
Abstract
Objectives
Herpes simplex encephalitis (HSE) is one of the most common causes of severe viral encephalitis. The characteristic manifestations of HSE include cerebrospinal fluid with mild cytopenia, dominated by lymphocytes, elevated protein, and normal blood glucose values (3.9–6.1 mmol/L). Although it is not difficult to diagnose classical HSE, diagnosing clinically atypical cases is more difficult.
Methods
We reviewed the results of next-generation sequencing (NGS) of CSF in a series of patients diagnosed with atypical HSE.
Results
Four patients lacking classical clinical manifestations of HSE, including no fever, headache, or other typical neurological deficit symptoms, 1–2 × 106 cells/L CSF leucocyte count, and no typical imaging features, were diagnosed with atypical HSE by NGS of CSF. The NGS reads corresponding to herpes simplex virus type 1 ranged from 2 to 13,174.
Conclusions
Mild HSE may not present with classic frontotemporal lobe syndrome and fever may not be an inevitable symptom in patients with immunosuppression. However, the possibility of HSE should be considered in patients with atypical intracranial infection, and these patients should be tested by NGS.
Keywords
Introduction
Herpes simplex encephalitis (HSE) is one of the most common causes of severe viral encephalitis. Most cases of adult HSE are caused by herpes simplex virus type 1 (HSV-1), and about 10% of cases can be attributed to HSV-2. HSE mainly affects the temporal lobe and lower frontal lobe, leading to characteristic manifestations of acute fever, headache, disorientation, change of consciousness level, and various neurological signs. Cerebrospinal fluid (CSF) analysis usually shows mild cytopenia, dominated by lymphocytes, elevated protein, and 3.9 to 6.1 mmol/L blood glucose. 1 Magnetic resonance imaging (MRI) is the most sensitive diagnostic method, and the main features include frontotemporal lobe edema, sometimes with a space-occupying effect. Virus isolation and CSF polymerase chain reaction (PCR) have become the gold standard for the diagnosis of HSE, and it is relatively straightforward to diagnose classical HSE based on a combination of clinical manifestations and PCR technology. However, virus isolation and identification are time-consuming and have a low detection rate, while PCR is limited by the nucleic acid fragments that can be combined by primers. It is therefore harder to diagnose atypical HSE in patients who show no signs of fever, headache, and other typical neurological deficit symptoms, and who have no significant leukocytes in the CSF and no typical imaging features. HSE was previously associated with 70% mortality in untreated patients, and only 2.5% of patients who survived without appropriate treatment recovered normal neurological function. However, a correct diagnosis and treatment before the patient loses consciousness can reduce the mortality rate to 17% to 30%, and treatment started within 4 days of onset can further reduce the rate to 8%. 2 It is therefore crucial to make an early diagnosis of HSE, given the serious consequences of misdiagnosis and missed diagnosis. Second-generation sequencing technology (NGS) is not limited by targeted primers, has a fast detection speed and high detection rate, and can quickly and efficiently realize an accurate diagnosis of infectious diseases of the central nervous system (CNS). Since it was first reported in 2014, NGS has been widely used for the detection of CSF pathogens.3–5 In this study, we analyzed the clinical, CSF, and imaging features of four patients with atypical HSE diagnosed by CSF NGS, with the aim of improving clinicians’ understanding of atypical HSE and thus facilitating its early diagnosis and improving its prognosis.
Materials and methods
Patients
This study included patients with HSE who were hospitalized and diagnosed in the Department of Neurology at our hospital from January 2019 to January 2021. This study was approved by the Ethics Committee of Hengshui People’s Hospital (approval no. 2019-1-024), and the patients and their families were informed of the study content and signed an informed consent form.
