
Abstract
Purpose:
Managing severe scoliosis is challenging and risky with a significant complication rate regardless of treatment strategy. In this retrospective comparative study, we report our results using a three-rod compared to two-rod construct in the surgical treatment of severe spine deformities to investigate which technique is safer, and which provides superior radiological outcomes.
Methods:
Forty-six consecutive patients undergoing posterior spine fusion for scoliosis between 2006 and 2017 were identified in our institutional records. Inclusion criteria were minimum coronal deformity of 90°, age < 18 years at the time of surgery and a minimum 2 years of follow-up. Radiographic and clinical parameters, as well as post-operative complications were compared between the two groups.
Results:
There were 21 patients in the three-rod group and 25 in the two-rod group. The mean preoperative major coronal deformity was 100°± 9 and 102°± 10 in the three-rod and two-rod, respectively (p = 0.6). The average major curve correction was 51% and 59% in three-rod and two-rod groups, respectively (p = 0.03). The post-operative thoracic kyphosis was 30°± 11 and 21°± 12 in the three-rod and the two-rod groups, respectively (p = 0.01). The surgical time was 476 ± 52 and 387 ± 84 min in three-rod and two-rod, respectively (p < 0.01). One patient in the two-rod cohort showed permanent post-operative sensory deficit. There were three unplanned returns to operating theater in the two-rod group.
Conclusions:
Coronal correction was better with two-rod, whereas sagittal balance was superior with three-rod. Both techniques achieved balanced spine treating severe scoliosis. The two-rod technique was associated with a higher likelihood of requiring revision surgery.
Level of evidence:
level 3.
Keywords
Introduction
Posterior instrumented correction and fusion with a pair of rods is the most common strategy used to surgically treat pediatric scoliosis (a two-rod technique (2R)). As technology and techniques have progressed, surgeons are able to treat larger, stiffer curves with confidence. Nevertheless, treating stiff curves greater than 90° carries significant risk, and methods that can safely correct severe deformities are a necessary tool.1–5
Surgeons can select from several strategies when managing severe scoliosis. Alongside 2R constructs with or without osteotomy, these include preoperative halogravity traction (HGT), three-column osteotomy, anterior release and posterior fusion, and three-rod (3R) constructs, each with their relative merits and disadvantages.6–9 Pre-operative HGT comes with a 1% risk of neurological complications, and three-column osteotomy with an high of independent post-operative neurological complication when compared to 2R posterior instrumented fusion alone (odds ratio (OR) = 1.7, 95% confidence interval (CI) = 1.11–2.85, p = 0.015).6,7 Anterior release followed by posterior fusion has historically been commonplace, however, has fallen from favor as the correction achieved has been shown to be comparable to posterior correction alone. 10
The 3R technique was first described by Cotrel 11 and uses the sequential application of two rods to the concavity of the coronal deformity to create a corrective distraction before applying a stabilizing rod on the convexity. Recent work by Rocos et al. 9 has shown that it is able to safely and effectively correct severe, stiff deformities. The technique has several possible advantages over 2R constructs including a stiffer construct and the option to partially release the sequential correction in response to neuromonitoring deterioration.9,12
The risks and effectiveness of both three-column osteotomy and HGT have been defined relative to 2R constructs, however, no such comparison has been made between 2R and 3R.7,13–15 In this study, we compare the radiographic results of these techniques and the complications associated with their use. We hypothesize that with the ability of the 3R technique to respond to changes in intraoperative neuromonitoring, the technique will offer a lower rate of neurological complication while offering a similar correction in both the coronal and sagittal planes, and an equivalent overall rate of complication.
Methods
Institutional research ethics board approval was granted for this retrospective case series. Every patient aged less than 18 years treated at our institution between 2006 and 2017 for scoliosis with a coronal angular deformity exceeding 90° and 2 years of documented follow-up was included. Patients were excluded if they were treated for a congenital deformity, or using HGT, three-column osteotomy or anterior release followed by posterior instrumented fusion. Patients were also excluded if fused to the pelvis. Eligible patients were categorized into two groups, dependent on the surgical technique used to correct their deformity as selected by the operating surgeon. Each case was undertaken with intraoperative neuromonitoring of somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs).
The 3R group was treated with a 3R technique by a single surgeon (Figure 1). 9 After recording baseline evoked potentials, perioperative skeletal traction and exposure, anchors for the short rod are placed at the concave apex of the curve. Often, these are hooks because of the small size of the pedicles at the apex of the curve. The short rod is then attached to the proximal and distal anchors before it is brought to the apical anchor that creates corrective translation, further improved by rod rolling and in situ contouring. The long concave rod is then inserted and contoured in situ to further correct the deformity. Finally, a convex rod is fixed to the contralateral side of the spine to stabilize the construct. The final step is to affix one proximal and one distal crosslink connecting the two long rods and one short crosslink connecting the short apical rod to the concave rod.
