
Abstract
Background:
The study aim was to present four new well-documented cases of spontaneous improvement of olisthetic scoliosis and to analyze well-documented cases from the literature.
Methods:
Surgical log search and systematic review were conducted. Inclusion criteria were (1) age less than 18 years, (2) symptomatic high-grade (≥50%) spondylolisthesis, (3) scoliosis ≥20o, (4) primary surgical treatment via lumbosacral fusion, (5) complete x-rays, and (6) minimum 1-year radiographic follow-up or until curve resolution.
Results:
A total of 13 patients with average age of 13.9 years were included in the study, 4 from the authors’ surgical logs and 9 from the literature. Slip percentage of L5-S1 ranged from 51% to 95%. Olisthetic curve magnitude averaged 34.6° (range: 20°–45°) with majority (8/13) demonstrating long thoracic curves with lateral trunk shift. All but one of these were apex right with rightward trunk shift. The remainder of the curves were isolated lumbar curves, with an apex left morphology without trunk shift. Eleven of the 13 patients showed curve improvement following isolated lumbosacral fusion. Three patients experienced a decrease in curve magnitude of 12°–28° and eight patients enjoyed complete resolution (≤10°) of their scoliosis.
Conclusion:
The current study summarizes 13 well-documented cases of olisthetic scoliosis (4 new cases and 9 from the literature) that associated with symptomatic high-grade spondylolisthesis. All were treated via a primary posterior lumbosacral fusion strategy. Eleven of the 13 curves showed spontaneous improvement (8 complete resolution of scoliosis) following their lumbosacral surgery.
Level of evidence:
Therapeutic level IV.
Introduction
The pain and reflexive muscle spasm of spondylolisthesis may give rise to a substantial secondary scoliosis in pediatric patients. In a mixed pediatric and adult cohort of 115 spondylolisthesis patients, Bosworth et al., 1 reported “severe scoliosis” in about 2% of cases. McPhee and O’Brien 2 found that 3% of their symptomatic spondylolisthesis patients demonstrated an associated scoliosis in excess of 15°. Pediatric orthopedic spine surgeons commonly refer to such scoliosis occurring together with symptomatic lumbosacral spondylolisthesis as olisthetic scoliosis.3 –6 Patients who present with this combination of pediatric spinal problems provide a special challenge to the pediatric spinal deformity surgeons who care for them.
Olisthetic scoliosis will spontaneously improve and even resolve completely following successful fusion of symptomatic high-grade spondylolisthesis. None other than Joseph Risser was the earliest author to present well-documented pediatric cases illustrating this phenomenon. 7 Similar cases have been illustrated by other authors over the last 60 years.8 –13 The purpose of the current study was to present four new well-documented cases of spontaneous improvement of olisthetic scoliosis in such patients as well as to offer a systematic review of the existing literature on this topic.
Materials and methods
This research was reviewed and approved as an exempt human subjects study. A convenience sample of six pediatric patients demonstrating scoliosis in association with spondylolisthesis was identified from the surgical logs of the two authors. The inclusion criteria utilized for this study were as follows: (1) age less than 18 years, (2) symptomatic high-grade lumbosacral spondylolisthesis, defined as greater than or equal to 50%, (3) maximal scoliotic curve of greater than or equal to 20°, (4) primary surgical treatment via lumbosacral fusion, and (5) minimum of 1-year radiographic follow-up. Two patients (an 8-year-old male and a 10-year-old female) had inadequate radiographs and were excluded. A literature search was also conducted aimed at identifying radiographically documented pediatric olisthetic scoliosis patients in English language publications.
PubMed was utilized and searched using keywords olisthetic, spondylolisthesis scoliosis, and sciatic spondylolisthesis scoliosis. Abstracts of identified articles were screened and those focused on children or including children in addition to adult patients were subjected to full article review. Reference lists of identified articles and bibliographies of pediatric orthopedic reference texts were reviewed in order to identify any additional pertinent articles not captured by the PubMed search. In addition to this, a Google search of the term “olisthetic scoliosis” was conducted with the intention of capturing any additional publications not indexed in PubMed. Publications that provided preoperative radiographic images of both a child’s spondylolisthesis as well as their concomitant scoliosis in addition to follow-up spine radiographs demonstrating an outcome of interest (either scoliosis stability, worsening, or improvement) were included. These radiographic images were re-measured by the authors.
Spondylolisthesis slip percentages were measured using the validated method of Wright and Bell.14,15 Sagittal rotation was measured via the method of Wiltse and Winter. 16 Scoliosis measurements were performed using the Cobb method. 17 These measurements were performed digitally for the four new cases (Merge PACS/Merge Healthcare, Heartland, WI) and with a sharp pencil and protractor on digitally enlarged images for the cases identified from the literature. Resolution of scoliosis was defined as curve magnitude of less than or equal to 10°. Apical vertebral rotation was assessed via the Nash–Moe method. 18 Lateral trunk shift was measured by the method described by Richards et al. 19 and expressed as a percentage of pelvic width in order to control for radiographic magnification.
Results
A total of 13 patients were included in this study. Four patients that met the inclusion criteria were identified from the surgical logs of the authors (Table 1). Case synopses of these patients are presented below. The primary search strategy identified six publications accounting for eight well-documented cases7 –9,11 –13 of the phenomenon of interest, and the Google search identified one additional article contributing another case 10 (Table 2).
Four new olisthetic scoliosis patients.
