
Abstract
Objective:
To analyze the clinical characteristics, X-ray and magnetic resonance imaging manifestations, and treatment efficacy of idiopathic chondrolysis of the hip.
Methods:
Ten patients with idiopathic chondrolysis of the hip treated at our hospital from September 2013 to April 2022 were collected, and their clinical features, X-ray and magnetic resonance imaging manifestations, and treatment outcomes were analyzed.
Results:
Their main clinical features included single hip pain, claudication gait, and pelvic tilt, without specific clinical symptoms and signs. Laboratory tests such as blood analysis, erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, autoimmune test, coagulation function, interferon release test for tuberculosis infection, and tuberculosis antibody test were normal. In the late stage, the imaging shows degeneration or ankylosis of the joint. The disease progresses rapidly, and joint degeneration can occur in adolescence without effective treatment. Herein, seven patients were treated with recombinant human tumor necrosis factor receptor–antibody type II fusion protein. Among them, four (according to Camarnat magnetic resonance imaging classification, three were Stage I and one was Stage II) showed improved symptoms and function, while two (Stage III) had progressed. One patient (Stage I) who received recombinant human tumor necrosis factor receptor had no significant relief of symptoms, for whom anterior capsular release surgery significantly improved the hip joint motion. Of the four patients who underwent hip release surgery, three showed progression.
Conclusion:
Idiopathic chondrolysis of the hip has no specific clinical and laboratory tests and a high misdiagnosis rate. Thus, early magnetic resonance imaging is a critical reference for diagnosis. We recommend that patients with magnetic resonance imaging Stage II or earlier be actively treated with recombinant human tumor necrosis factor receptor and start treatment as early as possible. In the third stage, the treatment effect is mediocre, and the narrowed hip space is difficult to change.
Idiopathic chondrolysis of the hip (ICH) is a rare and unexplained osteoarthritic disease first described by Jones 1 in 1971. It mainly occurs in adolescents around puberty, but the etiology is yet unknown. The disease progresses rapidly, and without effective treatment, it can lead to extensive and rapid dissolution of articular cartilage of the hip. In some cases, joint stiffness occurs before adulthood. The natural course of ICH is divided into two stages: an acute phase lasting approximately 18 months (characterized by active inflammation within the synovial lumen of the hip, resulting in hip pain and limited range of motion due to progressive destruction of the articular cartilage on both sides of the joint) and a chronic inflammatory phase lasting 3–5 years. 2 Segaren et al. 3 described three possible clinical outcomes: complete disappearance of symptoms, painless but stiff hip, and pain with hip ankylosis. The latter two are common occurrences. 4
All the patients in this study had unilateral onset. The age of onset was 8–13 years, and 9/10 cases in our hospital were females. The typical history is that of an adolescent or prepubertal child, with no history of fever or other joint pain, presenting pain in the groin, anterior thigh, or knee, accompanied by progressively increasing hip stiffness and a limp.
The lack of specific clinical manifestations and laboratory indices is a major reason for easy misdiagnosis. Therefore, some patients came to our hospital after several rounds of treatment at other hospitals; one of them had been ill for 3 years when he visited our hospital for treatment. The characteristic finding on physical examination is as follows: the pelvis is usually tilted to the affected side, and the limbs are unequal in appearance, often with Thomas sign and tightness of the hip adductors. Unlike the common childhood bone diseases, such as juvenile idiopathic arthritis and infectious diseases of the bone and joint, laboratory tests, such as inflammatory markers, blood analysis, rheumatic markers, and tuberculosis markers, are not abnormal.
The awareness of the natural history of ICH and the practice of conservative treatment strategies have led people to abandon the idea of early surgery for ICH.5–7 Reportedly, non-steroidal anti-inflammatory drugs (NSAIDs) combined with aggressive physical therapy and protective weight-bearing can improve symptoms in 50%–60% of acute cases.8,9 Traction therapy has also been attempted in several studies.4,8,10,11 Among the current group, some patients treated with NSAIDs, anti-rheumatic drugs, and anti-osteoporosis therapy showed less than satisfactory outcomes.
The histopathological features of the synovium and cartilage obtained intraoperatively from patients with ICH were similar to that of other rheumatic diseases, showing synovial inflammatory plasma cell infiltration with immunoglobulin deposition12,13 and cell fragmentation, detachment, thinning, and necrosis in the superficial areas of cartilage.2,14,15 Previous studies reported that HLA-B27-positive patients with this disease corroborate the possible autoimmune tendency of this group. 16 This evidence suggested that the development of the disease may be the result of autoimmune-mediated cartilage destruction in patients. 3
Recombinant human tumor necrosis factor (rhTNFR) is a tumor necrosis factor (TNF) antagonist that reduces the activity of TNF-α by competitively binding to it in the blood and blocking its binding to TNF receptors on the cell surface, which in turn blocks the release of inflammatory factors and controls the progression of inflammation during the treatment of joint inflammation.17–20 In our group, seven patients tried to use rhTNFR. Among them, four cases showed an obvious improvement of symptoms after 3 weeks of treatment with rhTNFR, and the continued follow-up showed that the joint gap widened and the signal of edema in the epiphysis and acetabulum diminished. One patient showed poor response to medication, but a significant improvement in symptoms after a gluteal muscle release. In the other two cases, the symptoms did not improve, and one of them already had obvious osteoarthritis at the time of consultation.
Clinical data
Source of data
Laboratory and imaging data of 10 patients with ICH, including one male and nine females, the age of onset was 8–13 years, admitted to our hospital from September 2013 to April 2022 were collected. The general medical history of the patients is summarized in Table 1. The following conditions were considered consistent with the diagnosis of ICH: 21 (a) Unilateral hip onset in adolescents, no inflammatory symptoms in small joints and attachment points, no history of fever before onset, no history of hip fracture, and no family history of the rheumatic disease; (b) Laboratory tests, such as blood analysis, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor, autoimmune test, coagulation function, interferon release test for tuberculosis infection, and tuberculosis antibody test, did not show any significant abnormalities; (c) Imaging manifestations. A concentric narrowing of the hip space on the affected side to <3 mm was observed on X-ray, often with peripheral osteoporosis. Magnetic resonance imaging (MRI) suggested thinning of the articular cartilage; (d) Adolescent idiopathic arthritis, traumatic arthritis, juvenile osteochondrosis of the femoral head, hip tuberculosis, and septic hip arthritis were excluded.
The course and previous diagnosis and treatment of 10 patients.
