
Abstract
Purpose:
Slipped capital femoral epiphysis is a common pediatric hip disease and was associated with femoral retroversion, but femoral version was rarely measured. Therefore, mean femoral version, mean femoral neck version, and prevalence of femoral retroversion were analyzed for slipped capital femoral epiphysis patients.
Methods:
A retrospective observational study evaluating preoperative hip magnetic resonance imaging of 27 patients (49 hips) was performed. Twenty-seven untreated slipped capital femoral epiphysis patients (28 slipped capital femoral epiphysis hips and 21 contralateral hips, age 10–16 years) were evaluated (79% stable slipped capital femoral epiphysis, 22 patients; 43% severe slipped capital femoral epiphysis, 12 patients). Femoral version was measured using Murphy method on magnetic resonance imaging (January 2014–December 2021, rapid bilateral 3-dimensional T1 water-only Dixon-based images of pelvis and knee). All slipped capital femoral epiphysis patients underwent surgery after magnetic resonance imaging.
Results:
Mean femoral version of slipped capital femoral epiphysis patients (−1° ± 15°) was significantly (p < 0.001) lower compared to contralateral side (15° ± 14°). Femoral version of slipped capital femoral epiphysis patients had significantly (p < 0.001) wider range from –42° to 35° (range 77°) compared to contralateral side (−5° to 44°, range 49°). Mean femoral neck version of slipped capital femoral epiphysis patients (6° ± 15°) was lower compared to contralateral side (11° ± 12°). Fifteen slipped capital femoral epiphysis patients (54%) had absolute femoral retroversion (femoral version < 0°). Six of the 12 hips (50%) with severe slips and 4 of the 8 hips (50%) with mild slips had absolute femoral retroversion (femoral version < 0°). Ten slipped capital femoral epiphysis patients (40%) had absolute femoral neck retroversion (femoral neck version < 0°).
Conclusion:
Although slipped capital femoral epiphysis patients showed asymmetrically lower femoral version compared to contralateral side, there was a wide range of femoral version, underlining the importance of patient-specific femoral version analysis on preoperative magnetic resonance imaging. Absolute femoral retroversion was prevalent in half of slipped capital femoral epiphysis patients, in half of severe slipped capital femoral epiphysis patients, and in half of mild slipped capital femoral epiphysis patients. This has implications for anterior hip impingement and for surgical treatment with in situ pinning or femoral osteotomy (e.g. proximal femoral derotation osteotomy) or other hip preservation surgery.
Keywords
Purpose
Slipped capital femoral epiphysis (SCFE) is a long known pediatric hip disease with the risk for early hip osteoarthritis and disability. 1 SCFE is a hip disease in adolescents and has an overall incidence of 11 per 100,000 children in the United States 2 and 12 per 100,000 children in Europe. 3 Several factors have been linked to SCFE, for example, femoral retroversion. 4 Femoral retroversion was already found to be associated with SCFE in 1986 5 , but femoral version (FV) was rarely measured in these patients. Various radiographic methods to measure FV were described previously. 6 Measurement of FV for patients with SCFE varies considerably depending on the measurement method. 6 A previous study that described an association of femoral retroversion and SCFE 7 used the femoral neck version. For FV measurement, the center of the femoral head was used as a reference. Because of the displacement of the epiphysis in posteroinferior direction in patients with SCFE, measurements of femoral neck version may underestimate the severity. A finite element study reported increasing stress and strain for the capital femoral physis in case of varus and femoral retroversion 8 ; however, this study was based on a model of one single SCFE patient.
Surgical treatment of SCFE usually depends on the severity of slippage. Femoral osteotomies were applied to correct femoral retroversion mostly for severe and moderate SCFE.9,10 Femoral osteotomies can be performed safely at the intertrochanteric level and can be combined with hip arthroscopy or open proximal femoral bone resection (osteochondroplasty/cam resection) of the post-SCFE deformity.9,10 In situ pinning is commonly performed for acute treatment in hips with SCFE, 11 especially for mild slips.
FV and femoral neck version have been investigated since decades using different modalities12–15, but the true frequency of femoral retroversion in patients with SCFE was rarely investigated. One recent study described an FV of –4 ± 16° (range –39 to 61) and a high prevalence (up to 60%) of femoral retroversion using computed tomography (CT) scans for FV measurement for patients with SCFE. 6
Preoperative measurement of FV allows to detect and to quantify femoral retroversion. This may provide relevant information for planning of adequate surgery in patients with SCFE and could help to estimate the risk for further surgical correction of SCFE deformities. Femoral retroversion was previously reported to contribute to internal rotation of the hip joint, external rotation (out-toeing) of the foot 16 and anterior hip impingement. 17 This could be even more valuable for patients with severe or unstable SCFE to plan the amount of surgical correction of femoral retroversion.
The purpose of this study was, therefore, to report mean FV, mean femoral neck version, and frequency of femoral retroversion for SCFE patients.
Methods
A retrospective, controlled, single-center study at the university hospital for pediatric care was performed and included patients with SCFE treated in an 8-year period (between January 2014 and December 2021). In this time period, 51 hips of 49 patients with SCFE were identified. The institutional patient information system was reviewed for SCFE patients who had undergone preoperative magnetic resonance imaging (MRI) of the hip, independent of treatment. In this time period, the reason for obtaining preoperative MRI (Figures 1 and 2) was to assess slip severity, to measure slip angle, and to assess intra-articular damage (labrum or cartilage) for surgical planning.
