In the locking plate construct, only the distal screws in the proximal phalanx were locked. Dynamic compression was achieved using eccentric screw placement in the proximal screws. This technique using angular stable implants proven to be safe and favorable at different anatomical levels in children with CP.
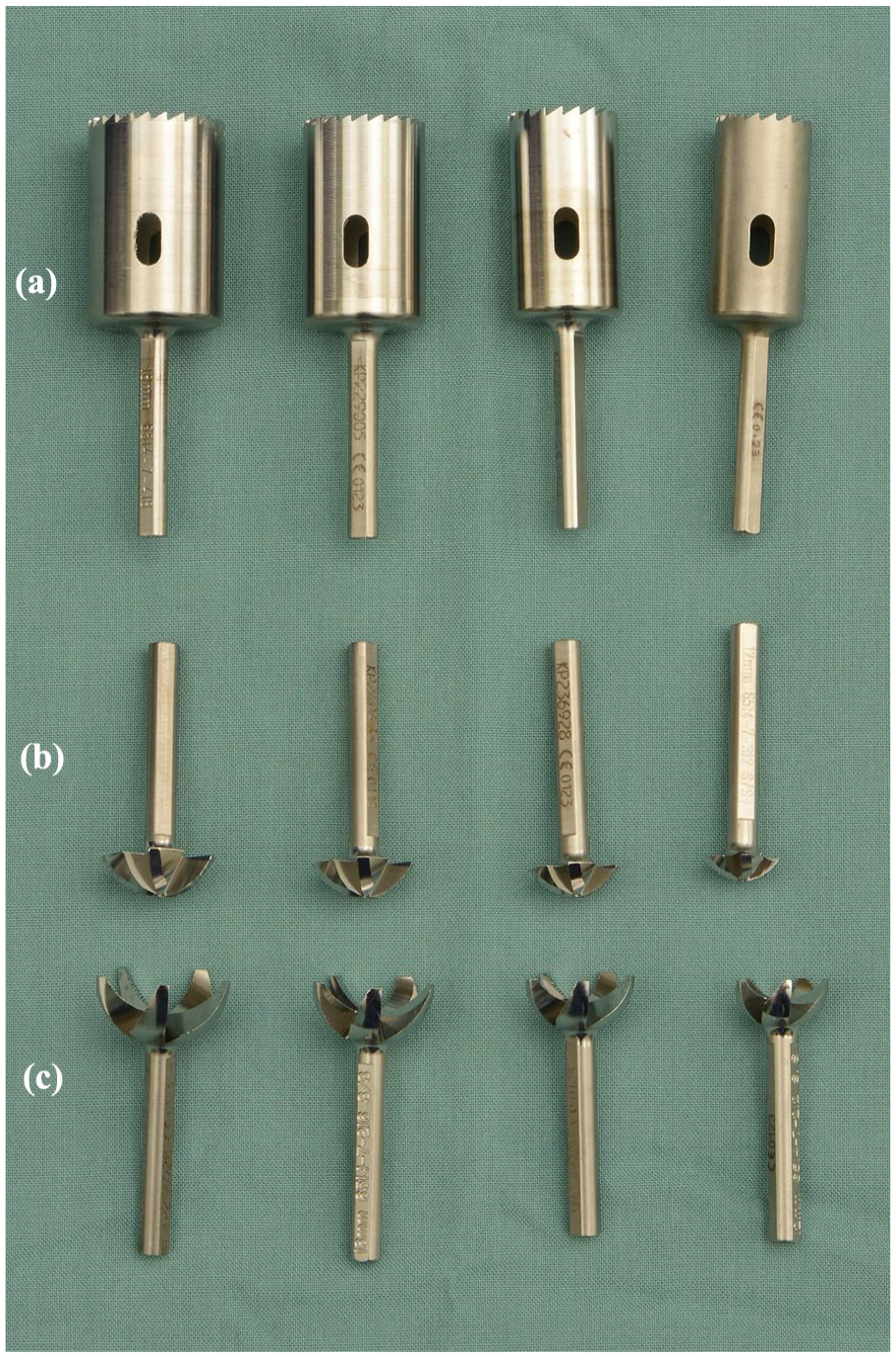
Hole saw and cup, and cone reamers, used for joint preparation in the dorsal plating groups. Four sizes are available for each set: (a) Hole saw. (b) Convex reamer (base of proximal phalanx). (c) Concave reamer (head of first metatarsal).