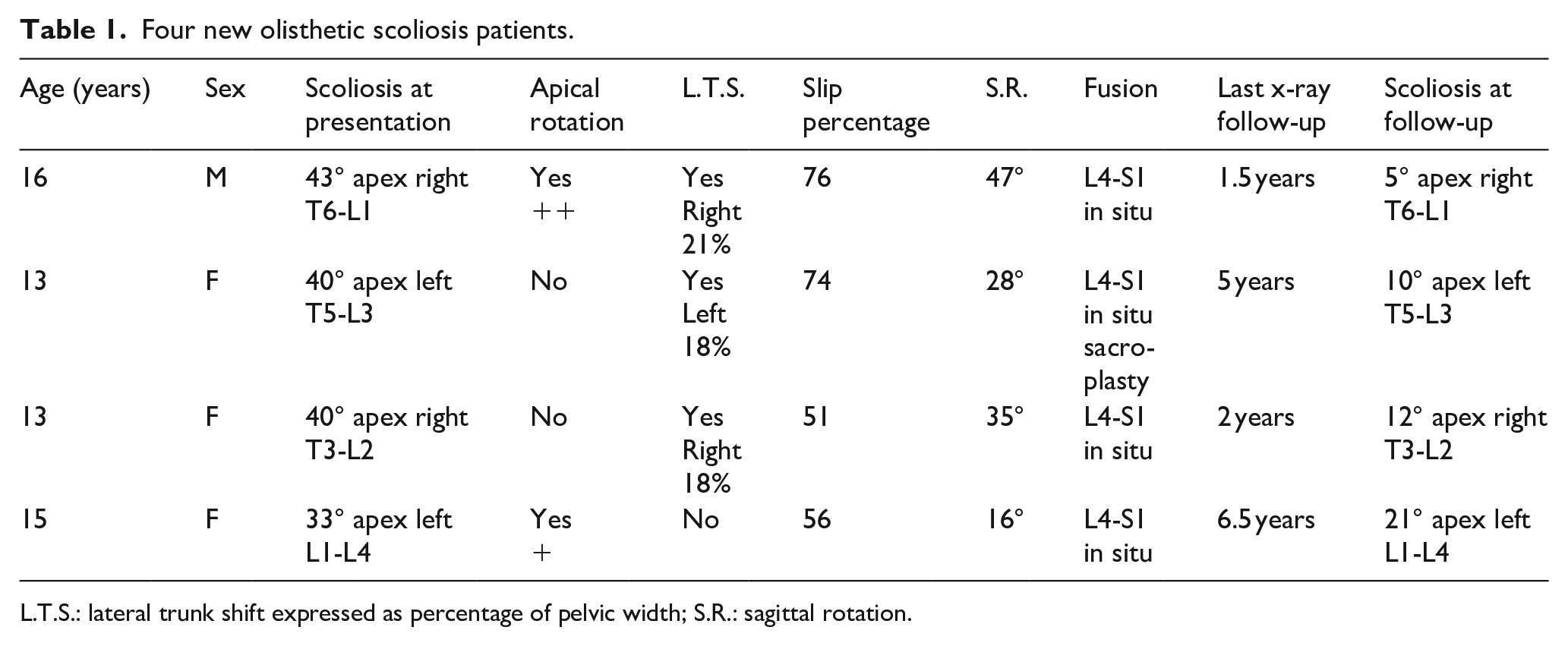
L.T.S.: lateral trunk shift expressed as percentage of pelvic width; S.R.: sagittal rotation.
Nine radiographically documented pediatric cases from the literature.
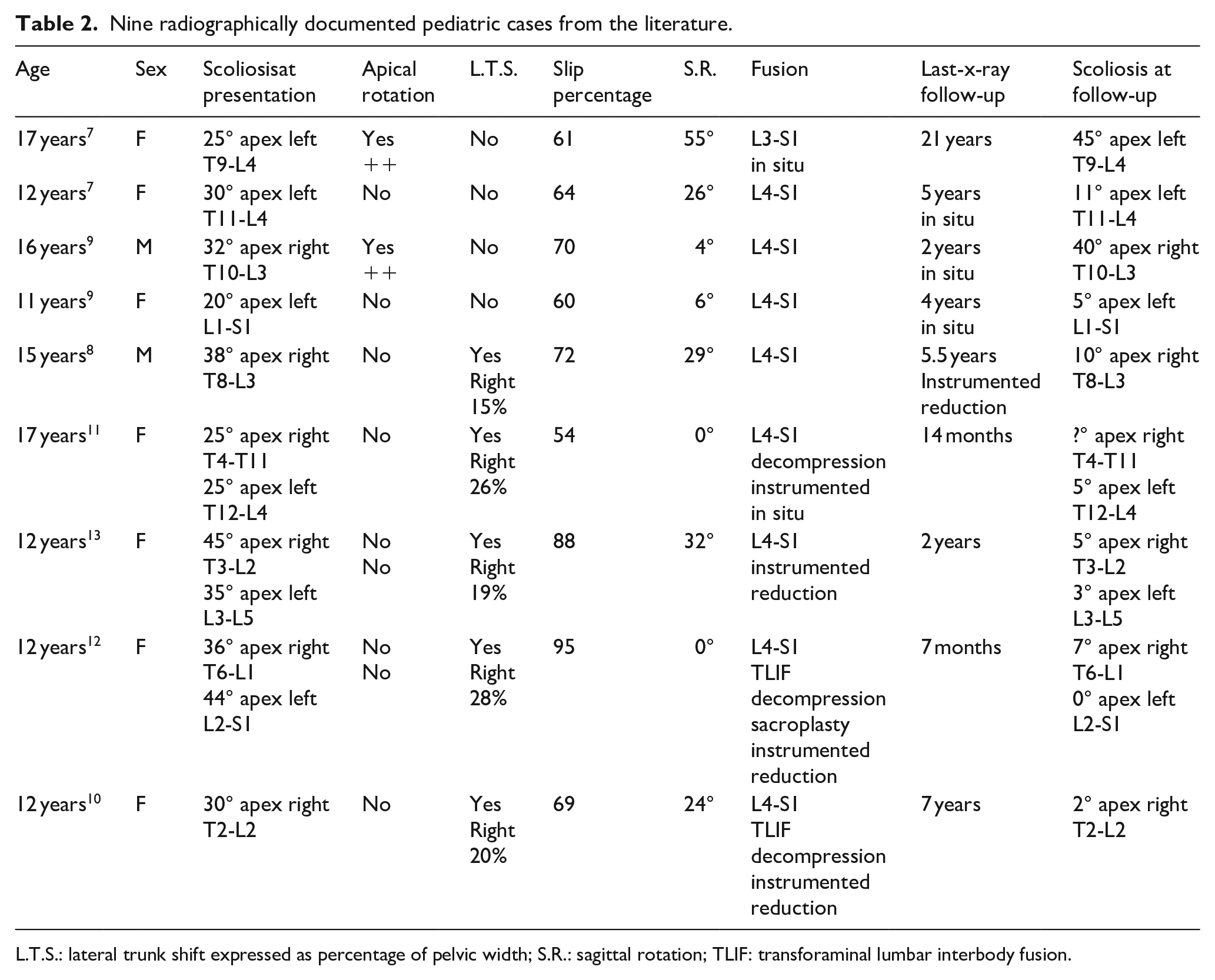
L.T.S.: lateral trunk shift expressed as percentage of pelvic width; S.R.: sagittal rotation; TLIF: transforaminal lumbar interbody fusion.