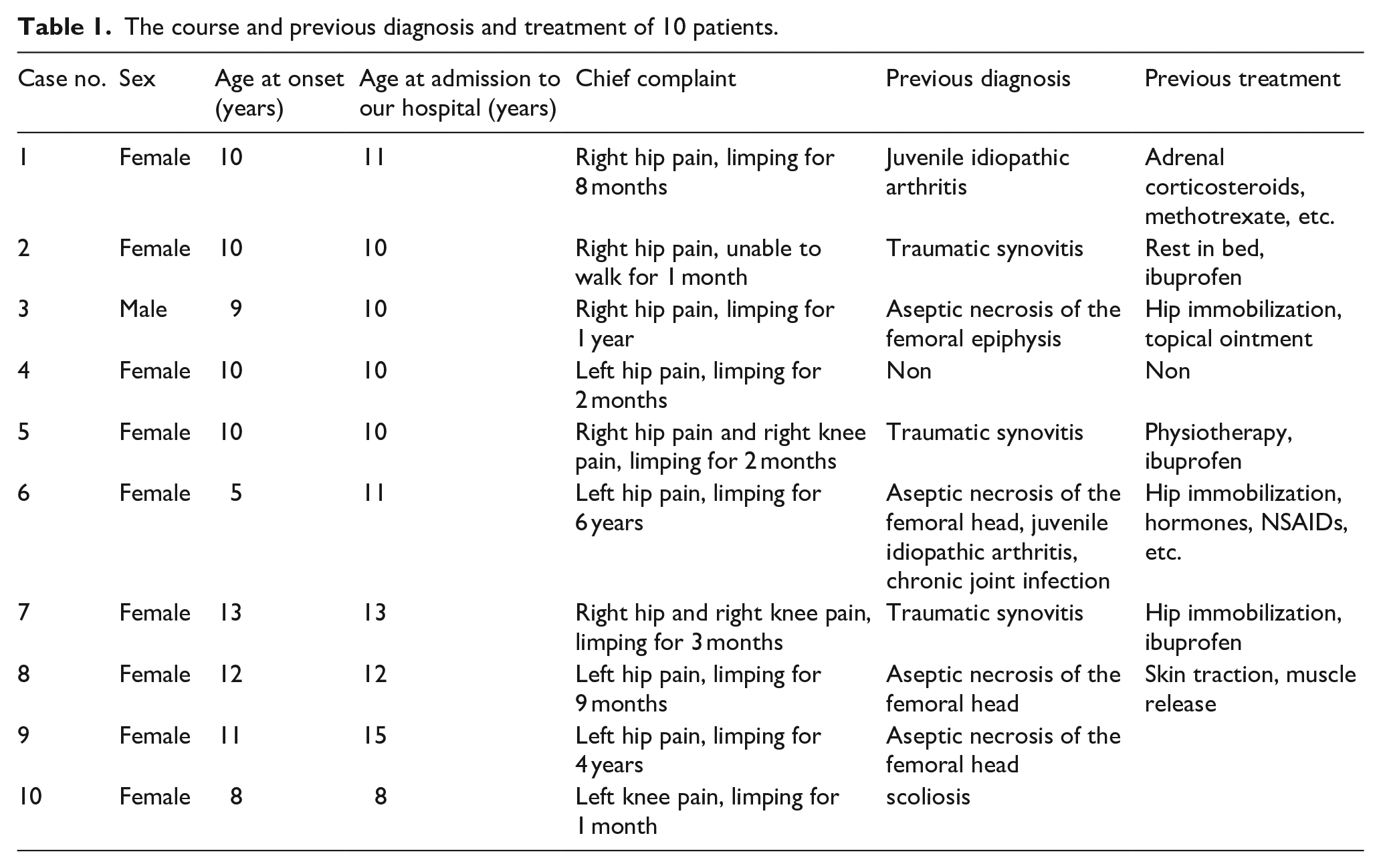
Course of disease, previous misdiagnosis, and treatment of patients (Table 1)
The duration of symptoms prior to diagnosis of ICH ranged from 1 month to 4 years, and most of them had been misdiagnosed in other hospitals. Two cases had been misdiagnosed as juvenile idiopathic arthritis and were treated with salbutamol, steroids, and methotrexate without improvement; three cases had been misdiagnosed as aseptic necrosis of the femoral head and were treated with immobilization and traditional Chinese medicine without improvement in pain and dysfunction; one of them had undergone adductor longus release due to limited hip abduction; three cases were considered traumatic hip synovitis and were treated with non-weight-bearing and ibuprofen symptomatically. Three cases were synovitis of the hip joint and were referred to our hospital because previous treatments were ineffective; two cases were first treated in our hospital.
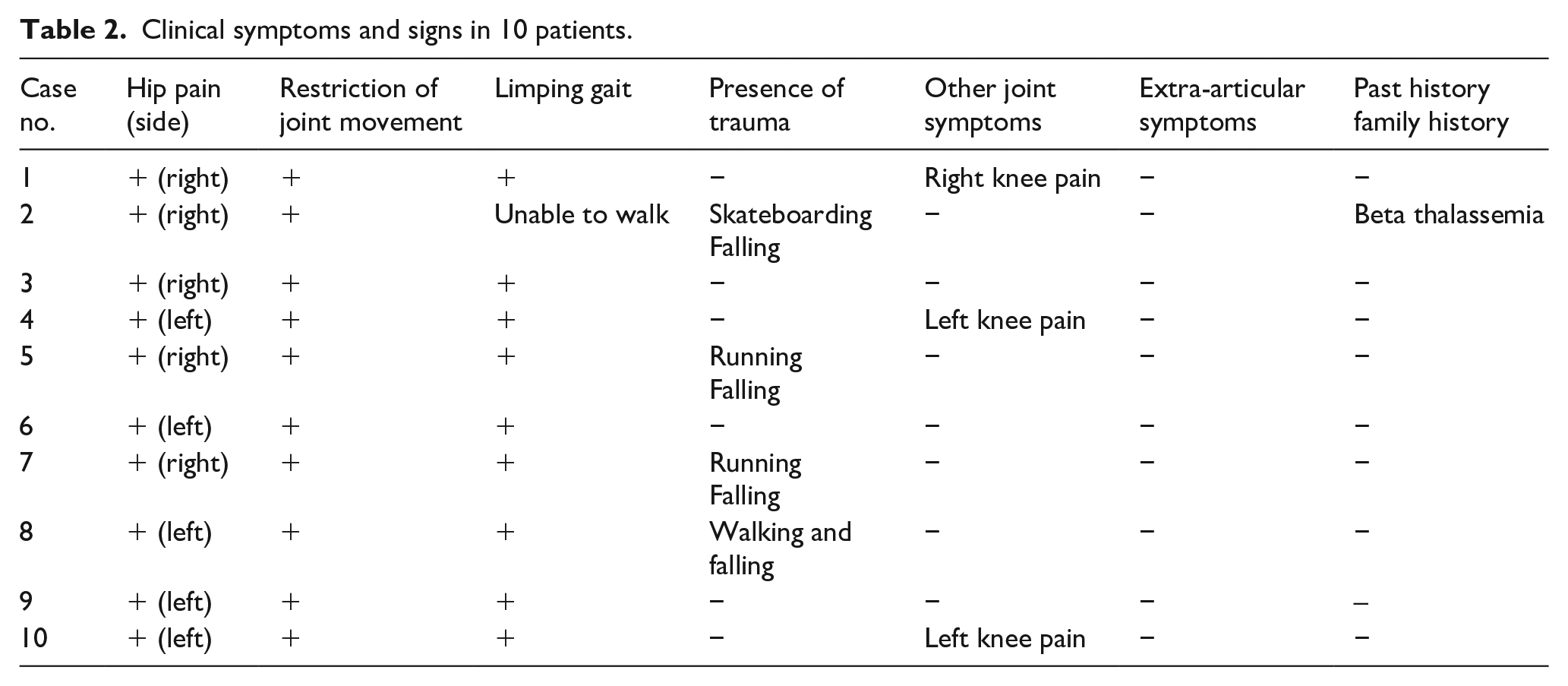
Clinical symptoms and signs of patients (Table 2)
All 10 patients had unilateral hip pain and progressive limping as the chief complaints, with varying degrees of pain. In mild cases, oral ibuprofen was effective for analgesia, while in severe cases, an intravenous morphine drip was required at night to relieve the pain and fall asleep. Among them, three cases were accompanied by ipsilateral knee pain. The physical examination showed varying degrees of hip stiffness, limited movement in all directions, especially internal rotation of the hip, squatting obstruction, pelvic tilt to the affected side, and positive Allis sign and Thomas sign. Four patients had a history of trauma before the onset of the disease, while the rest had no obvious cause for the onset of the disease. Also, none of the patients had extra-articular symptoms or family history of autoimmune diseases.