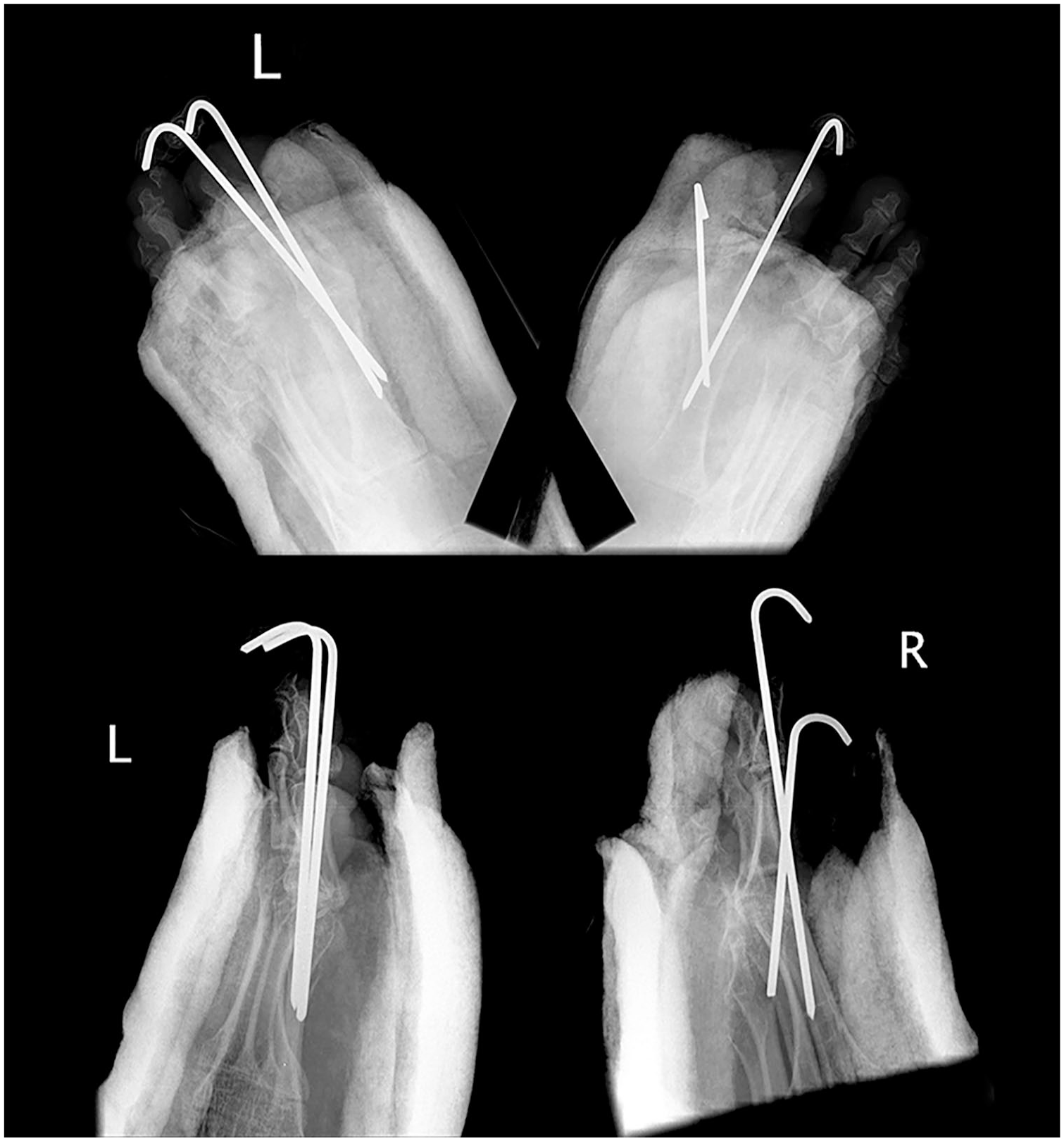
Post-operative AP (top) and lateral radiographs (bottom) after bilateral correction of hallux valgus and crossed K-wire fixation. It can be difficult to get stable fixation in the metatarsal and maintain adequate dorsiflexion at the arthrodesis site, using a straight K-wire.

Post-operative AP (top) and lateral radiographs (bottom) after bilateral correction of hallux valgus. Joint preparation was with cup and cone reamers and four-hole, Luhr plate fixation.