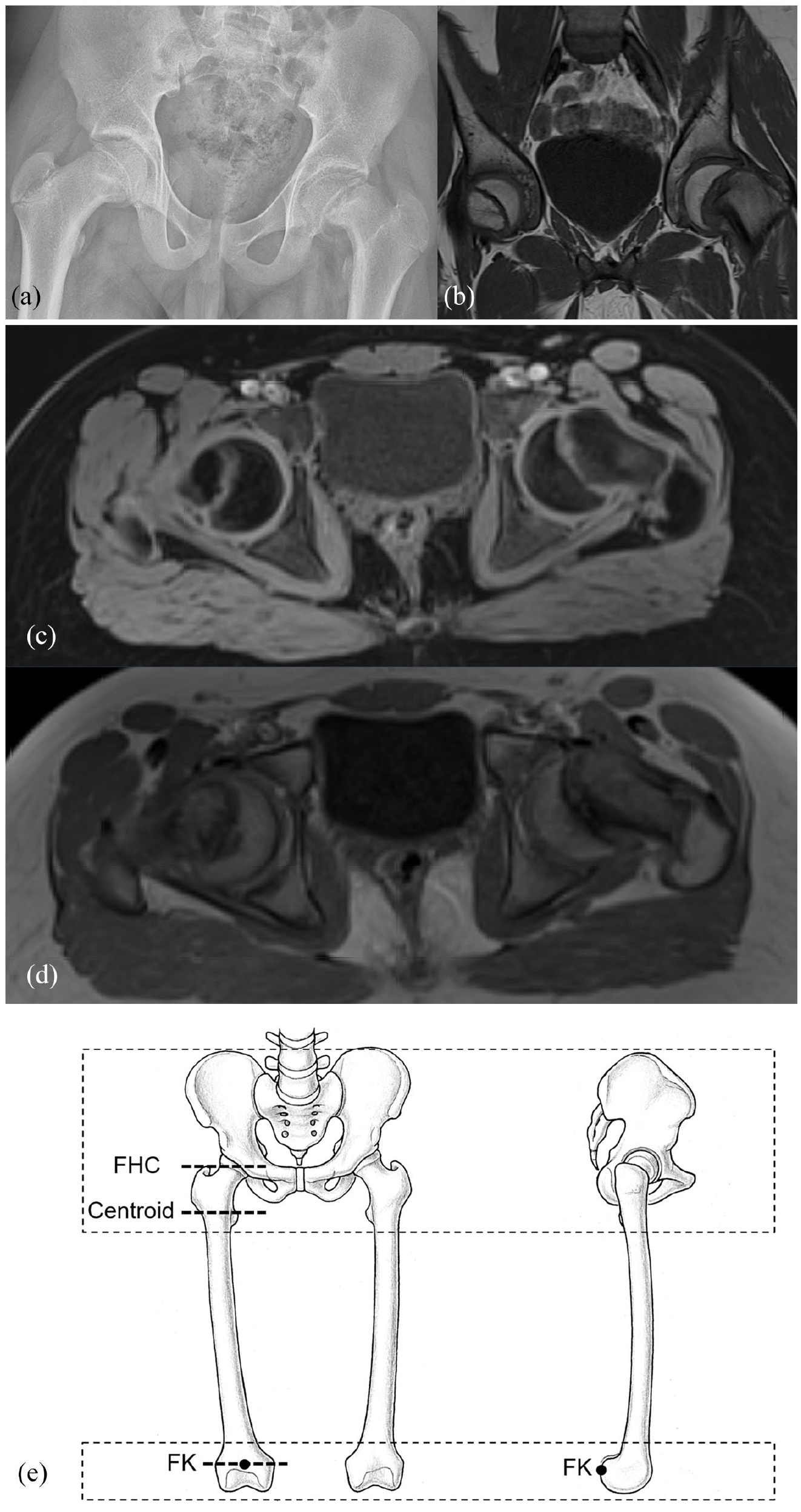
Radiograph (a) and coronal T1 MRI image of the pelvis (b) and 3D T1 VIBE Dixon images (c), water-only images and (d) of a patient with severe SCFE is shown. The field of view of the preoperative MRI of the entire pelvis is shown (e).