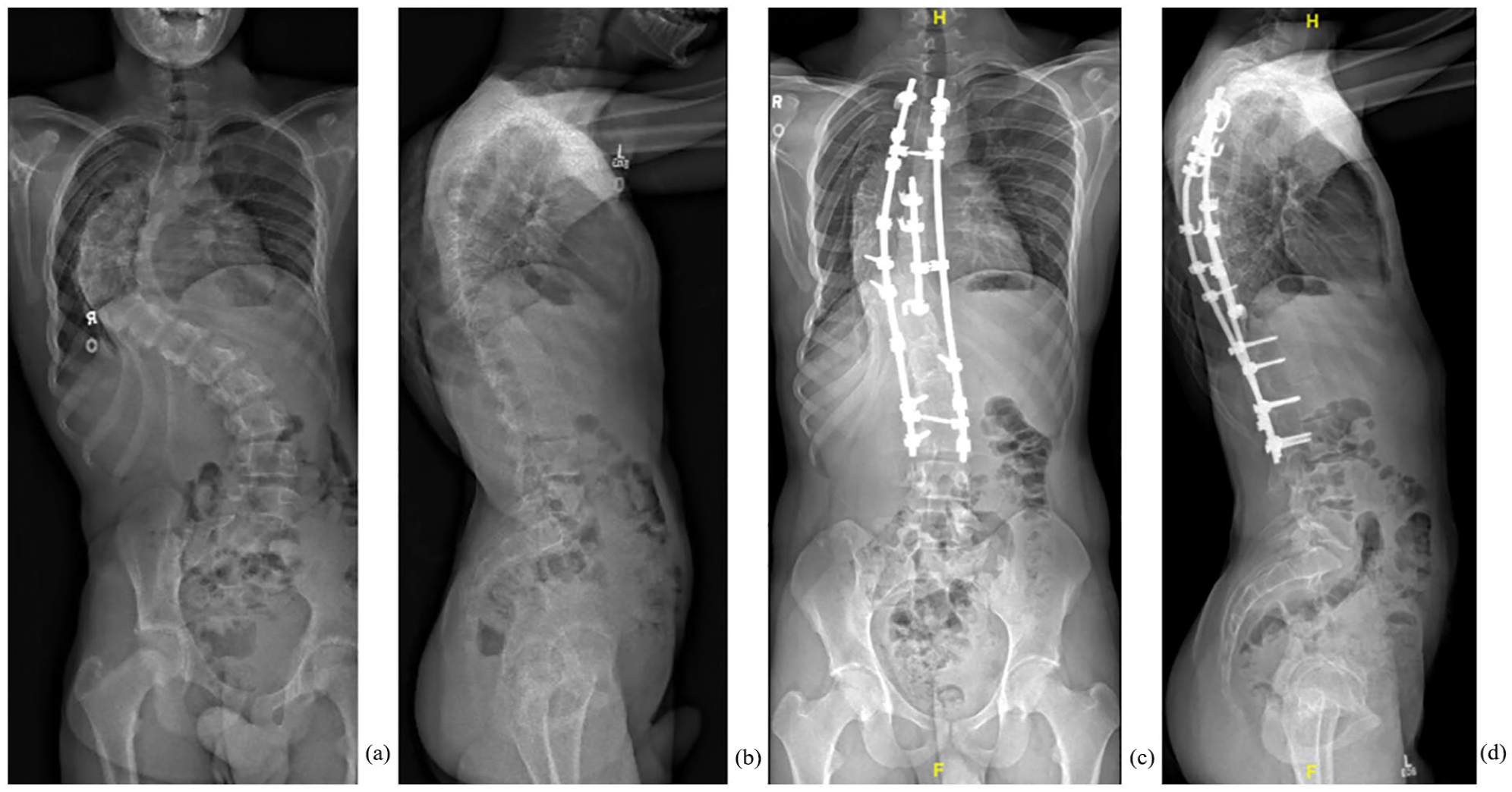
A 12.5-year-old boy with AIS. (a) Pre-operative anteroposterior radiographic showing 45° proximal thoracic, 108° main thoracic, and 66.3° lumbar scoliosis. (b) Pre-operative lateral radiograph showed 40° thoracic kyphosis and 53° lumber lordosis. (c) Anteroposterior radiograph with three-rod constructs at post-operative. The proximal thoracic curve was corrected to 31°, main thoracic curve to 37°, and lumber curve to 27°. (d) Lateral radiograph at post-operative. Thoracic kyphosis was 33° and lumber lordosis was 49°. AIS: adolescent idiopathic scoliosis.
