
Abstract
Purpose:
Blount disease is most common among obese Black children. The reason for Blount’s racial predisposition is unclear. Given that obesity is a risk factor for Blount disease and the known associations between race, obesity, and socioeconomic status in the United States, we hypothesized that socioeconomic status and severity of obesity differ between Black and non-Black children with late-onset Blount disease. We additionally examined differences in treatment types between Black and non-Black children.
Methods:
One hundred twenty-five patients from two institutions were included. Age at presentation, age of onset, body mass index, race, sex, and treatment type were recorded. These variables were compared between Black and non-Black children. Insurance type and estimated household income were used as markers of socioeconomic status.
Results:
Of the 125 patients with late-onset Blount disease, body mass index percentiles were higher for Black patients (96th ± 12th percentile) than non-Black patients (89th ± 22nd percentile) (p = 0.04). Black patients also had lower estimated incomes (US$48,000 ± US$23,000 vs US$62,000 ± US$30,000) (p = 0.01) and much higher rates of Medicaid enrollment (69% vs 24%) (p < 0.01) than did non-Black patients. Regarding treatment types, osteotomy was more common among Black patients (60%) than non-Black patients (38%) (p = 0.033).
Conclusion:
The race-related associations we found between obesity and socioeconomic status suggest that non-genetic factors may contribute to observed racial differences in the prevalence of Blount disease.
Level of evidence:
level III.
Introduction
Blount disease is a progressive tibia vara of childhood caused by osteochondrosis of the proximal tibial physis. 1 Although Blount disease is frequently used to refer to a single entity, it is commonly divided into two or three distinct forms: early-onset and late-onset; or infantile, juvenile, and adolescent.2–4
The etiology of Blount disease is still elusive, with evidence for genetic, nutritional, environmental, and behavioral mechanisms at play. 5 Obesity and Black race are observed to be risk factors for both types of Blount disease, but while the mechanical effect of a high body mass on the tibial physis is clear,6–9 the reason for its racial predisposition is poorly understood.4,10–13 Past hypotheses have included racial differences in vitamin D status or joint laxity. 14 However, only one retrospective database study, representing 12 patients with Blount disease, has shown differences in vitamin D levels.5,15 A larger and more recent prospective study of 50 patients was unable to replicate these findings. 16 In addition, increased joint laxity in Black children has never been shown.10,17 Conversely, obesity is widely believed to be a strong risk factor for late-onset Blount disease, and evidence has demonstrated that Black children in the United States are 1.4 times more likely to be obese than are White children. 18 With Black children in the United States being three times more likely to live below the poverty line than White children, 19 and the known association between socioeconomic status and obesity, 20 socioeconomic status is questioned to play a role in the racial disparity of Blount disease. 19
In this study, we examined differences in demographic characteristics and socioeconomic status between Black and non-Black children with late-onset Blount disease. We hypothesized that Black children with late-onset Blount disease would have greater obesity and lower socioeconomic status than non-Black children with late-onset Blount disease. We additionally examined the rates of operative treatment in this population.
Methods
Institutional review board approval and a waiver of consent were obtained. Hospital records of two large tertiary care centers were used to identify all children diagnosed with Blount disease at either institution from 2006 to 2017. Patients were included only if an orthopedic surgeon had documented the diagnosis of Blount disease. This criterion excluded patients with congenital tibia vara, physiologic varus, or a pre-existing physeal bar. Retrospective review was performed to assess age at presentation, age of first bowing, laterality, body mass index (BMI) within 6 months of presentation, race, zip code, insurance type, and treatment type. Patients’ races were obtained from the electronic medical record. Owing to lower numbers of non-Black patients, “Black” and “non-Black” were compared for the purpose of analysis, similar to a prior study. 21 BMI percentiles based on patients’ ages were determined using the Centers for Disease Control calculator.22–24
We included patients with late-onset disease only. Late-onset disease was defined as bowing at ≥4 years. Further subdivision into juvenile (ages 4–10 years) and adolescent (age >10 years) forms was not done, so as to preserve sample size and since this distinction has not gained widespread use.4,25 Insurance type and estimated median household income were used as indicators of socioeconomic status, consistent with other studies.26–28 Insurance was coded as Medicaid or non-Medicaid. Household income was estimated by comparing zip codes to 2016 inflation-adjusted census data. Student’s t test was used for continuous data, and Chi-square or Fisher’s exact tests were used for categorical data. Significance was defined as p < 0.05. Figure was designed on Microsoft Excel 2018 release (Microsoft Corporation, Redmond, WA, USA).