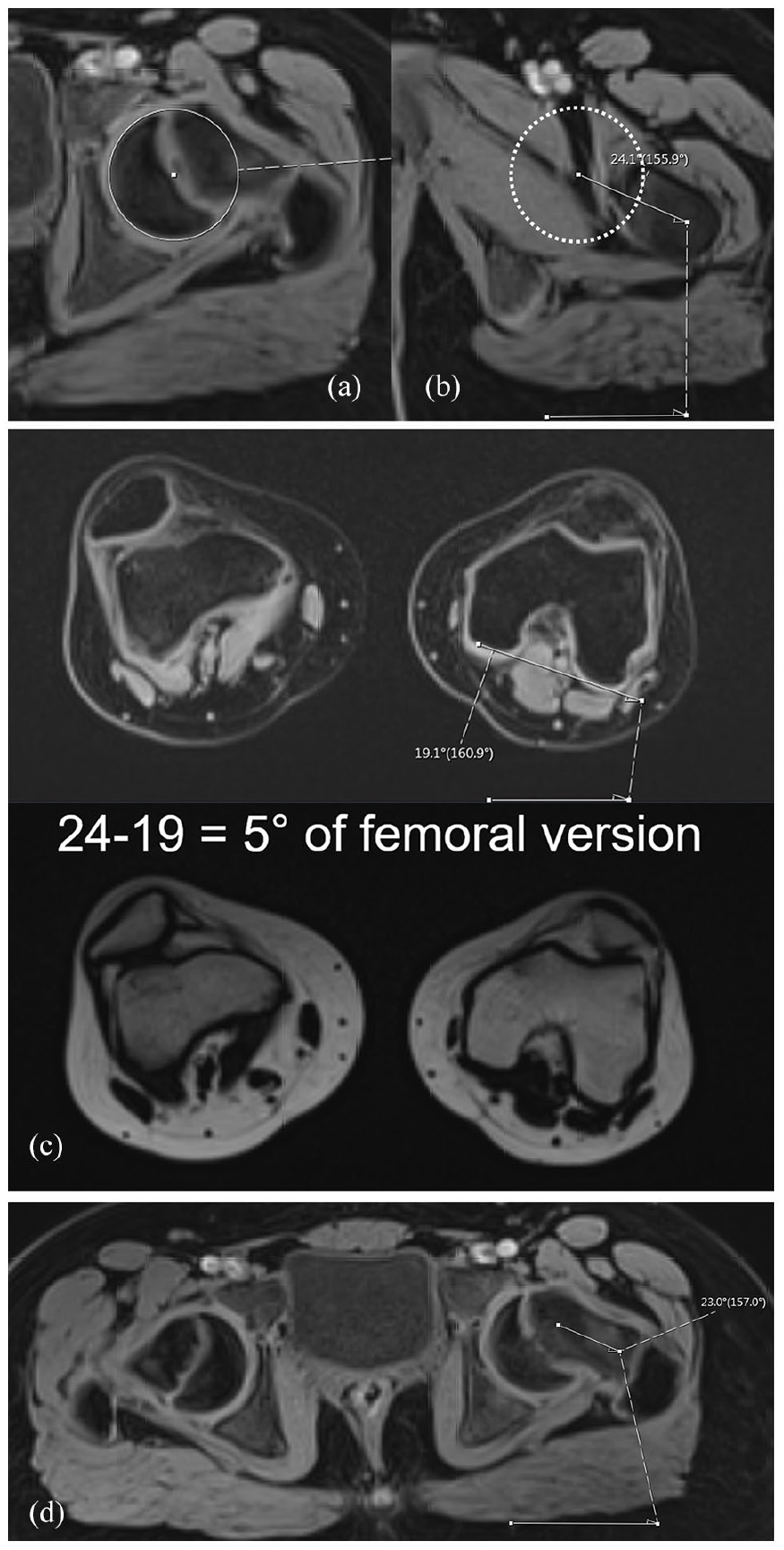
MRI of the pelvis with water-only images of 3D T1 VIBE Dixon of the pelvis (a and b) and of the knee (c) with measurement of femoral version using Murphy method is shown. Measurement of femoral neck version (d) is shown.
Of the 51 hips of 49 patients diagnosed with SCFE, 43 hips of 41 patients underwent preoperative MRI in our institution. Eight patients underwent MRI in another institution and were excluded (Figure 3). Of the 43 hips of 41 patients who underwent preoperative MRI in our institution, 13 hips of 12 patients had no knee images and were excluded (Figure 3). Furthermore, two patients (2 hips) were excluded due to previous hip surgery (one hip) and syndromal diseases (1 hip). Finally, 27 patients (28 SCFE hips, one bilateral SCFE patient) were included who underwent preoperative MRI in our institution with knee images (images of the femoral condyles). Exclusion criteria were incomplete preoperative MRI (without femoral condyles), previous hip surgery (femoral osteotomies or previous in situ fixation), and syndromal disease. Institutional review board approval was obtained, and because of the retrospective review, informed consent was not required.