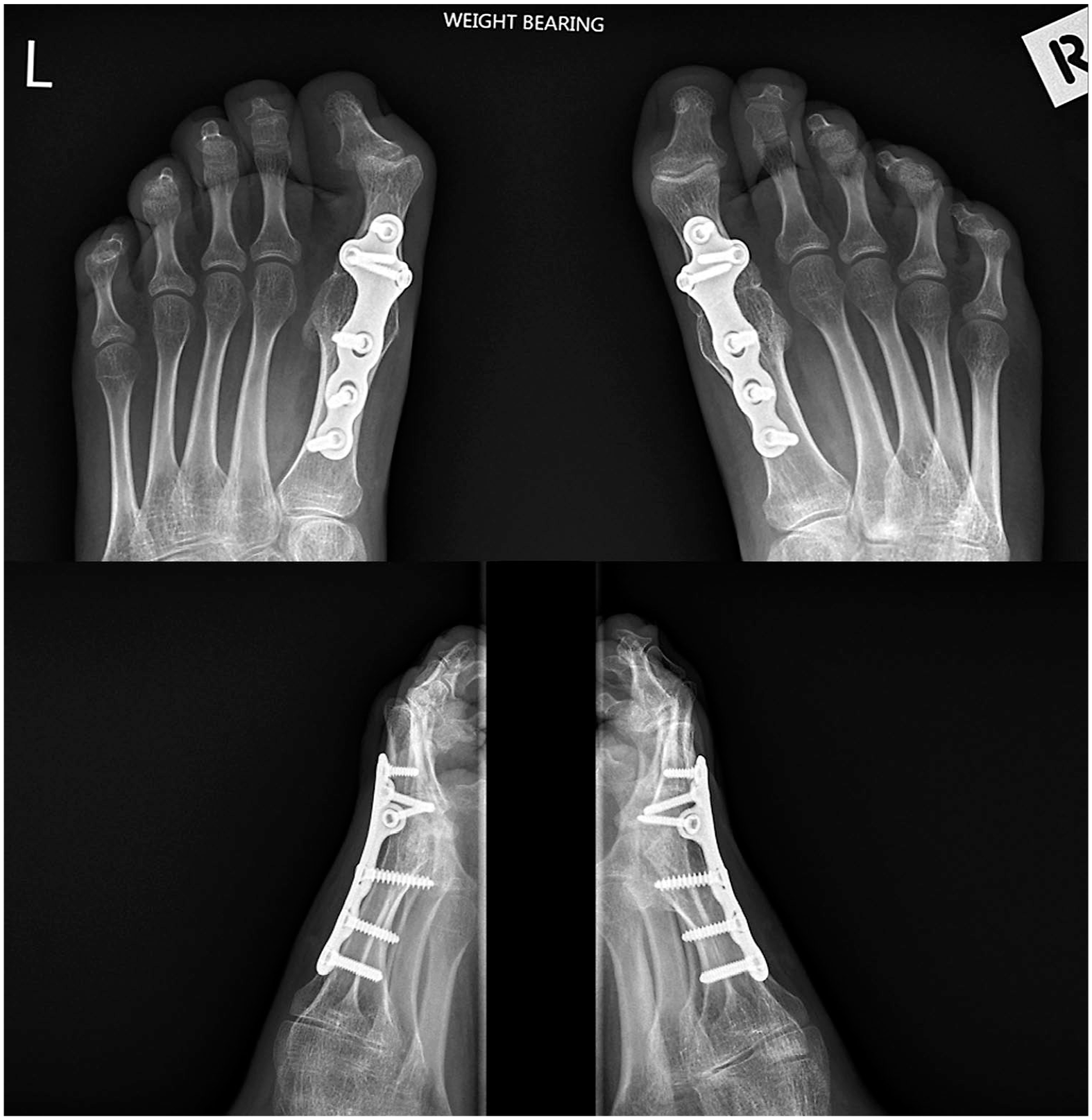
Post-operative AP (top) and lateral radiographs (bottom) after bilateral correction of hallux valgus and fixation with six-hole locking plates. The intermetatarsal angles improved after surgery, but the interphalangeal valgus increased and the left side was symptomatic. A tight FHL may have contributed to the interphalangeal valgus and flexion.
The incisions were closed in layers after deflation of the tourniquet and hemostasis. The skin was closed with interrupted nylon sutures to reduce the risk of wound dehiscence. Well-padded, below knee casts were applied in all groups, with the foot plantigrade. The forefoot section of the cast was reinforced with fiberglass.
Post-operative weight-bearing protocols varied according to the perceived stability of fixation, as follows. The K-wire group was advised to be non–weight-bearing, for 6 weeks, except for essential transfers. The casts were removed after 6 weeks, when follow-up radiographs were obtained and the K-wires were removed in the outpatient clinic. 9 Weight-bearing was then individualized according to the degree of bone healing on the 6-week radiographs, after cast removal.
The Luhr plate group was advised to have 3-week non–weight-bearing, followed by 3-week weight-bearing as tolerated. The locking plate group was permitted full weight-bearing as tolerated after 1 week of elevation. Bony healing can be difficult to assess after the use of cup and cone reamers.11,12 All groups were advised to use ankle foot orthosis (AFO) protection during all weight-bearing activities until a minimum of 6 months after surgery.
Results
The mean follow-up time was 48 months (range: 33–77 months). Thirty-one patients who were included in this study were registered on the state-wide Cerebral Palsy Register and follow-up of patients were facilitated by the mandated necessity for adolescents to attend a transition clinic prior to transfer to adult services. During the study period, two adolescents who lived in other states, had follow-up of 9 and 15 months respectively, however, they were not available to long-term review and were therefore excluded from this study.
Demographics
The mean age at time of surgery was 15 years and 10 months (range: 12 years and 1 month–18 years and 7 months). From the 31 patients in this study, a total of 59 primary operations were performed with most patients having bilateral surgery. Sixteen patients were male (52%) and 15 patients were female (48%). Twenty-six patients (84%) were classified as having a spastic movement disorder with 5 patients (16%) having mixed tone. Twenty-five patients (81%) had diplegia, 3 (10%) had hemiplegia, 2 (6%) had quadriplegia and 1 (3%) patient had triplegia. GMFCS levels were: 2 Level I, 18 Level II, 9 Level III, and 2 GMFCS IV.