Results
The initial query returned 339 unique patients, of whom 156 were excluded for having a diagnosis different than Blount disease and 7 were excluded due to missing data. Of the 176 patients with confirmed Blount disease, 51 (29%) were categorized as early-onset and excluded, leaving 125 patients with late-onset Blount’s disease for analysis (Table 1).
Characteristics of 125 patients with late-onset Blount disease, 2006–2017.
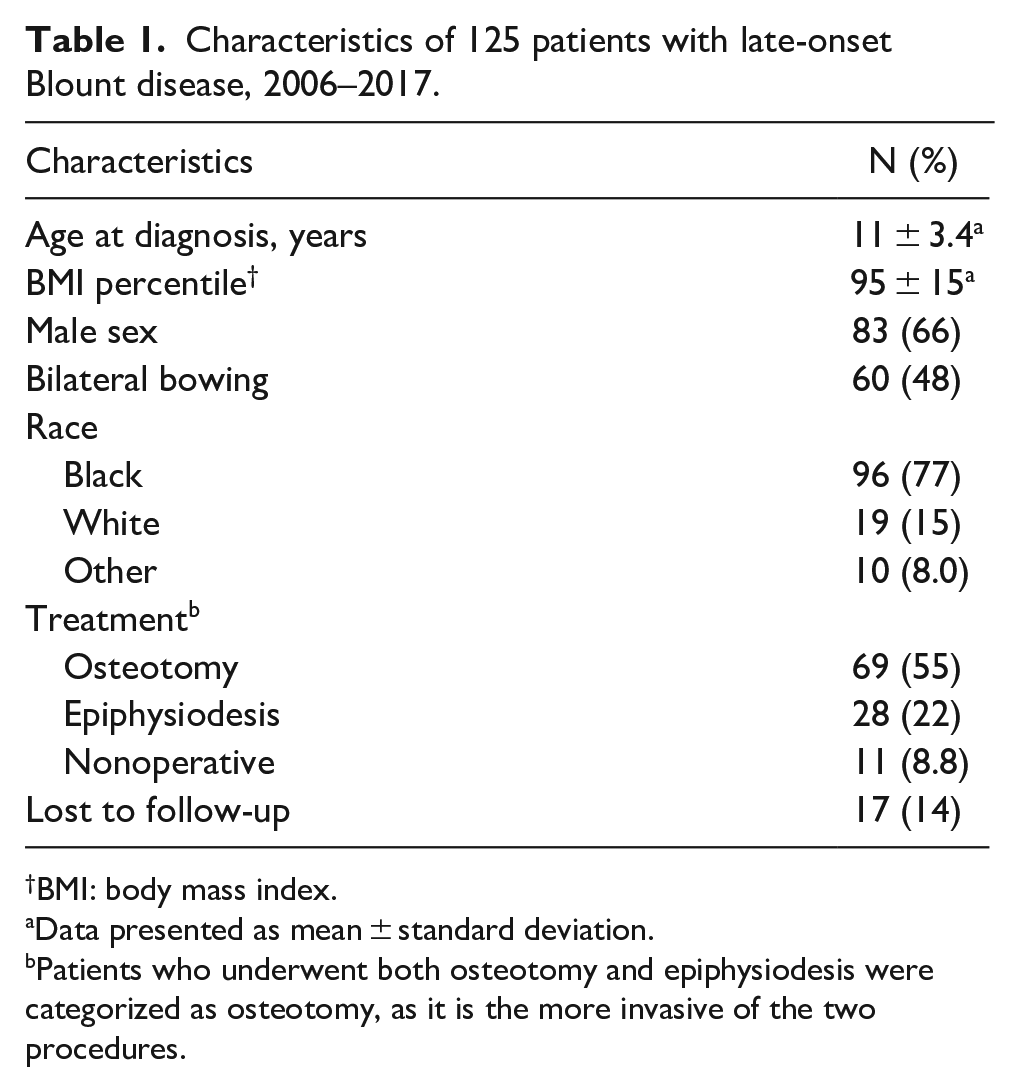
BMI: body mass index.
Data presented as mean ± standard deviation.
Patients who underwent both osteotomy and epiphysiodesis were categorized as osteotomy, as it is the more invasive of the two procedures.