The 2R group was treated with a conventional two rod technique by a second independent surgeon (Figure 2). Between 2006 and 2011, the 2R group underwent posterior instrumented fusion with accompanying intraoperative traction. Since then, 2R patients have undergone posterior instrumented fusion with two rods and periapical posterior column osteotomies (PCOs) without intraoperative traction.
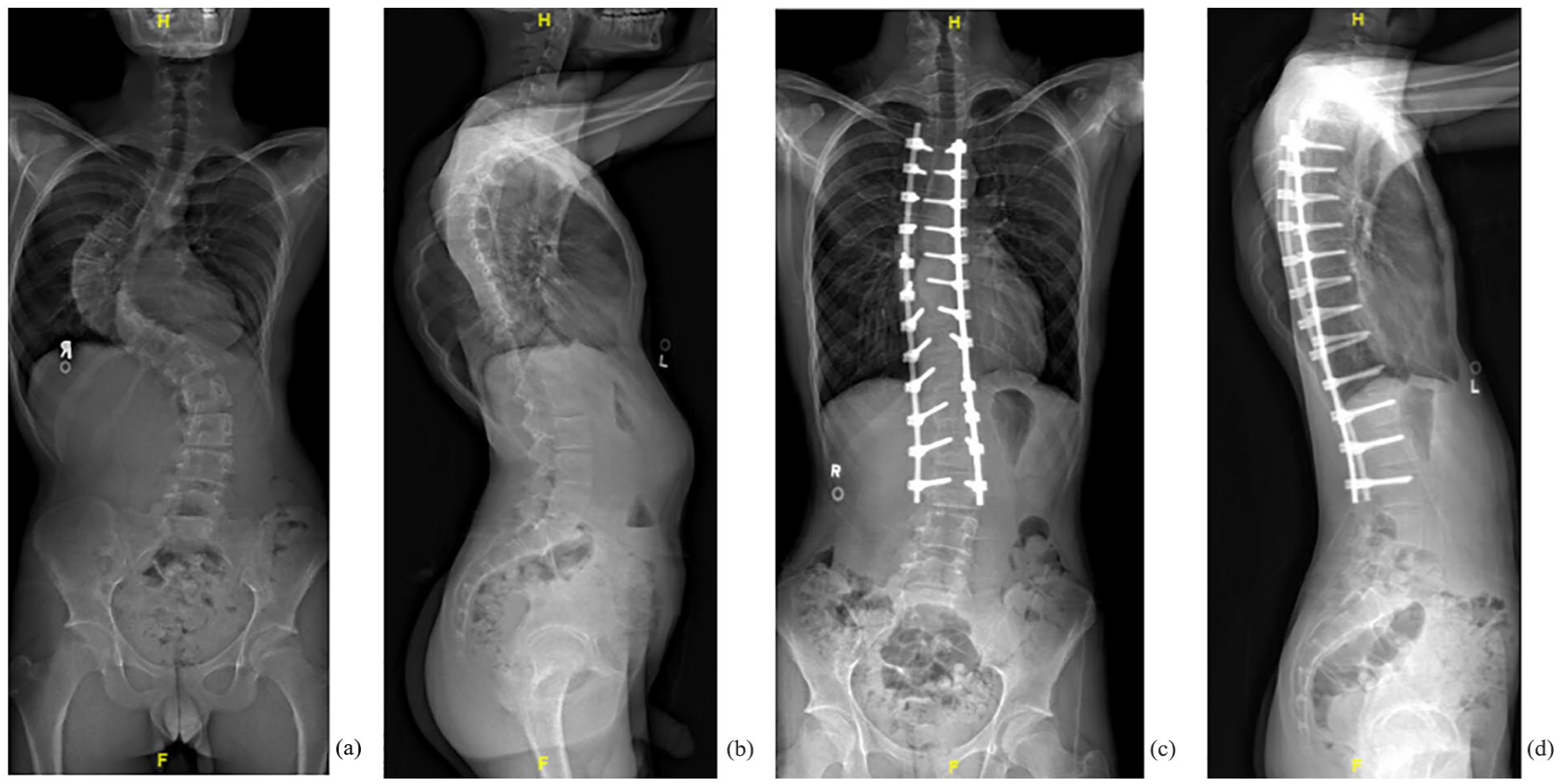
A 15.9-year-old boy with AIS. (a) Pre-operative anteroposterior radiographic showed 41° proximal thoracic, 92° main thoracic, and 57° lumbar scoliosis. (b) Pre-operative lateral radiograph showed 44° thoracic kyphosis and 59° lumber lordosis. (c) Anteroposterior radiograph with two-rod constructs and Smith-Peterson osteotomy at post-operative. The proximal thoracic curve was corrected to 16°, main thoracic curve to 19°, and lumber curve to 17°. (d) Lateral radiograph at post-operative. Thoracic kyphosis was 27° and lumber lordosis was 41°. AIS: adolescenr idiopathic scoliosis.
