
Abstract
Purpose:
We present the paraspinal approach use for neuromuscular scoliosis with focus on deformity correction, perioperative (≤30 days) morbidity and outcome at a minimal follow-up length of 2 years.
Methods:
We prospectively collected data of 61 neuromuscular scoliosis patients operated using a paraspinal (Wiltse) approach between 2013 and 2019. We additionally collected data of 104 control cases, operated using a midline approach between 2005 and 2016. Fifteen Wiltse, respectively 37 control patients were excluded due to a short follow-up (<2 years), and 22 controls were excluded secondary to lacking follow-up data. Hence, 46 Wiltse and 45 control patients were compared.
Results:
Wiltse and control patients had comparable follow-up lengths, demographics, deformity corrections, complication rates, number of levels fused, and intensive care unit and hospital lengths of stay. Wiltse cases had a lower estimated blood loss (535 vs 1187 mL; p-value < 0.001), allogenic transfusion rate (48% vs 96%; p-value < 0.001), and operating time (ORT) (337 vs 428 min; p-value < 0.001) than controls. This was also the case when selecting for patients without pelvic fixation (p-values < 0.001). When selecting the cases with pelvic fixation (20 among 91 cases), only the number of levels fused and the ORT differed significantly according to the approach (p-value <0.015 and <0.041).
Conclusion:
The paraspinal approach for neuromuscular scoliosis is safe, associated with significant deformity correction, reduced estimated blood loss, and allogenic transfusion rate. These potential benefits still need to be evaluated, especially for cases with pelvic fixation, with further follow-up of larger cohorts.
Level of evidence:
level III.
Keywords
Introduction
The posterior paraspinal muscle approach, equivalent to a Wiltse approach, is widely used for spinal trauma, degenerative, and neoplastic adult cases.1–6 It is becoming commonly used for adult spine deformity and was recently implemented to adolescent idiopathic scoliosis (AIS).7–10 The potential advantages of this technique over the posterior midline approach are related to a reduced soft tissue trauma lowering the post-operative pain, the post-operative opioid consumption, the estimated blood loss (EBL), the allogenic transfusion rate, and the length of stay (LOS). In the pediatric population, the best evidence supporting these advantages has been shown for AIS patients.7–10 The largest retrospective comparative study reporting AIS cases compared 192 cases operated using a paraspinal muscle approach to 293 cases operated through a midline approach. 7 This study reporting AIS cases showed a lower opioid consumption, EBL, and transfusion rate, and a shorter hospital LOS for the paraspinal muscle group. The literature reporting the use of this approach for neuromuscular scoliosis (NMS) is scarce. Only one retrospective comparative series including 24 patients and one surgical technique paper including two case reports have been published up to date.11,12 Both publications reported a lower EBL in comparison to the posterior midline approach and the surgical technique paper showed additionally a shorter intensive care unit (ICU) and hospital LOS.
The aims of this study were to compare the deformity correction, intraoperative parameters including the EBL and the safety of the posterior paraspinal muscle approach (Wiltse) to the use of the posterior midline approach for treating NMS patients. Our primary hypothesis was that the Wiltse approach, in comparison to the posterior midline approach, allows a comparable deformity correction along with similar or lower intraoperative and perioperative complication rates and a lower EBL and hospital LOS.
Materials and methods
Since August 2013, three senior surgeons (R.D., V.S., and T.A.) have utilized the Wiltse approach in NMS patients at three tertiary medical centers. A total of 61 NMS patients, operated between August 2013 and June 2019 using this approach, are part of a continuously maintained prospective database. These patients and an additional series of 104 control patients were included. The control patients were operated by two senior surgeons (V.S. and T.A.) at two tertiary institutions using a posterior midline approach between November 2005 and March 2016. Fifteen Wiltse, respectively 37 control patients were excluded due to a short follow-up (FU) (<2 years), and 22 control patients were excluded secondary to lacking FU data. Hence, 46 Wiltse and 45 control patients with a clear neuromuscular pathology leading to NMS were retrospectively compared. All patients excepted one had a minimal FU of 2 years. It was a control patient which died of bacterial tracheitis at post-operative day (POD) 24 and was not excluded to avoid a selection bias. The collected data were as follows: age, gender, body mass index (BMI), the diagnosis leading to NMS, the pre-operative gastrostomy tube and/or respiratory assistance presence, major curve, and pelvic obliquity measurements (pre-operative, post-operative, and at final FU). Complications were recorded too and categorized in function of their chronological occurrence in relation to the timing of the surgery (intraoperative, perioperative (≤30 POD), late (>30 POD)). Perioperative complications were reported globally, independently of their origin, and as approach-related complications. The latter were consisting of those complications which might be associated with the used approach. We further assessed the following surgical variables, globally and with subgroup analysis according to the presence or absence of pelvic fixation: number of levels fused, operating time (ORT), EBL, percentage of EBL of estimated blood volume, allogenic transfusion rate, and the ICU and hospital LOS. The ORT was calculated from the time of incision to the wound closure. The anesthetic team evaluated the EBL by counting blood loss in the suction cannula and cell saver. Surgical sponges were not typically used, but if used, they were also taken into account for blood loss estimation. The estimated blood volume was calculated as 70 mL/kg (weight). 13 Tranexamic acid and cell saver were used for all cases, and a uniform post-operative protocol was followed. The ICU and hospital LOS were calculated from the time the patient left the operating theater to the time the patient left the ICU, respectively, the hospital.