Clinical symptoms and signs in 10 patients.
Laboratory and imaging examinations
All patients underwent blood analysis, including ESR, CRP, rheumatoid factor, autoimmune test, coagulation function, interferon release test for tuberculosis infection, and tuberculosis antibody test. The remaining test results were within normal limits in all patients except for Case 3 with mildly elevated procalcitonin (0.06 ng/m), Case 4 with mildly decreased leukocytes (3.70E + 9/L), and Case 9 with mildly elevated complement 4 (0.113 g/L).
Hip plain radiographs and computed tomography (CT) scan in all 10 cases showed concentric narrowing of the joint space, gross joint surface of the acetabulum and femoral head, and periarticular osteoporosis. 9/10 cases were accompanied by a pelvic tilt to the affected side. The degenerative changes in the hip joint were observed in three cases. As the specific characteristic of MRI, the thinning of articular cartilage was seen in all 10 cases, and lamellar long T1 and long T2 edema areas were detected in the middle and lateral epiphyses of the femoral head in nine patients, of which six were accompanied by acetabular bone edema in the corresponding area, mild synovitis and mild to moderate joint effusion were seen in eight patients, and some patients had periarticular muscle atrophy.
Treatment and follow-ups
All 10 cases were followed up for 6–96 (mean 48) months. Cases 1, 2, 3, 4, 5, 6, and 7 were treated with rhTNFR (Product name: Yi SaiPu, Shanghai Zhongxin Guojian Pharmaceutical Co., Ltd). The medication was administered by subcutaneous injection at 12.5 mg twice a week. Among these cases, the symptoms were relieved gradually in Cases 1, 2, 6, and 7, with significant improvements in the range of joint motion function gait, articular cartilage repair, and joint space widening. Case 3 was transferred to the hospital after treatment with no improvement in symptoms and function. Case 4 had pain