Patient-reported outcomes
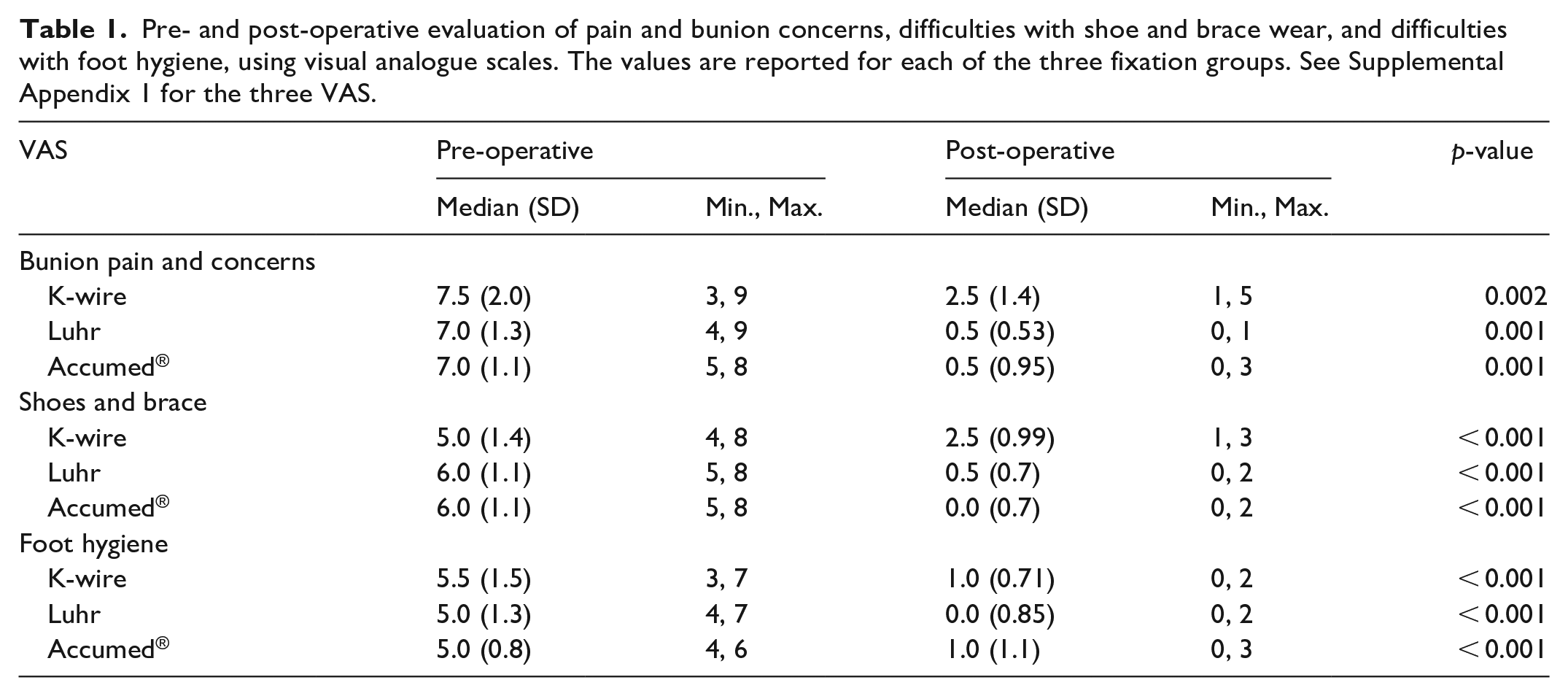
Preliminary use of VAS questionnaires showed that it could be difficult for some patients to articulate differences between bunion pain and bunion callosity concerns, as previously reported. 2 These were combined as a single question: “bunion pain and callosity concerns” (Supplemental Appendix 1). VAS scores were available for 28 patients pre-operatively and 29 patients post-operatively. The three patient groups had similar pre-operatively VAS scores for pain with median value of 7.5 for K-wire group and 7.0 for both plate groups. Similarly, VAS scores were elevated for shoes and brace (5–6) and hygiene (5–5.5) for all groups pre-operatively. All groups showed statistically significant improvement in VAS scores across the three domains (Table 1). When comparing post-operative VAS scores with the K-wire group, both plate groups showed statistically significant improvement in the domains of bunion pain and concerns, and shoe and brace wear. There was no difference in foot hygiene domain when comparing K-wire with plate fixation.
Pre- and post-operative evaluation of pain and bunion concerns, difficulties with shoe and brace wear, and difficulties with foot hygiene, using visual analogue scales. The values are reported for each of the three fixation groups. See Supplemental Appendix 1 for the three VAS.