Surgical technique
The technique using paraspinal muscle approach for treating AIS patients has been previously reported.8,14 A modification of it was described to adapt for NMS cases which need longer instrumentations and usually present with more rigid curves. 11 We used a single midline skin incision extending from upper to lower instrumented vertebra and following the spinous processes. No fluoroscopy was used to determine the length and localization of it. After skin incision, the skin was undermined laterally to allow paramedian extraperiosteal bilateral fascial incisions. A blunt, muscle-sparing approach was used down to the facet joints in the lumbar spine, respectively, to the transverse processes in the thoracic spine. This was similar to the approach described by Wiltse et al. 15 for the lumbar spine. The posterior elements were exposed using electrocautery, from the base of the lamina to the transverse process. If pelvic fixation was performed, the skin was more laterally undermined in the caudal aspect of the incision up to the posterior superior iliac spine (PSIS) where a separate fascial incision was performed. The cortex was opened at the PSIS with a Luer to avoid screw head protrusion and the Iliac bone was cannulated using free-hand technique. Wide facetectomies were performed, and the pedicles were cannulated using a free-hand technique. 16 We did not routinely used navigation with intraoperative computed tomography (CT) scans or fluoroscopy for the pedicle preparation to reduce the radiation exposure. After cannulation, the pedicles remained localized by the insertion of pedicle markers. The facet joints were decorticated using a high-speed burr and bone graft (mixture of local autograft and freeze-dried allograft) was applied. We routinely used all-pedicle-screw constructs.
After the exposure, facetectomies, pedicle marker introduction, decortication, and bone grafting were performed on both sides, the definitive instrumentation was undertaken. Cannulated pedicle screws connected to reduction tubes were inserted on the convex or the concave side of the major curve, as was the surgeon’s preference. They were exchanged with the cannulated pedicle markers using guide wires. After all the pedicle screws were introduced, two 5.5-mm diameter cobalt-chrome rods were cut to the measured length. The first to be inserted was contoured with the appropriate sagittal profile. The rod was inserted first on the convex or the concave side as was the surgeon’s preference, from caudal to cephalad using the slots of the reduction tubes to avoid inadvertently pushing on patient’s head. Rod de-rotation or translation with gradual spine-to-rod reduction was used to correct most of the deformity. The rod was secured using screws, and direct apical segmental de-rotation was additionally performed. A second contoured rod was then used for the other side. In case of pelvic fixation, each rod was connected to the ipsilateral iliac screw using a transverse connector which was transmuscularly tunneled. For the standard approach, the instrumentation and correction techniques were similar. The exposure, in contrast, was in the midline elevating all the muscles off the posterior elements exposing the spine from spinous process till the tips of transverse processes; if pelvic fixation was performed, the caudal aspect of the incision was laterally extended up to the PSIS. The study had institutional ethical approval (CCER 15152).
Statistical analysis
The Shapiro–Wilk test was used to evaluate the data distribution’s normality. The characteristics depicting normal distribution between groups were compared using unpaired Student’s t-tests and Pearson’s chi-square test for dichotomous outcomes. Characteristics showing non-normal distribution were compared using unpaired Wilcoxon–Mann–Whitney tests. The significance level was set at p < 0.05. Cohen’s effect size and 95% confidence intervals (95% CIs) were reported. Analyses were performed using R software (version 3.1.3) and the RStudio interface.
Results
The mean follow-up was 3.3 (range 2–8) versus 4 (range 2–8) years for the Wiltse respectively the control cases. Cerebral palsy was the most prevalent diagnosis (44 among 91 cases) and was equivalently represented in both groups (p-value > 0.999) (Table 1). Baseline parameters (i.e. demographics, diagnosis, pre-operative radiographic parameters, and pre-operative need for gastrostomy tube or respiratory assistance) were not significantly different among both groups (Table 1). The initial major curve correction was significant, even when significance was set at p < 0.0001, and equivalent in both groups (Wiltse 39° or 57%, controls 44° or 60%, p-values = 0.153 and 0.421) and lasted at final FU (Wiltse 39° or 57%, controls 42° or 56%, p-values = 0.440 and 0.817) (Figure 1). The initial pelvic obliquity correction was 6° in both groups (p-value = 0.668) and remained 6° at final FU (p-value = 0.938) (Figure 1). The complication and mortality rates were not differing significantly in both groups (Table 3 and Figure 2). No neurologic complication occurred. Wiltse cases (n = 46) globally had a lower EBL (535 vs 1187 mL; p-value < 0.001), percentage of EBL of estimated blood volume (23% vs 57%; p-value < 0.001), allogenic transfusion rate (48% vs 96%; p-value < 0.001), and ORT (337 vs 428 min; p-value < 0.001) than controls (n = 45). This was also the case when selecting for patients without pelvic fixation (p-values < 0.001). In this subgroup (32 among 46 Wiltse and 39 among 45 Controls), the hospital LOS was additionally significantly shorter for Wiltse cases. When selecting the cases with pelvic fixation (14 among 46 Wiltse and 6 among 45 Controls), only the number of levels fused and the ORT differed significantly according to the approach (p-values < 0.015 and < 0.041). Table 2 reports the surgical variables mentioned here above and the approach-related perioperative complications, globally and with subgroup analysis in function of the variable “pelvic fixation.”