relief after rhTNFR treatment, but hip function was still poor and showed hip flexion contracture deformity; the anterior joint capsule release of the left hip was performed in October 2021, and flexion hip contracture improved after surgery. After failed physiotherapy and anti-inflammatory drugs, Cases 8, 9, and 10 were treated with an operation. Case 8 underwent anterior hip capsule resection, and femoral head decompression with drilling in February 2014 significantly narrowed the joint space, while the joint function was poor at 7 years of follow-up. Case 9 underwent partial hip capsule resection and arthroplasty in March 2014, the joint space was narrowed, and joint function was poor at the last follow-up. Case 10 underwent left hip arthrotomy with arthroplasty, inferior transposition of the greater trochanter in March 2016, with joint space narrowing, mild osteoarthritis of the hip, and poor hip function at 5 years of follow-up.
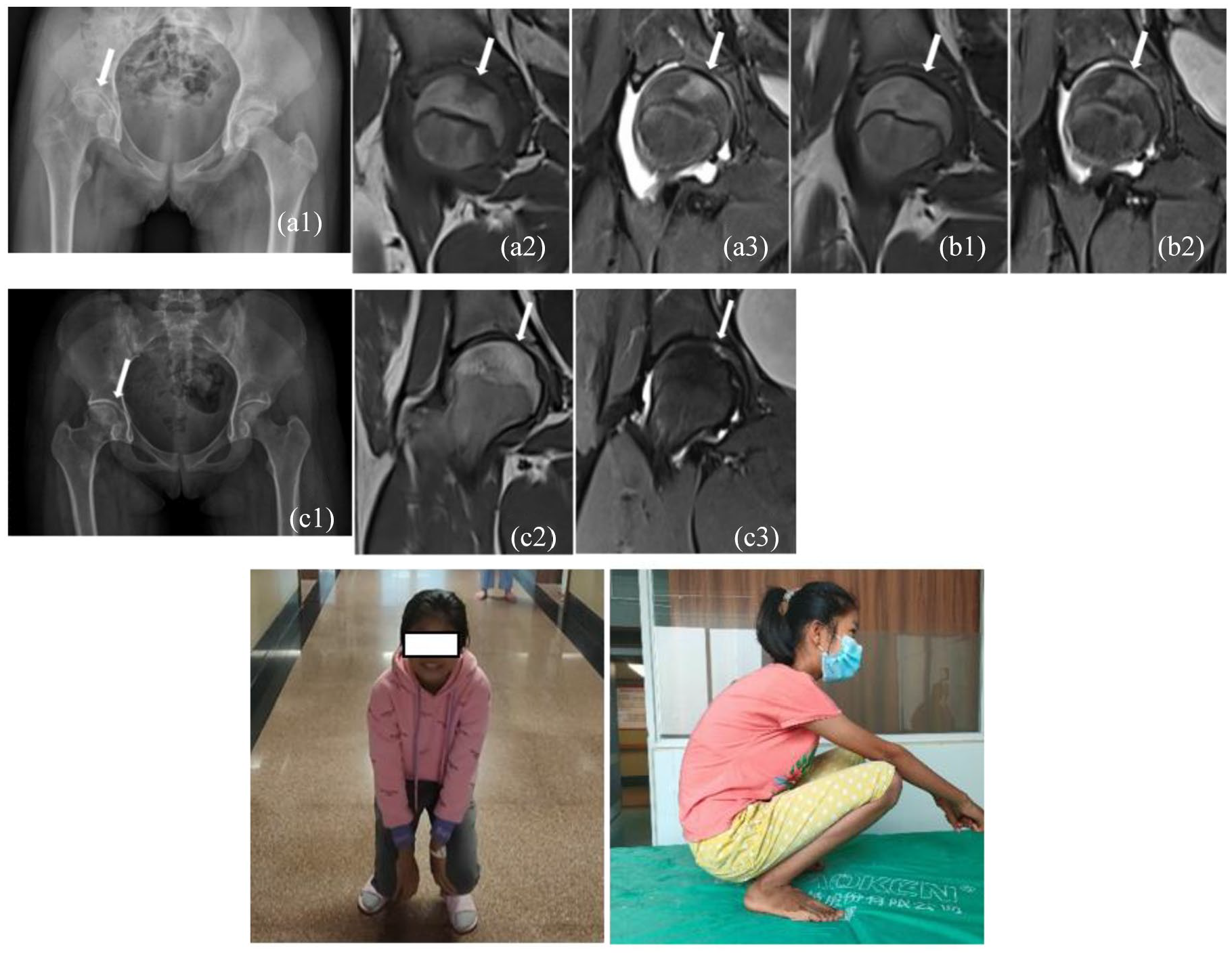
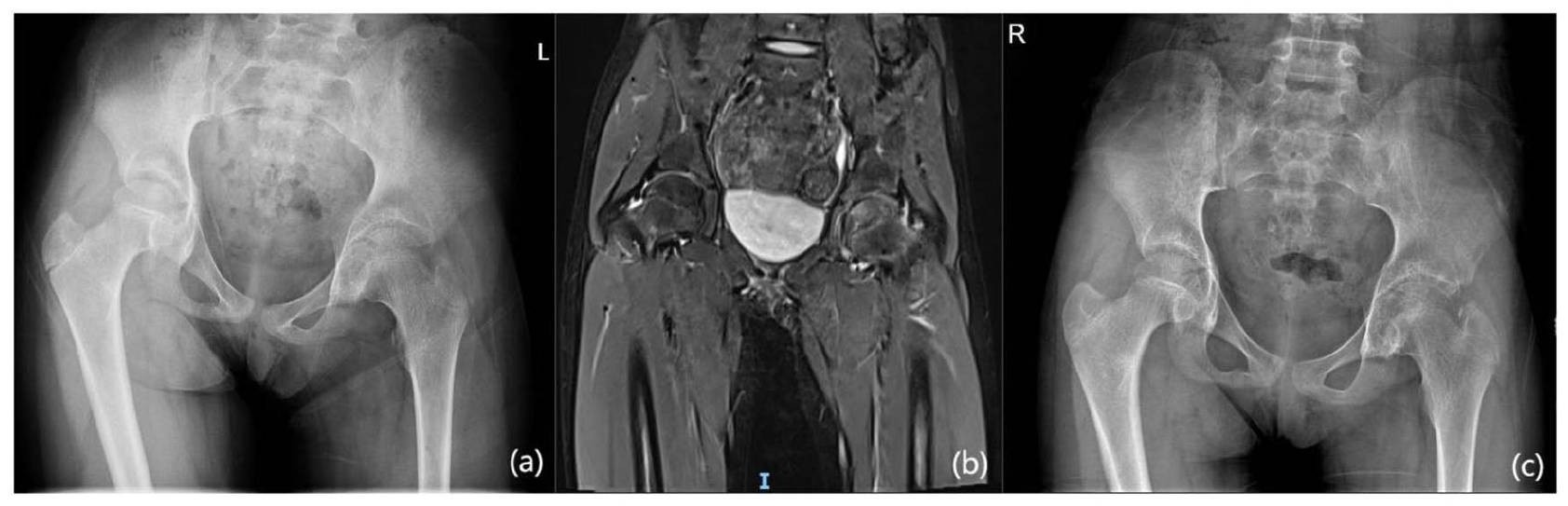
Two years after treatment, the hip flexion and squatting function improved significantly compared to that before treatment. (a1) Before treatment, the pelvis was right-tilted and the right joint space was uniformly narrowed on X-ray, with no obvious bone destruction. (a2/a3) Before treatment, a trapezoidal abnormal signal shadow was seen in the middle column of the right epiphysis, with high signal on T2WI and low signal on TIW1 and a small to moderate amount of effusion shadow in the right hip capsule. (b1/b2) Re-examination of MRI after rhTNFR treatment for 2 weeks showed a weakened trapezoidal signal. (c1) Three years after treatment, the pelvic tilt improved, the bilateral hip gaps were approximately the same, and no bone destruction was observed in either of the hips. (c2/c3) After 3 years, the MRI examination of the right hip showed that the subchondral edema of the femoral head had disappeared.
