
Abstract
Early detection of feeding difficulties in childhood is critical for timely support, which may prevent simple feeding problems from becoming pervasive or resistant to intervention. Our study aimed to describe the range of the knowledge, attitudes and practices of established paediatricians, GPs, CHNs and early childcare educators working with young children with feeding difficulties and their caregivers. Focus groups and semi-structured interviews were conducted with Australian paediatricians, General Practitioners (GPs), Child Health Nurses (CHNs), and early childhood educators working with children aged two years and below. Findings from our study suggest that healthcare practitioners are relying on anthropometric measurements of growth to identify feeding difficulties, and the most common age at which feeding difficulties are seen in practice is after two years of age. Food insecurity, cultural factors, and access to specialised services are still a challenge, creating a barrier to early identification and intervention.
Introduction
Establishing healthy feeding practices early in life may promote healthy eating patterns later in life (Craigie et al., 2011; Nicklaus & Remy, 2013) and provide protection from multiple chronic diseases (Schwartz et al., 2011). Assessing and managing feeding difficulties in the early years, however, can be complicated and frustrating for health professionals and parents (Baraskewich et al., 2021), with many healthcare practitioners having difficulty differentiating feeding difficulties from typical patterns of development (Ashley et al., 2020). Subsequently, a ‘wait-and-see’ approach is commonly adopted by healthcare practitioners and parents, which is thought to delay the identification and treatment of problematic feeding patterns (Bahr & Johanson, 2013; Taylor & Taylor, 2021). There is no evidence to suggest that feeding difficulties will resolve over time or what length of time is reasonable to wait before seeking support (Taylor & Taylor, 2021). There is consistent evidence, however, in the literature that feeding difficulties do not improve over time without access to treatment (Suarez et al., 2014).
In young children, feeding difficulties can manifest as significantly limited food preferences, hypersensitivity to food textures or temperatures and pocketing food without swallowing (Mayes & Zickgraf, 2019). Multiple factors, including breastfeeding, prematurity, the introduction of solids and textured foods, restrictive parental feeding styles, child’s sensory sensitivities, feeding techniques, and child temperament, are associated with the early emergence of feeding difficulties in neurotypical children (Mudholkar et al., 2023). The prevalence of feeding difficulties is on the rise as medical advancements are improving the life expectancy of infants and children born prematurely with low birth weights and complex medical conditions (Kovacic et al., 2021). Evidence also suggests that feeding difficulties in early childhood are predictive of eating disorders such as anorexia nervosa and bulimia nervosa in adolescence (Herle et al., 2020).
Early detection of feeding problems in childhood is critical for timely support, which may prevent simple feeding problems from becoming pervasive or resistant to intervention. However, many reports in the literature indicate inconsistent practice in detecting feeding issues in young children (Brackett et al., 2006; Sdravou et al., 2021). One of the reasons given for the failure to detect atypical feeding behaviours during child health check-ups has been a tendency to focus on anthropometric measures of growth as a marker for problem eating (Sharp, Berry, et al., 2013). This approach, however, has been observed to be flawed, given that many young children with feeding challenges do not present with growth concerns (Cooke et al., 2017). Furthermore, feeding difficulties are multifactorial, making it more difficult for early childhood practitioners to isolate feeding as a primary issue. In Australia, General medical Practitioners (GPs) and Child Health Nurses (CHNs) are generally the first point of contact when parents/caregivers are concerned with their child’s feeding development. Children with more complex feeding difficulties are referred to a paediatrician. Further, with more than 45% of children aged 0–5 years attending childcare in Australia (AIHW, 2022), childcare educators are an increasing resource for families regarding healthy eating and carry the responsibility to support young children’s development in this area. There is a common practice to ‘wait and see’ before acting on early feeding concerns (Taylor & Taylor, 2021). Within the Australian context, it has been recognised that child nutrition is a major public health concern (Australian Institute of & Welfare, 2012; Gibney, 2004). To date, however, there are no studies examining the practices of Australian early childhood practitioners regarding the identification and referral for the treatment of young children with feeding difficulties.
This study aimed to describe the range of knowledge, attitudes, and practices of established paediatricians, GPs, CHNs, and early childhood educators in Australia regarding the identification of feeding difficulties in infants and young children (0–2 years).
Methods
Study design
A descriptive qualitative study design utilising both focus groups and individual interviews was adopted for this study.
Sampling and recruitment
Paediatricians, GPs, CHNs, and childcare educators working with children aged 0–2 and practising in Australia were invited to participate. A convenience sampling strategy followed by snowball sampling was employed, and interested participants were encouraged to tell eligible colleagues about the study. Letters of invitation were sent to the GP and paediatricians’ practices and early childcare centres in the authors’ local areas. Participants were also recruited through social media such as Facebook, Twitter, and LinkedIn, targeting specific GP, paediatrician, MCHN, and early childhood educators’ groups. Authors distributed the letter of invitation through their professional networks as well.