Baseline parameters, including diagnosis leading to NMS.
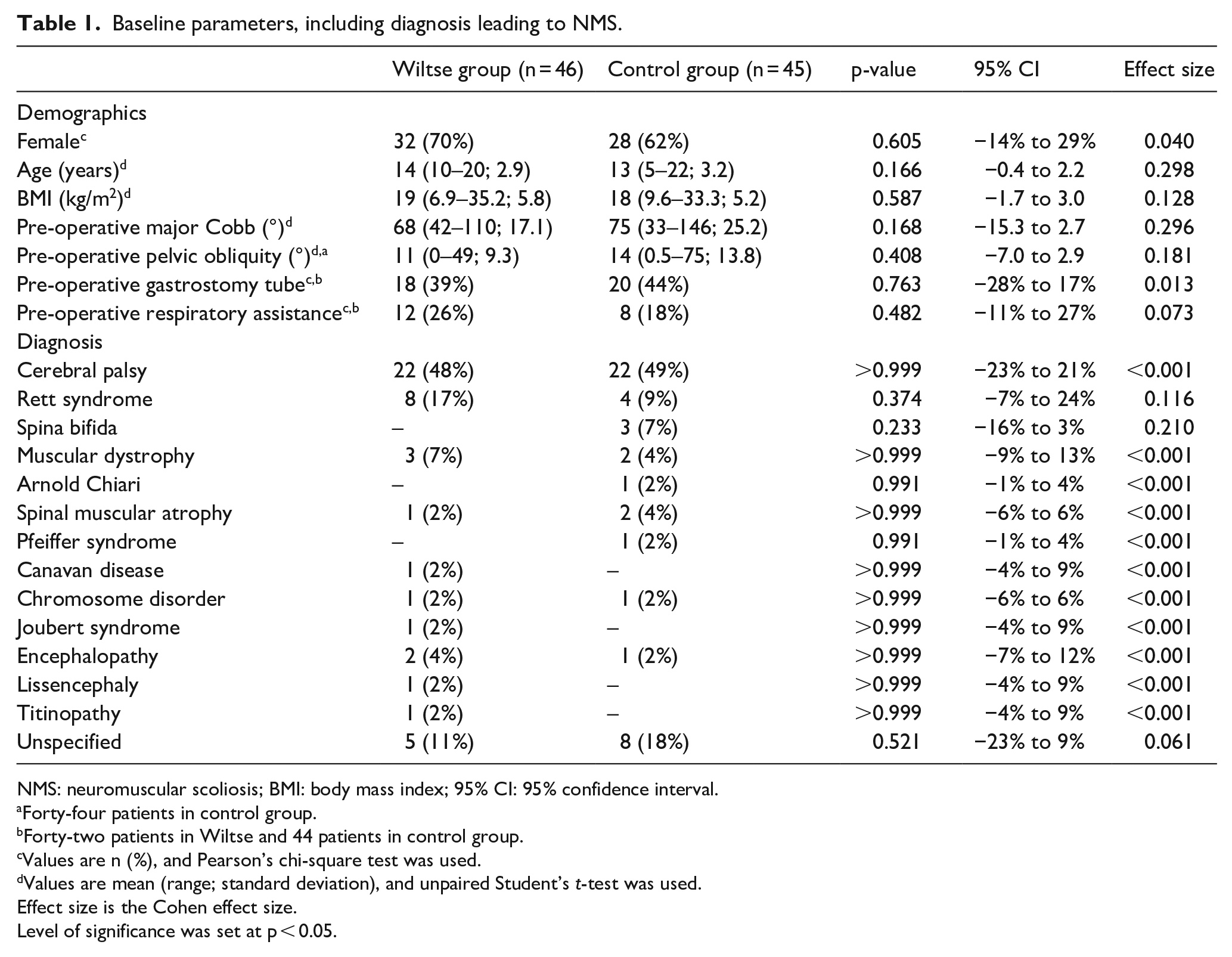
NMS: neuromuscular scoliosis; BMI: body mass index; 95% CI: 95% confidence interval.
Forty-four patients in control group.
Forty-two patients in Wiltse and 44 patients in control group.
Values are n (%), and Pearson’s chi-square test was used.
Values are mean (range; standard deviation), and unpaired Student’s t-test was used.
Effect size is the Cohen effect size.
Level of significance was set at p < 0.05.
