
Abstract
Purpose:
Serial casting is an effective treatment for infantile idiopathic scoliosis. The most common casting table types are Mehta, Risser, and spica tables. We compared major curve correction between patients with infantile idiopathic scoliosis treated using pediatric hip spica tables versus Risser or Mehta tables.
Methods:
In this multicenter retrospective study, we included 52 children younger than 3 years (mean ± standard deviation age, 1.6 ± 0.68 years) treated with ≥2 consecutive casts for infantile idiopathic scoliosis between September 2011 and July 2018. We compared major curve angle (measured using the Cobb method) before and after treatment and improvement in curve angle between the spica tables group (n = 12) and the Risser or Mehta tables group (n = 40). The primary outcome was the difference in percentage correction of the major curve according to radiographs taken after first casting and at final follow-up.
Results:
The mean major curve was 47° ± 18° before casting. A median of six casts (range: 2–14) were applied. Mean follow-up after treatment initiation was 22 months (range: 7–86 months). At baseline, the major curve was significantly larger in the spica tables group (58°) than in the Risser or Mehta tables group (43°) (p = 0.01). We found no differences in the percentage curve correction in the spica tables group versus Risser or Mehta tables group after first casting or at final follow-up.
Conclusion:
Serial casting was associated with substantial major curve correction in patients with infantile idiopathic scoliosis. Curve correction did not differ between patients treated with a spica table versus a Risser or Mehta table.
Level of Evidence:
Level III, retrospective cohort study
Keywords
Introduction
Infantile idiopathic scoliosis (IIS) is a >10° curvature of the spine that occurs in patients younger than 3 years. 1 Patients with IIS account for approximately 1% of all patients with idiopathic scoliosis.2,3 For many patients, IIS resolves spontaneously, and thus observation is indicated for most patients. 4 Findings that indicate an increased risk of developing progressive IIS necessitating treatment include a rib vertebral angle difference >20° and a curvature >30°. Left untreated, progressive IIS can cause severe disfigurement and lung restriction. 5 In 1955, Scott and Morgan 6 reported that 4 of 28 patients with progressive IIS died before age 20 from cardiopulmonary disease.
Treatments such as bracing, casting, and spinal arthrodesis aim to control deformity progression. 7 In certain cases of progressive IIS, surgical treatment with growth-friendly systems has become the preferred treatment for deformity correction. 8 However, high complication rates among young patients have driven a desire to delay or avoid surgery. 9 Serial cast application has shown excellent results in controlling curve progression and even resolving IIS. 10 Casting influences the shape of the spine by applying forces of derotation, extension, and flexion during periods of rapid growth. 11 Serial casting is most commonly performed on a Risser, Mehta, or spica casting table. Risser and Mehta tables are dedicated to the sole purpose of scoliosis casting.10–12 However, these large tables require ample space and may not be cost-effective for some hospitals because the incidence of IIS is low. Furthermore, the Risser frame can be too large for an infant’s body. The pediatric hip spica table (ST), in contrast, has a wide range of uses and offers additional advantages, including portability and ease of use and setup. To our knowledge, no studies have assessed differences in IIS outcomes among the three table types. We hypothesized that patients who underwent casting on a Risser or Mehta table (RMT group) would experience greater major curve correction than those who underwent casting on a ST (ST group).
Materials and methods
Institutional review board approval was obtained from all participating centers before study initiation.
Patient selection
We retrospectively reviewed an international multicenter registry with data representing 72 centers in 11 countries. We included patients with IIS who were younger than 3 years and who were treated with at least two casts from September 2011 to July 2018. All patients requiring cast application were considered to have progressive forms of IIS. We excluded patients whose scoliosis was caused by neuromuscular, syndromic, or congenital conditions; those who had undergone previous spine surgery; and those who had been casted with more than one table type.
Patients in both groups underwent serial casting with general anesthesia. The longitudinal traction was applied manually (ST), 13 with skin traction (Mehta), or with head halter–pelvic traction (Risser). Longitudinal support for the back was provided by the retractable piece in the ST, the hammock strap in the Risser table, or the cloth strap in the Mehta table. 14 The ST was placed at slight Trendelenburg angle to provide counter-traction. Elongation, derotation at the apex, and flexion were applied. Relief areas at the apical concavity were created as described by Mehta. 10 Casts, which were made from fiberglass in all centers, were changed every 6–10 weeks, depending on patient age and growth, and typically did not include the shoulders or neck. The only major structural difference between the tables is the presence of a mirror in the Mehta table, which is used for hand visualization and placement of the mold. 14 Essentially, cast application technique was similar for all three tables.