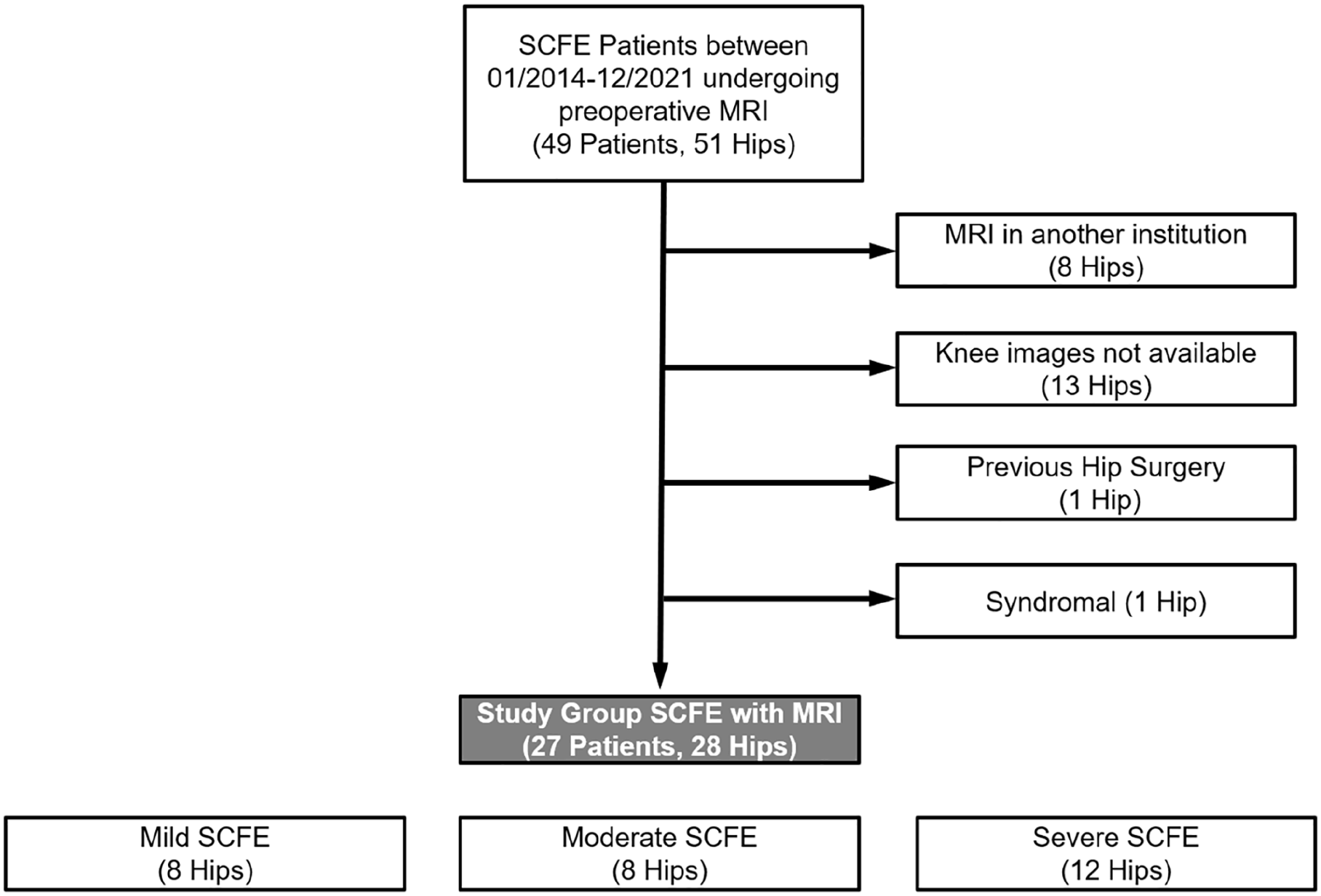
Flowchart of SCFE patients who underwent preoperative hip MRI. On the right, exclusion of patients without knee images or MRI in another institution or previous hip surgery or syndromal disease is listed.
The mean age at operation was 13 ± 2 (range, 10–16) years and 17 patients (18 hips (64%)) were male (Table 1). Six patients (six hips (21%)) showed an unstable hip according to Loder. 21 A moderate slip angle according to Southwick 22 ranging from 30° to 60° was present in 8 hips (29%, Table 1). Eight hips (29%) presented with a mild slip angle of less than 30° and 12 hips (43%) with a severe angle exceeding 60° (Figure 1). Half of SCFE patients had chronic slips (14 hips, 50%, Table 1).
Demographic and clinical data of the patient series are shown.
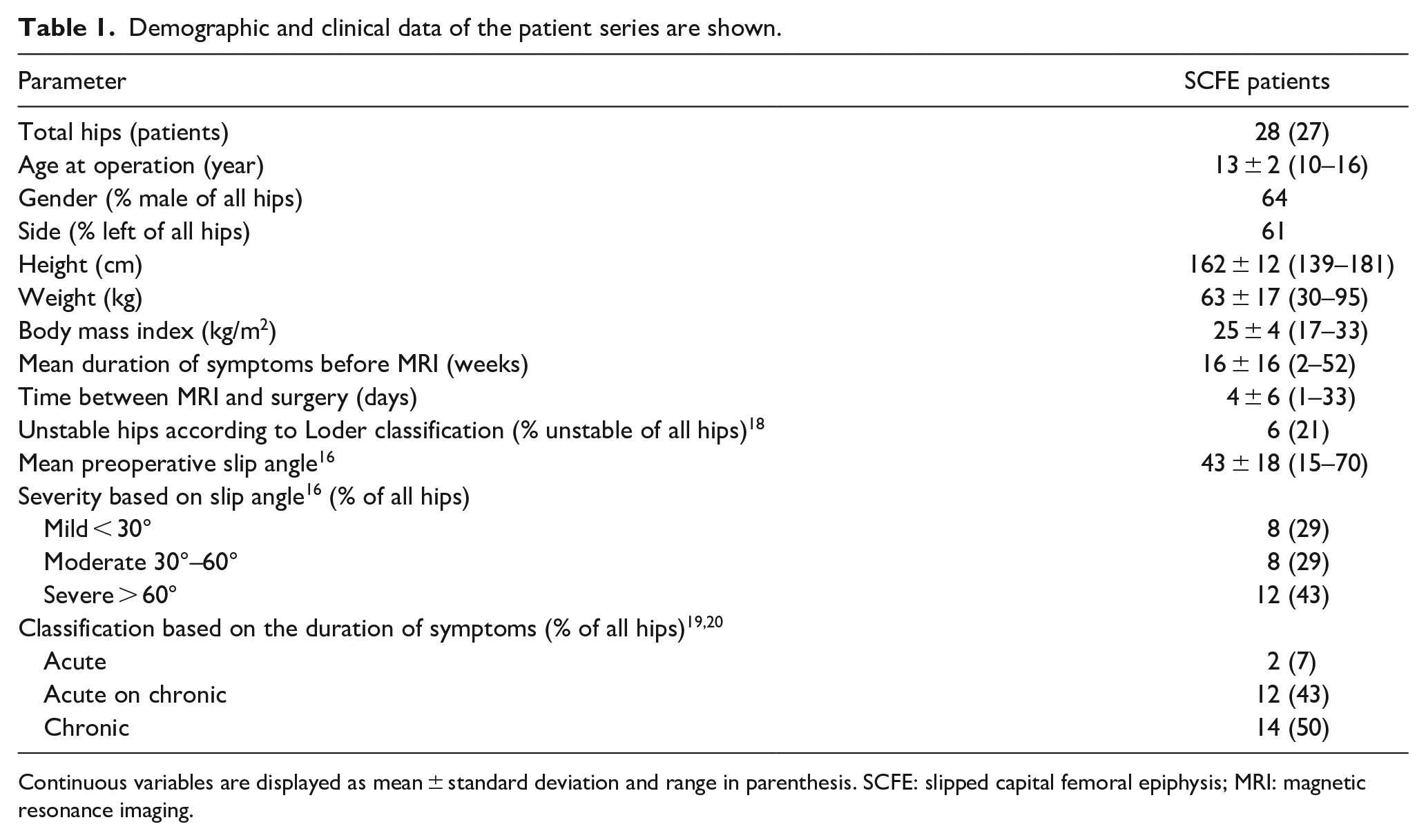
Continuous variables are displayed as mean ± standard deviation and range in parenthesis. SCFE: slipped capital femoral epiphysis; MRI: magnetic resonance imaging.