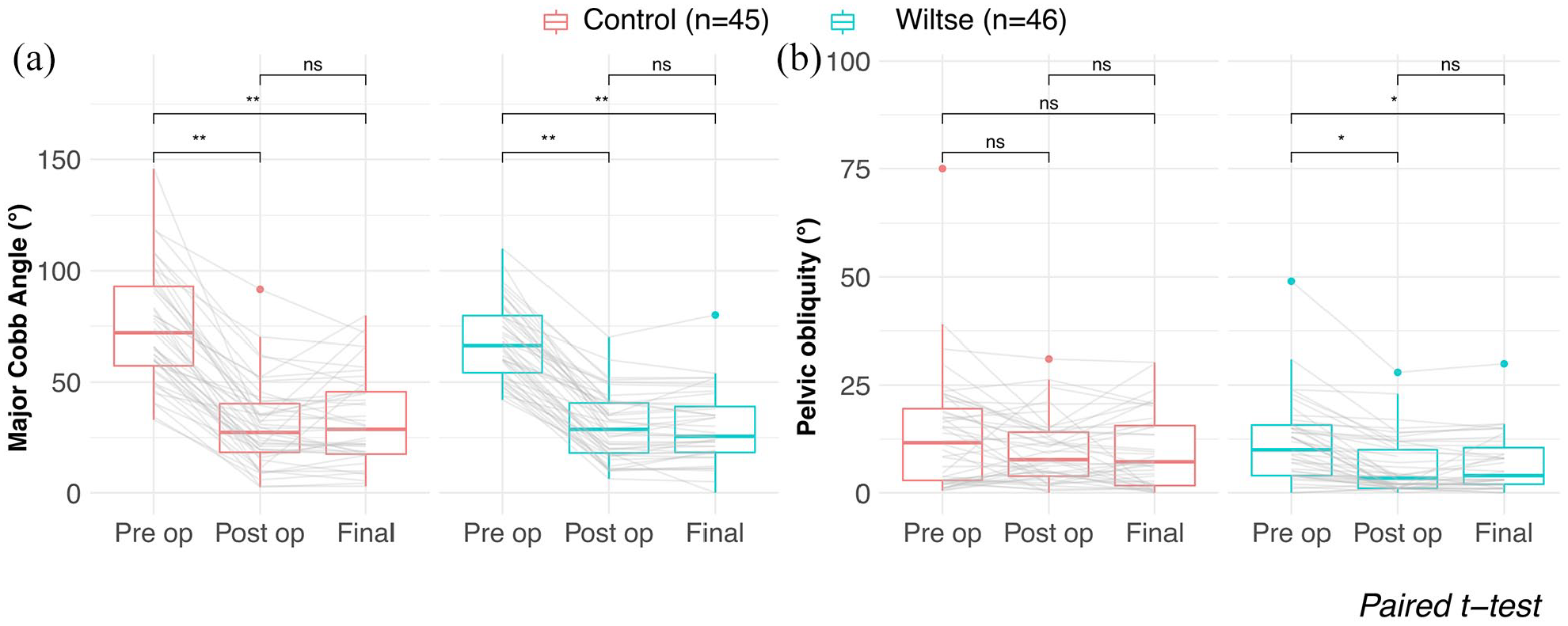
(a) Comparison of pre-operative (Pre op) with initial (Post op) and final post-operative (Final) major curve, respectively, pelvic obliquity in Wiltse and control cases (mean FU 3.3 vs 4 years in Wiltse respectively control cases). (b) Wiltse patients were operated using a paraspinal muscle approach. Controls were operated through a posterior midline approach. Paired Student’s t-tests were used. Thick lines represent median values, squares represent interquartile range (25th to 75th percentile), vertical lines represent ranges at most 1.5 × Interquartile range and dots represent outliers. “ns” means no statistical significant difference..