Ethical considerations
The study was approved by La Trobe University’s Human Research Ethics Committee (approval number: HEC23125). All eligible and interested participants read and signed the participant information sheet and consent form before their involvement in the study. To preserve participant and service provider anonymity, no identifying information is included in this article. This study was considered low risk as the participants were trained professionals equipped to manage difficult situations.
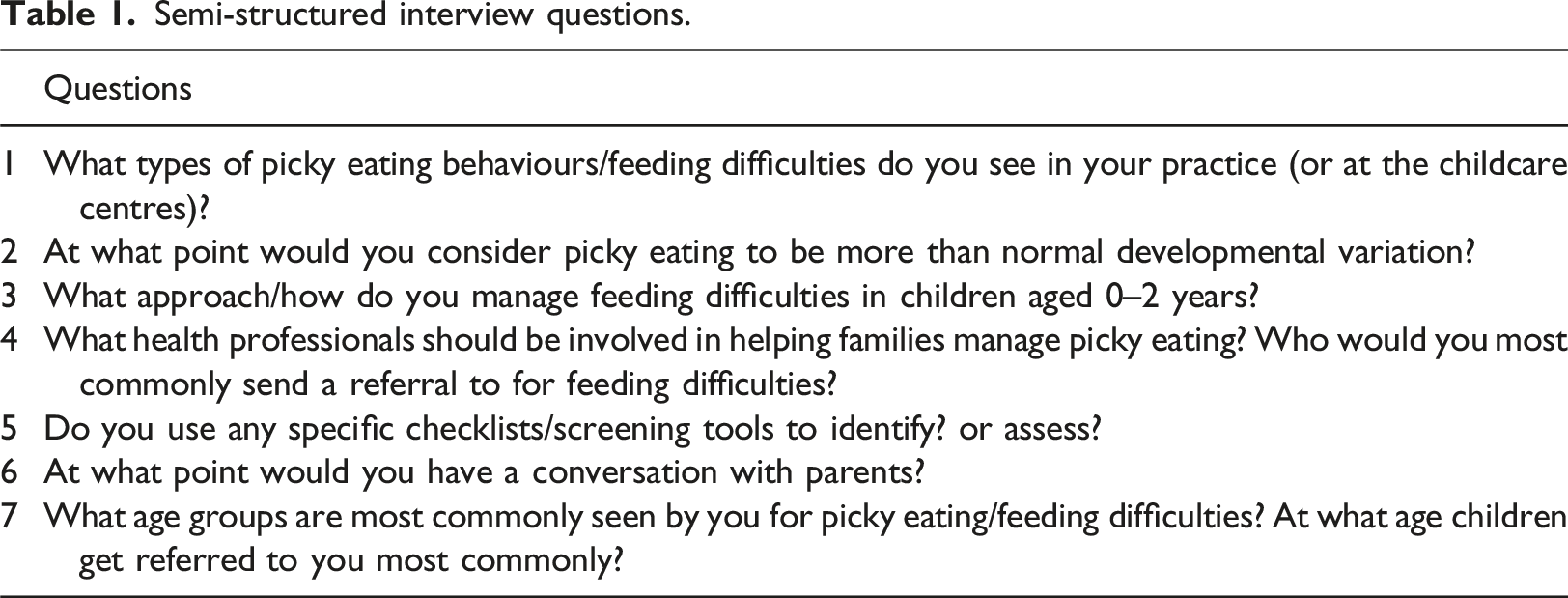
Procedure
Semi-structured interview questions.
Data analysis
Inductive thematic analysis was carried out on the participant responses by the first author (Braun & Clarke, 2019). The data from transcriptions was organised within NVivo 12.0 to highlight emergent themes. The first author started the analysis by familiarising themselves with the data by reading and re-reading the transcripts. Next, initial codes and themes were generated. Codes were then categorised into themes and subthemes following an iterative and reflexive stance. Codes were then assigned to quotations and rearranged. Finally, the analysis process was completed with the interpretation and mapping of the data. The themes were then shared, discussed, and agreed upon with the last author. Data was also triangulated by debriefing meetings with all the co-authors, diagramming (mind mapping) to make sense of the theme connections, and the first author reflecting on their own assumptions and biases that may affect the interpretation of data.
Next, as per Braun and Clarke’s (Braun & Clarke, 2006) recommendation, the data was analysed at a semantic level, focusing on what the participants said rather than interpreting the underlying meanings. Reflexive thematic analysis was chosen for its inductive process by allowing new knowledge to be created, which is suitable for this under-researched area (Yehl, 2016).