The inclusion criteria were: (1) patients with suspected encephalitis, and human HSV-1 virus sequence detected by NGS of CSF; (2) clinical and laboratory examination excluded evidence of other microbial infection; and (3) patients who signed informed consent. The exclusion criteria were: (1) non-infectious encephalitis such as autoimmune encephalitis, paraneoplastic marginal encephalitis, optic neuromyelitis pedigree disease, and immune rheumatic diseases involving the CNS; (2) patients with CNS tumors and space-occupying diseases; and (3) patients who had contraindications to lumbar puncture or inability to obtain CSF. The reporting of this study conformed to the CARE guidelines. 6
Methods
NGS of CSF
CSF (1–2 mL) specimens were obtained by lumbar puncture, added to test tubes, and stored at −80°C for 30 minutes and used for NGS. DNA was extracted from the CSF samples using a micro-sample genomic DNA extraction kit (Tiangen Biotech, Beijing, China) and fragmented into 200 to 300 bp fragments using a DNA cutting ultrasonic crusher (Bioruptor Pico protocols, Diagenode, Liege, Belgium). After quality control to check the size of the fragments using a 2100 biological analyzer (Agilent Technologies, Santa Clara, CA, USA), the DNA library was detected by quantitative PCR. (3) DNA libraries were constructed by end-repair, A-tailing, adapter ligation, and PCR amplification using an NGS library construction kit (Genskey, Tianjin, China). Roller amplification technology was performed to increase single-stranded circular DNA two to three fold to obtain DNA nanospheres. (4) The DNA nanospheres were loaded on the sequencing chip (Institute of Medical Laboratory, Tianjin BGI Technology Co., Ltd. Tianjin, China) and sequenced using the BGISEQ.50 sequencing platform (Medical Laboratory of Tianjin Huada Genome Technology Co., Ltd., Tianjin, China).
After data analysis and quality control sequencing, reads with low quality, low complexity, and sequences <35 bp were removed, and the high-quality sequencing data were compared with the BWA human genome database. Interference from human genome sequence information was eliminated, and the remaining data were compared with a microbial database to achieve a preliminary identification of bacteria, viruses, fungi, and protozoa. All species included in the curated pathogen reference database were collected from published manuals or the NCBI RefSeq genome database. The database contained 9855 bacterial genomes, 6926 whole genome sequences of viral taxa, 1582 fungal taxa, 312 parasites, 184 mycoplasma, and 177 mycobacteria. The main observation index was virus species, which were identified conditional on the detection of >1 virus sequences by NGS of CSF.
Antibody detection
Indirect immunofluorescence assay (autoimmune encephalitis test kit; Hebei Jianhai Medical Laboratory, Shijiazhuang, Hebei, China) was used to detect autoimmune encephalitis antibodies, with initial dilution titers of CSF and serum of 1:1 and 1:10, respectively. The cell-based assay had high diagnostic specificity and sensitivity. Cells were observed under a fluorescence microscope (Olympus, Tokyo, Japan).
Results
Clinical findings
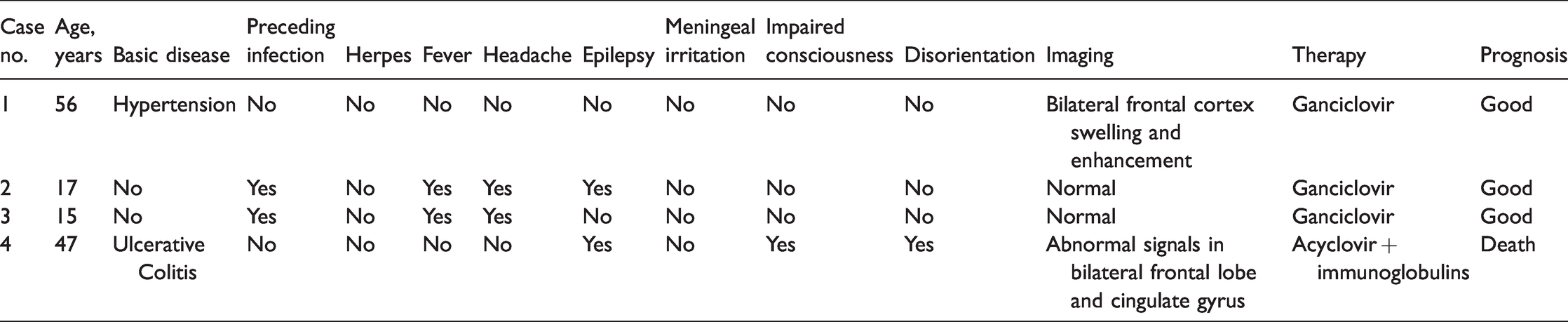
Four patients met the enrollment criteria. All patients were female, aged 15 to 56 years old (33.75 years), and all four had experienced acute attacks of HSE. HSV-1 was identified in all four patients by NGS of CSF. Their clinical features are summarized in Table 1 and their laboratory results are summarized in Table 2.