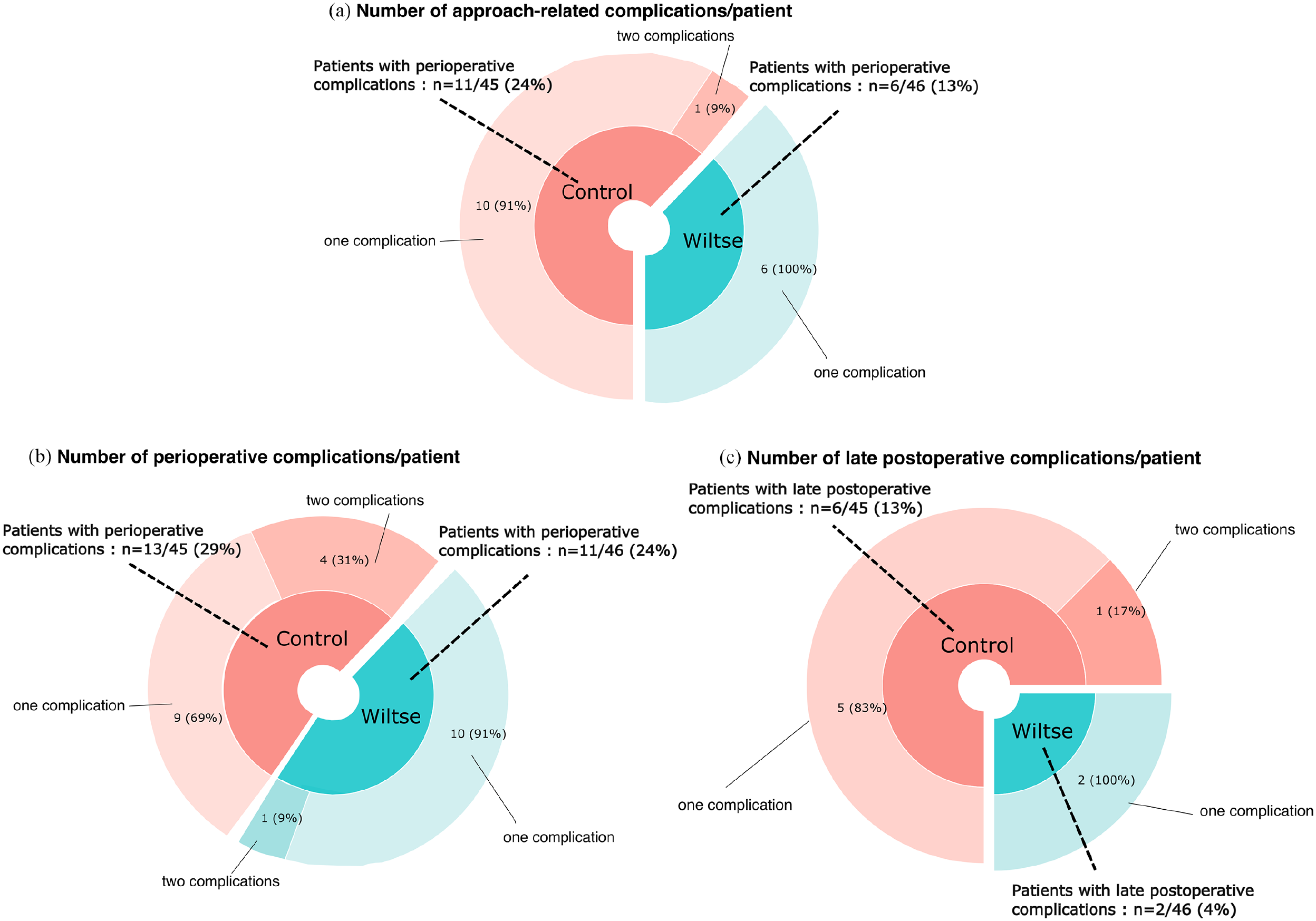
(a) Comparison of perioperative approach–related complication rates by groups. (b) Comparison of perioperative complication rates (any type) by groups. (c) Comparison of late complication (>30 days until final FU) rates by groups. Wiltse patients were operated using a paraspinal muscle approach. Controls were operated through a posterior midline approach.
Surgical variables and approach-related perioperative complications by group, with additional subgroup comparison (with vs without pelvic fixation).
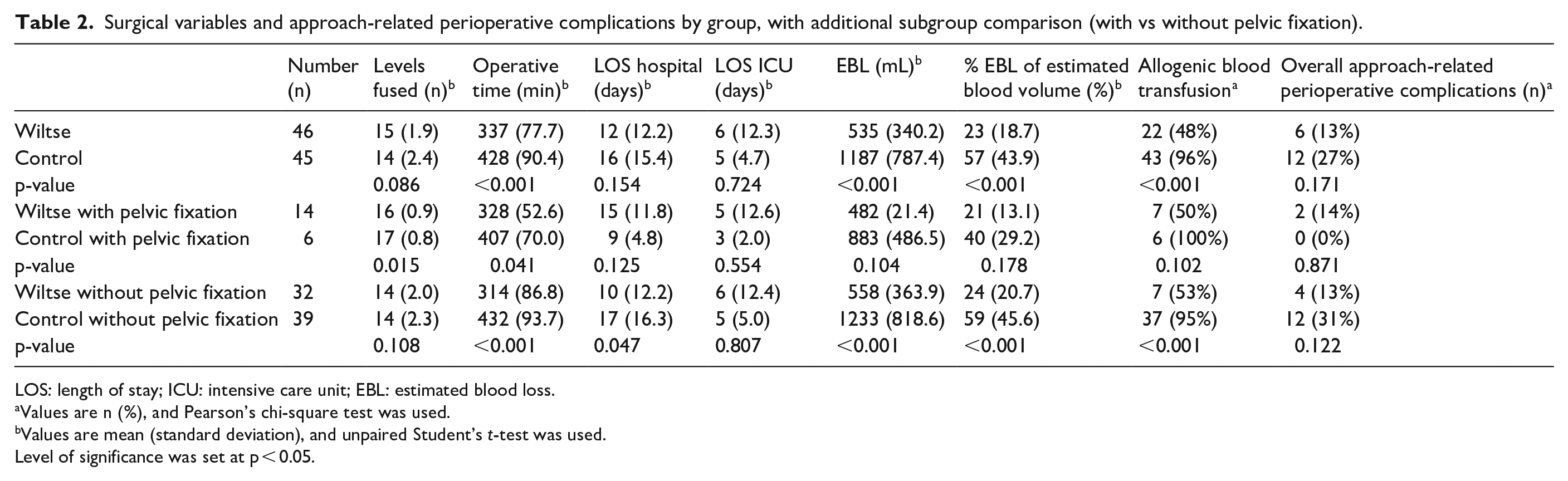
LOS: length of stay; ICU: intensive care unit; EBL: estimated blood loss.