Imaging technique and image analysis
Preoperative hip MRI was performed on 3-Tesla or 1.5-Tesla scanner (Siemens Medical Solutions, Erlangen, Germany). Mainly, large flexible surface coils were used. Multiplanar T1-weighted images in coronal orientation and proton density (PD)-weighted images in sagittal, axial, and radial orientations were acquired. In addition, water-only images of a bilateral high-resolution 3-dimensional (3D) T1 VIBE (volume interpolated breath-hold examination) Dixon sequence of the pelvis (Figure 1) and of the knee were acquired. The water-only Dixon-based images of pelvis and knee were used for FV measurement. The field of view (FOV) of the bilateral 3D sequence included the complete pelvis and proximal femur to the level below the lesser trochanter (Figure 1(e)). The FOV of the bilateral distal femur covered the knee joint entirely. These images were acquired without contrast agent. The 3D T1 VIBE Dixon sequence included the entire pelvis with the following parameters for 3 Tesla: TR/TE1/TE2, 3.94/1.27/2.5 ms, flip angle 9°, slice thickness of 1 mm, FOV of 312 × 400 mm, a matrix size of 175 × 320 mm, anisotropic voxel size of 1.2 × 1.2 × 1 mm for 192 slices. A second 3D T1 VIBE Dixon (same parameters) for the bilateral knee was acquired. Acquisition time for 3D T1 VIBE Dixon sequence was 40 seconds for 3 Tesla. Additional sequences for evaluation of viability of the femoral epiphysis were added for some patients if needed. The time between clinical symptoms and MRI as well as the time between MRI and surgery were noted.
Femoral version
Two observers with 5 years of experience in musculoskeletal imaging performed measurements of FV. The two observers had good inter-rater agreement for reproducibility and reliability of FV measurement (intraclass correlation coefficient (ICC) ranging from 0.85 to 0.92). The same two observers measured FV for a previous study and a good agreement between the two observers was reported. 23 All measurements were performed on axial images without reformatting. The method described by Murphy et al. 24 was used for measurement of FV on the SCFE side and on the contralateral side. No summation images were used. This method defined the most proximal reference on the femoral head’s center. 24 The Murphy method uses the so-called centroid as a second proximal landmark; this is located at the center of the femoral shaft 24 superior to the lesser trochanter at the base of the femoral neck (Figure 2).
To measure femoral neck version, first the midpoint of the femoral neck axis is identified. The midpoint is identified on the image where the ventral and dorsal cortices can be seen parallel. This was the proximal reference axis. 5 One single image was used for measurement of the femoral neck version on the proximal femur. Distal femoral condyles were used for calculation of femoral neck version. Absolute femoral neck retroversion was defined as femoral neck version < 0°.
A preoperative anteroposterior (AP) pelvis radiograph was performed in addition to cross-table lateral or Lauenstein view for radiographic evaluation. Severity of SCFE was quantified using the slip angle. 25 The Klein line was used for diagnosis of SCFE. 26
Twenty SCFE patients presented with moderate or severe slips and underwent open hip surgery (most often the modified Dunn procedure 25 ). Mild slip patients underwent in situ pinning. Surgical procedures were noted using medical chart review.
Statistical analysis
A post hoc power analysis was performed using mean FV of SCFE patients and the contralateral side. This resulted in power of 90% (α level of 0.05) and a sample size of 21 hips per group. Post hoc power analysis was performed with clincalc.com. The Kolmogorov–Smirnov test was used to test for normal distribution of the continuous parameters. Because most parameters were not normally distributed, only nonparametric tests were used. The Wilcoxon test was used for pairwise comparison for continuous parameters. Binominal data were compared using the chi-square or Fisher’s exact tests.
Results
Mean FV of SCFE patients (–1 ± 15° vs 15 ± 14°, Table 2) was significantly (p < 0.001) decreased compared to contralateral side. The range of FV angles of SCFE patients was significantly (p < 0.001) wider from –42° to 35° (range of 77°) compared to contralateral side (–5° to 44°, range of 49°, Table 2).