The clinical records were scrutinized for the surgical duration, blood loss, neuromonitoring events (SSEPs and MEPs), critical care and hospital length of stay, and early (within 30 days) or late (after 30 days) complications. Anteroposterior and lateral full-length spinal radiographs were assessed for global alignment, angular deformity using the Cobb method and flexibility. Sagittal balance was defined as the distance between C7 plumb line and the posterior superior corner of S1. Thoracic kyphosis (TK) was measured from the superior endplate of T5 to the inferior endplate of T12. Curve flexibility was assessed using standing bending films when patients could stand, and traction films while supine when standing was not possible. Flexibility was expressed as a percentage of the pre-operative deformity. Thoracic hypokyphosis was defined under 20°.
The data were analyzed using R (version 3.6.1, The R Foundation for Statistical Computing, Vienna, Austria). Distributions of variables are given as means with standard deviation (SD) and ranges. Unpaired t-tests, Fisher’s exact, and χ2 tests were used to assess the significance of any difference in categorical data between two groups. P-values of less than 0.05 were considered to indicate statistical significance.
Results
The 3R group comprised 14 female and seven male patients (n = 21) with a mean age of 14.5 years (range: 9.0–17.5 years) and a mean follow-up of 3.6 years. Eight patients were diagnosed with idiopathic scoliosis, seven with neuromuscular, and six with syndromic-associated deformity (Table 1). The mean pre-operative coronal angular deformity was 100° (Table 2) with a flexibility of 38%. Global coronal balance was 7.6 mm. TK measured 39° and global sagittal balance 24 mm.
Comparison of baseline characteristics between two groups.
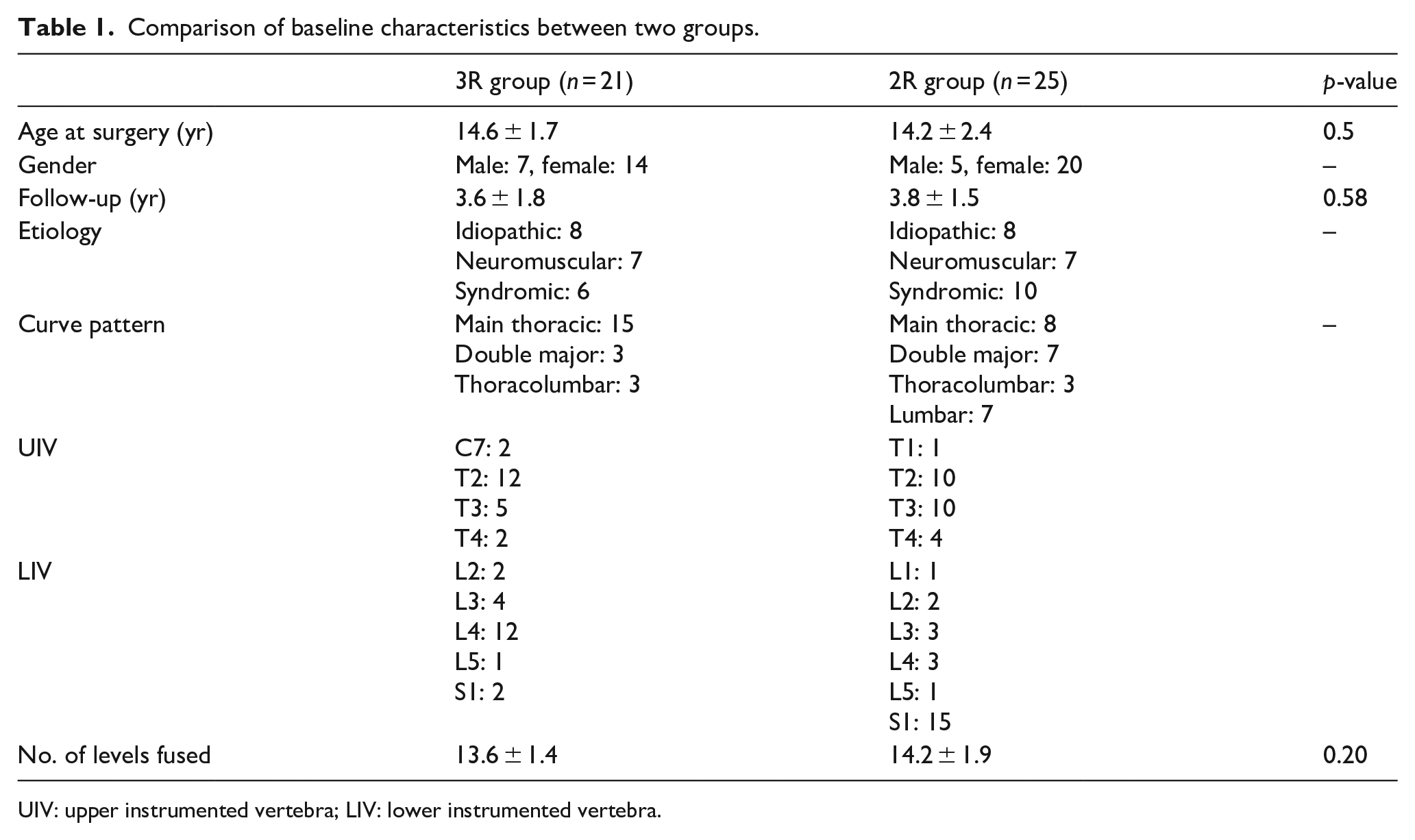
UIV: upper instrumented vertebra; LIV: lower instrumented vertebra.