Race-associated differences in obesity and socioeconomic status
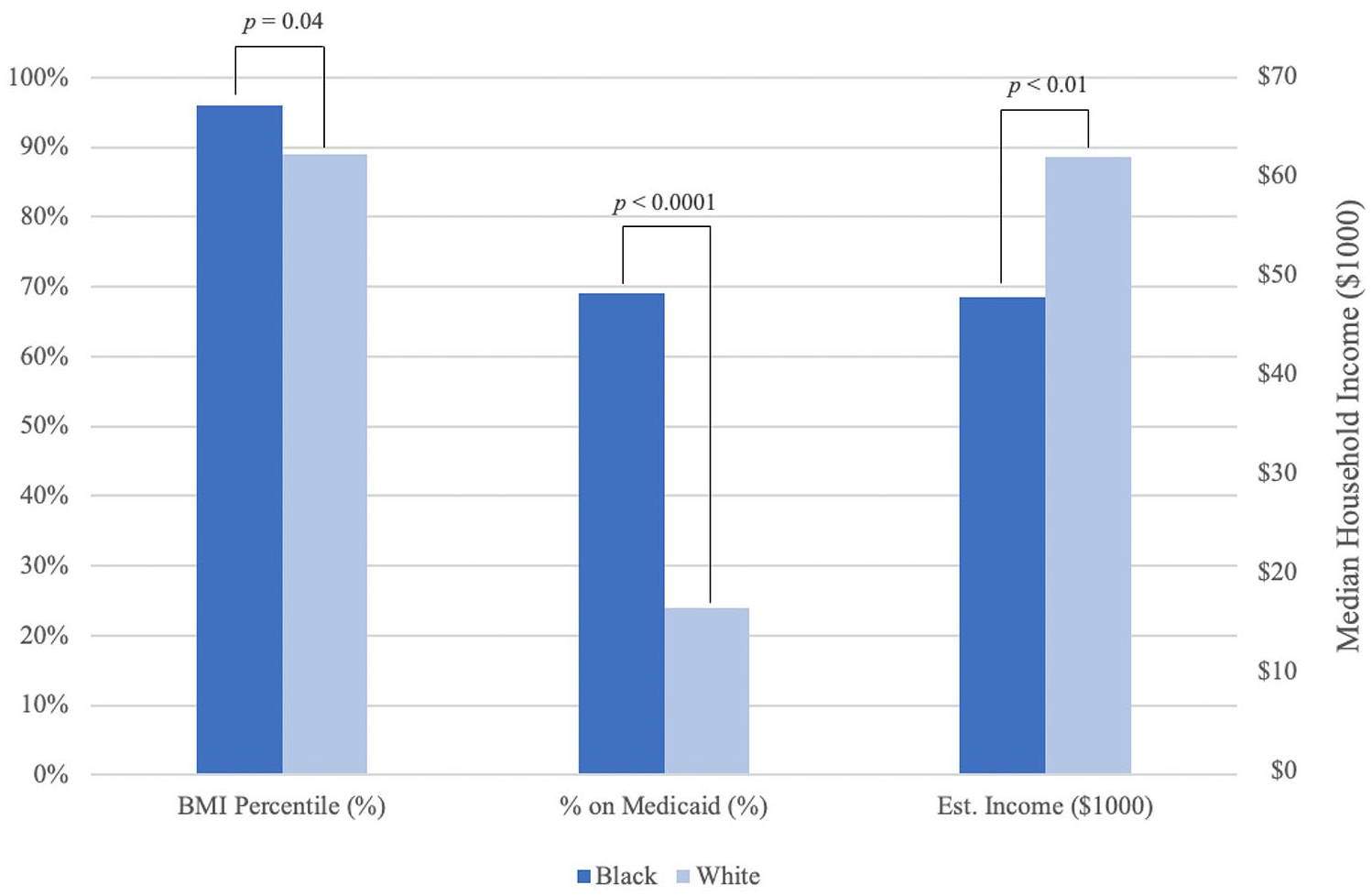
Black patients had significantly higher mean BMI values (expressed as kg/m2) (37 ± 11 vs 32 ± 9, p = 0.03) and BMI percentiles (96th ± 12th percentile vs 89th ± 22nd percentile, p = 0.04) than non-Black patients (Table 2). Black patients also had significantly lower mean estimated household incomes (US$48,000 ± US$23,000 vs US$62,000 ± US$30,000; p = 0.01) and three times higher incidence of Medicaid enrollment (69% vs 24%, p < 0.01) than non-Black patients with late-onset disease (Figure 1).
Characteristics of 125 patients with late-onset Blount’s disease by race.
Characteristics of 125 patients with late-onset Blount disease by race.