There were 10 females and 3 males with an average age at presentation of 13.9 years (range: 11–17 years). Females were just over 2 years younger than males, 13.5 years versus 15.6 years. Olisthetic curve magnitude of the main curve (some children did have double curve patterns) averaged 34.6° (range: 20°–45°). Apical rotation was rare with only three patients demonstrating this feature, and all registering at the low end of the Nash–Moe scale. Two of these three apical rotation cases demonstrated curve progression (average 14°). The remaining 11 curves all demonstrated resolution or improvement.
Long thoracic curves with lateral trunk shift predominated (8/13 curves) with all but one of these being apex right with rightward trunk shift. The remainder of the curves were isolated lumbar curves, all with an apex left morphology and no measureable truncal shift. All patients’ slip percentages exceeded 50% (range: 51%–95%), and all occurred at the L5-S1 level.
Case #1
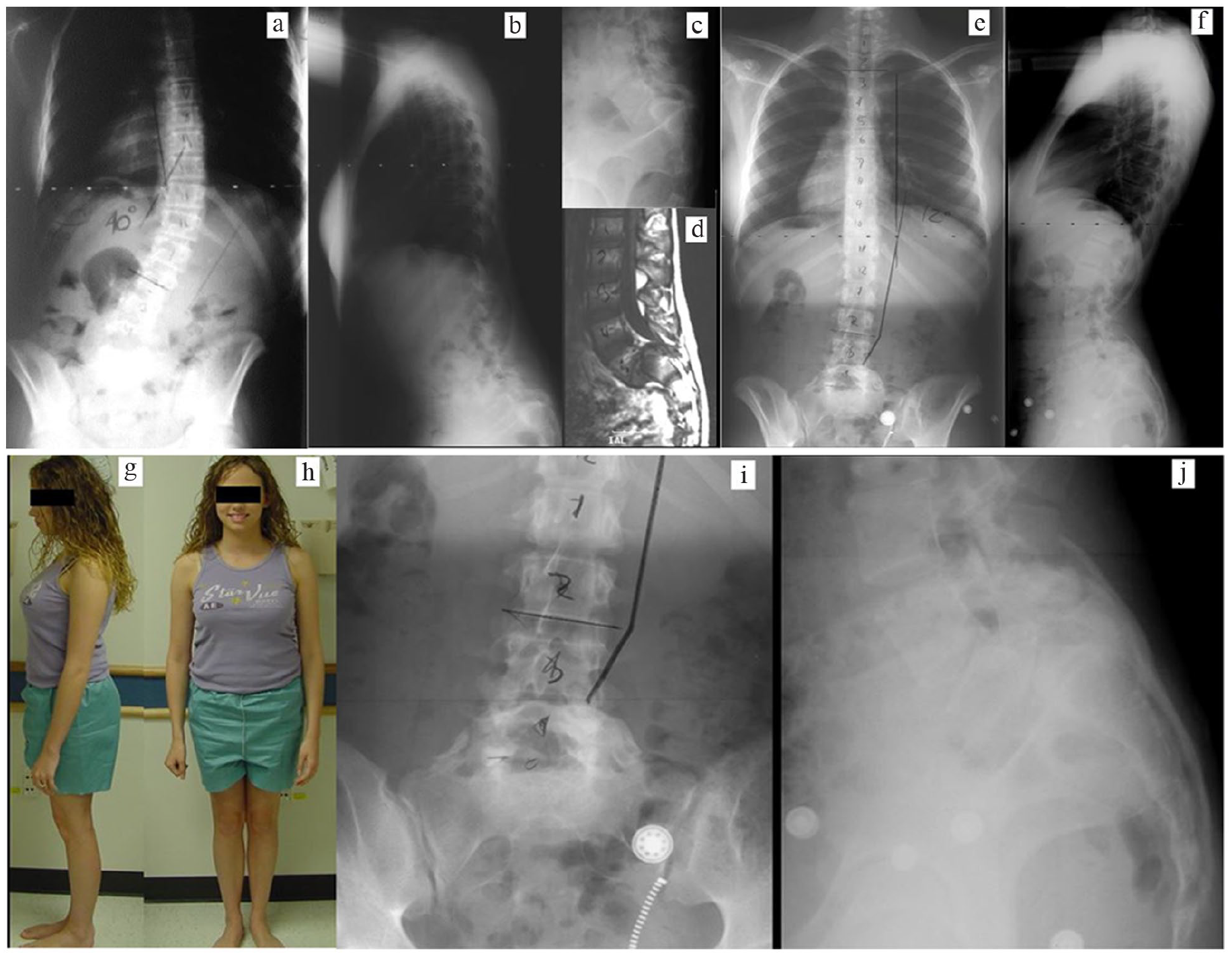
A 16-year-old male presented with spinal deformity and sensory radicular pain (Figure 1). A 76% L5-S1 spondylolisthesis and apex right 43° T6 to L1 scoliosis with rightward trunk shift were noted. A lumbar myelogram revealed no evidence of herniated nucleus pulposus. Minimal apical vertebral rotation was noted, and a supine bending film demonstrated significant curve flexibility. An in situ L4 to S1 posterior spine fusion was performed utilizing autogenous bone graft. Postoperative immobilization in a double pantaloon Risser cast was used for 6 weeks followed by a single thigh extension thoracolumbar spinal orthosis for an additional 6 weeks. At 1.5-year radiographic follow-up, spinal balance had been restored, and the T6 to L1 scoliosis was resolved.
