
Abstract
Abstract
Background/purpose
In our clinical practice we found that some patients treated with external fixation, especially those with Blount disease, had notable weight gain. We hypothesized that correction of Blount disease using external fixation would be associated with weight gain and that the weight gain would be greater than that seen in other patients.
Methods
This was a retrospective chart review of patients with Blount disease at two children's hospitals. Patients with Blount disease were compared to patients treated with external fixation for fracture or other deformity. The data recorded included initial and post-treatment weight and time in external fixation. Within each group pre-operative weight was compared with post-treatment weight, and weight gain was compared between groups.
Results
The study cohort comprised 39 patients with Blount disease and 13 control patients. The average age and weight of the patients with Blount disease and the controls were 12.8 years and 106.4 kg (1.7 × the 95th percentile weight for age) and 12.2 years and 52.4 kg (0.89 × the 95th percentile weight for age), respectively. Patients with Blount disease gained an average of 3.7 kg (range −12.5 to +43.1 kg) during 18 weeks of treatment (0.19 kg/week), and the controls gained an average of 4.1 kg (range −4.4 to +19 kg) over 17 weeks (0.247 kg/week). The weight gain during treatment was statistically significant for both groups, but was not statistically different between groups.
Conclusion
Patients with Blount disease as well as those with other conditions treated with prolonged external fixation experience significant weight gain which could complicate rehabilitation or return to previous activity.
Introduction
Obesity now affects one in five children in the USA and has become a global concern. It is the most prevalent nutritional disease of children and adolescence [1]. The association between obesity and Blount disease is well established [2, 3]. Although the etiology of Blount disease may be multifactorial, the strong association with childhood obesity suggests a mechanical basis [4–6]. Adolescent Blount disease patients will often report pain in the affected limb(s) and an inability to participate in physical activity. The subsequent sedentary lifestyle promotes weight gain in an already obese patient population.
Surgical treatment of this condition is aimed at deformity correction in the hope of restoring function, alleviating pain, and enabling a return to a more active lifestyle. One effective method of treatment includes osteotomy followed by gradual correction with a circular external fixator [7, 8]. Prior outcome analyses for Blount patients undergoing surgical correction have included radiographic and clinical parameters [9]. None of these studies have assessed weight change, which may have clinical implications for future function, restoration of normal development, safety, bone health, and self-esteem [10–15].
The aim of our study was to examine the weight change associated with prolonged external fixation in Blount patients. We hypothesized that significant weight gains may occur due to enforced inactivity. For comparison, we chose a group of patients undergoing external fixation for fracture or deformity correction other than Blount disease. Information from this study may be used to inform patients and caregivers about possible weight gain and to develop strategies to limit weight gain and promote weight loss after the completion of treatment.
Materials and methods
After obtaining approval from our Institutional Review Board, retrospective analyses were performed on 39 consecutive juvenile or adolescent Blount patients who underwent surgical osteotomy with external fixation. Data were included from two institutions over a 5-year period (2005–2010). Weight was recorded from the medical record at time of the operation, at frame removal with return to weight bearing, and at clinical follow-up. Patients who underwent sequential bilateral procedures or bilateral procedures with less than 6 months intervening between the two procedures were considered to have undergone a single procedure. Patients who underwent bilateral procedures separated by more than 6 months were considered to have undergone two separate procedures. All patients had physical therapy in the hospital for ambulation following their procedure. The patients’ weight-bearing status was touch-down weight bearing for the first 4 weeks followed by progressive weight bearing as tolerated. Following frame removal, patients were placed in a long leg cast for 4 weeks and allowed to ambulate as tolerated. Upon cast removal, patients were instructed to gradually increase activity as tolerated to a self-selected level.
A control group included 13 consecutive patients with fracture or lower extremity deformity other than Blount disease who were treated with circular external fixation. These patients underwent a period of non-weight bearing similar in duration to that of the study group. Body weight was recorded from the medical record at the time of the operation, at frame removal with return to weight bearing, and at clinical follow-up. In most cases height was missing or self-reported, precluding the calculation of body mass index.
Data from the study and control groups were compared using Student's t test. Significance was set at p < 0.05.
Results
The average age of patients with Blount disease and the controls was 12.8 and 12.2, respectively. In the Blount disease group, two patients were Caucasian and 37 were African-American compared to eight Caucasian and five African-American control patients. The patients of both groups experienced significant weight gain during treatment (Fig. 1). Patients with Blount disease weighed an average of 106.4 kg before treatment, which is 1.7-fold the 95th percentile weight for age (range 0.88–2.65; only 2 patients weighed less than the 95th percentile for their age). The average weight of the control patients was 52.4 kg, which is 0.89-fold the 95th percentile weight for age (range 0.66–1.3) (Fig. 3).