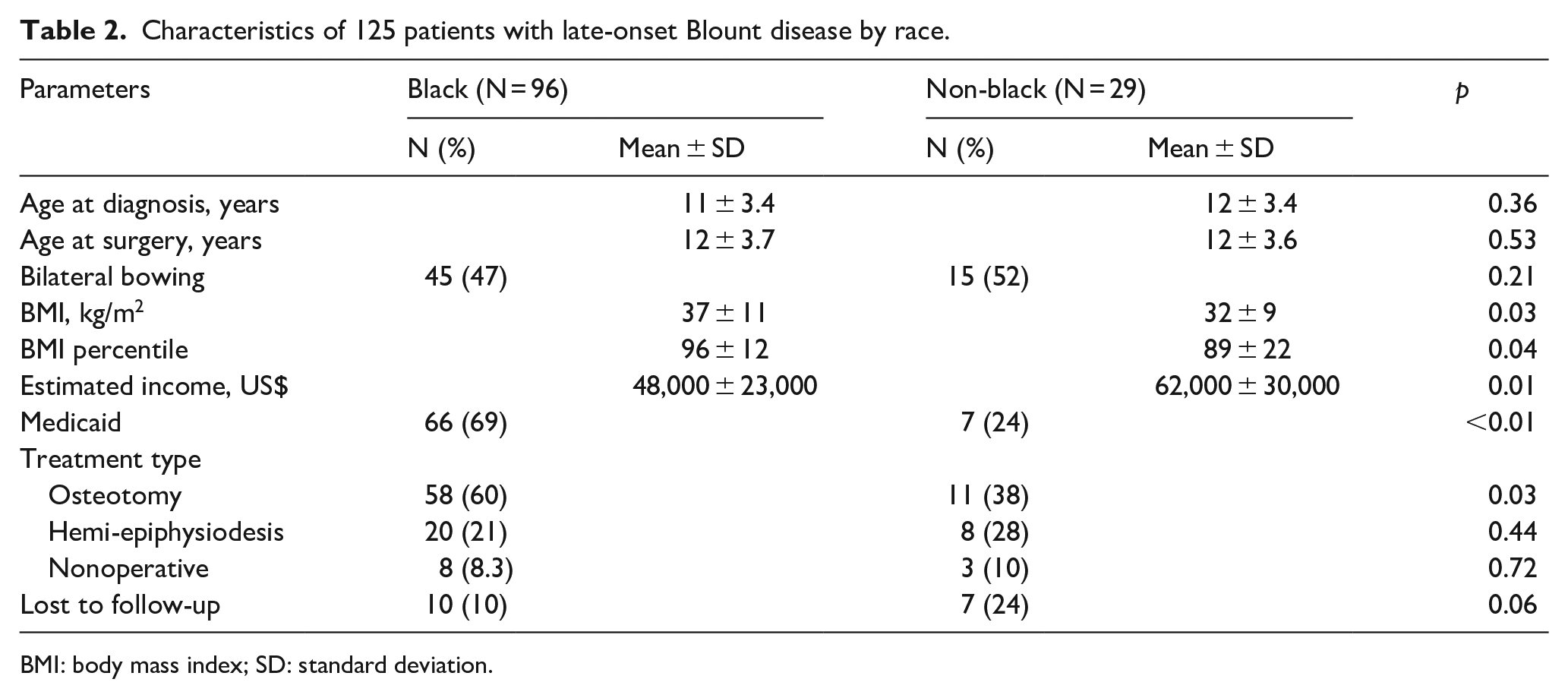
BMI: body mass index; SD: standard deviation.
Race-associated differences in treatment type
In total, 77% of late-onset patients underwent surgery (Table 1). Surgeries performed were osteotomies or hemi-epiphysiodeses. There was no significant difference in mean age at surgery between Black and non-Black patients (p = 0.53). There was no significant difference in the rate of all surgeries between Black and non-Black patients (p = 0.55). However, Black patients with late-onset disease were significantly more likely to undergo osteotomy than were non-Black patients (60% vs 38%, p = 0.03). There was no significant difference by race in the proportion of patients lost to follow-up, although the difference came close to significance (24% of non-Black patients vs 10% of Black patients; p = 0.06).
Discussion
This is the first study to examine the role of socioeconomic status in the racial predilection of Blount disease. Black patients with late-onset Blount disease have substantially lower household incomes and are more likely to be enrolled in Medicaid than non-Black patients. Considered together, these markers point to an overall difference in socioeconomic status between Black and non-Black patients presenting with late-onset Blount disease. Although the association of race with socioeconomic status and childhood obesity in the United States is well-known,18–20 these interrelationships have not previously been considered with regard to the racial disparity of Blount disease. To best test this hypothesis, we would have to correlate race with Blount’s disease, controlling for BMI, which our study is not designed to do. This is potentially an area for future study.