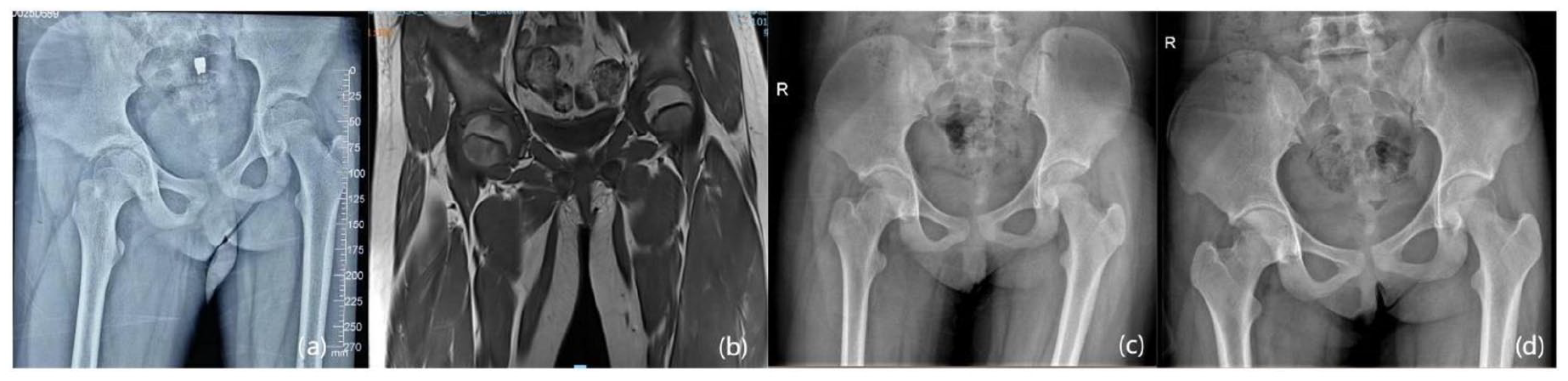
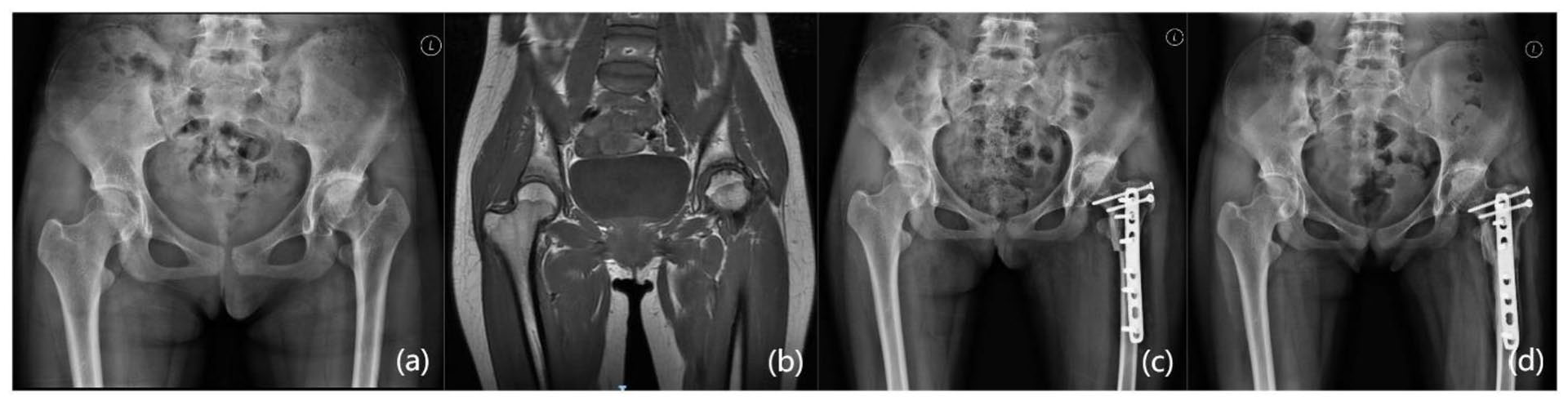
(a) Pre-treatment X-ray showed a narrowing of the right hip joint space. (b) The MRI show trapezoidal signal shadow of the right femoral head. (c) Two years follow-up after rhTNFR treatment. (d) Four years after treatment, the pelvic tilt improved, the bilateral hip gaps were approximately the same, and no bone destruction was observed in either of the hips.

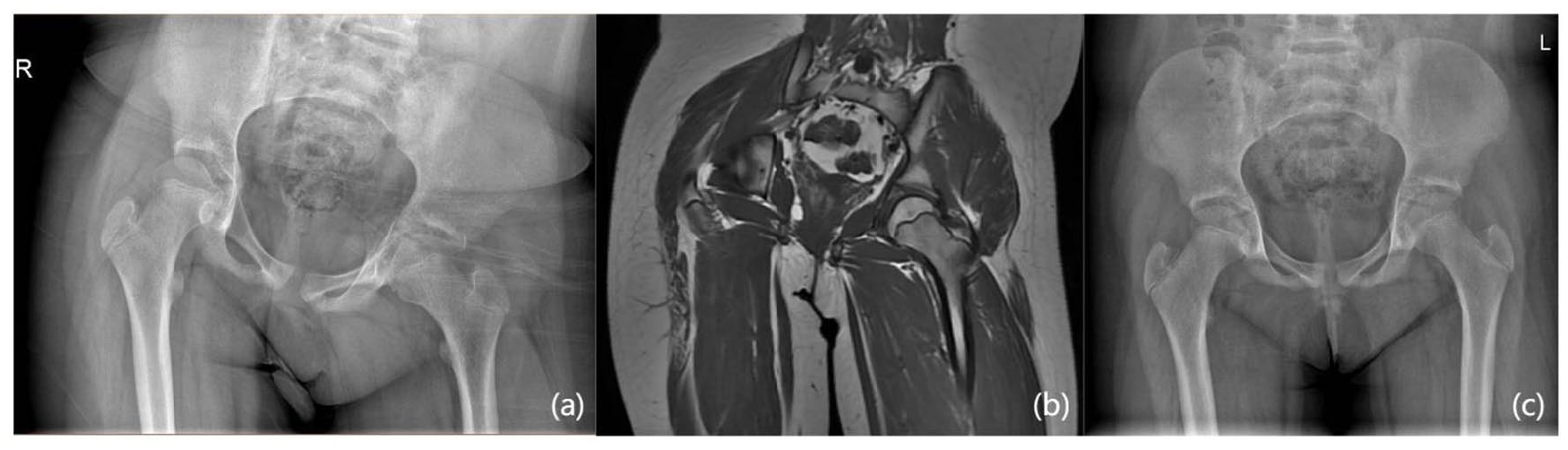
(a) There was marked arthritis of the hip with periacetabular sclerosis at presentation. (b) MRI showed a large area of high signal shadow in the right hip epiphysis and a large amount of fluid collection. (c) Showed no significant improvement after treatment.
(a) The joint space of the left hip was narrow at the time of the patient’s initial visit. (b) There was more hip joint effusion after treatment with rh TNFR, and the patient’s pain was not relieved. (c) Increased hip joint space after hip joint release.

(a) The patient visited our hospital for treatment for the first time in 2015. X-ray showed that the patient had hip arthritis, the joint space was significantly narrowed than the opposite side, the femoral head was deformed. (b) Recheck after 2 years. (c) After 3 years of follow-up, the joint space was much clearer than before, but the shape of the femoral head and acetabulum was not improved compared to that before treatment.

(a) The patient visited our hospital for treatment for the first time in 2015 after 3 years of pain in the left hip. X-ray showed that the patient had hip arthritis, the joint space was significantly narrowed than the opposite side, the femoral head was deformed, the greater trochanter was moved upward, the cartilage was damaged, the acetabular depression was obvious, and the pelvis was inclined. (b) Recheck after 2 years. (c) After 3 years of follow-up, the joint space was much clearer than before, but the shape of the femoral head and acetabulum was not improved compared to that before treatment.
(a) X-ray showed a narrowing of the left hip joint space. (b) The MRI show irregular signal shadow of the left femoral head. (c) After rh TNFR treatment, the bilateral hip joint space was basically the same.