Results
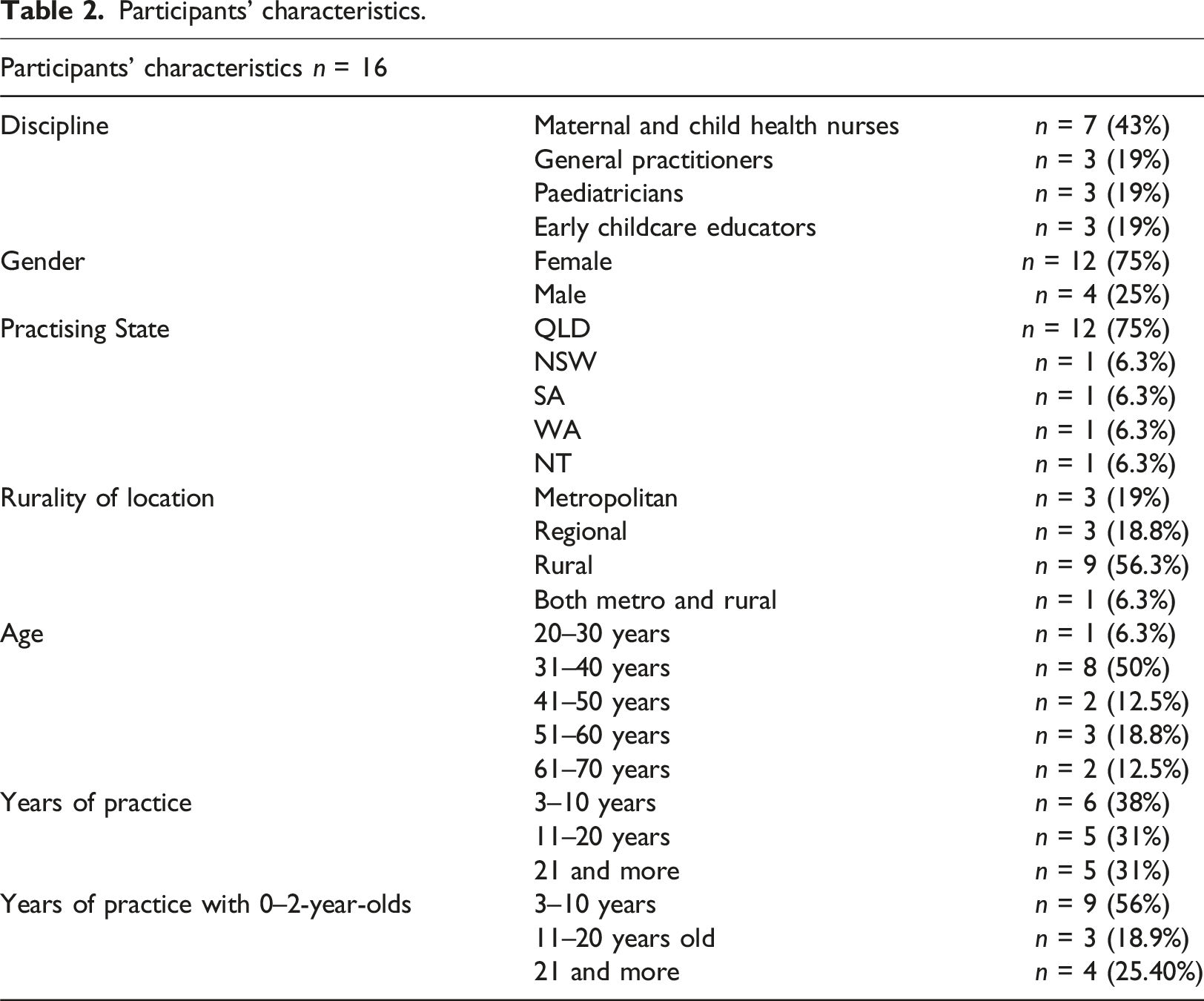
Participant characteristics
Participants’ characteristics.