Values are n (%), and Pearson’s chi-square test was used.
Values are mean (standard deviation), and unpaired Student’s t-test was used.
Level of significance was set at p < 0.05.
Discussion
Consistent with our hypothesis, the Wiltse and the control group achieved comparable mean initial and final post-operative major curve and pelvic obliquity corrections. The mortality rate and the intraoperative, perioperative (global and approach-related), and late complication rates were not differing significantly between both groups. Compared to the Controls, Wiltse cases had a lower EBL, percentage of EBL of estimated blood volume and allogenic transfusion rate when considering all patients (46 Wiltse and 45 Controls), respectively, selectively the cases without pelvic fixation (32 Wiltse and 39 Controls).
The mean initial major curve correction of Wiltse and control patients was equivalent for both groups, lasted at final FU and fell within the range of correction (i.e. 49%–74%) reported in the literature for NMS patients using all pedicle screw constructs and a posterior midline approach.17–20 Both groups achieved an equivalent initial pelvic obliquity correction which persisted at final FU and was comparable to the mean pelvic obliquity correction of 56% or 5.2° reported by Modi et al., 18 using a posterior midline approach.
The intraoperative complication rate was similar for both approaches (Table 3). However, more serious complications occurred in the posterior midline approach group. Indeed, two control, respectively no Wiltse patients experienced an intraoperative hemorrhagic shock. This finding cannot be attributed to variations in tranexamic acid use or in nutritional status as tranexamic acid was always used, and the mean BMI as well as the pre-operative gastrostomy tube presence rate were comparable in both groups. It neither can be attributed to pelvic fixation, as both concerned cases had none. Therefore, and because the control group had a higher EBL, we assume that the hemorrhagic shock occurrence in the two control patients was associated with the extensive wound surface created using the posterior midline approach. Mortality rate, perioperative, and late complication rates were not differing significantly in Wiltse cases in comparison to Controls (Table 3). This was also the case for approach-related perioperative complications, despite Wiltse cases had tendentially less complications of this type than Controls (6 vs 12 cases or 13% vs 27%). As opioid consumption was decreased in the paraspinal approach group of a study comparing this approach to the midline approach for AIS patients, we included per analogy non-infectious respiratory complications, ileus, and abdominal compartment syndromes which all are associated with opioid use in the approach-related complications. 7 We also included surgical site infection and wound dehiscence in this entity, as these might be related to the extent of the wound surface. The published perioperative complication rates for NMS surgeries are usually quite high. Complications in NMS can be considered as disease or procedure related. Thus, pre-existing or disease-related factors like pulmonary compromise, urinary incontinence, poor nutrition and other co-morbidities increase the chance of complications. We cannot exclude that some disease-related factors could have influenced our complication rates. However, our results are strengthened by the comparable rates of pre-operative respiratory assistance and pre-operative gastrostomy tube presence and a similar mean BMI among both groups. Surgery-related complications result from increased blood loss, longer ORT, and extensive tissue dissection due to curve severity and pelvic fixation. Rumalla et al. 21 queried the “Nationwide Inpatient Sample” database from 2002 to 2011 and reported an overall complication rate of 40.1% and a respiratory complication rate of 28.2%. Mohamad et al. 22 reviewed 175 NMS patients and reported an overall perioperative complication rate of 33.1%. Toll et al. 17 retrospectively reviewed 102 consecutive NMS surgery patients between January 2008 and December 2016 with a minimum of 6 months FU. They reported a perioperative complication rate of 27% (81.1% major vs 18.9% minor complications). Complications were predicted by multiple factors including increased EBL (p = 0.012) and increased ORT (p = 0.046). Modi et al. 18 reported a perioperative complication rate of 27%, including 2 perioperative deaths (4% mortality) in a series of 52 patients operated using exclusively a posterior midline approach. Cognetti et al. 23 reviewed the voluntarily reported “SRS M&M” database, that included 29,019 NMS cases. The database collects mortality, return to operating room, paralysis, and surgical site infections as complications. Based on these variables, they reported an overall post-operative complication rate of 6.3%. When using this classification, this study found a complication rate of 0% for Wiltse and 4% for control patients.
Complications (intraoperative; perioperative (≤30 days) (global vs approach-related); late post-operative (>30 days)) and mortality.