Radiological measures
Pre-operative radiological measures were similar across all groups with no significant baseline differences between the three groups. The mean pre-operative HVA varied from 46.6 degrees in the K-wire group to 48.8 degrees in the non-locking plate group (range: 18 degrees to a maximum of 76 degrees). Improvements were seen for HVA, IMA, and LMTPA radiological measures across all three groups. The mean improvement in HVA for K-wire group was 30.8 degrees with a mean post-operative HVA of 15.8 degrees (p < 0.001). Both non-locking and locking plate groups showed significant improvement over the K-wire group with a mean improvement of 39.5 degrees for non-locking, and 40.5 degrees for locking plate group. The post-operative mean HVA for the non-locking group was 9.3 degrees and 7.6 degrees for the locking plates.
Similar improvements were seen in the IMA and LMTPA in all groups. The IMA improved significantly without the need for basal osteotomy, as described in previous studies.8,9 However, the IPA worsened after first MTP arthrodesis, was symptomatic in 2 feet and was associated with a flexion contracture in one patient (Figure 6). There was a statistically greater improvement in LMTPA between both plate groups and the K-wire group. The K-wire group achieved a post-operative mean LMTPA of 19.1 degrees against 25.8 degrees for the non-locking plate and 25.2 degrees for the locking plate group. The radiological results are summarized in Table 2.
Mean radiographic values pre- and post-operative for each of the three fixation groups: K-wire, Luhr plate, and Accumed® plate.
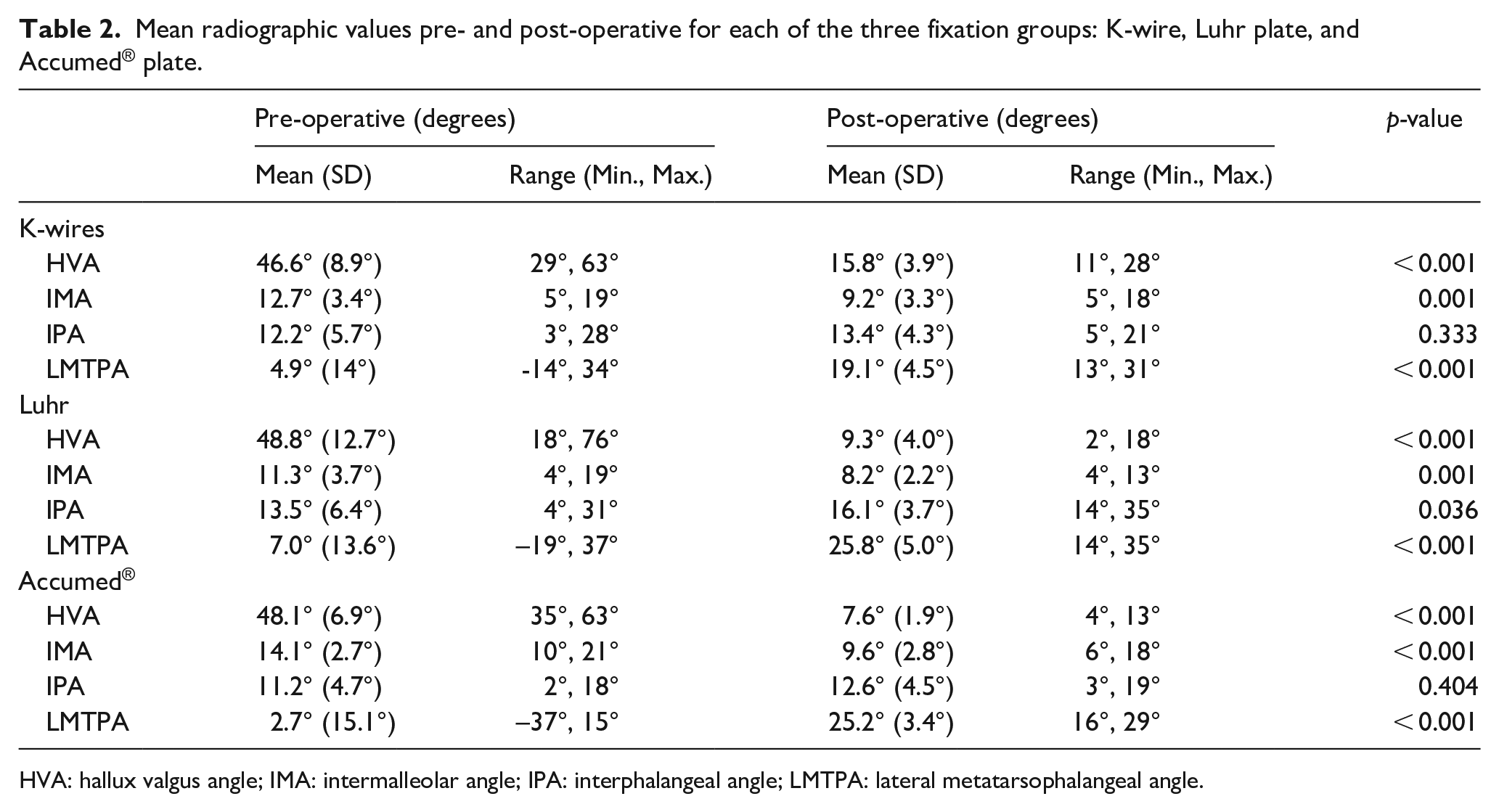
HVA: hallux valgus angle; IMA: intermalleolar angle; IPA: interphalangeal angle; LMTPA: lateral metatarsophalangeal angle.