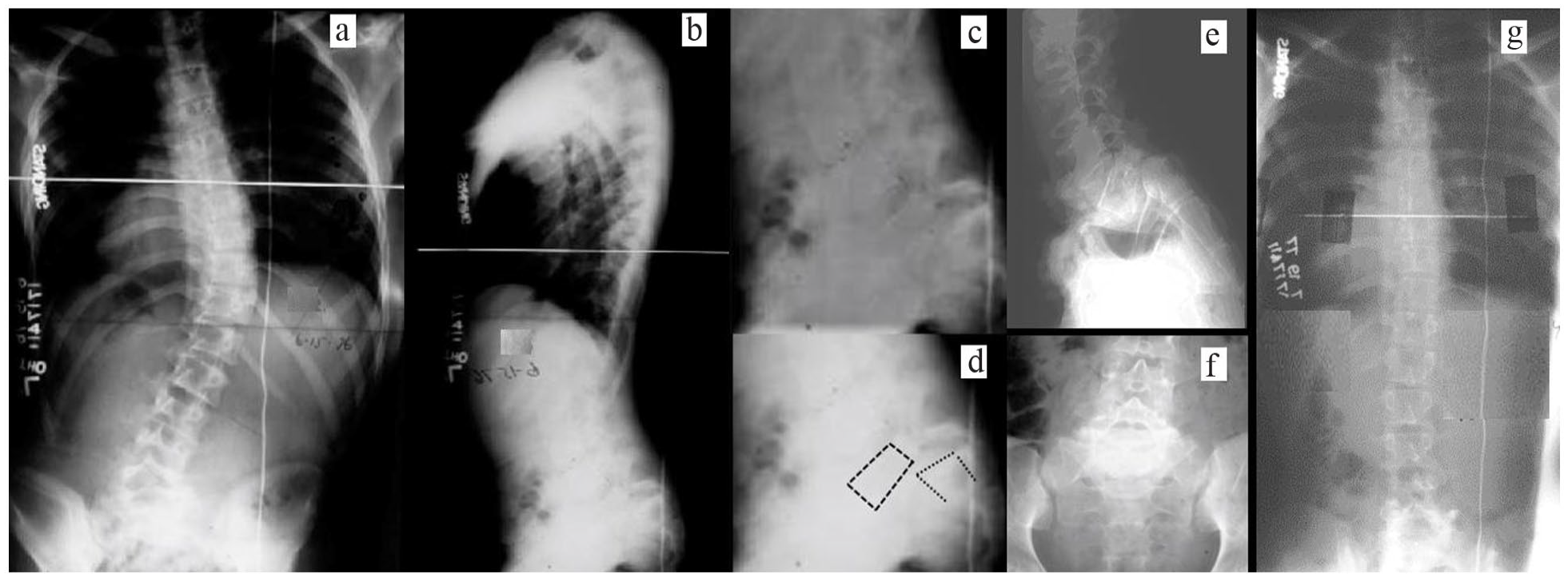
Sixteen-year-old male. (a) Preoperative posteroanterior scoliosis radiograph demonstrating large apex right curve with rightward trunk shift. (b) Preoperative lateral scoliosis radiograph with normal sagittal profile other than lumbosacral kyphosis. (c) Preoperative lateral lumbosacral radiograph showing high-grade spondylolisthesis. (d) Same radiograph as 1°C but with key edges outlined. (e) One-year postoperative lateral lumbosacral radiograph revealing L4 to S1 posterior fusion. (f) One-year postoperative anteroposterior lumbosacral radiograph. (g) One-year postoperative posteroanterior scoliosis radiograph demonstrating curve resolution.
Case #2
A 13-year-old female sought care for her back pain, spinal deformity, and right leg sensory and motor radiculopathy (Figure 2). A 74% L5-S1 spondylolisthesis was noted as well as 40° apex left T5 to L3 scoliosis with leftward trunk shift. Right leg straight leg raise testing was positive at 10°. A myelogram and magnetic resonance imaging revealed bulging L5-S1 disk and tight dural sac draped over the superior aspect of S1. Utilizing autogenous bone graft an in situ L4 to S1 posterior spine fusion was performed in addition to L5-S1 discectomy and decompressive sacroplasty. A double pantaloon Risser cast was utilized postoperatively for 6 weeks followed by a single thigh extension thoracolumbar spinal orthosis for an additional 6 weeks. Radiculopathy findings resolved postoperatively. At 5-year radiographic follow-up, spinal balance had been restored, and the T5 to L3 scoliosis was resolved.
