
Abstract
This study evaluated the effectiveness of an online short course based on the Health Promoting Schools Framework and specifically designed for Early Childhood Education and Care (ECEC) professionals. The short course aimed to enhance ECEC professionals’ nutrition knowledge, confidence, role legitimacy and adequacy to model healthy behaviours, teach healthy food habits and create health-promoting environments. Participants (n = 116) working at Australian ECEC services were assigned to control (n = 62) or intervention (n = 54) groups. Both groups completed a pre-intervention survey. The intervention group accessed the four-week course and completed the post-intervention survey. The control group completed a second survey after four weeks but before accessing the course. Statistical analyses revealed significant positive changes in confidence, nutrition information utilisation and role perception for the intervention group. This study’s findings suggest that evidence-based online nutrition training could be used to improve ECEC professionals’ practice to foster better nutrition outcomes for young children.
Keywords
Introduction
Globally, rates of overweight and obesity have tripled since 1975, with the World Health Organisation (WHO, 2021a) reporting 39 million children (to age five years) are affected by this preventable disease. In Australia, one in four children is affected by overweight/obesity, increasing their risk of chronic disease (Australian Institute of Health & Welfare [AIHW], 2020). Overweight/obesity is a complex health issue influenced by genetics, health inequalities, environmental and societal factors, with diet being a major contributing factor (Australian Institute of Health & Welfare, 2021; Sambell et al., 2020). According to the National Health Survey (Australian Bureau of Statistics [ABS], 2018), discretionary foods contribute 38.5% of a child’s daily energy intake, raising concerns about the quality of children’s diets and effects on overweight/obesity (Jakobsen et al., 2023).
Approximately 1.4 million Australian children attend an ECEC service for, on average, 27 hours/week (Australian Government Department of Education, 2023), presenting an opportunity for services to promote lifelong healthy food habits and preferences for children; recommended by the WHO (2016) and Australian National Obesity Strategy (Commonwealth of Australia, 2022). In addition, the National Quality Standards (Element 2.1.3) mandate the promotion of food and drinks that are “nutritious and appropriate for each child” (Australian Children’s Education & Care Quality Authority [ACECQA], 2017, p. 62). Therefore, ECEC professionals are expected to role-model healthy eating behaviours and provide nutrition education to children, which should be captured in a comprehensive healthy eating policy (ACECQA, 2017).
However, a review of 523 ECEC services found 12.6% had no nutrition policy, while 50.5% had only a partially implemented policy (Lum et al., 2023), highlighting an urgent need for ongoing monitoring and support to ensure policies translate into practice (Ramia et al., 2023). ECEC Directors have reported difficulties establishing a healthy food environment at their service across all domains, from tailored nutrition policies to providing nutrition education to children in a workplace constrained by time and resources (Kirkegaard et al., 2023).
When food is prepared on site and provided to children, it often does not meet the Australian Dietary Guidelines standards for young children (Yoong et al., 2014). Discretionary foods are overprovided (Wallace et al., 2017a) and role modelling healthy eating behaviours at mealtimes is inconsistent (Byrne et al., 2022). Additionally, ECEC professionals may lack the skills and confidence needed to teach children basic nutritional concepts (Wallace et al., 2017b), which may lead to diminished perceptions of their role adequacy and legitimacy regarding promoting healthy eating (Forde et al., 2021).
Offering evidence-based food and nutrition training to ECEC professionals is important as it can help them to provide healthy food environments (Wallace, 2016) and enhance their perceptions of role adequacy and legitimacy (Forde et al., 2021), leading to greater job satisfaction and motivation (Skinner et al., 2009). Training can also increase ECEC professionals’ confidence to share food and nutrition information with children and their families (Devine et al., 2019), important as professionals can be misinformed by less credible sources of food and nutrition information (Devine et al., 2019; Wallace et al., 2017b).
