
Abstract
Abstract
Background
Hallux valgus deformity is a common sequel of spastic cerebral palsy.
Methods
Twenty ambulatory patients (24 feet) suffering hallux valgus deformity, with painful forefoot and restricted footwear, secondary to spastic cerebral palsy acquired perinatally, were treated with great toe metatarsophalangeal (MTP) arthrodesis using percutaneous K-wires for fixation. The mean age at the time of surgery was 16.2 years (range 14–18 years). They were retrospectively evaluated for the results after arthrodesis at a mean interval of 3 years and 4 months (range 3–4 years) by physical examination and radiographs.
Results
All patients had a stable painless aligned great toe, with <10° valgus, <20° dorsiflexion and neutral rotation after arthrodesis, evidenced by improvement in pain, cosmesis, functional activity, footwear, callosities and hygiene, as well as by significant improvement in the measures of the MTP and the intermetatarsal angles (IMA) by postoperative radiographs. Neither non-union (pseudoarthrosis) nor recurrence of the deformity developed. Complications included superficial wound slough in a single case. Using the modified American Orthopaedic Foot Ankle Society (AOFAS) Hallux Metatarsophalangeal–Interphalangeal Scale, 18 feet (75%) were classified as excellent and six feet (25%) as good. Neither fair nor poor cases were recorded.
Conclusion
Hallux valgus deformity in adolescents with spastic cerebral palsy is best treated by great toe MTP arthrodesis to improve segmental foot malalignment and dynamic foot deviation.
Introduction
Hallux valgus deformity is a component of complex multisegmental foot and ankle malalignment that is common in patients with spastic cerebral palsy as a result of foot intrinsic muscle imbalance and extrinsic abnormal load due to the disruption of forefoot biomechanics during the stance phase of the gait cycle [1]. Disabilities in adolescents include a part of the great toe deformity, pain, difficulty in purchasing comfortable footwear, poor hygiene and gait deviation [2].
The development of hallux valgus in the non-ambulatory children with cerebral palsy supports the role of foot intrinsic muscle imbalance [3]. Abnormal extrinsic factors due to the disruption of forefoot biomechanics during the stance phase of the gait cycle could also contribute to the development of hallux valgus deformity in the ambulatory children with cerebral palsy. Collapse of the medial longitudinal arch, midfoot abduction and neuromuscular planovalgus deformity cause pronation and axial rotation of the first ray and medialisation of the great toe metatarsophalangeal (MTP) joint, with its flexion–extension axis deviated out of the sagittal plane. Associated transverse plane rotation of the femur and/or the tibia contributes further to asymmetric forefoot loading.
When surgical treatment is considered for established hallux valgus deformity in adolescents with spastic cerebral palsy, the neuromuscular status mandates the choice of MTP arthrodesis as a primary treatment strategy and not as a salvage procedure [3]. Other surgical reconstructive procedures, such as soft-tissue balancing and corrective osteotomies, though useful in the management of hallux valgus in neurologically normal adolescents, are of not much benefit in the case of spastic cerebral palsy, as recurrence of the deformity is very high [4].
The aim of the study was to evaluate the outcome of the correction of hallux valgus deformity in adolescents with spastic cerebral palsy by great toe MTP arthrodesis as the first-choice corrective procedure of foot segmental malalignment and dynamic gait deviation with respect to technical and functional domains. The objective of great toe MTP arthrodesis in the current study was to obtain stability and adequate alignment of the great toe away from the second toe and parallel to the lesser toe and in 10–15° dorsiflexion relative to the floor, as evidenced by radiographic correction of the measurements of the hallux valgus angle (HVA) and intermetatarsal angle (IMA) in the transverse plane, and the lateral metatarsophalangeal angle (LAT-MTPA) in the sagittal plane.
Material and methods
A retrospective review of 20 patients who presented to the National Institute of Neuromotor System, Imbaba, Giza, Egypt, and to Al-Sahel Teaching Hospital, Shoubra, Cairo, Egypt, between September 2003 and September 2004 with hallux valgus deformity secondary to spastic cerebral palsy was conducted. The results in this group after at least 3 years of follow-up were reported in November 2007 using previous medical records, history and physical and radiographic examinations.