Patient characteristics
We included 52 patients with IIS (12 in the ST group and 40 in the RMT group). Mean (±standard deviation) age was 1.6 ± 0.68 years, and mean major curve was 47° ± 18° before initiation of casting (Table 1).
Characteristics of 52 patients who underwent casting for scoliosis, by casting table type and time point.
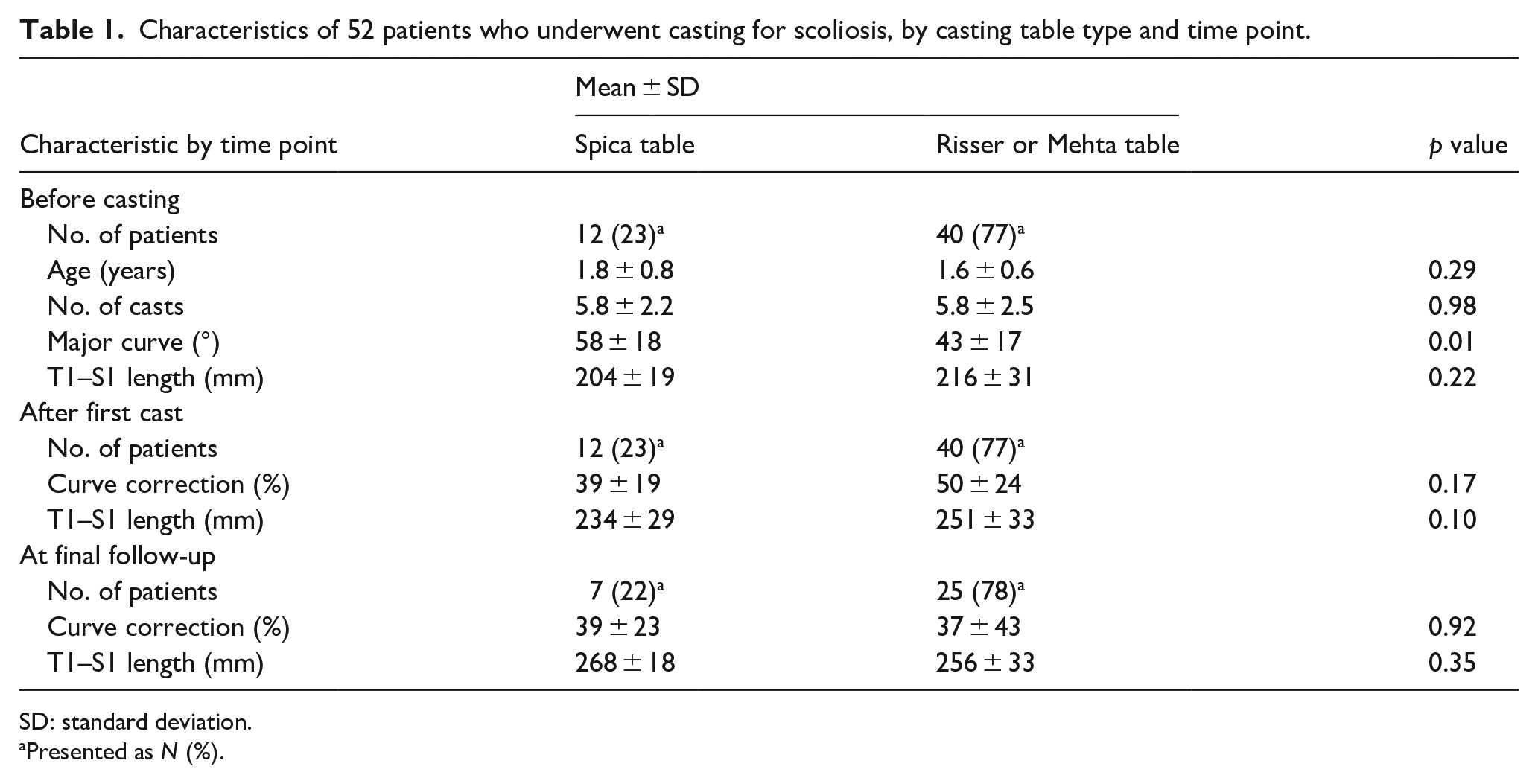
SD: standard deviation.