When comparing post-operative radiological results between surgical groups, significant differences were seen between both plate groups and the K-wire group in improvement of the HVA and LMTPA angle. There was no significant difference between the improvement of the IMA between all three groups (Table 3).
Comparison of post-operative radiographic results between the three surgical groups.
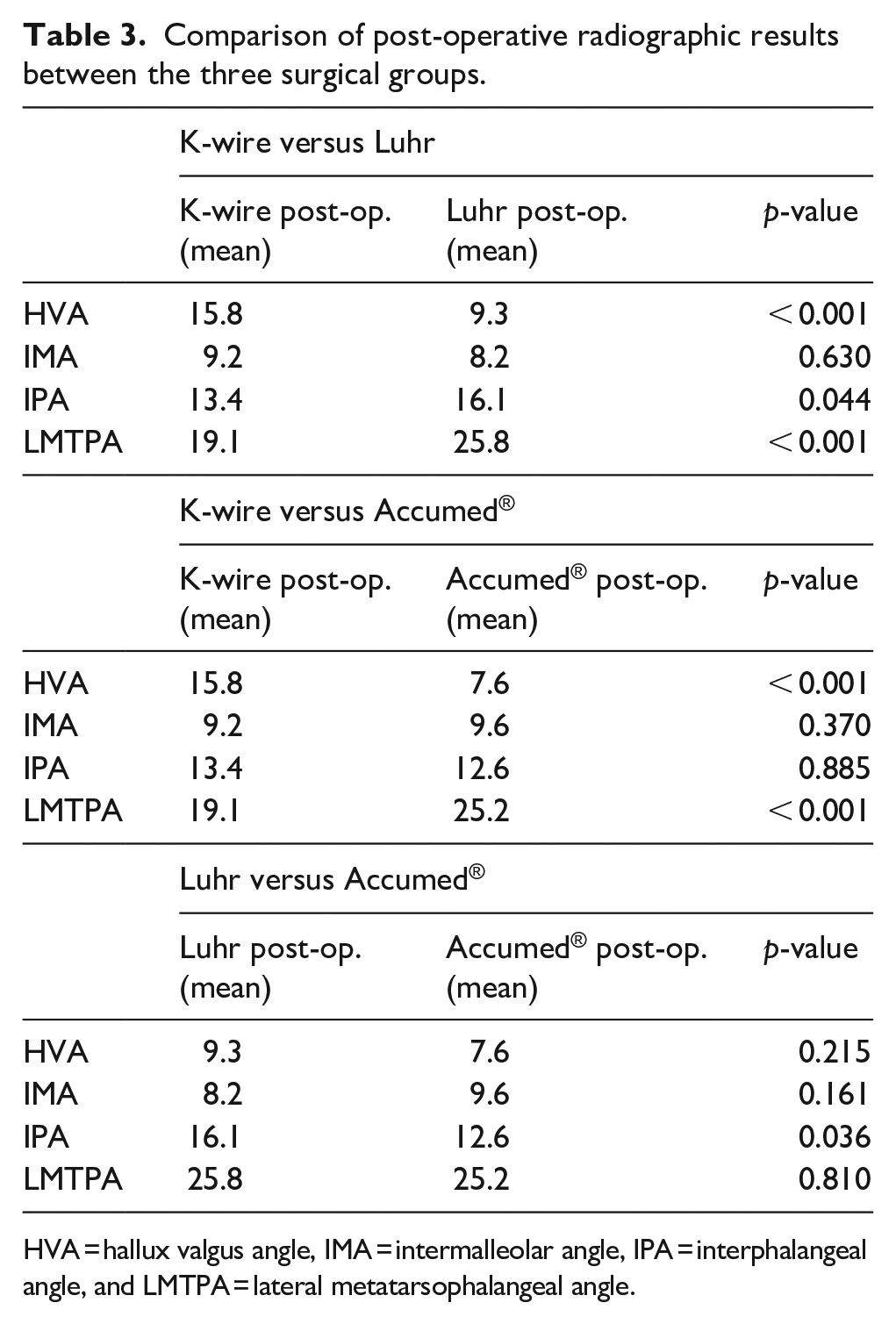
HVA = hallux valgus angle, IMA = intermalleolar angle, IPA = interphalangeal angle, and LMTPA = lateral metatarsophalangeal angle.
Time to weight-bearing
The mean time to full weight-bearing was 7.1 weeks for the K-wire group with a range of 6–10 weeks. The mean time to weight-bearing was 3.1 weeks for the non-locking plate group and 1 week for the locking plate group. This was based on radiological evidence of cortical bridging on anteroposterior and lateral radiographs, as well as clinical evidence of no pain or tenderness on manual stress applied to the hallux or absence of pain on a trial of weight-bearing. When bridging callus was difficult to assess, we relied more on the clinical assessment to determine weight-bearing status.