Parameters of FV and femoral neck version are shown for two groups.
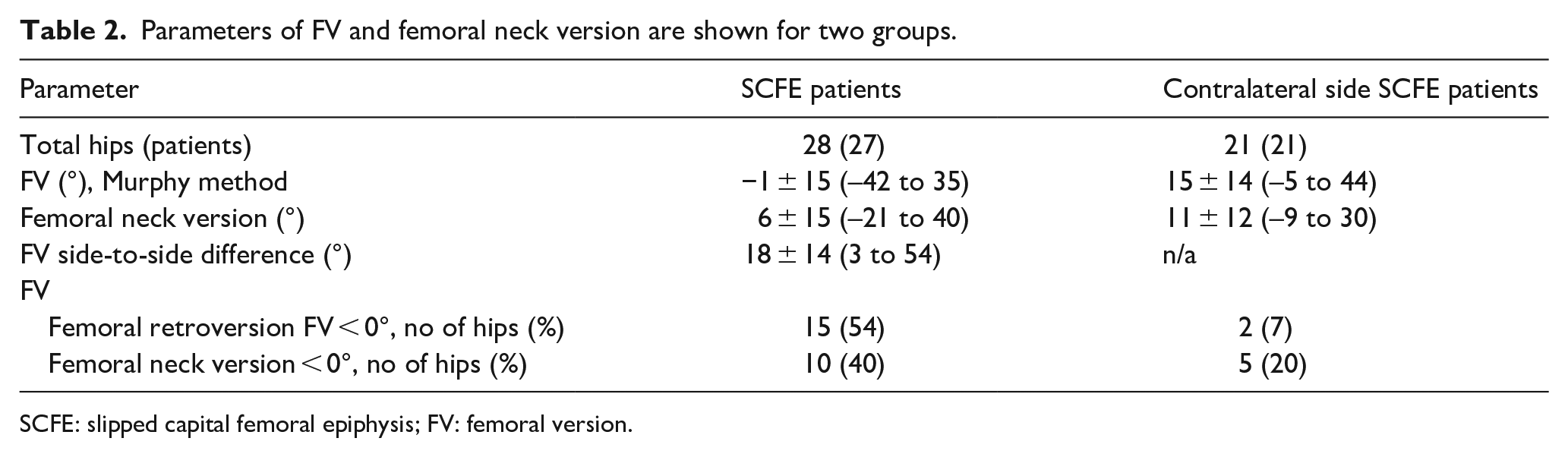
SCFE: slipped capital femoral epiphysis; FV: femoral version.
FV was lower for patients with severe SCFE (−5° ± 17°, Table 3) compared to mild (2° ± 11°) and moderate SCFE (1° ± 16°), but not significantly different.
Parameters of FV and femoral neck version are shown for mild, moderate, and severe SCFE patients.
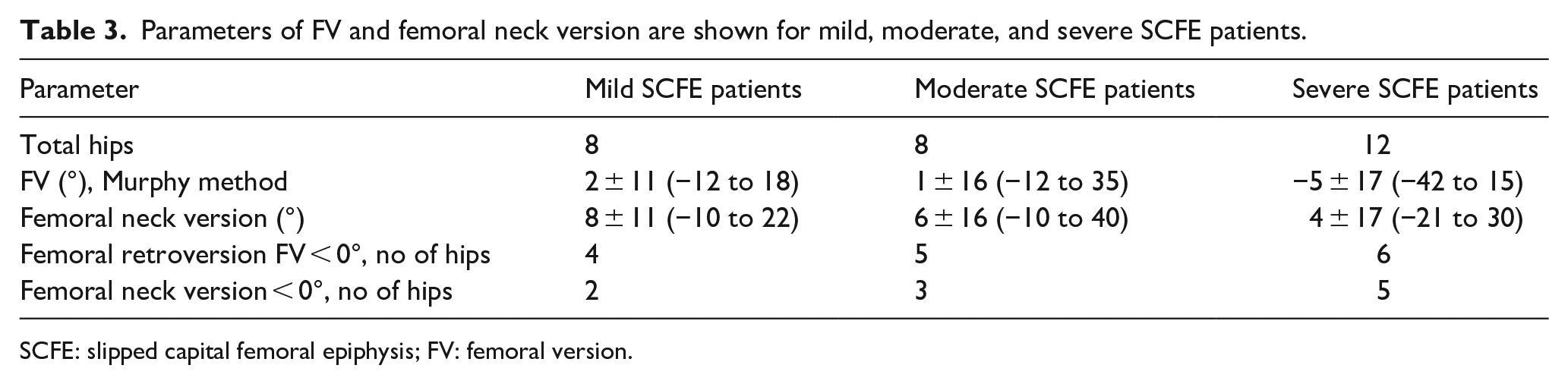
SCFE: slipped capital femoral epiphysis; FV: femoral version.
Mean FV for male SCFE patients and for female SCFE patients was 3° ± 13° and −8° ± 16°, respectively. Mean FV for acute on chronic SCFE patients and for chronic SCFE patients was 0.2° ± 16° and −2.4° ± 15°, respectively. The two patients with acute SCFE had a mean FV of −0.3° ± 11°. Mean FV for unstable SCFE patients and for stable SCFE patients was −2.2° ± 14° and −0.9° ± 16°, respectively.