Physical examination, original disease and treatment
Sixteen patients were diplegic and four hemiplegic. No patient was of the total body involvement (TBI) type. All were able to walk without support and were considered to be community-level ambulators. We did not use the Growth Motor Function Classification Scale (GMFCS) in the evaluation because it restricts the cases to between 2 and 12 years of age, while the youngest age in our study cohort was 14 years. Each of the 20 patients had received some forms of non-operative treatment, such as physical therapy programmes and skeletal muscle relaxants, and had undergone some form of surgical procedure in the lower and/or the upper extremities before they were operated upon for great toe MTP arthrodesis. All had previous surgeries to correct ankle–foot deformities and to improve gait deviation in the 24 feet. These included Achilles’ tendon lengthening in 18 ankles, gastrocnemius recession in 22 legs, lateral column calcaneal lengthening osteotomy in six feet, ankle arthrodesis in four ankles and triple arthrodesis in two feet. Sixteen patients had unilateral hallux valgus deformity and the great toe arthrodeses were applied to their 16 feet. Four patients had bilateral hallux valgus deformity and great toe arthrodeses were applied to their eight feet one side after the other through staged procedures. All patients had painful forefoot and restricted footwear. The indication for arthrodesis was hallux valgus deformity in an adolescent ambulatory cerebral palsy patient with pain over the medial eminence after the failure of non-operative treatment, wide shoes or orthosis. The mean age at the time of surgery was 16.2 years (range 14–18 years). Fifteen patients were females, of which three had bilateral great toe deformity, giving a total of 18 feet (75%), and five males, of which one had bilateral great toe deformity, giving a total of six feet (25%). Twelve patients, of which ten females and two males, had undergone previous soft-tissue balancing and corrective osteotomies in their great toes before MTP arthrodesis and were identified as recurrent great toe cases. Eight patients, of which five females and three males, had undergone no previous great toe surgeries and were identified as new great toe cases.
Preoperative radiographic appearance
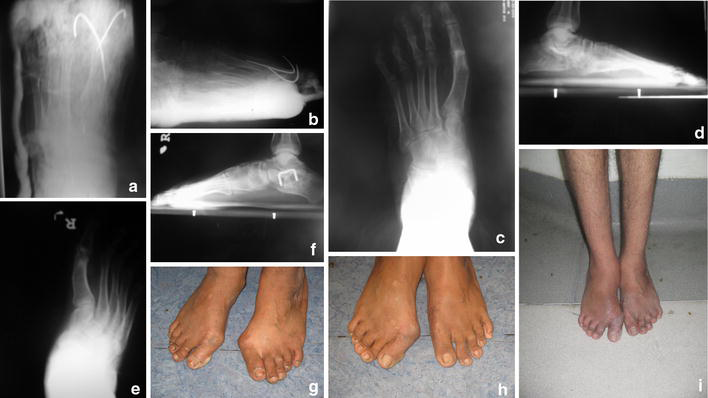
Anteroposterior and lateral standing weight-bearing radiographs of both feet were obtained. Lines were drawn along the axes (middles) of the first and second metatarsals and the proximal and distal phalanx of the great toe. The anteroposterior MTP or HVA (normally 0–<10°, valgus alignment “+”), the anteroposterior IMA (normally 0–<10°) and the LAT-MTPA (normally 25–35°, dorsiflexion alignment “+”) were measured [3] (Fig. 1).