Clinical features of four patients with herpes simplex encephalitis.
Test results of cerebrospinal fluid in four patients with herpes simplex encephalitis.

Numbers in brackets indicate normal range. WBC, white blood cells; LYM, lymphocytes; NGS, next-generation sequencing.
Case 1
A 56-year-old woman presented with head discomfort for more than 10 days. She had an 8-year history of hypertension. Nervous system examination showed no abnormality, and no obvious blood, urine, or stool abnormalities were detected by routine observations and blood biochemical tests. Human immunodeficiency virus (HIV), syphilis, and hepatitis B were excluded. Her autoantibody spectrum and immune functions were normal and her autoimmune encephalitis antibody was negative. MRI showed high fluid-attenuated inversion recovery (FLAIR), low diffusion-weighted imaging (DWI), and high apparent diffusion coefficient (ADC) signals in the bilateral frontal lobes. Head MRI enhancement showed swelling of the bilateral frontal cortex with mild enhancement (Figure 1). Her CSF results are shown in Table 2. HSV-1 was identified by NGS of the CSF and confirmed by PCR. The revised diagnosis was HSV encephalitis. The patient was treated with ganciclovir for 21 days. During the follow-up 3 months after discharge, the patient resumed her daily life and working ability with no symptoms of neurological impairment.

Magnetic resonance imaging (MRI) results in patient 1. MRI showed high fluid-attenuated inversion recovery (a), low diffusion-weighted imaging (b), and high apparent diffusion coefficient signals (c) in the bilateral frontal lobes. MRI enhancement showed slight enhancement of the complete nidus (d) (red arrows).
Case 2
A 15-year-old girl with no medical history presented with fever and headache for 6 days after catching a cold. Nervous system examination, electroencephalogram, and head MRI showed no abnormalities and no obvious blood, urine, or stool abnormalities were detected by routine observations and blood biochemical tests. Tests for hepatitis B (HB) surface antigen, HB surface antibody, HB e antigen, HB e antibody, HB core antibody, HIV antibody, thymostimulin, and hepatitis C virus antibody were all normal. Her autoantibody spectrum and immune functions were normal and autoimmune encephalitis antibody was negative. Her CSF results are shown in Table 2. HSV-1 was identified by NGS of the CSF and confirmed by PCR. The diagnosis was HSV encephalitis, and the patient was treated with ganciclovir for 14 days. The patient’s condition improved and she was discharged, with no symptoms of neurological impairment during the 3 months after discharge.
Case 3
A 17-year-old girl presented with convulsion for 2 hours. Nervous system examination showed and MRI showed no abnormalities. No obvious blood, urine, or stool abnormalities were detected by routine observations and blood biochemical tests, and tests for HB surface antigen, HB surface antibody, HB e antigen, HB e antibody, HB core antibody, HIV antibody, thymostimulin, and hepatitis C virus antibody were all normal. Her autoantibody spectrum and immune functions were normal and autoimmune encephalitis antibody was negative. Her CSF results are shown in Table 2. HSV-1 was identified by NGS of the CSF and confirmed by PCR. The final diagnosis was HSE, which was treated with ganciclovir for 14 days, and the patient had no symptoms of neurological impairment at 1 month after discharge.
Case 4
A 47-year-old woman was hospitalized for 1.5 hours due to urinary incontinence and disturbed consciousness. She had a history of ulcerative colitis and a history long-term oral prednisone and azathioprine use. The patient was unresponsive during physical examination on admission, but no other abnormalities were found. MRI showed symmetrical abnormal signals in the bilateral frontal lobes and cingulate gyrus (Figure 2). Laboratory tests showed a white blood count 14.29 × 109/L and neutrophil ratio 94.5%. Liver function tests showed total protein 53.4 g/L, albumin 33.9 g/L, and prealbumin 413 mg/L. HB surface antigen, HB surface antibody, HB e antigen, HB e antibody, HB core antibody, HIV antibody, thymostimulin, and hepatitis C virus antibody were all normal. Her CSF results are shown in Table 2. The patient had a CSF leukocyte count of 1 × 106 cells/L and lacked the inflammatory CSF features of infectious CNS diseases. Combined with the patient’s history of immune abnormalities, the likely diagnosis was autoimmune encephalitis. Autoimmune encephalitis antibody detection and CSF NGS detection were performed to exclude herpes simplex virus, and methylprednisolone sodium succinate 1 g pulse + acyclovir was given at the same time. The patient’s consciousness gradually worsened and she developed status epilepticus. Re-examination of the images showed multiple intracranial hemorrhage foci. In addition, autoimmune encephalitis antibody was negative and HSV-1 was identified by NGS of the CSF and confirmed by PCR. The patient was finally diagnosed with HSE. Antiviral therapy was continued with intravenous injection of human immunoglobulin, but the patient eventually died of central respiratory and circulatory failure.