Adopting a whole-of-service approach is essential to consider all aspects of the food environment, including the nutritional quality of food, staff role modelling healthy behaviours, teaching healthy food habits to children and creating a health promoting environment (Matwiejczyk et al., 2018). The WHO (2021b) recommends strengthening the ECEC workforce’s capability to improve food environments by establishing systems within services for ongoing competency-based training and programs to address sector-specific needs. However, there is a lack of evaluated online nutrition training specifically designed for ECEC settings, and professionals receive limited food and nutrition training as part of their education (Wallace, 2016).
This study sought to develop and test an online short course, called ‘SNACing_101’, specifically designed to enhance the nutrition knowledge of ECEC professionals. We aimed to improve participants confidence as effective role models for children and to communicate appropriate nutrition messages to families. We hypothesised that increased knowledge, delivered through specific training, would enable professionals to improve the quality of food environments within ECEC settings – crucial for wider health promotion (Walker & Littlewood, 2018).
Methods
This study was approved by Edith Cowan University Human Research Ethics Committee (approval number 19469-WALLACE), with informed consent obtained from all participants.
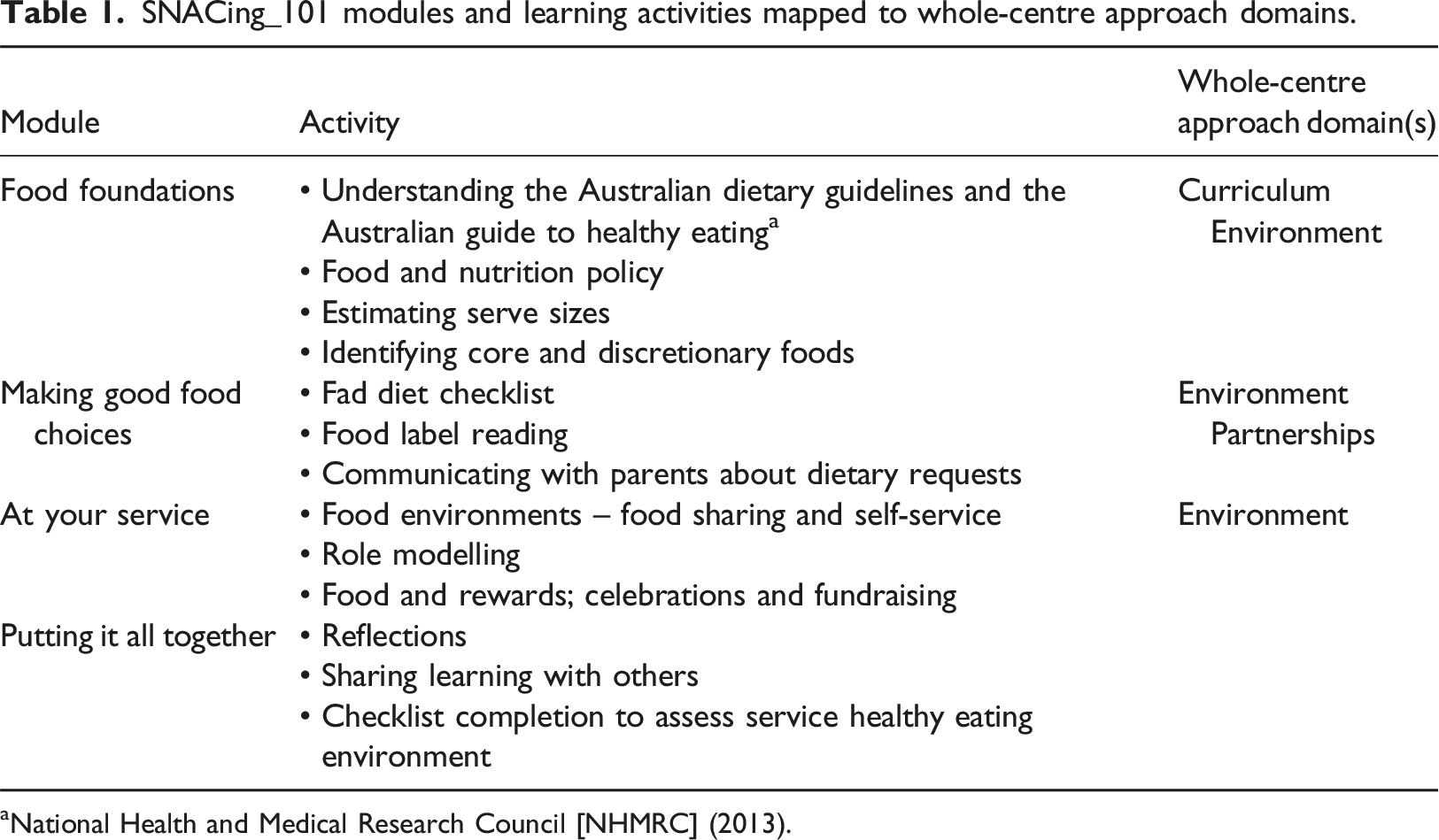
Evidence-based content was developed by nutrition experts and learning designers at Edith Cowan University to ensure the training was pedagogically sound and pitched at the appropriate educational level. The short course followed a ‘whole-service-approach’, based on the Health Promoting Schools Framework (Gillies et al., 2011), with three interrelated components: curriculum; environment; and partnerships (Figure 1). Within the curriculum domain, online nutrition-focused training was provided to enable professionals to incorporate nutrition knowledge into their teaching practice. The environment domain considered the physical and cultural aspects of ECEC settings, including food quality, attitudes towards healthy eating, role modelling healthy eating behaviours, and understanding Australian food and nutrition guidelines. Finally, partnerships examined relationships between professionals, children and parents/caregivers. Whole-service-approach to healthy eating in early childhood education and care used to frame ‘SNACing_101’ (adapted from the Health Promoting School Framework).