Comparison of change in coronal curves.
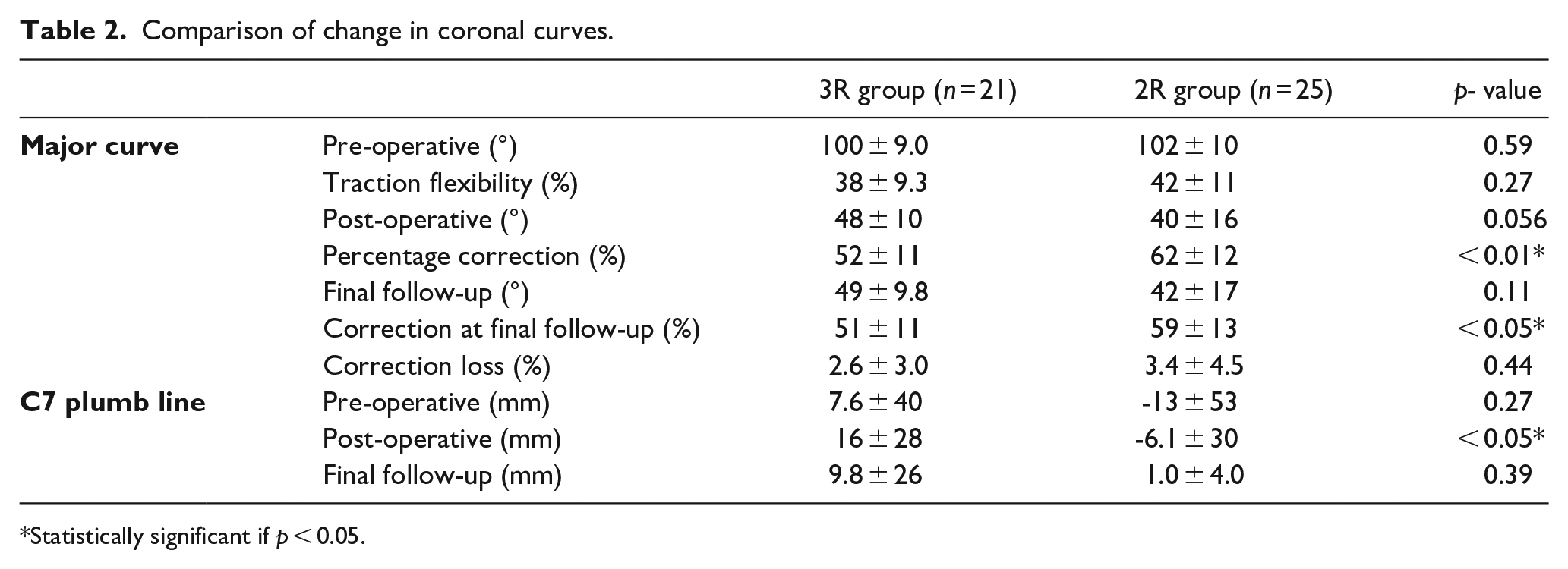
Statistically significant if p < 0.05.
The 2R group comprised 20 female and five male patients (n = 25) with a mean age at surgery of 14.2 years (range: 8.6–17.9) and a mean follow-up of 3.8 years. Eight patients were diagnosed with idiopathic scoliosis, seven with neuromuscular and 10 with syndromic-associated deformity. Thirteen patients were treated with intraoperative traction and all pedicle screw posterior instrumented fusion. The remaining 12 were treated without intraoperative traction with periapical PCO and all pedicle screw constructs. Mean pre-operative coronal angular deformity was 102° with 42% flexibility and –13 mm global coronal balance. TK measured 35° and global sagittal balance –1.2 mm.
There was no significant difference in the age at surgery (t = 0.67, df = 44, p = 0.51) and follow-up (t = –0.56, df = 44, p = 0.58) pre-operative coronal angular deformity (t = 0.54, df = 44, p = 0.59), flexibility (t = 1.17, df = 42, p = 0.27), or coronal balance (t = 1.12, df = 37, p = 0.27) between the two groups. The proportions of each diagnosis were similar in each group (p > 0.05). Post-operatively, the coronal deformity corrected by 51% to 49° in the 3R group and 59% to 42° in the 2R group (p < 0.005). Within the 2R group, there was no difference in the coronal correction achieved between those treated with intraoperative traction and instrumentation and those treated with periapical PCO and instrumentation (Table 2).