Thematic analysis
Data was coded against four broad descriptive themes: knowledge, attitudes, practices, and related factors, with one overarching analytical theme: feeding difficulties as an invisible condition (Figure 1). These four themes overlap and are further categorised into subthemes, indicating further exploration. Analytical and descriptive themes and subthemes. Note. The themes are bold, and the subthemes are italic.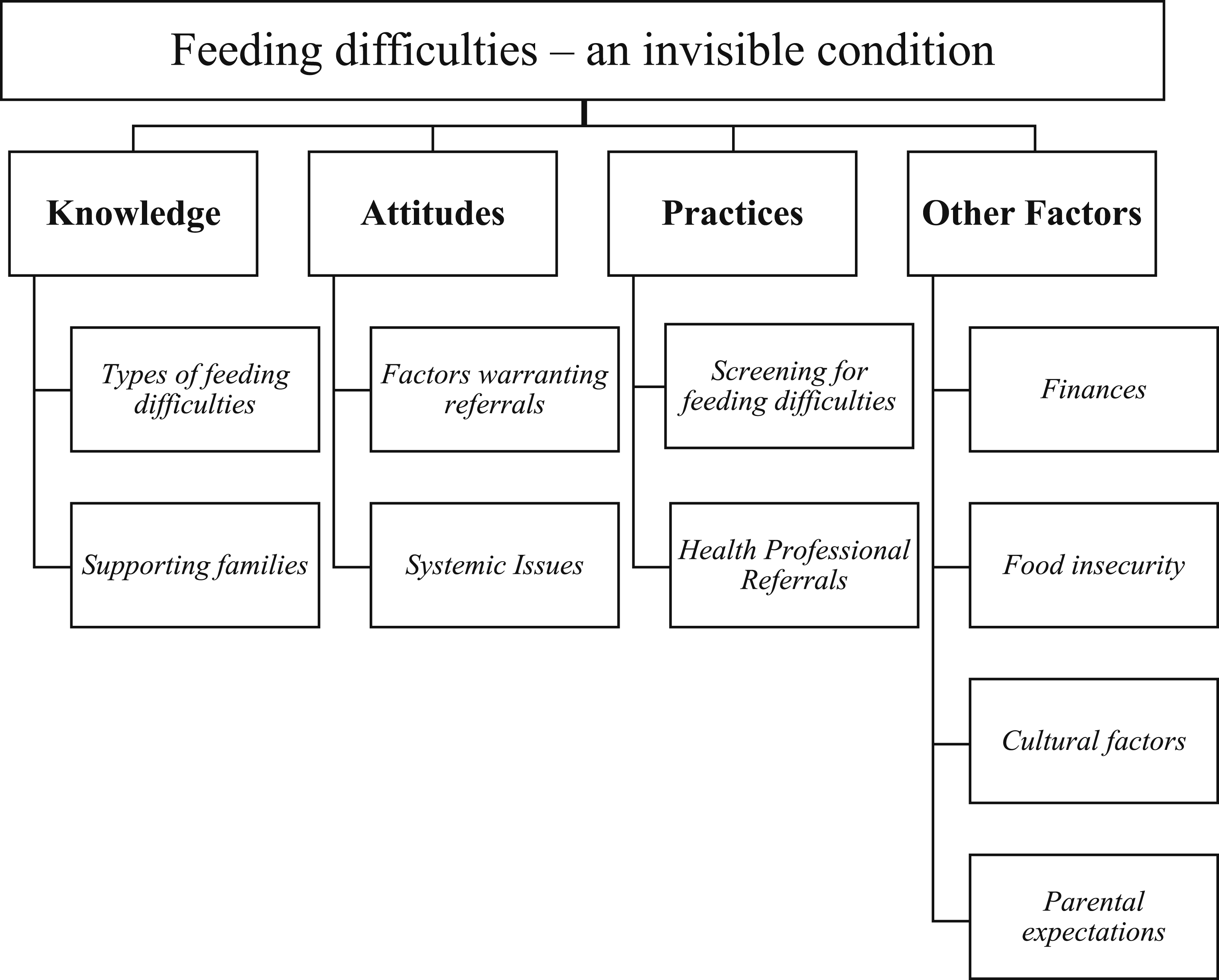
Descriptive theme 1: Knowledge of participants
Subtheme (a) Types of feeding difficulties
This subtheme refers to the types of feeding difficulties in healthcare professionals’ practice and at childcare centres across the early years. During the first six months of age, the most common feeding difficulties seen were concerns with breast and bottle-feeding, including poor fit and latch, lip and tongue ties, and laryngomalacia. Feeding difficulties associated with prematurity and genetic conditions, such as congenital heart disease, Down Syndrome, and Angelman’s Syndrome, were also seen in this age group.
“We see a lot of babies that are on purees for a long period of time. And they’re either not interested in picking up foods and eating them, or their gag reflex is prolonged, and it’s taking them a long time to get rid of that.” (Participant 3 – Early Childcare Educator)
From 12 months of age onwards, the most commonly identified feeding challenges were difficulties with weaning off bottles, picky eating, parental concerns for inadequate volumes, and sensitivity to taste and textures. One of the paediatricians (Participant 11) said that the “most common things that we would see would be parental concern around inadequate volumes. So, you know, parents feeling that their children relatively survive on cheese and air during the day.”