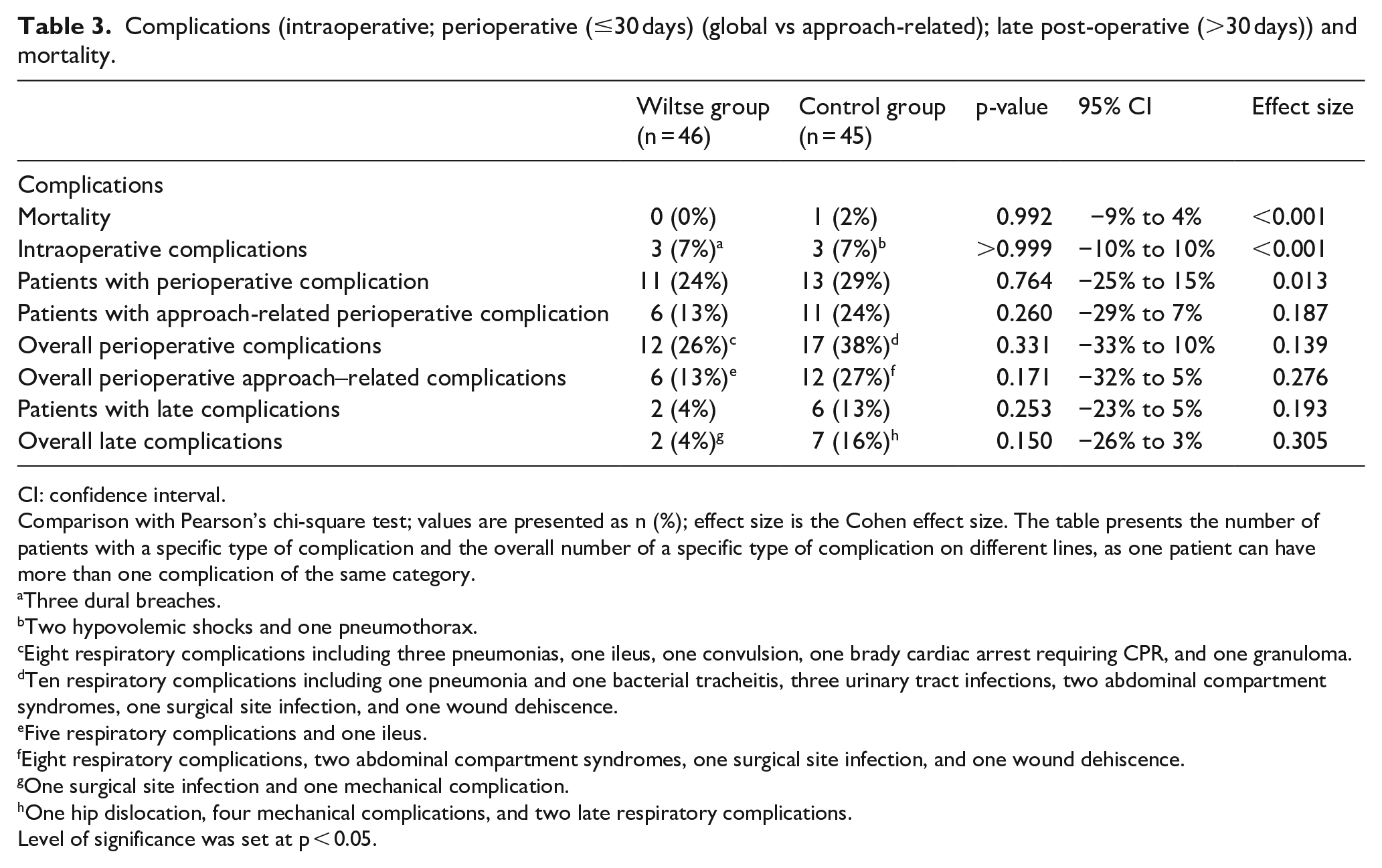
CI: confidence interval.
Comparison with Pearson’s chi-square test; values are presented as n (%); effect size is the Cohen effect size. The table presents the number of patients with a specific type of complication and the overall number of a specific type of complication on different lines, as one patient can have more than one complication of the same category.
Three dural breaches.
Two hypovolemic shocks and one pneumothorax.
Eight respiratory complications including three pneumonias, one ileus, one convulsion, one brady cardiac arrest requiring CPR, and one granuloma.
Ten respiratory complications including one pneumonia and one bacterial tracheitis, three urinary tract infections, two abdominal compartment syndromes, one surgical site infection, and one wound dehiscence.
Five respiratory complications and one ileus.
Eight respiratory complications, two abdominal compartment syndromes, one surgical site infection, and one wound dehiscence.
One surgical site infection and one mechanical complication.
One hip dislocation, four mechanical complications, and two late respiratory complications.
Level of significance was set at p < 0.05.
Wiltse patients experienced less EBL (535 vs 1187 mL) and lower allogenic transfusion rates (48% vs 96%) than controls considering all patients (n = 91), and when selecting those without pelvic fixation (n = 71 among 91) (558 vs 1233 mL respectively 53% vs 95%). When considering specifically the minority of patients with pelvic fixation (14 Wiltse among 46 and 6 Controls among 45), no statistical differences of EBL or transfusion rates were found according to the used approach. As Wiltse group globally had less EBL and lower transfusion rates despite holding a higher proportion of patients with pelvic fixation than the control group do (30% vs 13%), we might attribute the absence of significant differences in the subgroup with pelvic fixation to its small size (n = 20, holding 14 Wiltse and 6 Controls).