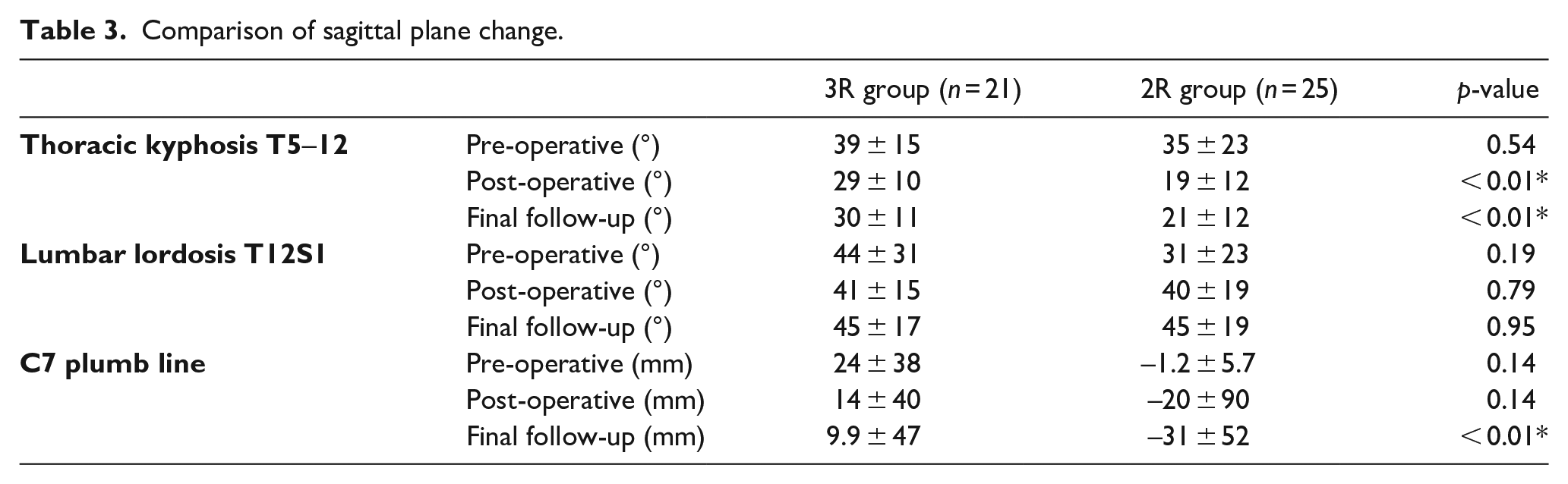
In the sagittal plane, mean TK reduced to 30° in the 3R group and 21° in the 2R group (p = 0.01). There were significantly more thoracic hypokyphosis cases at final follow-up in the 2R group compared to the 3R group (14 versus 4, respectively, OR = 0.19, p = 0.016). Mean post-operative sagittal balance was 10 mm in the 3R and –31 mm in the 2R group (p = 0.01). Within the 2R group, there was no difference in the post-operative global sagittal alignment between those treated with intraoperative traction and instrumentation and those treated with periapical PCO and instrumentation (Table 3).
Comparison of sagittal plane change.
Blood loss and length of stay in critical care or the ward were similar in each group (Table 4). The rate of post-operative transfusion was 13/21 in the 3R group and 18/25 in the 2R group, which failed to reach statistical significance (p = 0.63). The surgical time was 476 ± 52 min in the 3R group and 387 ± 84 min in the 2R, respectively (p < 0.01).
Comparison of other parameters.