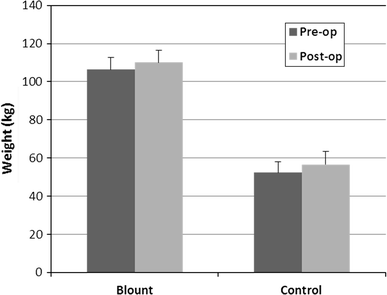
Mean pre- and post-operative weights of patients with Blount disease and the controls. Error bars Standard error of the mean (SEM)
Our patients with Blount disease gained an average of 3.7 kg (range −12.5 to +43.1 kg) during 18 weeks of treatment (0.19 kg/week). Among these patients eight lost weight (20 %) during the study period, five maintained their weight (±1 kg from pre-operative timepoint), and 26 (67 %) gained weight (Fig. 2). For those who gained weight, the average gain was 7.3 kg. Control patients gained an average of 4.1 kg (range −4.4 to +19 kg) over 17 weeks (0.24 kg/week). In the control group, two patients lost weight (15 %) during the study period, three patients maintained their weight (±1 kg from pre-operative time point), and eight (62 %) gained weight. Of those who gained weight, the average gain was 7.7 kg. The weight gain during treatment was statistically significant for both groups, but was not statistically different between groups (control vs. patients with Blount disease). Four outliers were identified with a gain or loss more than two standard deviations from the mean for their group, but their exclusion did not change the comparisons or the statistical significance. The pre-operative weight and weight change during treatment were compared (Fig. 3). Weights at follow-ups between 6 and 12 months were available for only a very limited number of patients. The seven patients with Blount disease with known follow-up weights had continued to gain weight (average 22.7 kg, range 1.2–60 kg) while the three control patients had gained 0.3, 2.5, and 5.4 kg.
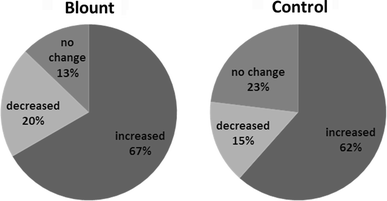
Percentage of patients who gained or lost weight. Weights within 1 kg of the pre-operative weight are not considered to have changed
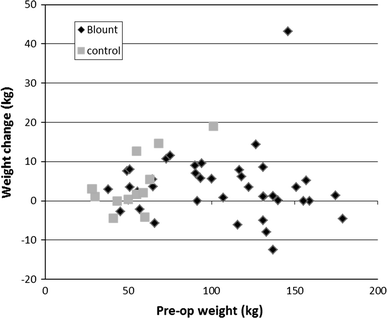
Change in weight vs. pre-operative weight. Each graph point represents a single patient with weight change plotted against pre-operative weight
Discussion
The majority of patients with Blount disease as well as other conditions treated with prolonged external fixation experience significant weight gain during treatment, with the amount of weight gained greater than would be expected during normal growth and development [16]. In this population of patients, there is a trend toward excessive weight gain even after healing of the osteotomy and a return to activity. This trend suggests that adolescents undergoing Blount deformity correction are at significant risk for further weight gain, which carries numerous health consequences. It also suggests that despite surgical correction these patients may not return to being physically active to a degree sufficient to reduce weight. Similar findings have been reported in studies on knee arthroplasty in adults [17]. It is important for orthopaedic surgeons to inform patients and families of this likely post-surgical consequence, to offer resources for dietary counseling, and to encourage a return to physical activity after healing [18].
In our study, our control patient population gained a similar amount of weight as the patients with Blount disease, which is surprising, and most likely has multifactorial origin. One possibility is that the relative immobility in Blount patients does not differ much from their baseline activities, whereas in the control group a period of treatment and immobilization produces a significant decrease in their baseline activity level and caloric expenditure, leading to weight gain. Our data show that all patients, not just obese patients with Blount disease, may benefit from pre- and post-operative counseling on nutritional and caloric intake as well as post-operative activity levels. Specific protocols to increase activity levels during and following treatment may need to be developed.
This study has several limitations. The sample size was relatively small and, therefore, we are only able to identify trends in weight gain after external fixation. A larger group of patients would allow us to further analyze the subgroup of patients who had excessive weight gain in order identify the associated risk factors. This information would lead to more effective post-operative treatment strategies. Additionally, data on follow-up weights were often not recorded in the medical record, which limits our ability to draw conclusions on the progression of weight gain or loss with return to physical activity. Future prospective studies with accurate height and weight measurements as well as patient-based outcome measures, such as pain scales, activity assessments, or dietary logs, may be helpful in identifying the causes of the observed weight gain.