Presented as N (%).
Treatment variables
Of the 40 patients in the RMT group, 30 were treated using a Mehta table and 10 using a Risser table. Mean follow-up time after initiation of casting for all patients was 22 months (range: 7–86), with a median of six serial casts (range: 2–14) applied to 38 (73%) thoracic curves, 13 (25%) thoracolumbar curves, and 1 (2%) proximal curve.
Radiographic assessment
Anteroposterior and lateral spine radiographs were taken before initial casting, after first casting, and after every subsequent casting. Thirty-two patients had radiographic data available from the final follow-up visit. Trained study coordinators at each participating center used the Cobb method to measure the angle of the major curve. 15 The same examiners measured spine length, which was defined as distance between the T1 and S1 segments. The outcomes of interest were improvement in curve magnitude after first casting (defined as improvement of at least 20°) and the percentages of curve correction achieved after the first casting and after the final casting. Percentage curve correction was calculated as follows:

Statistical analysis
Categorical variables are described as frequency (percentage) and continuous variables as mean ± standard deviation unless otherwise specified. Chi-square tests were used to assess differences in the proportions of infants experiencing successful improvement in curve magnitude between the two groups. The Shapiro–Wilk test and the homogeneity of variances by Levene’s test were used to assess normality of data. The Mann–Whitney U test was used to evaluate differences in curve magnitude between the two groups. Statistical analysis was conducted using SAS, version 9.4, software (SAS Institute, Cary, NC, USA). Significance was set at p < 0.05.
Results
Overall, the mean major curve improved significantly after the first casting (mean improvement: 22° ± 13°) and after the final casting (mean improvement: 20° ± 17° (both, p < 0.001).