Preoperative:
Operative technique
The surgical procedure in all of the patients in the current study consisted of arthrodesis of the great toe MTP joint. The approach was through a dorsal longitudinal incision along the great toe and the adjoining first metatarsal along the medial edge of the extensor hallucis longus tendon a few millimetres proximal to the interphalangeal joint extending proximally for 5–6 cm [5]. The skin and the subcutaneous tissues were reflected on both sides. Care was taken to avoid injury of the medial branch of the superficial peroneal nerve. The first MTP joint capsule was incised transversely to expose the first metatarsal head and proximal phalangeal base. Exostectomy of the prominent first metatarsal head flush with the medial cortex was performed. Direct resection of the articular cartilage and subchondral bone preserving the contour of the first metatarsal head and proximal phalangeal base was performed [3]. The great toe was properly aligned. Percutaneous two crossing K-wires fixation were inserted [6]. The wound was closed in layers. A POP back-slab under the great toe and the first metatarsal was applied and kept for 12 weeks.
Postoperative care
Postoperative anteroposterior and lateral radiographs of the foot were taken the day after surgery, then after 6 weeks, after which the two K-wires were removed, and after 12 weeks to assess the position and to ensure complete fusion, after which weight-bearing was allowed. Physiotherapy gait training programme with footwear care was instituted for a further 1–3 months.
Evaluation
The modified American Orthopaedic Foot Ankle Society (AOFAS) Hallux Metatarsophalangeal–Interphalangeal Scale, used by Davids et al. [3], with an optimal score of 100 marks was used. The clinical rating system [7] considered pain (40 marks), alignment (25 marks) and function (35 marks). Modifications of the original AOFAS rating system were introduced [8] to make it applicable to the current study. MTP joint motion and stability (20 marks), which are not relevant in arthrodesis, were replaced by hygiene of the great and second toes (10 marks). The remaining 10 marks were transferred to the alignment section (Table 1). Cases were classified as excellent with a score of >90–100, good with a score 75–90, fair with a score 60–<75 and poor with a score less than 60.
The modified American Orthopaedic Foot and Ankle Society (AOFAS) Hallux Metatarsophalangeal–Interphalangeal Scale
Results
Twenty patients (24 feet) were followed-up for a mean of 3 years and 4 months (range 3–4 years) after arthrodesis.
Great toe MTP fusion was determined to be present in all (100%) of the 20 patients (24 feet) with a stable painless aligned great toe after arthrodesis, with <10° valgus, <20° dorsiflexion and neutral rotation, and this could be confirmed by intra-operative radiology. Evidence of arthrodesis was determined after 12 weeks both by physical examination showing the absence of swelling, warmth and local tenderness, and by radiographic examination showing the crossing trabeculation of fusion (Fig. 2).
Postoperative:
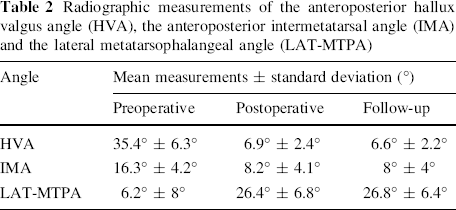
Radiographic correction of the deformity was evidenced by decreases in the postoperative measurements of the anteroposterior HVA, the anteroposterior IMA and by increases in the postoperative measurements of the LAT-MTPA (Table 2).
Radiographic measurements of the anteroposterior hallux valgus angle (HVA), the anteroposterior intermetatarsal angle (IMA) and the lateral metatarsophalangeal angle (LAT-MTPA)
Pain was relieved in 18 feet (75%), mild in six feet (25%) in the form of occasional pain in the forefoot not over the site of fusion, but worsened in no feet. Cosmesis was improved after surgery with adequate alignment in all of the 24 feet (100%), with neither overlap nor underlap. Activity was full in 16 feet (≈66.6%), limited recreational in six feet (25%), limited daily in two feet (≈8.4%), but restricted in no feet. Footwear was not restricted in 20 feet (≈83.3%), restricted but over the counter footwear possible in four feet (≈16.7%), but fully restricted with custom modification in no feet. Callosities were absent in all of the 24 feet (100%). Poor hygiene was improved for 22 feet (≈91.6%), but unchanged in two feet (≈8.4%). There was no difference practically, apart from the technical difficulty, between the recurrent and the new great toe cases regarding pain relief, alignment and functional activity.