SNACing_101 modules and learning activities mapped to whole-centre approach domains.
In July 2018, recruitment emails were sent to all Australian ECEC services (n = 7,826) identified through publicly available lists (ACECQA, 2023) and through our existing networks. Eligible participants were ECEC professionals aged over 18 years. Participants were allocated to intervention or control groups using a simple computer-generated randomisation list, with only the research assistant aware of allocations. During October 2018, intervention participants completed the pre-survey, the course and post-survey, then received a certificate of completion and a $30 gift card. Control participants completed the same survey twice, one month apart, and were then provided with access to the course (November, 2018) and entry into a draw to win one of four $50 gift cards. Assuming a two-sided significance threshold of α = 0.05, a standardised mean difference of d = 0.5 and retention rate of 90%, the target sample size was calculated to be 69 participants per group to achieve a statistical power of .8 (Lu et al., 2008).
The survey, administered electronically via Qualtrics (2023), was designed to capture nutrition knowledge based on the Australian Dietary Guidelines (NHMRC, 2013), attitudes toward healthy eating, food provision at their workplace, confidence, role legitimacy and adequacy and, for intervention participants only, the useability and likeability of the online short course. Devine et al. (2019) provides the survey design, validity and scoring details.
Data analysis was performed using R version 4.1 (R Core Team, 2021). Demographic comparisons between control and intervention groups were conducted using chi-square or Fisher exact tests, as appropriate. Linear mixed effect modelling was used to determine any statistically significant differences in confidence, and role legitimacy and adequacy, between and within control and intervention groups. Generalised linear mixed-effect models were used to assess changes in knowledge. Group membership and time were treated as fixed effects and individual participants as random effects. Linear modelling assumptions were checked by inspecting residual plots.
Results
Demographic data are followed by survey results, organised according to the three course modules (Table 1).
Demographic data
Participant demographic profile.