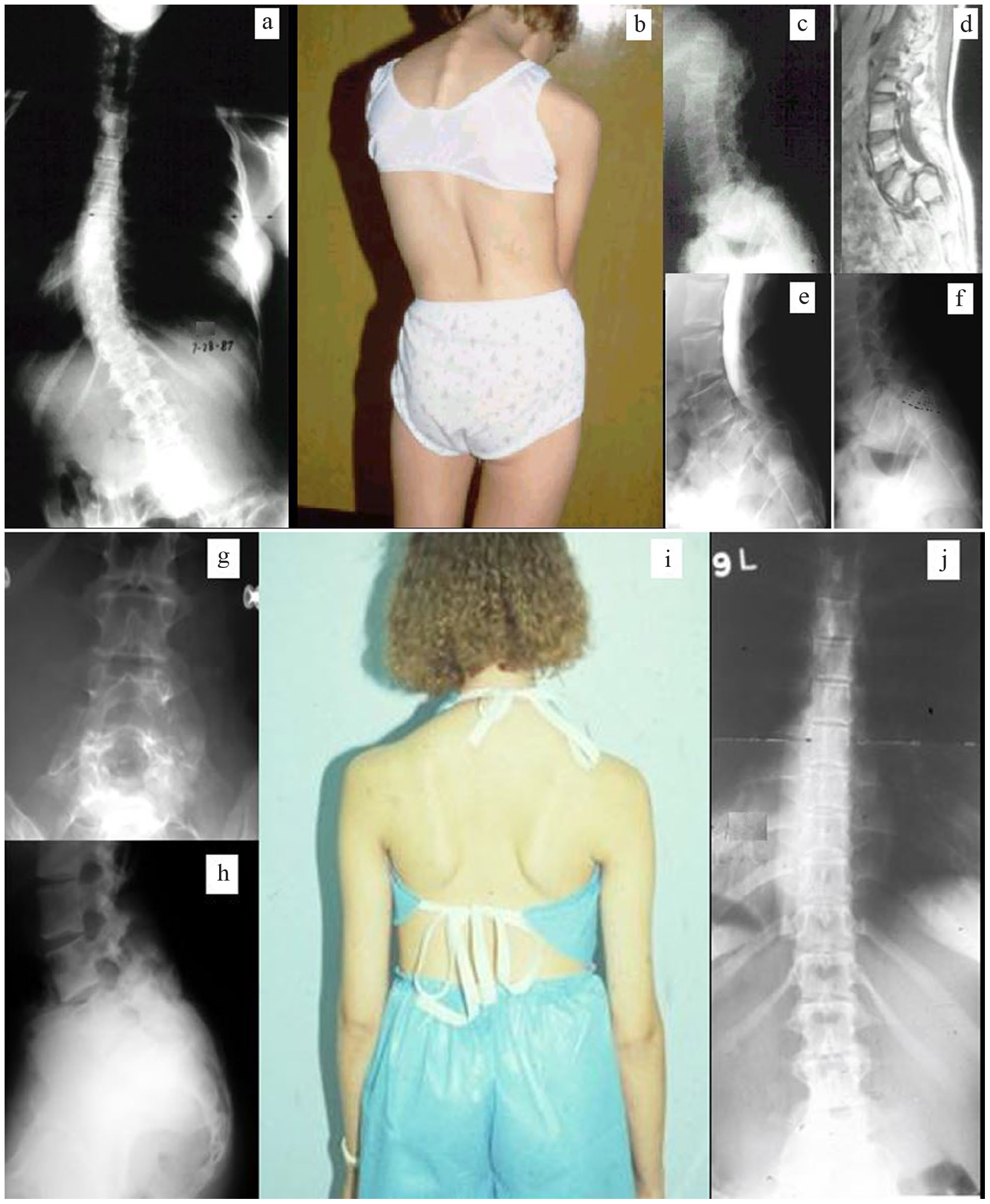
Thriteen-year-old female. (a) Preoperative posteroanteror scoliosis radiograph demonstrating large apex left curve with leftward trunk shift. (b) Preoperative clinical photograph showing curve morphology and trunk imbalance. (c) Preoperative lateral lumbosacral radiograph revealing high-grade spondylolisthesis. (d) Preoperative sagittal magnetic resonance image further illustrating slip severity. (e) Myelographic image revealing stenosis. (f) Preoperative plan outlining planned sacroplasty/decompression. (g) Five-year postoperative anteroposterior lumbosacral radiograph. (h) Five-year postoperative lateral lumbosacral radiograph revealing L4 to S1 posterior fusion. (i) Five-year postoperative clinical photograph showing improved balance and alignment. (j) Five-year postoperative posteroanterior scoliosis radiograph demonstrating curve resolution.
Case #3
A 13-year-old female presented with non-radicular low back pain and abnormal gait (Figure 3). Physical examination revealed tight hamstrings and a forward stooped posture with trunk shift to the right. There were no sensorimotor deficits in the lower extremities. A 51% L5-S1 spondylolisthesis and apex right 40° T3 to L2 scoliosis with rightward trunk shift were noted. Magnetic resonance imaging revealed central stenosis at L5-S1 and no significant disk disease. An in situ L4 to S1 posterior spine fusion with autogenous iliac crest bone graft was performed. A postoperative double pantaloon Risser cast was utilized for 6 weeks followed by a thoracolumbar spinal orthosis with thigh extension for a second 6 weeks. Satisfactory posterior spine fusion was achieved from L4 to S1 and sagittal rotation decreased from 35° to 22°. Low back pain and hamstring tightness resolved, and at 2-year radiographic follow-up, the T3 to L2 scoliosis had diminished to 12°.