Most participants said parents approach them about feeding difficulties, most commonly after two years of age. Participants agreed that parents generally contact their peer support group for advice if they notice feeding concerns. Parents only seek medical advice if the child consistently struggles to eat or is not gaining enough weight.
“I think a lot of parents are willing to tolerate up until about two, particularly, you know, the use of the bottle is quite normal up to the age of two, whereas parents would expect that their child is not on bottles after the age of two. And so, I think parents start becoming increasingly concerned in that three to five age group. And it’s often when they (parent) look back at that, they go, oh, actually, you know, they were always picky as a toddler, and they (child) just got more and more picky as they got older.” (Participant 11 - Paediatrician)
Subtheme (b) Supporting families
This subtheme refers to how participants support families presenting with a child with feeding difficulties. The majority of health care professionals provided education for breast and bottle feeding, as well as introduction to solids. They also recommended modelling healthy eating and providing opportunities for the child to eat different foods. Almost all participants directed families to refer to the Australian Web site, “Raising Children Network”, and social media pages for healthy eating. The childcare educators provided information for community resource groups, mothers groups, and WHO guidelines for early feeding milestones. The CHNs recommended that parents read the child health record book provided by local community health services to families where information regarding the child’s growth, development, and immunisations is found.
“Just, I guess, giving them some sound solid strategies without too much, you know, you must not do this, or you must do this because that makes people feel like they’re not doing a good job”. (Participant 2 – GP)
“I’m just very aware that a lot of what parents will spend a lot of their day being exposed to is actually social media. I think, for example, if you used the Raising Children Network, although that’s a very helpful resource, it is still quite linguistically mature and can take quite a period for a family to sit down and read through all of those concepts. Whereas, you know, if they’re following you know, Feeding Littlies or something on Instagram or Facebook, then, the story might pop up about, you know, this meal is okay, but this meal is also okay. And just provides that positive reinforcement in 5–10 seconds for a family about you know, that what they’re doing is okay, and providing small tips along the way”. (Participant 11 – Paediatrician)
Descriptive theme 2: Attitudes of participants
Subtheme (a) Factors warranting referrals
This subtheme refers to participants’ opinions on feeding difficulties warranting action or referrals to other healthcare professionals. Participants agreed on four factors that triggered their action to refer to other health professionals for more detailed follow-up. Those factors were: (i) meeting criteria for failure-to-thrive, (ii) medical complexity, (iii) deficiency in micronutrients, and (iv) not putting on enough weight.
“I guess with babies, you would pick it up if the weight gain wasn’t, you know, what we desire, in the 120 g a week, if even though they’re feeding, they’re not gaining weight, you’d pick up that, you know, something is going on and refer them on.” (Participant 10 - CHN)
“And whether I may need to do further investigations, checking for iron and other micronutrient deficiencies, such as vitamin A. And then it will depend on whether the child has other comorbidities, which usually, you know, haven’t been diagnosed in the zero to two age group.” (Participant 11 - Paediatrician)
Subtheme (b) Systemic care issues preventing action
This subtheme refers to systemic challenges the participants faced in their work settings that prevented action regarding feeding difficulties in young children. Specifically, access to suitable or timely care may be limited due to financial barriers or geographical isolation, lack of staff availability, waitlists, poor post-partum care, and other gaps in the system.
“We have very limited availability in the public service, and that would need a significant associated growth disruption to be seen publicly (in the public system).” (Participant 11 – Paediatrician)
“We really don’t see them (babies) too often. So, we see them at six months. And because we’re just such a busy service, we don’t, unless they’re specifically targeted. Because, in the Red Book (local child health record), as you know, there’s no real nine-month assessment. Unless we’ve specifically targeted something at six months, then we’re not going to see them. We just don’t have the capacity to offer nine-month appointments to families.” (Participant 4 – CHN)
“So, there’s decreasing numbers of nurses and midwives’ in remote areas. There is a high turnover of staff, and this contributes to an endless stream of locums that absolutely impacts on the quality and continuity of care”. (Participant 13 – CHN)
Descriptive theme 3: Practices of participants
Subtheme (a) Screening for feeding difficulties
This subtheme refers to tools participants used to identify, screen, or assess for feeding difficulties in their day-to-day practice. Participants reported not having a specific screening tool for feeding difficulties. Most participants mentioned talking to parents to gather information (history taking), checking for developmental milestones, asking for blood tests, checking for weight and height, and relying on their clinical judgement.