Post-operative complications
Complications rates were higher in the K-wire group compared to the plate fixation groups. There were seven complications in the K-wire group of 10 patients (70%) and most of these were mild, self-limiting MCD Grade II. The most common was infection, around the tip of the K-wire, where it exits the tip of the toe. Three patients had infected K-wires during the 6-week post-operative period with two requiring antibiotic treatment and one requiring early K-wire removal for signs of deep infection (MCD Grade II). Two K-wires became loose and required early removal (MCD Grade II). There was one cast-related superficial skin injury that required dressings (MCD Grade II).
There was one case of non-union in the K-wire group and one case of malunion. Both patients declined further intervention and were graded as III using the MCD system, given that correction would be feasible by revision surgery. Two patients in the K-wire group had signs of interphalangeal arthritis on follow-up radiographs, perhaps related to low-grade infection around the K-wires.
There was one complication in the locking plate group, a superficial stitch abscess that resolved following suture removal (MCD Grade II). There were no complications recorded in the non-locking plate group.
Discussion
HV is a common deformity in adolescents with CP.1 –4 Some patients with severe symptoms may require surgical intervention, and the majority of patients who require surgery being ambulatory adolescents and young adults, functioning at GMFCS II and III, with a predominantly spastic motor disorder.1 –3 Few studies have compared methods of arthrodesis, and to our knowledge, this is the first study to compare K-wire fixation with plate fixation for first MTP arthrodesis in adolescents with CP. In our study, we demonstrated the use of plate fixation resulted in greater patient satisfaction, earlier mobilization, better post-operative radiographic parameters, and lower rates of complications when compared to K-wire fixation.
Some studies support non-fusion surgery in ambulatory adolescents.5 –7,19 However, others have supported the use of arthrodesis as primary surgery for severe HV deformities, quoting superior clinical outcomes, higher corrective capacity, and lower rates of revision in comparison to reconstructive osteotomies.8,9 The severity of pre-existing pes valgus and the severity of the HV deformities in this cohort, in our view indicated arthrodesis. Our mean pre-operative HVA in this series was greater than in previous studies in CP and much greater than reported in studies in the neurotypical population.8,9,11,12 Furthermore, at our center, the revision rate for non-fusion surgery in adolescents with HV deformity, was 40% at 5-year follow-up (unpublished). No new problems with gait or brace wear were reported in our cohort of patients following arthrodesis, as evidenced by improvements in the VAS. Sixteen patients in the cohort had final gait analysis before transition to adult services and we did not see evidence of gait problems related to arthrodesis of the first MTP on three-dimensional gait analysis (3DGA).
Previously, Bishay et al. 9 reported on their series of 20 ambulatory patients with HV treated with arthrodesis and percutaneous K-wire fixation. They reported improvement in pain, cosmesis, function in all patients with improvement in HV and IMA angle measures. Patients were non–weight-bearing for 12 weeks and there were no non-unions or revision procedures. Our study showed similar improvements in pain post-operatively and earlier weight-bearing. The three groups in our study reported improvements in the three VASs as well as objective improvement in three of the four radiological parameters.8,9 Both locking and non-locking plate groups showed improvement compared to K-wires in pain and callosity scores, and shoe and brace wear scores. There was also greater improvement in HVA and LMTPA measurements for plates versus K-wire, but no difference between locking and non-locking plates (Tables 1–3). This result is perhaps not surprising as we compared unstable, non-rigid fixation to stable plate fixation.11,12 In the case of the locking plates, anatomical positioning of arthrodesis was determined by the design of the plate itself. This improved the precision of the alignment of the fused joint in this series (Table 3). Furthermore, we think that joint preparation with cup and cone reamers is superior to planar joint resection. Once the joint surfaces are prepared with the hemispherical reamers, the alignment of the construct can be adjusted in three planes without further bone resection.11,12
Few studies have previously reported on PROMs in HV surgery for CP. Davids and colleagues were the first to report high levels of patient satisfaction after first MTP fusion in adolescents with CP using a modified American Orthopaedic Foot and Ankle Society (AOFAS) Hallux Metatarsophalangeal–Interphalangeal Scale. They also reported high fusion rates and excellent deformity correction using detailed radiographic analysis. 8 The DuPont bunion rating score is very useful, particularly for non-fusion outcome assessment. 5 The Oxford Foot and Ankle Score has the best evidence in terms of psychometric properties but has a more general foot and ankle perspective. 20 We used VASs because of pre-existing legacy issues. Future studies could be enhanced by prospective design using PROMs with robust psychometric properties.
Complication rates were lower in the plate groups than the K-wire group. Most of our complications reported were related to common issues related to K-wires, such as superficial local infection or early loosening. Although patients were advised to non–weight-bear for 6 weeks, most had walked in that time judging by the state of the casts as well as parental reports. This may be associated with our higher rate of reported K-wire complications, than in a previous study. 9 Our transition from non-locking to locking plates was reflective of trends in orthopedic practice over the past 10–15 years, due to increased popularity and availability of locking, anatomic specific, plating systems.21,22 We did not see any benefit of locking plating systems on patient function or radiographic parameters (Tables 2 and 3).