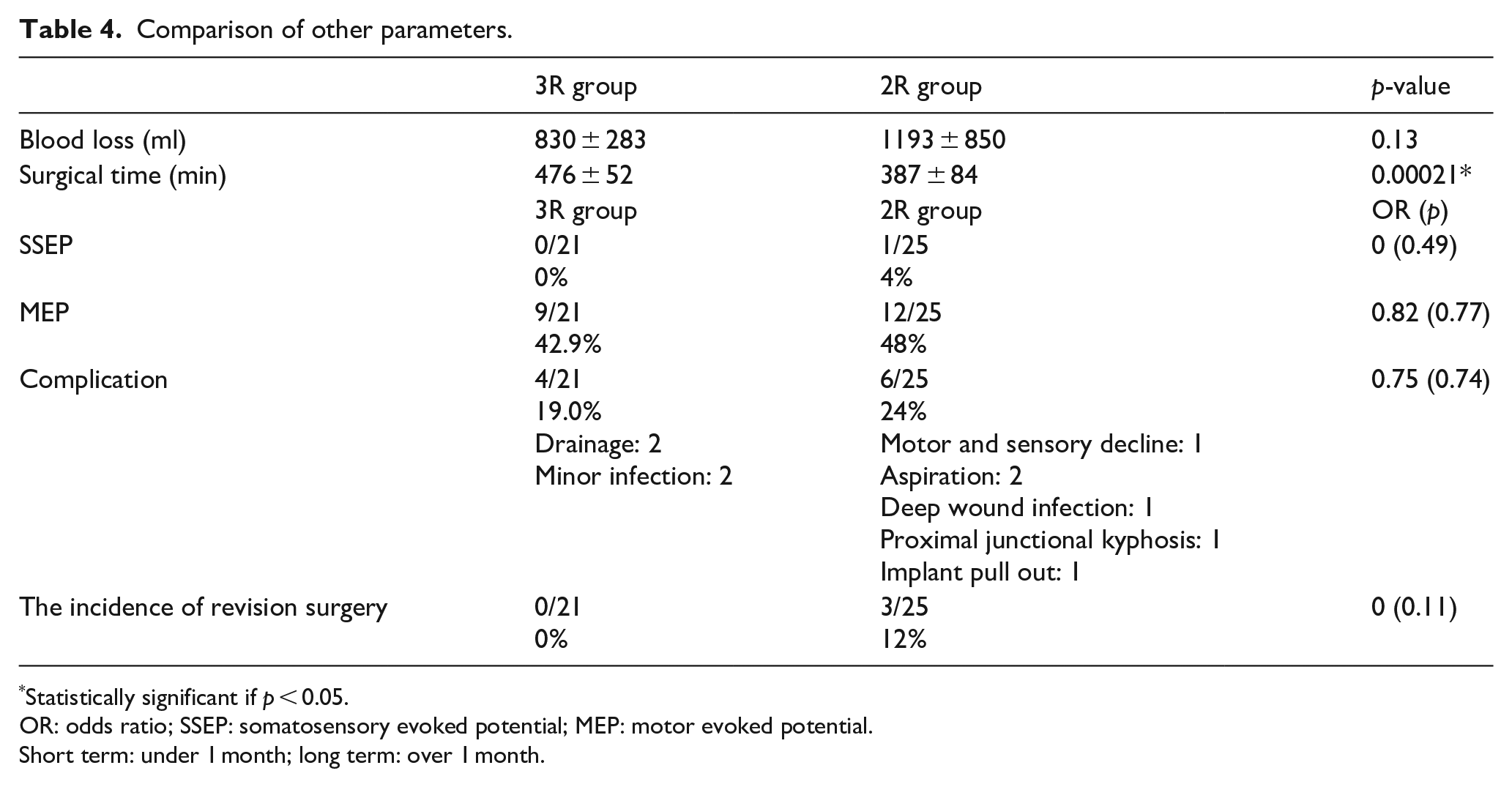
Statistically significant if p < 0.05.
OR: odds ratio; SSEP: somatosensory evoked potential; MEP: motor evoked potential.
Short term: under 1 month; long term: over 1 month.
In the 2R group, a single incidence of SSEP deterioration was observed, with none seen in the 3R group. Diminished MEPs were observed in nine patients in the 3R group and 12 in the 2R group. Neuromonitoring parameters returned to baseline after increasing blood pressure, release of traction or release of correction in every case except a single patient in the 2R group in whom a post-operative sensory-motor deficit was documented consistent with a periapical neurological compromise. Motor function returned to normal by post-operative week 8, however, sensory deficit persisted to final follow-up.
Two patients in the 3R group were diagnosed with a superficial post-operative surgical site infection requiring oral antibiotics and another two required regular community dressings for delayed wound healing. There were no unresolved complications by final follow-up. In the 2R group, three patients required an additional unplanned surgery, one for debridement of a deep wound infection, a second for proximal junctional kyphosis, and another for pull out of implants from the lower instrumented vertebra. Two further patients were diagnosed with post-operative aspiration pneumonia.
Discussion
This analysis suggests that a 2R construct achieves a superior mean coronal correction to 3R regardless of the use of intraoperative traction or PCO. In contrast, the 3R technique appears to have a superior ability to preserve mean global sagittal balance, with the 2R technique creating more thoracic flattening. Moreover, the 3R technique showed no incidents of long-term complication to 3.5 years, whereas the 2R technique showed a single incidence of persistent sensory deficit and three incidents of revision surgery because of infection, proximal junctional, and construct failure.
The correction possible with the 3R technique suggested by these data supports that observed by De Giorgi et al. 12 who reported a series of 36 patients treated with the 3R technique and achieved a 55% correction. However, this series investigated milder deformities than those described here with a coronal angular deformity of 70° and 33% flexibility, in contrast to 100° and 38% in our cohort, respectively. Rocos et al. 9 reported a comparable 50% correction in similarly severe, though stiffer curves.