“I don’t particularly think that we have a checklist as such. It’s when I have to go back to the organisation to see if they had something particular about if it’s not something that I’ve noticed, I mean, there is, you know, particular developmental milestones that we, you know, that we can look for it.” (Participant 5 – Early Childcare Educator)
“We have, you know, a four-month developmental assessment, six months, and on those sorts of all the milestones and that type of thing. But we don’t have a specific feeding checklist as such.” (Participant 10 - CHN)
Some participants also reported that having access to a feeding-specific screening tool would be useful in their practice.
“I think like a screening tool is a great idea because, you know, we have screening tools for hearing, we have screening tools for vision, we have screening tools for speech, but we don’t have a screening tool that I’m aware of a generic screening tool that all child health nurses use for feeding.” (Participant 4 – CHN)
Subtheme (b) Health professional referrals
This subtheme refers to whom participants commonly send referrals to manage feeding difficulties. Participants reported that they sent referrals to a dietitian, GP, or paediatrician if the child could not put on weight or was medically complex. A referral to lactation consultants was sent with difficulties with breast and bottle-feeding.
“And if they still need help, I refer them to dietitians, like particularly the dietitian who perhaps can go into what that baby at that particular age needs and the protein, carbohydrate, you know, this is what they need for growth.” (Participant 17 – CHN)
A referral to an occupational therapist or a speech therapist was made if there were developmental or speech delays.
“I would mostly recommend them to a speech pathologist over a doctor, just because they are more experienced with the mouth.” (Participant 3 – Early Childcare Educator)
Early childcare educators mentioned that they generally ask parents to see a child health nurse or a GP.
“Yeah, child health nurse. Child health nurse out here who has come along to some of the playgroups. So, we can refer to the child health nurse, but basically, it’s to the GP.” (Participant 5 – Early Childcare Educator)
Descriptive theme 4: Other factors
This theme emerged from the unstructured conversation of participants while answering the study questions.
Subtheme (a) Finances
This subtheme concerns caregivers’ financial challenges, as feeding therapies can be expensive. Participants discussed that people living in remote areas find it financially challenging to travel for appointments. Also, access to fresh produce and means to store food safely may be limited for people from low socio-economic strata.
“In a resource-limited setting, it’s quite challenging. And often, parents can’t afford to pay lots of money to go see a dietitian or do some feeding therapy, for example.” (Participant 6: Paediatrician)
One of the remote area nurses shared her experience of visiting remote First Nations communities experiencing significant financial hardships.
“It’s just probably the expense, you know. So, foods are usually bought, like, on the day. They do that; it’s like one big shop. They just buy it for everyone and then cook it then. And then that’s the feed. And then suddenly in that week, you know, pay week, you have lots of food, those two days and then the rest of the four days, you know, you have Weetabix and noodles.” (Participant 14 – CHN)
Subtheme (b) Food insecurity
Along with financial challenges, participants discussed food insecurities faced by families, especially families from low socio-economic groups and First Nations families living in remote communities. Also, participants acknowledged that understanding and responding to food insecurity is an important part of their practice.
“I think we also see a lot of growth problems that have underlying feeding difficulties issues around food security”. (Participant 2 – GP)
“Yeah, and they get a referral to the paediatrician. And then they start on the pediasure drinks, but the problem is, we’ll give pediasure drinks to take home. And because there’s overcrowding in the house, and there’s, you know, eight or nine kids in the house, it’s all gets shared out. It’s not actually getting used for only that child.” (Participant 14 – CHN)
Subtheme (c) Cultural factors
Participants discussed their awareness of how cultural differences influence feeding and parental concerns around feeding difficulties.
“Also, cultural differences because some cultures have independent ideas; the child should feed on their own with a spoon and in some cultures, the mom wants to feed the child every single time. And also, this can change the dynamics of how the child feeds. Some children if they really want to eat, enjoy the food, they can have this with the spoons, and that’s good enough, but some children really want to be fed. And that can be a problem because if they (children) don’t like the taste or texture, or whatever the food is given, that can be a daily exercise for the mum, which can be really stressful.” (Participant 7 – GP)
One of the remote area nurses mentioned that it can be difficult to maintain continuity of services, especially for First Nations families who travel frequently for cultural reasons such as “Sorry Business”, which is an important time of mourning that involves responsibilities and obligations to attend funerals and participate in other cultural events, activities or ceremonies with the community.
“The hard thing about our population is the transient nature of the families. So, a lot of people travel for “sorry businesses”. That can be like, hundreds of kilometres away. Yeah. And so, you know, sometimes will see them for, you know, three months and then move on, and then we won’t see them until next year.” (participant 14 – CHN).
Another CHN, visiting remote Aboriginal communities, mentioned their knowledge and awareness about breastfeeding in First Nations families and how they are culturally well-supported to continue to breastfeed as compared to non-Indigenous families.