Thriteen-year-old female. (a) Preoperative posteroanterior scoliosis radiograph demonstrating large apex right curve with rightward trunk shift. (b) Preoperative lateral scoliosis radiograph with forward lean and lumbosacral kyphosis. (c) Preoperative lateral lumbosacral radiograph showing high-grade spondylolisthesis. (d) Preoperative sagittal magnetic resonance image further illustrating slip severity. (e) Two-year postoperative posteroanterior scoliosis radiograph demonstrating 12° residual curve. (f) Two-year postoperative lateral scoliosis radiograph showing normalized standing posture and sagittal profile. (g) Two-year postoperative side view clinical photograph consistent with lateral radiograph. (h) Two-year postoperative front view clinical photograph demonstrating restored trunk balance. (i) Two-year postoperative AP lumbosacral radiograph showing L4-S1 fusion (more robust on the right side). (j) Two-year postoperative lateral lumbosacral radiograph showing L4-S1 fusion.
Case #4
A 15-year-old female sought care for low back pain and bilateral burning sensation in her legs extending to below the knees (Figure 4). A 56% L5-S1 spondylolisthesis and apex left 33° L1 to L4 scoliosis were noted. In addition to a posterior decompression consisting of L5 laminotomy and sacroplasty, an L4 to S1 posterior spine fusion was performed utilizing autogenous iliac crest bone graft. At 6.5-year radiographic follow-up, the L1 to L4 scoliosis had decreased to 21°.
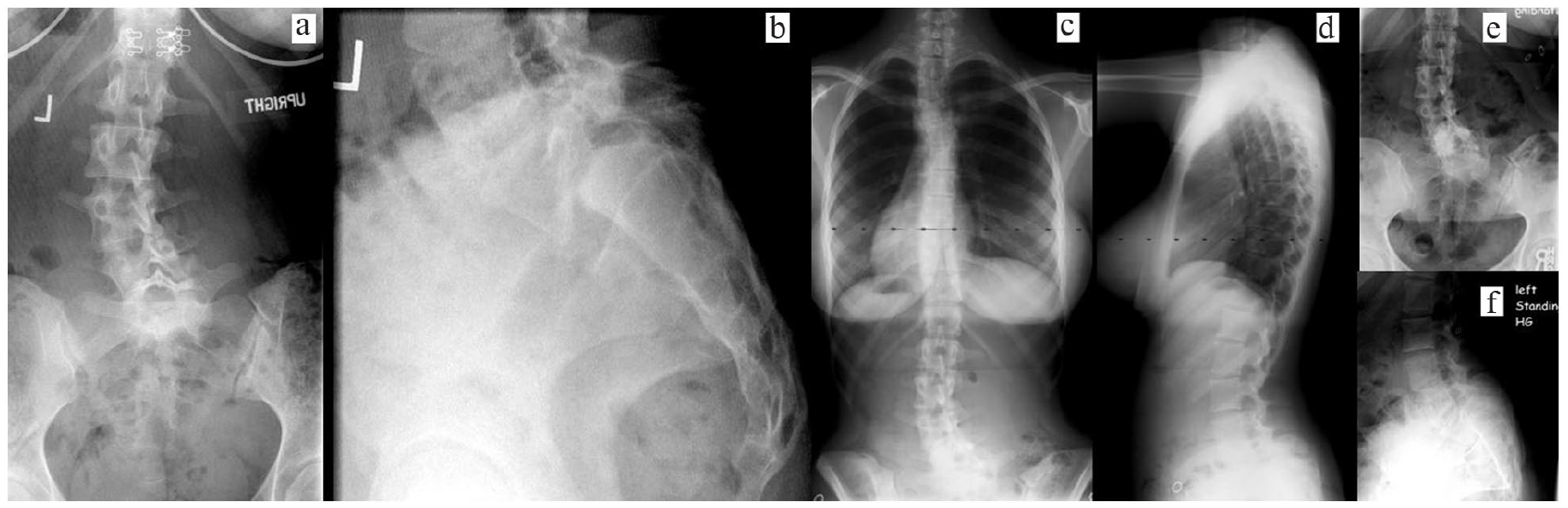
Fifteen-year-old female. (a) Preoperative anteroposterior lumbosacral radiograph demonstrating apex left lumbar scoliosis. (b) Preoperative lateral lumbosacral radiograph showing high-grade spondylolisthesis. (c) Two-year postoperative posteroanterior scoliosis radiograph. (d) Two-year postoperative lateral scoliosis radiograph. (e) Six-year anteroposterior lumbosacral radiograph. (f) Six-year lateral lumbosacral radiograph.
Discussion
The current study summarizes 13 well-documented cases of olisthetic scoliosis (4 new cases and 9 from the literature) that occurred in the setting of symptomatic high-grade spondylolisthesis. All were treated via a primary posterior lumbosacral fusion strategy. Two patients (a 16-year-old male and a 17-year-old female) had documented postoperative curve progression of 8° and 20°, respectively. Eleven of the 13 patients demonstrated curve improvement following isolated lumbosacral fusion. Three of these patients experienced a decrease in curve magnitude anywhere from 12° to 28°, and eight patients enjoyed complete resolution (≤10°) of their scoliosis. The average age of the nine female patients who experienced curve improvement was 13 years (range: 11–17 years), and the two males were 15 and 16 years of age. Due to the relative rarity of this specific condition, many pediatric spine surgeons may have little or no experience with olisthetic scoliosis cases such as those currently presented.
Scoliosis occurring in association with spondylolisthesis is not a new phenomenon. As early as 1882 (more than a decade before the introduction of Roentgenograms), the German author Franz Ludwig Neugebauer 20 identified the association between spondylolisthesis and scoliosis. He described a 45-year-old female spondylolisthesis patient he had examined in Strasburg, Germany who had experienced low back pain since she was a young girl. He stated that her “spinal column exhibited a compound scoliotic rotation—in the cervico-dorsal portion to the right, in the dorso-lumbar portion to the left, and in the lumbo-sacral back to the right. . . .” 20 His accompanying drawings of the patient clearly illustrate flattening of the buttocks and a leftward truncal shift (Figure 5). It would be nearly eight decades before a surgical treatment philosophy for spondylolisthesis would evolve.