Using the modified AOFAS Hallux Metatarsophalangeal–Interphalangeal Scale used by Davids et al. [3], 18 feet (75%) had >90 marks and were classified as excellent, six feet had 75–90 marks and were classified as good, but no feet had <75 marks, so there were neither fair nor poor cases. There was a significant improvement in the results (P > 0.05).
Discussion
Hallux valgus deformity in adolescents with spastic cerebral palsy is multifactorial. It could be attributed to foot intrinsic muscle imbalance. Overactivity of the abductor hallucis muscle causes varus first metatarsal [9] and overactivity of the peroneus longus causes planovalgus foot deformity and proximal and lateral shift of the oblique head of the adductor hallucis from the peroneus longus tendon sheath with valgus great toe proximal phalanx [10].
The aetiologic development of hallux valgus in the non-ambulatory children with cerebral palsy is caused by the combination of foot intrinsic muscle imbalance [3], abnormal extrinsic factors due to the disruption of forefoot biomechanics during the stance phase of the gait cycle, collapse of the medial longitudinal arch, midfoot abduction, neuromuscular planovalgus with pronation and axial rotation of the first ray and medialisation of the great toe MTP joint, and associated transverse plane rotation of the femur and/or the tibia causing asymmetric forefoot loading [11].
Hallux valgus deformity compromises the normal function of the great toe in stabilisation of the medial longitudinal arch by the “windlass” mechanism of the MTP joint dorsiflexion [11] and in increasing the surface contact area of the forefoot during the stance phase of the gait cycle [12, 13].
Soft-tissue realignment and metatarsal corrective osteotomies, which are the treatment of choice for neurologically normal adolescents with hallux valgus, cannot normalise forefoot biomechanics disruption in hallux valgus secondary to cerebral palsy and are followed by a high recurrence rate [14, 15].
Biomechanical studies of multiple joint-resection techniques and fixation options described for great toe MTP arthrodesis favoured non-planar joint excision and crossed-wire fixation to maintain intrinsic bony stability [16].
Using the modified AOFAS Hallux Metatarsophalangeal–Interphalangeal Scale, the functional outcome revealed significant improvement in regards to pain relief (75% of feet, with 25% still having forefoot but not pseudoarthrosis pain), cosmesis and alignment (100% of feet), activity (≈66.6% of feet), footwear possibility (≈83.3% of feet) and better hygiene (≈91.6% of feet). The forefoot pain in the remaining 25% of patients was tolerable, not present at rest but with strenuous activity, and ameliorated by local foments and occasional non-steroidal anti-inflammatory drugs. These were comparable to the outcome after the management of hallux valgus deformity in neurologically normal patients. Mann and Thompson reported successful fusion of the first MTP joint in more than 90% of patients suffering hallux valgus with osteoarthritis and rheumatoid arthritis. No patient had significant clinical symptoms [17].
Jenter et al. [10] concluded that the MTP arthrodesis gave the best result for hallux valgus in children with cerebral palsy. They have had a higher percentage of correction of the HVA that valued 89%, while our result only had 81%. However, we based our study on 24 feet, whereas Jenter et al.'s investigation considered only eight feet with MTP arthrodesis.
Although Davids et al. [3] had a relatively similar number of cases (26 feet), mean age (16 years) and average follow up (4 years and 11 months), we have better results, where the average HVA preoperatively was 35.4° and, after the last follow up, it was 6.9° with 81% correction, while that for Davids et al.'s study was 36.3° and 9.6°, respectively, with 73% correction.
Conclusion
The management of hallux valgus deformity in adolescents with spastic cerebral palsy should not be performed in isolation but, rather, in conjunction with other segmental forefoot malalignment and dynamic gait deviations.
Metatarsophalangeal (MTP) arthrodesis for hallux valgus deformity in adolescents with spastic cerebral palsy achieved satisfactory results with minimal associated morbidity in the technical and functional outcome domains, and is proposed to be the primary treatment of choice and not only as a salvage procedure in such cases.