Magnetic resonance imaging (MRI) results in patient 4. MRI showed high fluid-attenuated inversion recovery (a), high diffusion-weighted imaging (b), and low apparent diffusion coefficient signals (c) in the bilateral cingulate gyrus (red arrows).
Discussion
HSV leading to HSE can be classified as HSV-1 or HSV-2, with about 75% of viral encephalitis caused by HSV type 1. The mechanism by which HSV gains access to the CNS is still unclear; however there are currently two hypotheses for virus activation. HSV-1 may enter the semilunar ganglion of the trigeminal nerve through the oral and nasal mucosa, and then enter the frontotemporal lobe along the branch of trigeminal nerve to the meninges of the skull base. In primary infection, the virus enters the cerebral lobe directly through the olfactory bulb and olfactory tract, or enters the brain through the trigeminal nerve after oral infection. 7 HSV-1 is therefore characterized by involvement of the temporal lobe, the base of the frontal lobe, the insular cortex, and the cingulate gyrus. The clinical manifestations of HSE are nonspecific and are similar to meningoencephalitis caused by other pathogens, mainly including headache, fever, neck ankylosis, focal neurological deficit, disturbed consciousness, abnormal mental behavior, epilepsy, and cognitive impairment. The relatively specific symptoms of HSE include prodromal symptoms of upper respiratory tract infection and neurological manifestations associated with frontotemporal lobe dysfunction. In the present study, patients 1 and 4 had no prodromal symptoms of upper respiratory tract infection or classical encephalitis-like manifestations, such as fever and headache. In particular, patient 1 was only admitted to hospital with a main complaint of head discomfort, and no symptoms or signs of nervous system involvement were found by physical examination. The initial diagnosis in both these patients was therefore non-intracranial infectious disease. In contrast, patients 2 and 3 were young women with an acute onset and history of prodromal infection (fever, runny nose, and fatigue). Symptoms such as headache, fever, and seizures appeared sequentially during the course of the disease, in accord with the clinical characteristics of infectious CNS diseases.
Previous studies found that more than 95% of HSE patients had abnormal CSF, with a slight increase in the number of cells (usually 10–200 cells/mm3), mainly monocytes and red blood cells, reflecting the bleeding occurring as a result of brain parenchyma infection. More than 80% of patients had slightly elevated CSF protein levels. 8 However, no increase in CSF leukocyte count was found in any of the patients in this study, in contrast to the typical CSF changes in HSE. This tends to suggest a diagnosis of autoimmune encephalitis or other diseases. Comprehensive analysis showed no significant changes related to virus presence or replication in the CSF in patients 1, 2, and 3, while the changes in the CSF in patient 4 were not significantly related to long-term oral immunosuppressants, which inhibited activation of the immune system, resulting in a lack of characteristic changes in the CSF. Doctors should thus be aware of the possibility of HSE lacking typical CSF characteristics to avoid a missed diagnosis or delayed diagnosis and treatment.