There were no significant differences in the mean age of patients, T1–S1 length at baseline, or number of casts applied between the two groups (Table 1). Patients in the ST group had a significantly larger mean curve (58° ± 18°) than those in the RMT group (43° ± 17°) (p = 0.01).
After the first cast application, the mean percentage curve correction in the ST group (39% ± 19%) did not differ significantly from that of the RMT group (50% ± 24%) (p = 0.17). Similarly, at final follow-up, mean curve correction did not differ significantly between the ST group (39% ± 23%) and the RMT group (37% ± 43%) (p = 0.92) (Figure 1).
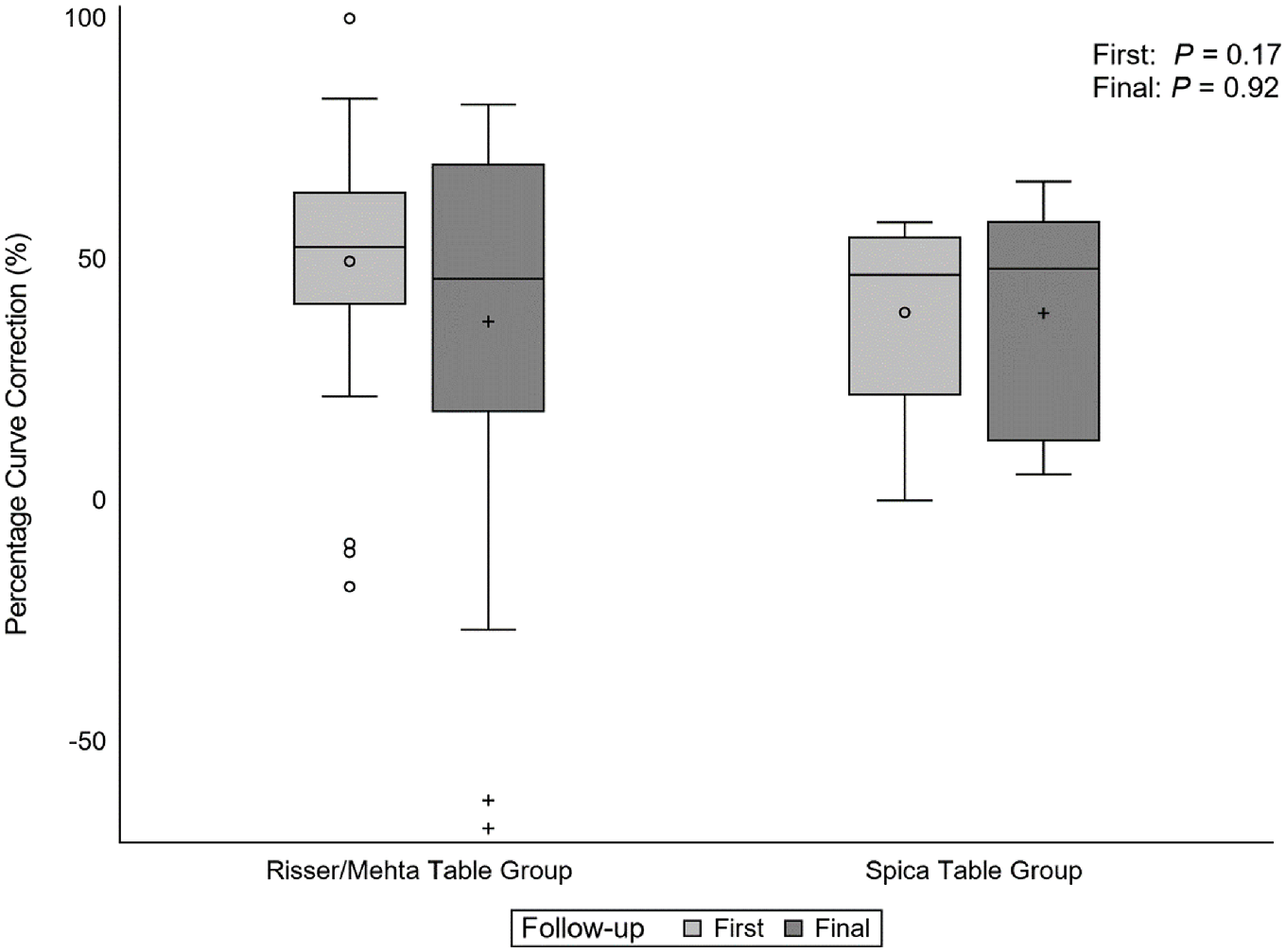
Difference in percentage curve correction after first casting (“First”) and at final follow-up (“Final”) between patients with idiopathic infantile scoliosis treated using a spica table (First, n = 12; Final, n = 7) or a Risser or Mehta table (First, n = 40; Final, n = 25). Circles = outliers; crosses = means; horizontal lines within boxes = medians; error bars = minimum and maximum values.
Mean spine length was similar between the ST group and RMT group after the first casting (234 ± 29 mm vs 251 ± 33 mm, p = 0.10) and at final follow-up (269 ± 18 mm vs 256 ± 33 mm, p = 0.35).
We found no significant difference in the proportion of infants who experienced improvement in curve magnitude between those in the ST group (67%) and those in the RMT group (55%) (p = 0.4).
Seven patients had cast-related complication (abrasion or irritation in six patients; respiratory distress caused by inability to maintain the airway during casting in one patient with asthma). The rates of cast-related complications did not differ between the ST and RMT groups (p = 0.33).
Discussion
We found no significant difference in the magnitude of curve correction achieved between patients with IIS who underwent serial casting using an ST versus an RMT. Although this result negates our hypothesis, it is unsurprising given that the tables all provide longitudinal traction while leaving the trunk free for cast application and have only slight differences in design.