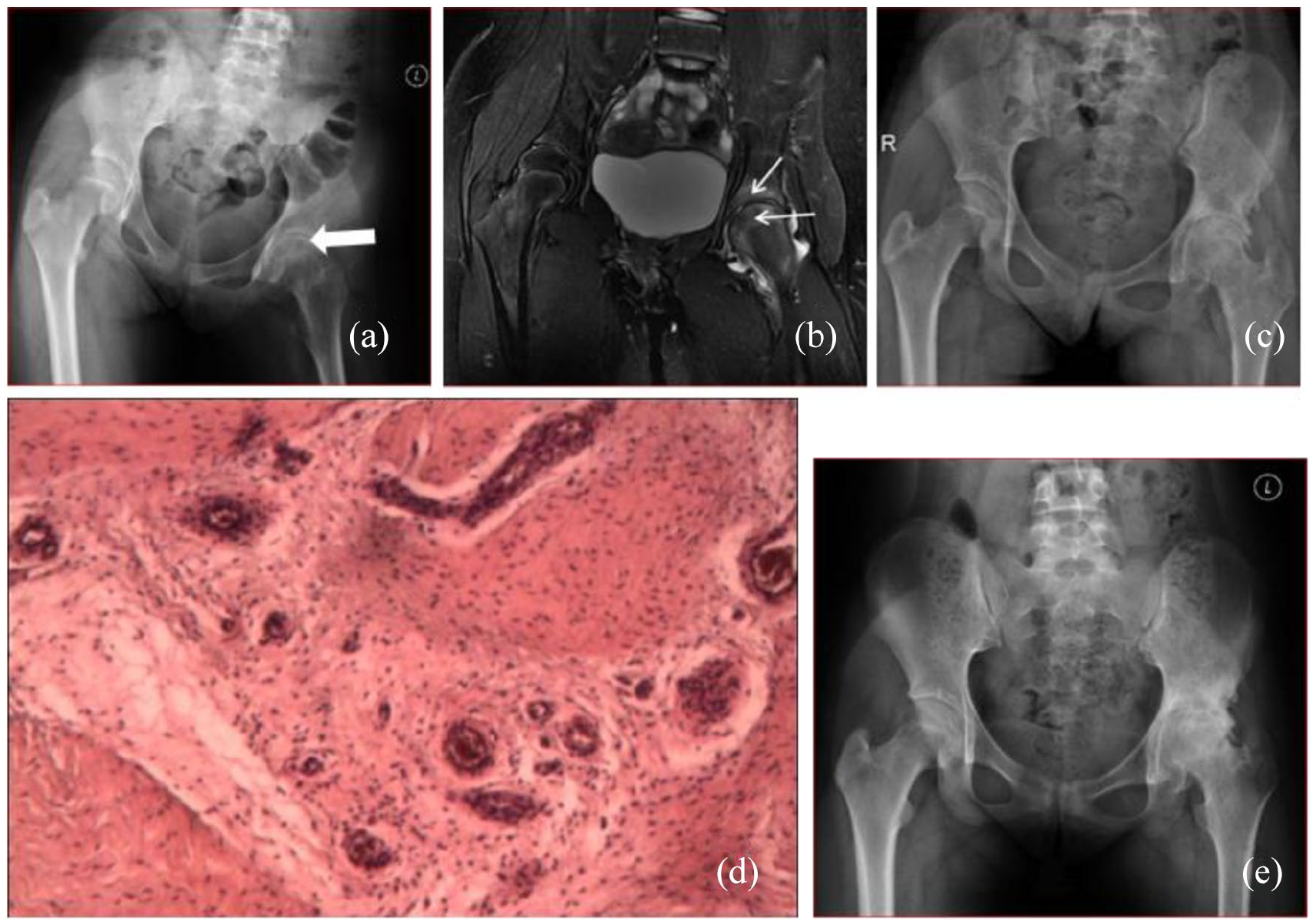
(a) X-ray of the hip joint at the time of consultation suggested a narrowing of the left hip joint gap (black arrow), the joint surface was not shiny, a few cystic bone destruction areas were seen under the joint surface, and the pelvis was tilted. (b) MR suggested thinning and discontinuity of the cartilage surface of the femoral head, and long T2 signal under the joint surface of the acetabulum and femoral head (white arrow), accompanied by a medium amount of joint fluid. (c) Calcium vitamin D chewable tablets, non-steroidal anti-inflammatory drugs, and joint rehabilitation physiotherapy were given as conservative treatment, but the joint gap was narrowed further, and degenerative changes in the hip joint were observed on plain film after 10 months of review. (d) After conservative treatment failed, left hip joint lesion removal + femoral head drilling decompression was performed, and postoperative synovial pathology indicated mild chronic aseptic inflammation. (e) At 30 months post-treatment, the plain film was reexamined, the joint gap disappeared, and the joint was tonic.
(a) Significant narrowing of the right hip joint space and pelvic tilt. (b) Trapezoid signal shadow of the right femoral head. The patient was treated with lower limb traction and hip joint release, but surgical effect was not good.
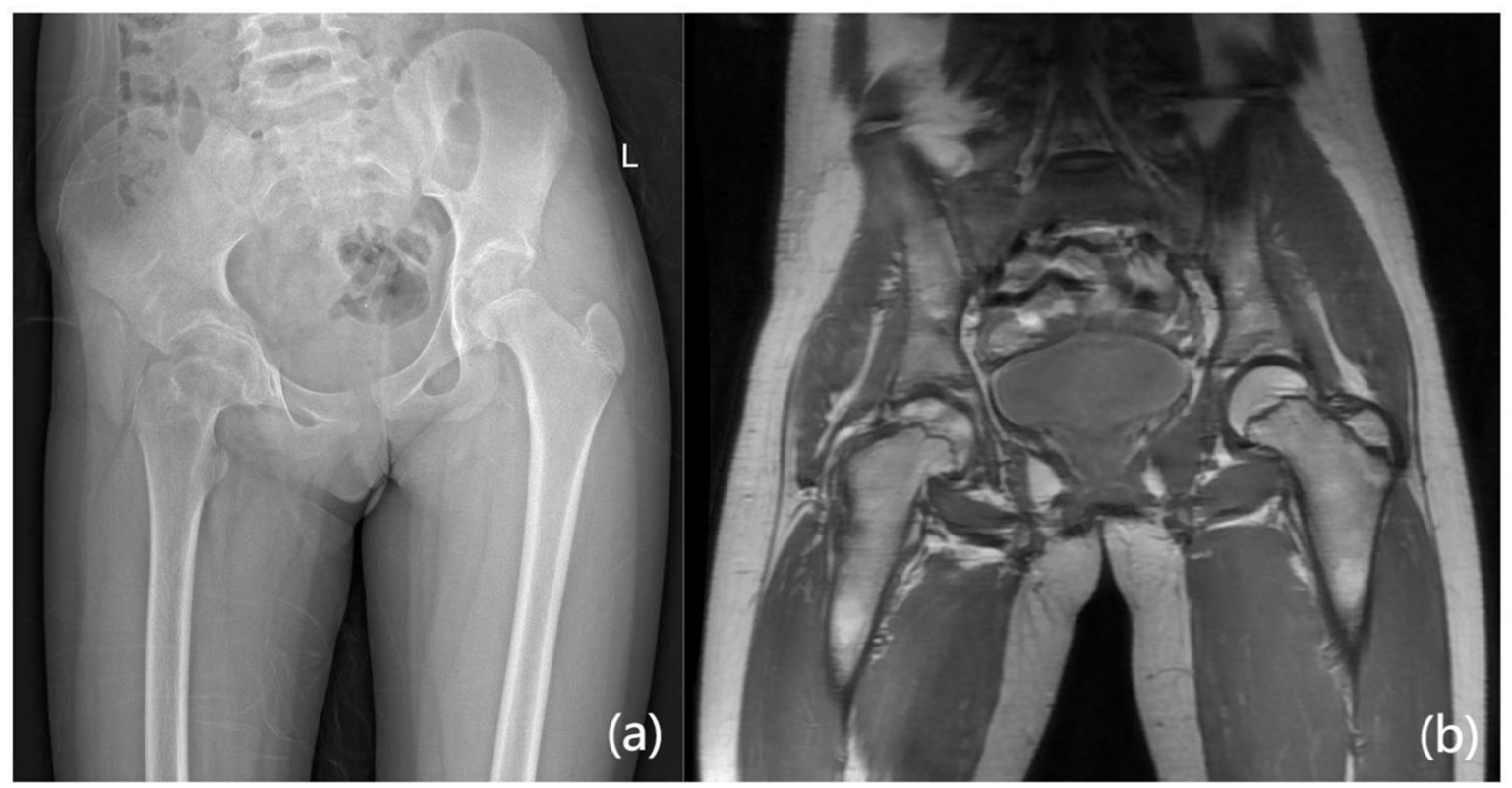
(a) Narrowing of the left hip joint space. There was sclerosis in the acetabulum and the corresponding femoral head. (b) MR showed that the cartilage of the left hip joint became thinner and the subchondral bone became cystic. (c) Underwent left femoral osteotomy. (d) Three months after surgery, the patient’s hip joint movement was limited and pain existed.
Classic case
Case 1, a female patient, 11 years old, was admitted to the hospital with the chief complaint of “right hip pain with limitation of movement for 8 months.” She was diagnosed with juvenile idiopathic arthritis and treated with corticosteroid (dexamethasone) and methotrexate, but her symptoms did not improve. At the time of admission, she had an obvious limping gait, a 30° flexion contracture of the hip joint, limited internal and external rotation, and a tilted pelvis. The imaging showed that the hip joint space was uniformly narrowed. Initially, she was given non-weight-bearing functional rehabilitation and oral ibuprofen to relieve pain and inflammation, but the outcome was not satisfactory. Subsequently, 12.5 mg subcutaneous injection of rhTNFR was administered for 6 months. At the 2-year follow-up, the hip joint function was improved significantly, the hip joint gap was widened, and the edema shadow in the femoral head was reduced.
Case 6, female, 11 years old, complained of “left hip pain, limping for 3 years.” The 8-year-old patient was misdiagnosed as aseptic necrosis of the femoral head and idiopathic hip arthritis in other hospitals. She had undergone hip arthrodesis to limit weight-bearing and was treated with corticosteroids and non-steroidal anti-inflammatory drug therapy. When she first visited our hospital, the patient had an oblique pelvis, unequal length of lower limbs, and significant limitation of hip motion in all directions. The image shows that the left hip space is <2 mm. rhTNFR was injected subcutaneously for 5 months, but no improvement was observed. The 7-year follow-up revealed significant hip arthritis and obvious walking pain obvious, which necessitated long-term oral pain medication.