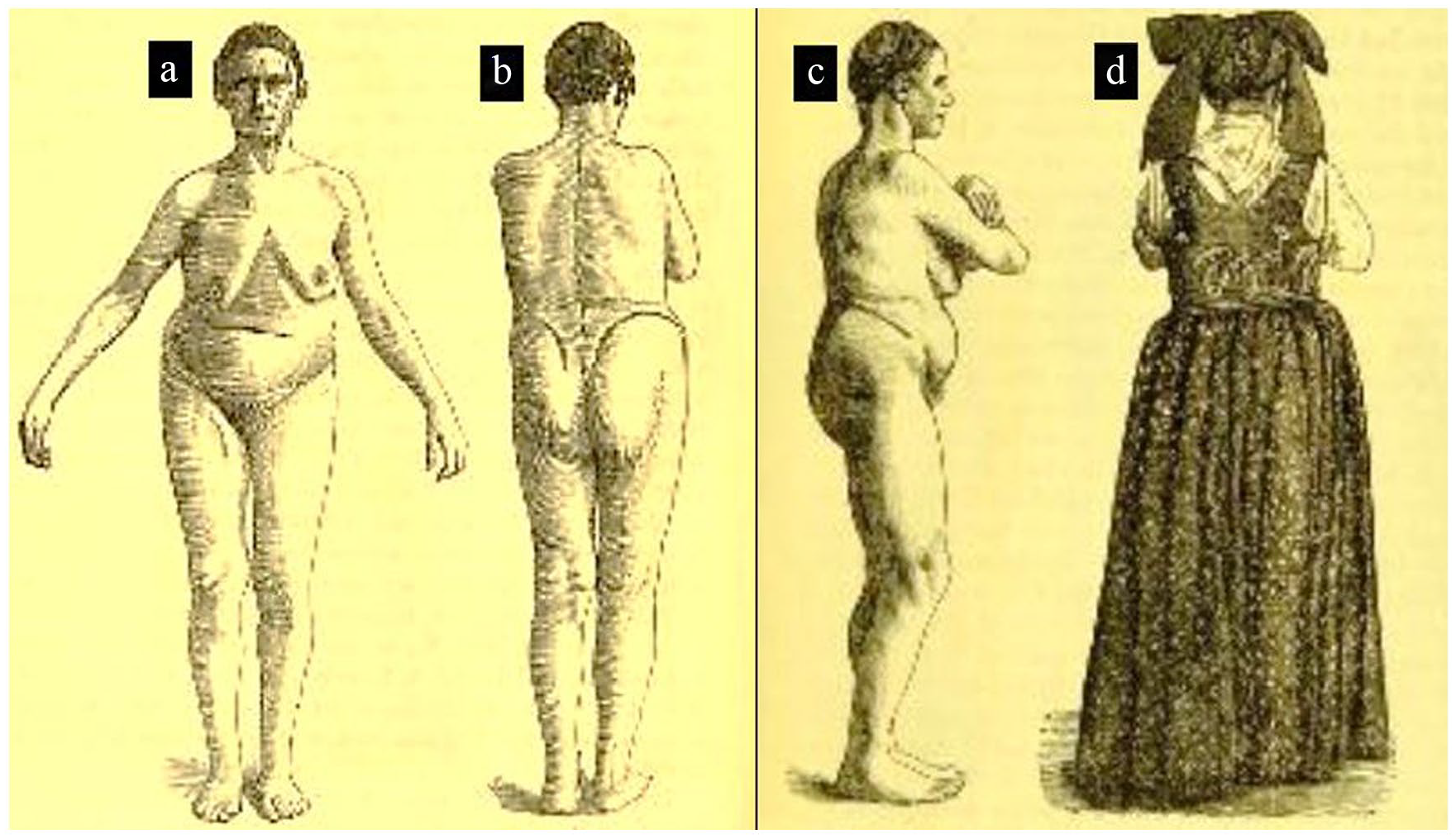
Neugebauer’s 45-year-old patient. (a) Frontal clinical view showing leftward trunk shift. (b) Clinical view from the back showing some pelvic obliquity and mild leftward trunk shift. (c) Right side clinical view showing flattening of the buttocks and flexed posture of the knees likely due to hamstring tightness. (d) Clinical view of clothed patient from the back showing all clinical deformities hidden other than mild pelvic obliquity.
The June 1961 report by Phalen and Dickson 21 showed that these authors were well aware of both the hamstring tightness and scoliosis associated with high-grade spondylolisthesis, but they thought it best treated via isolated laminectomy. In September of 1961, Risser and Norquist 7 offered their description of nine children with scoliosis they considered to be secondary to severe lumbosacral spondylolisthesis. They used the term “sciatic scoliosis” and considered early adequate lumbosacral fusion to be their preferred method of relieving the lumbar spasm and preventing progression of the scoliosis. 7 Henning Tøjner 22 is credited with what would appear to be the first use of the term “olisthetic scoliosis,” although his patients were almost exclusively adults with small lumbar curves. Some authors have only applied the olisthetic label to lumbar curves with some rotational component. In 1978, Fisk et al. 9 analyzed the relationship between scoliosis, spondylolysis, and spondylolisthesis in 39 patients and stated that the need for surgical intervention was thought to “parallel the indications for each problem arising independently.” These same authors clearly recognized the potential for nonstructural scoliosis to spontaneously correct following successful lumbosacral fusion.