Edler et al. 24 retrospectively reviewed 163 pediatric patients for blood loss during posterior spinal fusion (PSF). They found that neuromuscular patients had an almost seven times higher risk (adjusted odds ratio = 6.9, p < 0.05) of losing >50% of their estimated total blood volume during scoliosis surgery. Modi et al. 25 reported a mean EBL of 3221 mL when performing standard PSF in NMS cases. McLeod et al. 26 retrospectively reviewed the “Pediatric Health Information Systems” database between 1 January 2006 and 30 September 2009; 2722 AIS and 1547 NMS procedures were analyzed for antifibrinolytics use and blood transfusions in US children’s hospitals. They reported the median hospital-specific rate of red cell transfusions; it was 43% for NMS and 24% for AIS. In NMS, antifibrinolytics use did not decrease the odds of transfusions. Recently, Kieser et al. 12 reported a mean EBL of 2439 mL versus 795 mL in their retrospective series comparing 8 NMS patients operated using the posterior midline approach with 16 NMS patients operated using a paraspinal muscle approach. It is the first retrospective study comparing the use of these two approaches for NMS patients.
Considering the high EBL and transfusion rates reported in the literature for NMS cases operated using a posterior midline approach, together with the comparative decrease of those parameters in Kieser’s and our results when using the posterior paraspinal approach, the latter approach might have an intrinsic positive effect on those parameters, especially if no pelvic fixation was done. This statement is consistent with several publications comparing both approaches for AIS correction which found an association between the paraspinal approach use and decreased EBL, respectively, transfusion rate.7,9,27 Possible explanations for the reduced EBL and transfusion rates observed when using the paraspinal muscle approach might be that it is an anatomic approach taking advantage of avascular intermuscular planes and especially of the space between the multifidus and the longissimus muscles in the lumbar spine and, second that the exposed bone area using subperiosteal dissection is reduced when compared to the midline approach. In our series, a part of the difference of blood loss seen in group comparison might also be due to the shorter ORT needed for Wiltse cases.
The ICU LOS was 6 versus 5 days for Wiltse respectively control cases (p-value = 0.724), which compares well with the ICU LOS of 4.7 days reported by Brooks et al., 28 using a posterior midline approach in their retrospective study including 324 NMS patients. The hospital LOS was globally equivalent for both approach groups (12 vs 16 days for Wiltse respectively Controls). Murphy et al., 29 respectively Barsdorf et al., 30 reported that NMS children had a 9.2 versus 10.3 days average hospital LOS. When considering specifically the subgroup without pelvic fixation (n = 71), the hospital LOS was significantly shorter in the Wiltse than in the control patients (10 vs 17 days, p = 0.047). A shorter hospital LOS for Wiltse cases was also reported in a retrospective study comparing AIS cases operated either using a Wiltse (n = 192) or a posterior midline approach (n = 293) (5 vs 4 days, p < 0.001). 7
This study has limitations. It has a retrospective design, 20% of the control cases were excluded due to lack of FU data, we did not report functional outcome, and the control patients were operated on in a larger time frame compared to Wiltse patients which might have influenced the amount of blood loss. This study also has strengths. It is the first report with a minimal FU of 2 years comparing NMS patients operated either using a Wiltse or a posterior midline approach. In addition, baseline parameters were comprehensively reported and did not differ significantly between both groups.
Conclusion
In conclusion, paraspinal muscle approach (Wiltse) use for NMS patients provided adequate initial and long-lasting deformity correction. Since in contrast to the control cases, no surgery-related severe intraoperative complications occurred in Wiltse cases, the latter approach might be safer. Moreover, the Wiltse approach was globally and for the subgroup without pelvic fixation associated with a reduced EBL and a lower allogenic transfusion rate. Finally, it was associated with a shorter hospital LOS in the subgroup without pelvic fixation. These potential benefits still need to be evaluated with further FU of larger cohorts.
Footnotes
Author contributions
A.A. contributed to the study design, data collection, and manuscript preparation. J.G. contributed to the data collection, manuscript validation. S.H. contributed to the data collection and manuscript validation. A.T.-F. contributed to the study design, statistical analysis and interpretation, and manuscript validation. S.W. contributed to the data collection and manuscript validation. T.A. contributed to the data collection and manuscript validation. V.S. contributed to the data collection and manuscript validation. R.D. conceived and coordinated the study, data collection, and manuscript validation. All authors have read the final version of the manuscript and approved it for submission.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.D. received grants and personal fees from DePuy Synthes Spine and Medtronic outside of the present work, and V.S. received personal fees from Precision Spine outside the present work. The other authors have no conflict of interest to declare.
Ethical approval
This article does not contain any trial with human participants or animals performed by any of the authors. The study had institutional ethical approval (CCER 15152).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Due to retrospective nature of the research, no informed consent was requested by the ethical committee.