Case 8, female, 12 years old, had fallen and injured her left hip, which gave rise to the left hip pain 9 months ago. This phenomenon was osteochondritis of the left femoral head by the external hospital. The patient received left lower limb skin traction and left internal adductor muscle release without improvement of symptoms. The patient’s blood analysis, CRP, ESR, complement, and interferon release test for tuberculosis infection presented negative results. On February 19, 2014, a left hip lesion removal + femoral head drilling and decompression + removal of the lesion was performed. Intraoperative findings: hyperplasia and hypertrophy of the left hip capsule, swelling of the synovial membrane, thinning of the cartilage in the weight-bearing area of the femoral head, partial exfoliation of the defect, and no case-like necrotic tissue. The postoperative pathology showed mild chronic inflammation (left hip synovium). After the operation, the patient was treated with oral glucosamine hydrochloride capsules, and 30 months post-treatment, the function was extremely poor, and the joint space had disappeared.
Discussion
In this cohort of 10 cases, most of the children had a prolonged diagnosis, and one or more misdiagnoses had occurred. Clinical imaging (MRI and X-ray) has provided great help for our correct diagnosis. Referring to the MRI classification of Amarnath et al. 24 , we used rhTNRF for early-stage patients and achieved exciting efficacy.
Kozlowski and Scougall 22 found that ICH disease is often associated with joint space narrowing in the early stages, and many international studies demonstrated that the MRI manifestations are specific and have some reference value for their differential diagnosis. For example, Johnson et al. 23 summarized the characteristics of 10 MR images of ICH patients and found that all patients had cartilage loss, a small amount of joint effusion, bone remodeling, and muscle atrophy. Laor and Crawford 13 reviewed the MRI presentations of seven patients with ICH and found a specific sign in all patients: an inverted triangular or trapezoidal long T1 and long T2 edematous area below the articular surface in the middle of the epiphysis. Similar imaging signs were observed in 9/10 patients in our group, which is consistent with the documented presentation. Amarnath et al. 24 first proposed MRI staging based on this specific sign. These included Stage I: long T1 and T2 edema is seen in the middle of the inferior lateral articular surface of epiphysis, which might be accompanied by narrowing of the joint space and synovial thickening, with little or no joint effusion; Stage II: an edematous signal in the acetabulum based on Stage I; Stage III: loss of the joint space and degenerative changes in the hip joint. The patients with poor outcomes after rhTNRF treatment all showed significant hip degenerative changes on imaging (Table 3).
Treatment methods and outcomes of 10 patients.