This pragmatic approach was embraced by many other authors who understood the importance of ascertaining whether scoliosis associated with high-grade spondylolisthesis was structural or not.2,23 –26 The use of bending or recumbent scoliosis radiographs to assess curve flexibility and determining the presence or absence of vertebral rotation are both important concepts in the setting of suspected olisthetic scoliosis.11 –13 In addition to lack of significant apical rotation of the spine noted by evaluation of the pedicles, the almost complete correction of the scoliosis on supine reverse side bending x-rays is diagnostic as well as predictive of success following surgical stabilization of the high-grade spondylolisthesis. The senior author agrees wholeheartedly with flexibility radiographs and apical assessment of vertebral rotation for surgical decision-making. Both patients presented in the current study who demonstrated curve progression also had noteworthy apical vertebral rotation.
Not all authors have embraced this same philosophy. Crostelli and Mazza 27 stated their opinion that for all practical purposes the spinal curvature in adolescents with spondylolisthesis should be considered idiopathic in nature and treated accordingly. Researchers from the Hospital for Joint Disease reported their experience with adolescent idiopathic scoliosis and coexisting spondylolisthesis and found that low-grade slips did not progress following successful scoliosis surgery (posterior spinal fusion). Their study also included three symptomatic high-grade slip patients who had their scoliosis surgery approximately 6 months following successful lumbosacral fusion with the two fusion masses being separated by at least three levels. 28 These authors did not mention the concept of primary lumbosacral fusion and monitoring of the response of the scoliosis as an alternative treatment strategy. Similarly Mikhaylovskiy and Belozerov 29 reported 31 scoliosis patients (average primary curve 67°) with concomitant spondylolisthesis (largely asymptomatic and mostly grade I). These Russian authors acknowledged a subset of the literature supporting spontaneous improvement of scoliosis following lumbosacral fusion but reported no personal experience with this phenomenon.
There is general agreement that the root cause of olisthetic scoliosis is nerve irritation and muscle spasm accompanying high-grade spondylolisthesis.9 –12,26 There may or may not be associated pain. The ubiquitous hamstring spasm and frequent sensory radiculopathy are clear indicators of nerve irritation. 30 This is in sharp contradistinction to asymptomatic low-grade spondylolisthesis, which has little of no impact on the overall course of treatment of adolescent idiopathic scoliosis. 31 An important study from Israel found that the rate of scoliosis in individuals with symptomatic spondylolisthesis was almost twice that of those with asymptomatic slips. 32
The precise surgical tactic used for lumbosacral fusion appears to be less important than achieving robust stable lumbosacral fusion. Successful long-term follow-up studies have been published for high-grade spondylolisthesis patients treated both by uninstrumented in situ techniques as well as instrumented reduction techniques.33,34 The most common surgical strategy (8 out of 13) employed in the patients reported in this study was posterior in situ lumbosacral fusion followed by a period of postoperative external immobilization. It should be noted that the two cases of progression of the scoliosis following lumbosacral fusion (a 16-year-old male and a 17-year-old female) occurred in this uninstrumented in situ group. The other five patients had posteriorly instrumented fusions (usually in association with efforts at reduction and decompression) with two patients also receiving so called anterior column support via transforaminal lumbar interbody fusion. Thus, there is a spectrum of surgical tactics that have been utilized in this patient population.
The current research must be interpreted within the context of the study design. There was notable treatment heterogeneity among the cases in this study, the key similarity being a solid stable lumbosacral fusion. The new cases presented were drawn from the two authors’ practices at a tertiary care children’s hospital that has spanned more than 40 years. The nine well-documented cases drawn from the literature covered a comparable time period of over five decades. These facts speak to the rarity of the specific condition of children with symptomatic high-grade spondylolisthesis and scoliosis, and thus, the true numerator and denominator for such olisthetic scoliosis remain unknown. However, it has been the authors’ experience that few spine surgeons (pediatric or adult) have actually seen or treated such cases, and many are not aware of the possibility of resolving scoliosis following successful lumbosacral fusion. Thus presenting four new cases and summarizing those from the literature offers potential value to future spine surgeons called upon to treat children with olisthetic scoliosis.
Conclusion
The coexistence of symptomatic high-grade spondylolisthesis and scoliosis should stimulate the orthopedic surgeon to assess curve flexibility and apical rotation of the curve. In the scenario of a long sweeping curve (often with trunk imbalance) with little or no apical rotation, one should give strong consideration to primary treatment of the spondylolisthesis followed by extended observation of the scoliosis (often for a year or more). Older teenagers and those with evidence of substantial apical rotation may experience curve progression although additional surgical treatment of the scoliosis may not become necessary. The current study is both the largest collection of new resolving olisthetic cases ever reported and the first to review, remeasure, and summarize the other well-documented cases from the literature. It is important for pediatric spine surgeons to be aware of the phenomenon of spontaneous improvement of olisthetic scoliosis following successful treatment of high-grade spondylolisthesis via lumbosacral fusion.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231182427 – Supplemental material for Spontaneous improvement of olisthetic scoliosis in children following lumbosacral fusion for high-grade spondylolisthesis: A report of four new cases and systematic review of the literature
Supplemental material, sj-pdf-1-cho-10.1177_18632521231182427 for Spontaneous improvement of olisthetic scoliosis in children following lumbosacral fusion for high-grade spondylolisthesis: A report of four new cases and systematic review of the literature by Charles T Mehlman and Alvin H Crawford in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
C.T.M. conceived and designed, wrote manuscript, and analyzed and interpreted data. A.H.C. conceived and designed, reviewed and approved manuscript, and analyzed and interpreted data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Primary data associated with this study are available for review upon request.
Ethical statement
This study was reviewed and determined to be exempt by the Cincinnati Children’s Hospital Institutional Review Board (protocol 2019-10-01) on 14 August 2020. Patient data will not be shared with outside parties.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.