Mean femoral neck version of SCFE patients (6° ± 15°) was lower compared to contralateral side (11° ± 12°, Table 2). Mean femoral neck version of patients with severe SCFE was slightly decreased (4° ± 17°) compared to mild (8° ± 11°) and moderate SCFE (6 ± 16°, Table 3), but not significantly different (Table 3). Mean femoral neck version for male and for female patients was 9° ± 14° and –1 °± 14°, respectively. Mean femoral neck version for acute on chronic SCFE patients and for chronic SCFE patients was 8° ± 18° and 5° ± 12°. The two patients with acute SCFE had a mean femoral neck version of 0° ± 17°. Mean femoral neck version for unstable SCFE patients and for stable SCFE patients was 10° ± 15° and 5° ± 15°, respectively.
Frequency of SCFE patients (54%) with absolute femoral retroversion (FV < 0°) was high. Six of them had severe slips (21%) and four had mild slips (14%, Table 3). Seven SCFE patients (25%) had normal FV (between 10° and 25°). Ten SCFE patients (40%) had absolute femoral neck retroversion (femoral neck version < 0°), five had severe slips (18%), and two had mild slips (7%, Table 3). Of the 10 female SCFE patients, 6 had absolute femoral retroversion (FV < 0°). Of the 18 male SCFE patients, 9 (50%) had absolute femoral retroversion (FV < 0°). Of the 14 chronic SCFE patients, 8 (57%) had absolute femoral retroversion (FV < 0°). Of the 12 acute on chronic SCFE patients, 6 (50%) had absolute femoral retroversion (FV < 0°).
Side-to-side difference of FV (18° ± 14°) was higher compared to femoral neck version (9° ± 8°).
Discussion
Femoral retroversion was reported in SCFE patients, but quantification of FV using CT or MRI is rare. Individual preoperative FV measurement on MRI was performed in this study for patients with SCFE. Most importantly, 15 SCFE patients (54%) had absolute femoral retroversion (FV < 0°), six had severe slips, and four had mild slips. These patients have combined deformities (SCFE and femoral retroversion). Significantly, lower mean FV was found for SCFE patients compared to contralateral side (Table 2). Furthermore, the FV angles had a large variability, ranging from –42° to 35° (range of 77°, Table 2). In addition, slightly higher values for FV and femoral neck version were found for male patients compared to female patients. It seems that SCFE was not always associated with femoral retroversion and seven SCFE patients (25%) had normal FV. Femoral neck version was slightly lower in SCFE patients compared to contralateral side. And a slightly decreased femoral neck version of severe SCFE was found compared to mild and moderate SCFE (Table 3). No general conclusion is possible due to the inter-individual variation of FV angles.
Comparing the results for FV, similar results compared to a previous study 5 of 1986 were found that reported a mean FV of –0.7° ± 7.4° for SCFE patients. This is slightly higher compared to a more recent study 6 reporting FV of –4° ± 16° (range −39 to 61) and a high prevalence of femoral retroversion using CT scans (FV measured with Murphy method) for SCFE patients. The mentioned study 6 included patients with previous in situ pinning and this was not the case in this study. The study had a comparable prevalence of severe slips (51%) compared to this study (50%, Table 1). Regarding FV of the asymptomatic side, in this study we found slightly lower values compared to a recent large study 27 of adult patients with hip diseases (mean FV of 19°). Comparing the prevalence of femoral retroversion, a recent study 6 found a higher prevalence of 60% using the Murphy method. A large prevalence study evaluating adult patients with hip diseases found a lower prevalence of femoral retroversion. 27 Interestingly, four SCFE patients with absolute femoral retroversion (FV < 0°) had mild slips. If these patients are treated with in situ pinning (also called in situ fixation), they could be at risk for residual deformity and reduced internal rotation of the hip and anterior extra-articular subspine hip impingement 17 because this treatment usually does not alter FV.
Other described methods for FV measurement use different definitions of the proximal reference line. 23 The posterior femoral condyles were used to define the distal reference axis. Considerable differences between measurement methods for FV exist, for example, between the Murphy method and the Lee method. 23 The most pronounced difference of FV of 17° was reported between the Murphy method and the Lee method using CT scans. We have chosen the Murphy method because of the high reliability of the measurement using this method and because it reflects true anatomical FV. In a review comparing imaging modalities for FV, measurement of FV with CT was found to be more accurate than on conventional radiographs. 15 In addition, biplane radiography demonstrated greater inter- and intrarater variability than CT imaging for repeated measurements of FV. 15 In the meantime, MRI and CT can be used interchangeably for FV measurement. 28 Biplanar radiograph may underestimate the extent of the epiphyseal displacement, thereby potentially altering the management between in situ pinning and open hip surgery.