Prior literature has persuasively demonstrated the effect of high body mass in compressing the tibial physis, showing that regardless of age of onset, obese children with Blount disease had more severe deformity 11 and required surgery at higher rates 9 than non-obese children with Blount disease. The very high body mass percentiles and high rates of surgery found here are consistent with those findings. Black patients in this sample had significantly higher BMIs and BMI percentiles than non-Black patients. This points to a possibility of complex interplay between socioeconomic status, disease severity, and BMI. A socioeconomic gap may contribute to the disparity in obesity, with high BMI leading to more severe disease, but also an increase in BMI resulting from the pain and reduced activity in children with more severe disease. It is important to note, however, that the difference in BMI percentile found may be of questionable clinical significance (96 ± 12 in Blacks vs 89 ± 22 in non-Blacks).
We also found that the rate of osteotomy was significantly higher for Black than non-Black patients with late-onset disease. This difference could be attributable to the different BMIs between the two groups, as more severe cases are likely to receive more invasive treatment. Moreover, observed percent lost to follow-up in our study was 24% among non-Black late-onset patients, compared to 10% among Black late-onset patients. This difference was close to statistical significance (p = 0.06). Interestingly, this is opposite to what has been shown in previous studies, where governmental insurance, racial minority, and low socioeconomic status were risk factors for differential treatment and loss of follow-up in orthopedic surgery patients.26,29–31 A higher loss to follow-up among non-Black patients in our study could be a sign of less severe disease compared to Black patients, especially considering the flipped direction of association reported in the literature. 31 Nonetheless, we can only conjecture as we do not have the data to support this hypothesis.
Increasing rates of childhood obesity in the United States have presented a major health challenge.32,33 Although Blount disease remains rare, its incidence may scale with this trend. Large-scale studies have linked income level to childhood obesity, with Black children—especially Black boys—disproportionately at risk. 18 It is important to note that despite our findings, Blount disease has been reported with considerable prevalence in Scandinavian countries, 34 despite the low obesity rates. 35 This suggests that the etiology of Blount disease is likely multifactorial and cannot be explained by a single association. Although future research may or may not show that the racial predisposition of late-onset Blount disease is attributable to biochemical etiologies, our results suggest that the socioeconomic factors and racial disparities examined could be contributing to the observed predilection of Blount disease for Black children. An awareness of the effects of socioeconomic and racial disparities on disease is vitally important to develop effective interventions that can prevent disease on a public health perspective. This knowledge may also be useful on an individual level for surgeons to understand the factors influencing disease progression in their patients.
This study’s findings should be interpreted in the context of its limitations. As a retrospective study, it can identify associations only. As a chart-review study, it cannot comment on histologic or endocrine differences among Blount disease patients. Without a control group of non-Blount patients, this study also cannot assess independent risk factors for Blount disease. Given the heterogeneity of this multi-center population, however, designing a plausible control group was ultimately deemed unfeasible. In addition, attrition bias may be present as the proportion of patients lost to follow-up was nearly statistically different between Black and non-Black patients (p = 0.06). We were also unable to access patient radiographs to confirm Blount disease diagnosis or to account for disease severity. Future studies may be able to better assess the role of socioeconomic status in the racial disparities of Blount disease by examining the severity of Blount disease in relationship to socioeconomic status and obesity. Despite the limitations, to our knowledge, this study’s population, representing 125 late-onset patients from two large centers, constitutes the largest primary samples of Blount disease patients yet reported.
Conclusion
In our sample of late-onset Blount disease patients, Black patients had significantly higher mean BMI values, lower household incomes, and higher ratio of Medicaid enrollment than non-Black patients. Our findings suggest that race-associated socioeconomic factors are a relevant contributor to Blount disease and may help to explain the racial disparity of Blount disease in the United States
Footnotes
Author contributions
Walter Klyce—IRB, data acquisition, data management, result interpretation, manuscript drafting, manuscript revision. Daniel Badin—data acquisition, data management, result interpretation, manuscript drafting, manuscript revision. Jigar S. Gandhi—data acquisition, data management, result interpretation, manuscript drafting, manuscript revision. R. Jay Lee—IRB, conceptualization and design, data analysis, result interpretation, manuscript drafting, manuscript revision. B. David Horn—conceptualization and design, data analysis, result interpretation, manuscript drafting, manuscript revision. Erin Honcharuk—conceptualization and design, result interpretation, manuscript drafting, manuscript revision
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Johns Hopkins Hospital Department of Pediatric Orthopaedics and by the Children’s Hospital of Philadelphia Division of Orthopaedics.
Ethical approval
Institutional Review board approval was obtained from the Johns Hopkins Institutional Review Board (IRB00150443).
Consent to participate
Since this study was a retrospective chart review, consent for participation was waived and approval of this waiver was obtained by the institutional review boards at Johns Hopkins and at Children’s Hospital of Philadelphia.