Gomez et al. 16 investigated the predictive value of percentage curve correction after initial casting on the final Cobb angle of the major curve at final follow-up. They found that in 68 patients with IIS, the mean curve improved from 46° pre-casting to 23° after initial Mehta casting, for a mean 50% correction. After initial cast application, major curves in patients whose curves ultimately resolved continued to improve by a mean of 35% from initial casting to final follow-up at a mean of 2.5 years. 16 The authors did not adjust or stratify their data according to table type; however, our analysis shows that correction after first casting was similar to that reported by Gomez et al., 16 of 49% for the RMT group and 39% for the ST group. Smith et al. 17 compared the percentage curve correction achieved with bracing, casting, or vertical expandable prosthetic titanium rib for IIS. For the casting cohort, they used Mehta’s casting technique (table type not specified) and achieved initial curve correction of 43% and final correction of 59%. 17 Our results are also consistent with those of Iorio et al., 11 who showed a 51% correction in patients who responded to serial casting (defined as >10° of improvement during course of treatment). 11
Fedorak et al. 18 analyzed the results of serial casting at a minimum 5-year follow-up to identify predictors of sustained success in children who achieved >20° of improvement or reached a major curve of < 15°. In their sample of 38 patients, 73% had successful improvement. In our study, 67% of patients in the ST group and 55% in the RMT group reached this threshold of successful improvement, a > 20° improvement in major curve. Although our proportions are slightly lower, longer follow-up may show continued improvement in scoliosis as children grow. Furthermore, the similar proportions of patients who were considered to have successful correction between the ST group and RMT group in our study and the patients who were Mehta casted in the study by Fedorak et al. show no difference in curve correction between the table types and suggest that this finding may persist during longer follow-up.
Strengths of this study include our use of a multicenter database allowing for a large sample of patients with IIS. Initiation of casting before age 19 months in patients with curves <60° provides the best chance for successful correction.5,19,20 The mean age of patients in our study was 1.6 years, with a mean major curve of 47° at initial casting. This is well within the limits predicted by previous studies for a good response to serial casting, allowing comparison among table types by limiting the number of confounders that may affect the percentage of curve correction. To our knowledge, this is the first study to compare casting table types by IIS outcomes. Patients in this study were treated by different surgeons with different casting practices in their centers, as seen by the wide range in number of cast applications. Thus, there is an inherent bias when comparing tables because certain centers and surgeons use a specific table type. There was an unequal distribution of patients casted with each table type. Furthermore, at baseline, the ST group had a significantly larger mean curve than the RMT group; therefore, absolute curve size could not be compared at first and final casting. In addition, details regarding how the cast was tailored to each curve were not present in the database. However, regardless of the table type used, the casting technique is similar, with an emphasis on longitudinal traction and molding. Although the mean duration of follow-up for this study was 20 months, which is similar to that of previous studies,16,20 longer follow-up is necessary to determine differences in outcomes, particularly the need for further intervention and how patients’ overall quality of life and functional abilities may differ after they reach skeletal maturity.
In conclusion, serial casting resulted in significant correction of the major curve in patients with IIS. We found no differences in curve correction by casting table type. Our findings are particularly important for treatment centers that do not have access to or are unable to store a Mehta or Risser table because of space constraints. The ST can achieve similar results with the advantages of being versatile and easy to store.
Footnotes
Acknowledgements
The authors thank Rachel Box MS, ELS, in the Editorial Services group of the Department of Orthopaedic Surgery, The Johns Hopkins University, for editorial support.
Author contributions
All authors were involved in the drafting and critical revision of the manuscript and provided final approval. Other author contributions are as follows: M.M. (study design, data acquisition, analysis and interpretation); N.P. (data acquisition); G.H.T. (study design, data acquisition, analysis); Y.L. (data acquisition); M.G. (data acquisition), and P.D.S. (study design, data acquisition, analysis, and interpretation).
Compliance with ethical standards
The study was performed in compliance with the Declaration of Helsinki, and institutional review board approval was obtained from each center before initiation of the study. Parents/caregivers of study participants provided informed consent.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.G. reports consultant/teaching for Nuvasive, stock ownership/consulting fees for Orthobullets, teaching for Depuy Synthes, membership in PSSG/HSG. Y.L. is a member of Scoliosis Research Society and the advisory board of Medtronic, and reports travel from Zimmer Biomet. P.D.S. reports consulting for Nuvasive, royalties from Globus, and consulting for DePuy. G.H.T. reports royalties from OrthoPediatrics, salary from Wolters Kluwer, salary from Shriners Hospitals for Children, honorarium from Broadwater, consulting for OrthoPediatrics, travel from Scoliosis Research Society, and is an officer in Growing Spine Foundation and Pediatric Spine Study Group.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.