The surgical time was significantly shorter in the 2R group than that in the 3R group. There may have been differences in surgeon style, screw insertion methods, and time spent on correction. This might be the biggest bias in this study.
Sagittal spinal balance appears to be significantly better addressed with 3R. The reason for that might be explained by a superiority of the hybrid construct as suggested by Kim et al. 16 This may be critical because of the importance of maintaining TK in avoiding poor outcomes. 17 It may be that the 2R technique as employed here could give an excessively aggressive sagittal correction in patients at the lower end of normal TK.
The greater coronal correction achieved in the 2R group is also challenging to explain. It may be that with the additional release achieved through PCO, the increased flexibility of the spine allows more complete correction, though one may reasonably expect that to apply to the sagittal correction as well. Bekmez et al. 18 observed a similar degree of correction in the coronal plane of 60% in a cohort with a mean coronal angular deformity of 94°, through their cohort were all treated with posterior instrumentation and PCO. Further investigations have suggested an all pedicle screw construct may be responsible for the phenomenon via their three column purchase at each motion segment. 19
Rocos et al. 9 showed that the 3R technique is associated with a low risk of complication, with a single incidence of superior mesenteric artery syndrome and a single urinary tract infection. These data from this study show a complication rate of 4/21 (19%) due to delayed soft tissue healing or superficial infection. The cause for this is not clear, though each resolved with dressing management or oral antibiotics. This complication rate is higher than that reported by Reames et al. 20 in their analysis of 19,360 cases of all pediatric scoliosis treated by any surgical means of 10%, however, the authors were unable to assess the severity of the deformities included in the analysis.
The incidence of revision surgery in this series was 3/22 in the 2R and 0/21 in the 3R group. Although the numbers of cases are insufficient to conclude, it nonetheless raises the possibility that revision surgery is more likely in the 2R group. This finding is in line with work by Fruergaard et al. 21 who showed that the 2-year revision risk in pediatric spinal deformity surgery reaches 9.2% in a similarly mixed cohort, exceeding that observed in the 3R group in our study but broadly matching the 12% observed in the 2R group.
Both groups showed instances of deteriorating neuromonitoring signals which returned to baseline through release of correction or traction or an increase in blood pressure. The recommended steps to address neuromonitoring deteriorations have been previously described, however, it is notable that the single case with persisting changes was consistent with a direct cord injury caused by pedicle screw pullout. 22 This is more likely with the 2R technique because pedicle screws are used at the apex, and the translational forces applied in stiff deformity may cause pedicle fracture and translation of the convex screw into the canal, in addition to the risk of PCO at apical levels. 18 The 3R technique avoids this risk through using hooks at the apex, and by allowing the sequential correction of the apex through the two concavity rods and in situ contouring that can be reversed should there be a suggestion of anchor failure or neuromonitoring alert.
Although the 3R technique is overall lower rate revisions, there were no significant differences of complication between two group. From these results, it is impossible to conclude which technique is superior when the focus is on safety. Furthermore, although the percentage of correction was inferior to 2R technique, it may be sufficient correction ability. Especially, for the patients in poor general condition as neuromuscular scoliosis where overall balance is probably important that operator should select 2R or 3R technique based on this study.
There are limitations to this study. The 2R group is heterogeneous in surgical technique. Although it appears that one variation of the 2R technique does not appear superior to another when analyzed independently, it may be that these variables have been incompletely controlled for. Similarly, matching etiologies across both groups was not possible due to the low incidence of such severe deformities. A third potential limitation is the different selection of anchors employed in each strategy which may limit the generalizability of the comparisons. It may be that future investigations would benefit from evaluating a larger series where anchor selection as well as correction strategy can be matched. Finally, it has been established that cobalt chrome provides a greater correction potential due to its higher relative stiffness to titanium alloys. These data do not contain details regarding the specific material used in each case, however, future work comparing diverse techniques should this into consideration. Nevertheless, the potential bias of evolving technique among the 2R patients was analyzed and internal validity within the 2R group was reasonable. Finally, it may be that the persisting neurological complication observed in the 2R group may be avoided by eliminating periapical screws. To determine whether this is the case, additional data would be needed.
Conclusion
Both the 3R and 2R techniques, with or without traction and PCO, can be used to safely and effectively address pediatric scoliosis exceeding 90°. In this series, the 2R technique led to a greater coronal correction and the 3R a superior sagittal alignment. Though the rate of neurological and surgical complication may be equivalent, more soft tissue complication was observed in the 3R group and a higher rate of revision procedures seen in the 2R group.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Reinhard Zeller receives fellowship support from Stryker and SpineVision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Was not required—this study includes completely anonymized radiographs and no individual identifying information.