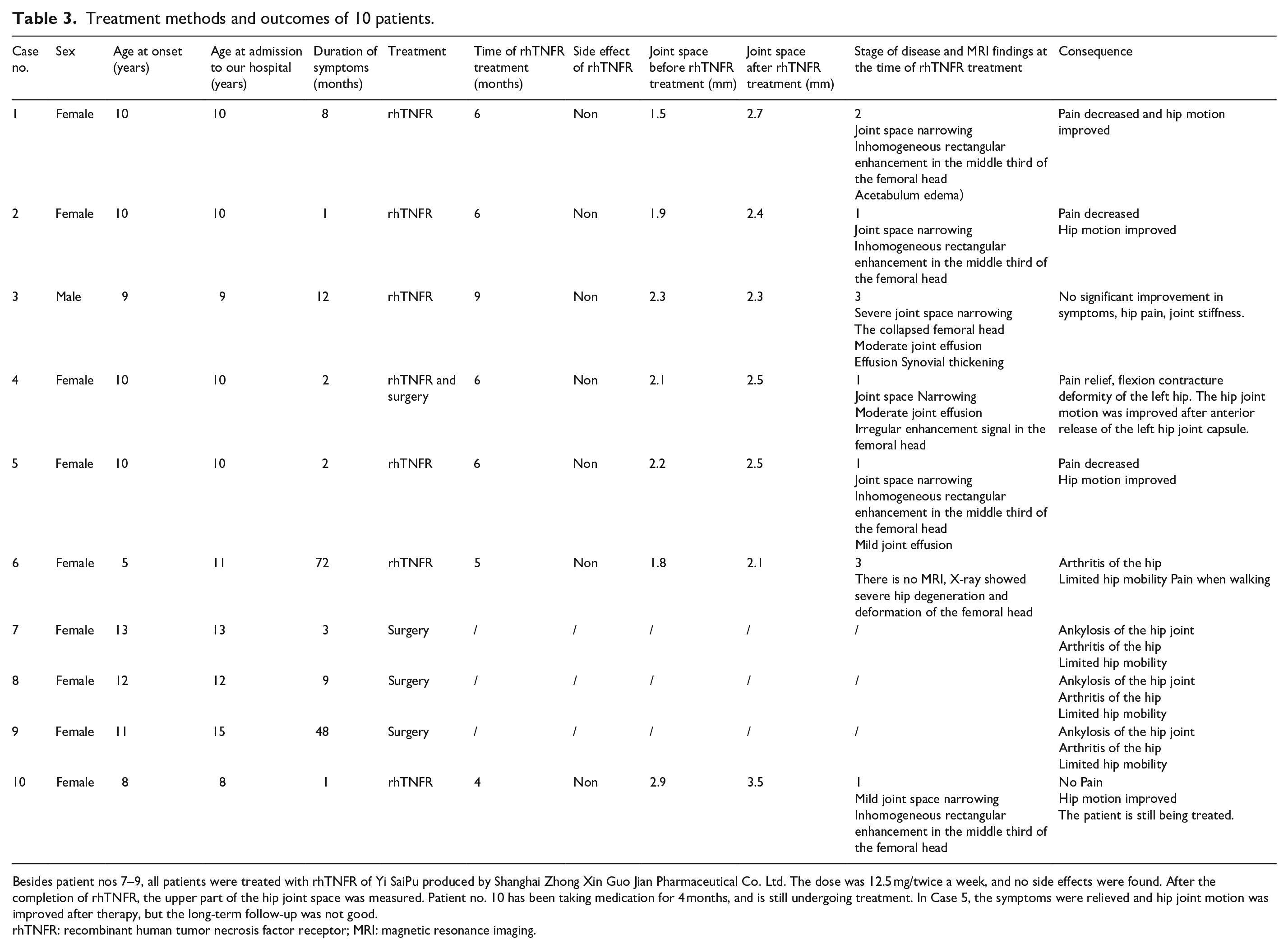
Besides patient nos 7–9, all patients were treated with rhTNFR of Yi SaiPu produced by Shanghai Zhong Xin Guo Jian Pharmaceutical Co. Ltd. The dose was 12.5 mg/twice a week, and no side effects were found. After the completion of rhTNFR, the upper part of the hip joint space was measured. Patient no. 10 has been taking medication for 4 months, and is still undergoing treatment. In Case 5, the symptoms were relieved and hip joint motion was improved after therapy, but the long-term follow-up was not good.
rhTNFR: recombinant human tumor necrosis factor receptor; MRI: magnetic resonance imaging.
In our study, a total of four patients had previously undergone surgery, only case 4 showed functional improvement. The patient was 10 years old and had pain for only 2 months. He was treated with rhTNFR directly in our hospital. After 6 months of continuous treatment with rhTNFR, the pain of the hip joint was relieved, but the deformity of flexion contracture remained. The joint effusion also increased. After discussion, it was decided to treat the patient with an anterior capsular release. Next, we observed significant relaxation of the hip joint after successful anesthesia and significant improvement in hip motion after the operation. Although, Korula et al. 4 and Laubscher et al. 25 considered the efficacy of surgery for ICH to be modest. We believe that surgical treatment is not useless, and appropriate surgical intervention can save the day when conservative treatment fails.
ICH and jejunoileal arthropathy (JIA) have many similar features, and it is still controversial whether the two are related or whether ICH is one of the unclassified phenotypes of JIA. In recent years, several case studies have been reported on the efficacy of immunosuppressor agents in this group of patients.16,21,26 RhTNFR plays a critical role in immune regulation and control of the inflammatory reactions. Blocking TNF-α may increase the risk of infection.27,28 Other adverse reactions include injection-site local reactions, such as mild to moderate erythema, itching, pain, and swelling. None of these adverse reactions occurred in our cases.
The efficacy of rhTNFR has been variable. The occurrence of this situation may be related to the duration of ICH and the stage of disease when receiving rhTNFR treatment. Patients in the third category of the Camarnat classification 24 who develop arthritis of the hip are less likely to respond to medication. In contrast, four of the five patients who had a response to rhTNFR were in Stage I of the Camarnat classification at the time of treatment (All four patients were admitted to our hospital for immunotherapy within 3 months after the onset of the disease), and one patient was in Stage II, according to the MRI of the patients.
In conclusion, ICH is a rare clinical condition that Kampani et al. 16 is easily misdiagnosed and delayed. Early MRI is a critical reference for diagnosis. Adequate knowledge of the disease is valuable in making an accurate diagnosis and timely intervention. Presently, there is no consensus on the treatment of this disease. In this study, the efficacy of rhTNFR was unexpected, particularly in the early stages of ICH. We recommend that patients with ICH prior to Stage III be actively treated with rhTNFR. And the earlier the treatment is started, the better and faster the effect is.
Footnotes
Acknowledgements
I would like to thank Professor Bin Fang for guiding the writing of the article in terms of clinical knowledge and treatment experience. I also thank Dr Hao Xiong for the case collection work, and finally, Dr Zhao Dun and Dr Guan Tianan for writing our treatment methods and experience into the manuscript.
Author contributions
T.G. is responsible for writing the paper. D.Z. is responsible for translation, typesetting, and contribution. H.X. and Y.L. are responsible for the collection of case related data. B.F. and Y.L. gave writing instructions. T.G. and D.Z. contributed equally to the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the institutional review board of the First Affiliated Hospital of Guangzhou University of Chinese Medicine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.