The definition of absolute femoral retroversion was FV < 0° in agreement with previous investigations.6,27 Normal FV was defined in accordance with previous studies13,27 (between 10° and 25°). Other studies investigating normal FV19,29 reported values between 8° and 18° and the measurement methods were variable. There is a considerable variability of studies that define normal FV and for categorization of femoral retroversion. Different definitions for femoral retroversion were <25°, 30 <10°, 13 <5°, 31 and <0°. 19 The Murphy method was previously used for measurement of FV for FAI patients, 27 for patients with post-Perthes deformities, 18 and for patients with SCFE and post-SCFE deformities. 6
A previous investigation reported a good intraobserver reliability (ICC of 0.96–0.99) and interobserver reliability (ICC of 0.98) for measurement of FV using the Murphy method 6 for patients with SCFE. Previous studies reported no clinically relevant difference between MRI and CT for FV measurements for pediatric patients with hip diseases 28 as well as for adult patients. 20 Agreement between MR-based and CT-based measurements of FV was good (bias 1.9°) for pediatric patients with hip diseases. 28
To the best of the authors’ knowledge, no study was found that reported normal values for MRI or CT-based quantification of femoral neck version in pediatric patients. Interestingly, Decker et al. 32 found a mean FV of 18° ± 10° of 211 hips with a contralateral femoral fracture (age 0–92 years). They reported a mean FV of 18° ± 9° for female patients and 19° ± 11° for male patients between 2 and 20 years of age. 32 The reported values are comparable to the mean FV of the contralateral hips of the current study (15° ± 14°). However, a previous study 7 reported a mean femoral neck version of 9.3° for symptomatic SCFE using CT scans. This is slightly higher compared to the results of patients with SCFE of the current study (mean femoral neck version of 6° ± 15°, Table 2).
Comparing the results for side-to-side difference, we found differing results of the current study compared to a previous study that reported no difference between affected and unaffected side. 7 Another study by Gelberman et al. 5 reported a side-to-side difference of the femoral neck version in 13 patients with acute SCFE (−0.7°± 7.4°) compared with the uninvolved side (6.3°± 8.2°). A more recent study found a side-to-side difference of 9° comparing affected and unaffected side. 6 This is consistent with the results found in the current study for femoral neck version (9° ± 8°).
One of the strengths of this study is that all SCFE patients had the same standardized MRI protocol including knee images. There was a short time between surgery and MRI (mean 4 days, Table 1) and MRI did not delay surgical treatment. Therefore, we do not assume that any remodeling is possible in this short time. In addition, previous studies reported so-called remodeling of the proximal femur after fixation of the epiphysis after 17 months.33,34 Another strength is that no patient had previous hip operations (e.g. no previous attempts of reduction with the Parsch method 35 or in situ pinning) that could influence FV measurement. This is different compared to previous studies. One of the previous studies reported that a measurement of the femoral neck version poses a risk of underestimation because of the displaced femoral epiphysis. In the current study, FV measurement in SCFE patients uses the center of the proximal femoral epiphysis (the femoral rotation’s center). This is important for patients treated with in situ pinning because FV is usually not altered with this treatment. Absolute femoral retroversion may influence internal rotation of the hip, external rotation gait,16,36 location of anterior hip impingement, 17 and probably long-term outcome and progression to hip osteoarthritis.13,14 Knowledge about FV and femoral retroversion may influence further follow-up examinations or can help to explain reduced hip internal rotation and theoretically could theoretically help to estimate if a SCFE patient is at risk for future anterior hip impingement.
This study has limitations. Because all patients were evaluated in a European university hospital, a certain selection bias is possible. The decision to perform preoperative MRI was to assess slip severity, to measure the slip angle on MRI, and to search for intra-articular damage (labrum and cartilage), and evolved over time due to the retrospective design of the study. This case series is not a completely consecutive series and probably patients with acute or unstable SCFE are underrepresented. It was challenging to perform preoperative MRI in acute or unstable SCFE due to the acuteness of the diseases. The time frame to perform an MRI is too short for these subgroups of SCFE patients due to limited availability of MRI scanners. This could be the reason for the high proportion of chronic SCFE (50%, Table 1). This decision was also dependent on patients’ factors and the availability of MRI. The higher costs of MRI compared to radiographs limit worldwide application. Previous studies reported similar FV measurements using CT and MRI28,20; therefore, the choice of modality should not affect the results. In addition, although we compared SCFE patients with the asymptomatic contralateral hips, it is unclear if these hips are normal. It is well known that the contralateral hip joint can develop SCFE as well.37,38 Future studies could compare FV of SCFE patients to age-matched asymptomatic volunteers without hip pain. The number of patients with mild or moderate slip deformity (Table 1) in this study are probably too small to draw general conclusions. Also, the number of patients with acute or unstable SCFE do not allow to formulate specific recommendations. Unfortunately, the FV before SCFE diagnosis is unknown; therefore, it is unclear if femoral retroversion was present before SCFE or vice versa. Osteonecrosis (avascular necrosis) of the femoral head is a known complication of SCFE, but was not analyzed in this study. Although there is a high prevalence in SCFE patients, we did not analyze the residual deformities of the proximal femur, 37 such as cam-type deformities. 37 Secondary impingement deformities after SCFE can result in early joint degeneration, loss of hip function, and premature osteoarthritis.1,39 This could be evaluated in further studies.
Conclusion
Although SCFE patients showed asymmetrically lower FV compared to contralateral side, there was a wide range of measured FV angles. Due to the wide variation of FV angles, patient-specific analysis of FV seems important. Absolute femoral retroversion was prevalent in half of SCFE patients, in half of severe SCFE patients, and in half of mild SCFE patients on preoperative MRI. This has theoretical implications for anterior hip impingement. This is important for planning of hip preservation surgery, e.g. treatment with in situ pinning or femoral osteotomy (proximal femoral derotation osteotomy) or the modified Dunn procedure.
Footnotes
Author contributions
All authors listed above have fulfilled the authorship qualification and met the following criteria for authorship:
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and
Drafting the work or revising it critically for important intellectual content; and
Final approval of the version to be published; and
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The local ethical committee approved this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T. L. has received funding from the Swiss National Science Foundation (Grant number P2BEP3_195241). Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.