Biomechanical studies, operative descriptions, and clinical studies have suggested that a compression screw combined with a dorsal locking or non-locking plate is the most stable fixation construct.23,24 However, fusion rates are so high with modern constructs that showing superior clinical outcomes would be very difficult. It would also be difficult technically, to insert a crossed screw with our current implant choice without compromising the three-screw fixation cluster inserted into the base of the proximal phalanx.
Earlier weight-bearing with plate fixation is one major functional advantage over K-wire fixation. Adolescents with CP have very different needs after arthrodesis for severe HV than adults without neurological disability. Typically developing adults can have simple immobilization after bunion surgery and can more easily comply with limitations in weight-bearing, especially if they have unilateral surgery.11,12 Adolescents with CP may be reluctant to give up their independence and we think that most of the patients in all three groups adopted very early weight-bearing. During the study period, two adolescents with severe symptomatic deformities declined or postponed surgery when counseled about the need for a period of non–weight-bearing and wheelchair mobility. We think that early weight-bearing contributed to both the higher complication rate and the suboptimal radiographic and clinical outcomes in the K-wire group. The combination of dorsal plating and cast immobilization was sufficiently robust to achieve a 100% fusion rate in good alignment.
We think that K-wires are not sufficiently stable for arthrodesis of the first MTPJ in adolescents with CP. Dorsal plating is more stable, more precise with reduced complications and improved precision and reproducibility. Our study was underpowered to detect meaningful differences between locking plates and standard plates.
A potential disadvantage of plating is the need for a second operation to remove the plate. However, the profile of the plates is concave, low profile, and we found no implant-related symptoms in any of our patients at short-term follow-up, as has been reported in previous series.11,12 One patient requested removal of the plates after healing, but this was related to his views on having a “foreign body” in situ. Locking plates also come at a significant cost: approximately US$3,000.00 for bilateral locking plate fixation compared to US$48.00 for four K-wires. The cost of Luhr plates was intermediate between these figures at US$1,200.00.
This study was limited by its retrospective nature and therefore lacks both randomization and a control group. Our study was limited by small numbers in each cohort, thus reducing the strength of any conclusions drawn from our results. We also did not compare non-fusion surgery as this was outside the scope of this study. The longitudinal nature of this study encompassed changes to surgical practice and instrumentation over time which may have introduced inherent biases. While our average follow-up period of 4 years may appear adequate to assess early results, longer-term follow-up is still required to assess problems that may arise later in life. Potential long-term problems might include the problems with the interphalangeal joint related to increase valgus deformity and degenerative changes.8,12 Interphalangeal valgus may be structural and may also be dynamic, the result of a tight flexor hallucis longus (FHL) acting eccentrically across the interphalangeal joint. Correction of FHL contracture may be indicated in selected cases.4,8
Conclusion
Arthrodesis for symptomatic HV in CP improves patient pain and function. Historically K-wire fixation was utilized with good effect, however, compared with plate fixation, there are concerns regarding increased rates of complications. Non-locking and locking plate options both provide excellent options for fixation and correction of deformity. The latter (angular stable implants) is the author’s preference.
Supplemental Material
sj-docx-3-cho-10.1177_18632521231200060 – Supplemental material for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques
Supplemental material, sj-docx-3-cho-10.1177_18632521231200060 for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques by Ken Ye, Megan Cashin, Samuel K Van de Velde, Abhay Khot, Kerr Graham and Erich Rutz in Journal of Children’s Orthopaedics
Supplemental Material
sj-docx-4-cho-10.1177_18632521231200060 – Supplemental material for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques
Supplemental material, sj-docx-4-cho-10.1177_18632521231200060 for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques by Ken Ye, Megan Cashin, Samuel K Van de Velde, Abhay Khot, Kerr Graham and Erich Rutz in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231200060 – Supplemental material for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques
Supplemental material, sj-pdf-1-cho-10.1177_18632521231200060 for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques by Ken Ye, Megan Cashin, Samuel K Van de Velde, Abhay Khot, Kerr Graham and Erich Rutz in Journal of Children’s Orthopaedics
Supplemental Material
sj-tif-2-cho-10.1177_18632521231200060 – Supplemental material for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques
Supplemental material, sj-tif-2-cho-10.1177_18632521231200060 for Arthrodesis of the first metatarsophalangeal joint for severe hallux valgus in adolescents with cerebral palsy: A retrospective comparison study of three surgical techniques by Ken Ye, Megan Cashin, Samuel K Van de Velde, Abhay Khot, Kerr Graham and Erich Rutz in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.Y. declares no conflicts of interest. M.C. declares no conflicts of interest. S.K.V.d.V. declares no conflicts of interest. A.K. declares no conflicts of interest. K.G. has received research support from the NHMRC-CRE-CP-Achieve outside the scope of the submitted work and is on the Surgeon’s Advisory Board of the OrthoPaediatrics Corp. E.R. declares no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
No patients or clinical subjects were used in this study; informed consent was not required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.