“I generally find that Aboriginal mums in communities have a lot higher breastfeeding rate. And I think it’s good for that sense of community and other moms that are supporting them, showing them how to put their babies on breast is unlike some of Western culture, where we are hiding the baby to breastfeed.” (Participant 15 – CHN)
Subtheme (d) Parental expectations and concerns
A few participants talked about how parental expectations and/or concerns about a child’s feeding can escalate the situation and cause more stress for both the child and the parent.
“When a child is picky, the parent becomes increasingly escalated, and they become quite focused then on exactly what the child is eating and encouraging the child to expand their variety at which point the child then doubles down on what they choose to eat, and they double down on the fact that they’re only going to have cheese, thank you so much. And it gets into a bit of a power-play struggle. So, it’s also dependent on parental concerns as part of it.” (Participant 11 – Paediatrician).
Analytical theme: Feeding difficulties – An invisible condition
The overarching theme that emerged from the data was that feeding difficulties are an invisible condition. This theme was evident in parents not commonly reporting feeding difficulties in the first two years of life and healthcare practitioners not considering them a serious issue unless the child is medically complex or meets the criteria for failure-to-thrive. Feeding difficulties in the first two years can be subtle and easily overlooked or misinterpreted, adding to the invisibility of the concerns.
“Yeah. I mean, usually, I like objective data. So, if it’s, if they have poor weight gain, if they’re deficient within their nutrients, or if the parents and child are distressed enough that it causes a functional problem, then I would be happy to say they had the feeding difficulties and need to be managed or supported.” (Participant 6 – Paediatrician).
“They (parents) just kind of fumble through and talk to their mothers’ group. And, you know, everyone’s like, yeah, no, my child only survived on biscuits today as well. And it’s when they kind of get past two years, and you know, you’re trying to really cut back on bottles, or they’re entering childcare, and maybe childcare makes a comment, Oh, you know, like, they don’t really eat as much compared to other kids that, that it starts becoming an issue for the family.” (Participant 11 – Paediatrician)
Discussion
This study aimed to describe the range of knowledge, attitudes, and practices of Australian paediatricians, GPs, CHNs, and early childhood educators about identifying feeding difficulties in infants and young children (0–2 years). Findings from this study show that healthcare practitioners are still relying on growth measures to identify feeding difficulties, and the most common age at which feeding difficulties are seen in practice is after two years of age. Further, challenges such as food insecurity and access to services are acting as barriers for practitioners in managing children with feeding difficulties.
Reports in prior literature indicate that feeding difficulties are often not detected during child health check-ups due to the focus on anthropometric measures of growth (Sharp, Jaquess, et al., 2013). Despite unbalanced nutrition, most children with feeding difficulties have average weight and growth (Sharp et al., 2013b), meaning that growth measures may not be sensitive to clinically significant feeding concerns. Also, a recent longitudinal study by Taylor et al. (2019) found that in a group of picky eaters, mean height, weight, and BMI trajectories did not indicate growth faltering as compared to their non-picky eating peers (Taylor et al., 2019). Despite consistent evidence in literature highlighting the limitations of growth measures for the detection of early feeding difficulties, all participants in our study reported that they prefer and rely on growth charts and blood tests to identify feeding difficulties. While reliance on anthropometric measures is warranted for children with medical complexity and failure to thrive, for most other children with feeding difficulties, it is essential to look at the characterisation and/or presentation of feeding difficulties. Although the child tracks well on the anthropometric measures, it is necessary to consider and investigate if parents report problematic feeding behaviours and restrictive or selective intake.
Furthermore, the participants reported not using a feeding-specific screening tool. It is known that feeding difficulties are complex and multifactorial (Mudholkar et al., 2023). A recent systematic review by Litchford et al. (2021) explored existing paediatric feeding screening tools that are valid and reliable in identifying feeding difficulties in children (Litchford et al., 2021). The authors identified 44 paediatric screening tools. The screening tools focused on four general methods to assess feeding difficulties: food intake, malnutrition, behaviour, and tools for specific conditions such as autism. Most screeners were caregiver-reported, spanned across a wider age group, and not validated. Also, there was no single tool that could identify feeding difficulties and risks in all populations, especially from birth to two years (Litchford et al., 2021). Developing a valid and reliable screening tool, specifically for children from birth to two years old, to screen for early feeding difficulties may be an effective way to improve rates of early identification and management.