HSE is a progressive inflammatory process that begins in the medial temporal lobe and gradually extends to the limbic system, including the frontal lobe and hippocampus. Neuroimaging has shown that HSE lesions first involved the temporal lobe, unilaterally or bilaterally, and may progress to the frontal lobe or occipital lobe, but rarely occurred in the frontal lobe or occipital lobe alone. The lesions have a clear boundary with the lenticular nucleus and the convex surface facing outwards, showing a “knife cutting sign”, which is the most characteristic manifestation of the disease. 9 In this study, none of the patients had any significant changes in the CSF and head MRI examination was therefore performed. However, the imaging changes were not in accord with the typical imaging characteristics, with initial temporal lobe involvement. MRI of patient 1 showed an abnormal signal in the bilateral frontal lobes with limited focus. FLAIR, T2, ADC high signal, and DWI low signal suggested the existence of angiogenic edema. Because the patient has no clinical encephalitis-like changes, a diagnosis of trauma or tumor was suggested. There were no definite MRI abnormalities in patients 2 and 3, but seizures occurred in the course of the disease, suggesting brain parenchyma injury, and the lack of abnormalities in head MRI in these two patients might have been related to the degree of brain injury. The bilateral frontal lobes and cingulate gyrus were the main regions involved, in patient 4, with no involvement of the temporal lobe. High signal intensity of FLAIR, T2, and DWI, and low signal intensity of ADC were relatively rare. Although neuroimaging examination is not routine in patients with suspected CNS infection, it is still necessary in patients older than 60 years, and in patients with immunosuppression, CNS history, seizures within 1 week, and neurological defects, 10 especially in cases with atypical symptoms and signs of HSE. MRI may thus facilitate a correct diagnosis.
NGS can provide direct information on pathogenic microorganisms from diseased brain tissue and CSF with high throughput, thus shortening the detection process and overcoming the limitations of targeted diagnostic methods. In 2015, Guan et al. reported the results of NGS CSF analysis in four patients with suspected viral encephalitis, and identified two cases of HSV1, one case of HSV2, and one case of varicella zoster virus, with genome coverage of 12% to 98%, indicating the value of NGS for the diagnosis of human herpesvirus CNS infections. 4 In 2016, Yao et al. reported the results of CSF NGS for the diagnosis of Listeria meningoencephalitis, thus expanding the its clinical application to the diagnosis of specific bacterial CNS infections. 5 NGS technology is thus of great significance for the diagnosis of atypical intracranial infections. Guan et al. also used NGS to make a clear diagnosis of meningeal cysticercosis in patients with atypical symptoms and signs with a long-term delay in diagnosis and treatment, further highlighting its value for identifying atypical intracranial infections. 11 In the current study, although the typical clinical manifestations and CSF changes of HSE were absent, comprehensive analysis suggested an intracranial infection and indicated the need to focus on the differential diagnosis of autoimmune encephalitis. We therefore carried out CSF NGS to detect the pathogen. The detection of autoimmune encephalitis antibodies excluded autoimmune encephalitis, and the patients were accordingly finally diagnosed with HSE.
The experience and lessons learnt through patient 4 were more profound. Because of the lack of typical CSF changes and the high DWI signal on in head MRI, patient 4 was initially diagnosed with acute cerebral infarction and autoimmune encephalitis. The early stage of nerve cell injury caused by HSV infection would include cytotoxic edema, followed by high signal intensity DWI, but the signal brightness was significantly less than that caused by acute cerebral infarction and the duration was relatively short. Notably, the focal area did not conform to the distribution of blood vessels. 9 In addition, the patient’s history of ulcerative colitis and lack of typical CSF changes may suggest autoimmune encephalitis. However, if autoimmune encephalitis antibody results are negative or not available, CNS infection should be ruled out before making a diagnosis of “clinically suspected autoimmune encephalitis. Routine and biochemical changes in the CSF following lumbar puncture in this patient were not obvious, which may lead doctors to ignore the possibility of a CNS infection and administer hormone shock therapy. In these patients, CSF NGS can help to identify or exclude CNS infection, and if conducted at an early stage, the results might avoid the use of high-dose hormone shock therapy.
Conclusions
In this study, patients with mild HSE may not show classic frontotemporal lobe syndrome. Fever is one of the most common symptoms at the onset of HSE, but may not be an inevitable symptom in patients with immunosuppression. The possibility of HSE should be considered in patients with atypical intracranial infection, and NGS detection should be carried out. To reduce the nervous system sequelae antiviral therapy (acyclovir) should be started immediately in patients with a suspected diagnosis of HSE, and treatment should then be adjusted according to the imaging, serology, and molecular testing results.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Projects in Science and Technique Plans of Hengshui City [grant number 2019014078Z].