Participants in our study reported that referrals were made to an occupational therapist or speech therapist for developmental delays and oral-motor difficulties, respectively. Referrals were sent to a lactation consultant for breastfeeding support and a dietitian for growth and nutritional support. Participants also sent referrals to CHNs for breastfeeding and transitioning to solids, and GPs for an initial assessment and referrals to a paediatrician and other specialised services. This referral pattern is consistent with the findings from literature with clinicians who are frequently referred to for children with feeding difficulties (Silverman, 2010). Earlier recognition and referrals to specialised feeding services may help reduce parental anxiety by promoting targeted support and advice for a child’s specific feeding challenges (Aldridge et al., 2010). Feeding difficulties are multifactorial in nature (Bruns & Thompson, 2010), and various factors can impact the progression of age-appropriate feeding skills (Silverman, 2010). The heterogeneity of feeding challenges requires a multidisciplinary or interdisciplinary approach to assessment and intervention (McComish et al., 2016). However, none of the participants mentioned referring to a multidisciplinary or interdisciplinary team. This may be related to not having access to services due to remote geographic locations, poor staff availability, and increased waitlists.
There is consistent evidence in the literature that many healthcare practitioners and caregivers of children with feeding difficulties fail to identify or underestimate the severity of feeding challenges and often use a wait-and-see approach (Taylor & Taylor, 2021). Also, a study on parental perspectives of feeding difficulties reported that most parents noticed feeding difficulties early on but only sought professional help after their child was two years old and above (Estrem et al., 2017). These findings are consistent with our results, where most participants reported that they don’t see children with feeding difficulties in their practice settings until after age two, when most parents seek help after exhausting suggestions from their peer support. Based on previous literature suggesting the transient nature of feeding difficulties in young children (Cardona Cano et al., 2015), health practitioners may be inclined to reassure the parents that their child will “grow out of it”. However, there is no evidence to suggest that factors associated with feeding difficulties will be resolved with time or how many months/years it could take. On the other hand, it is well-established that children with developmental vulnerability are at increased risk of feeding difficulties and these difficulties do not improve over time without access to intervention (Suarez et al., 2014).
Furthermore, food insecurity has been associated with restrictive compensatory parental feeding practices and unhealthier eating patterns (Feinberg et al., 2008; Kral et al., 2017). Food insecurity may also result in parents restricting their own diet in order to provide enough food for their children (Bruening et al., 2012). In our study, the child health nurses practising as remote area nurses and the health practitioners working in rural and remote areas demonstrated awareness and knowledge of food insecurity in limiting access to fresh and healthy food choices. Along with food insecurity, it is vital to consider cultural factors that may be regarded as healthy, harmful or culturally acceptable (Kumanyika, 2008). Cultural factors also influence where advice is sought regarding a child’s feeding (Cachelin & Thompson, 2013; Hughes et al., 2006). Participants in our study also reported awareness of feeding challenges influenced by cultural differences in their practices.
Inequity in the provision of health services is an ongoing challenge (Duplantie et al., 2007; O'Callaghan et al., 2005; “Publication of Health, United States, 2001 With Urban and Rural Health Chartbook,” 2001; Wakerman, 2008). In Australia, achieving health equity is particularly challenging due to its vast geographical landscape and sparsely distributed population (Alston, 2007). The most commonly reported barriers to people living in rural areas are travel, distance, waiting lists and expenses (O'Callaghan et al., 2005). Almost 75% of our participants were practising in rural and regional areas and reported challenges associated with long waitlists, not having access to feeding therapy providers and financial constraints due to geographical isolation. It may be an essential step to investigate and develop specialised feeding assessments and interventions to be delivered via telehealth for improved access.
Strengths and limitations
To the authors’ knowledge, this is the first study to examine the knowledge, attitudes, and practices of paediatricians, GPs, CHNs, and early childcare educators about feeding difficulties in young children from birth to two years. Our study also had a strong representation of rural and remote healthcare providers.
One limitation was the lack of direct caregiver input, as the perceptions of health care practitioners and early childcare educators regarding cultural factors, parental expectations, and reporting of feeding difficulties may be different. The second limitation was the relatively small sample size for a qualitative approach, as well as the convenience sampling, which limited the generalizability of the study results.
Conclusion
This study provided valuable insight into the knowledge, attitudes, and practices of established paediatricians, GPs, CHNs, and early childcare educators working with caregivers of young children with feeding difficulties. This study highlighted that early childhood practitioners may need to systematically identify and examine factors associated with feeding difficulties in young children. They also need to adopt a broader multidisciplinary approach to support caregivers and young children with feeding difficulties. Food insecurity, cultural factors, and access to specialised services are still a challenge for parents of children with feeding difficulties, creating a barrier to early identification and intervention. It is important to investigate and explore these contextual factors further to understand their impact on families, especially families from culturally diverse backgrounds and/or living in rural and remote communities.
Footnotes
Acknowledgements
We thank all the professionals who participated in the research despite their busy work schedules.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author, [AM], upon reasonable request.