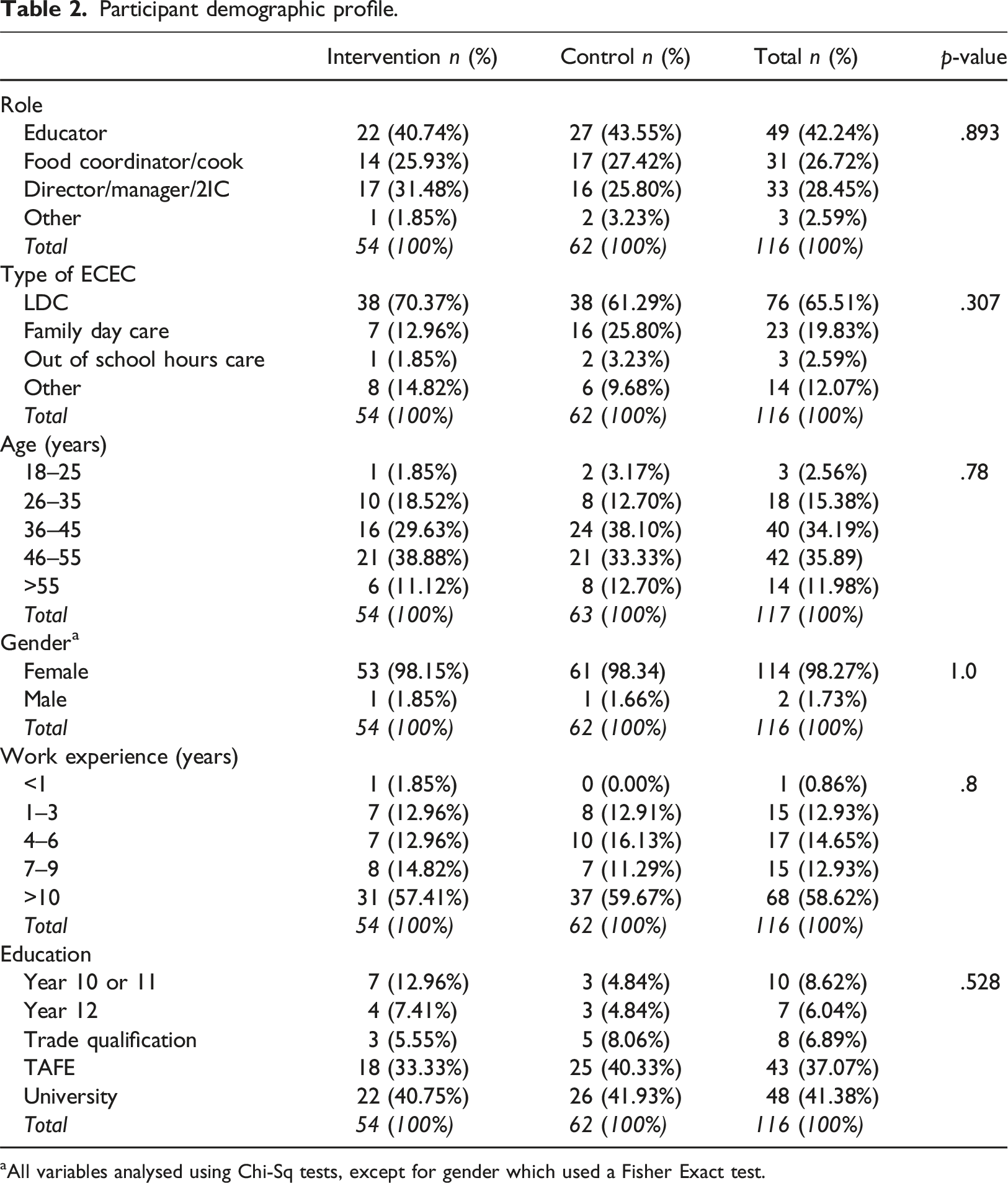
aAll variables analysed using Chi-Sq tests, except for gender which used a Fisher Exact test.
At the time of the survey, commercial companies delivering pre-prepared food to ECEC services was rare. Thus, food provision in these results relates to food prepared on site. Almost 80% of participants reported their service provided some or all food for children. Nearly all participants reported they made a conscious effort to provide healthy food all or most of the time, but approximately 20% (n = 23) felt the food was not healthy enough.
Food foundations
Participant confidence in menu meeting core food recommendations.
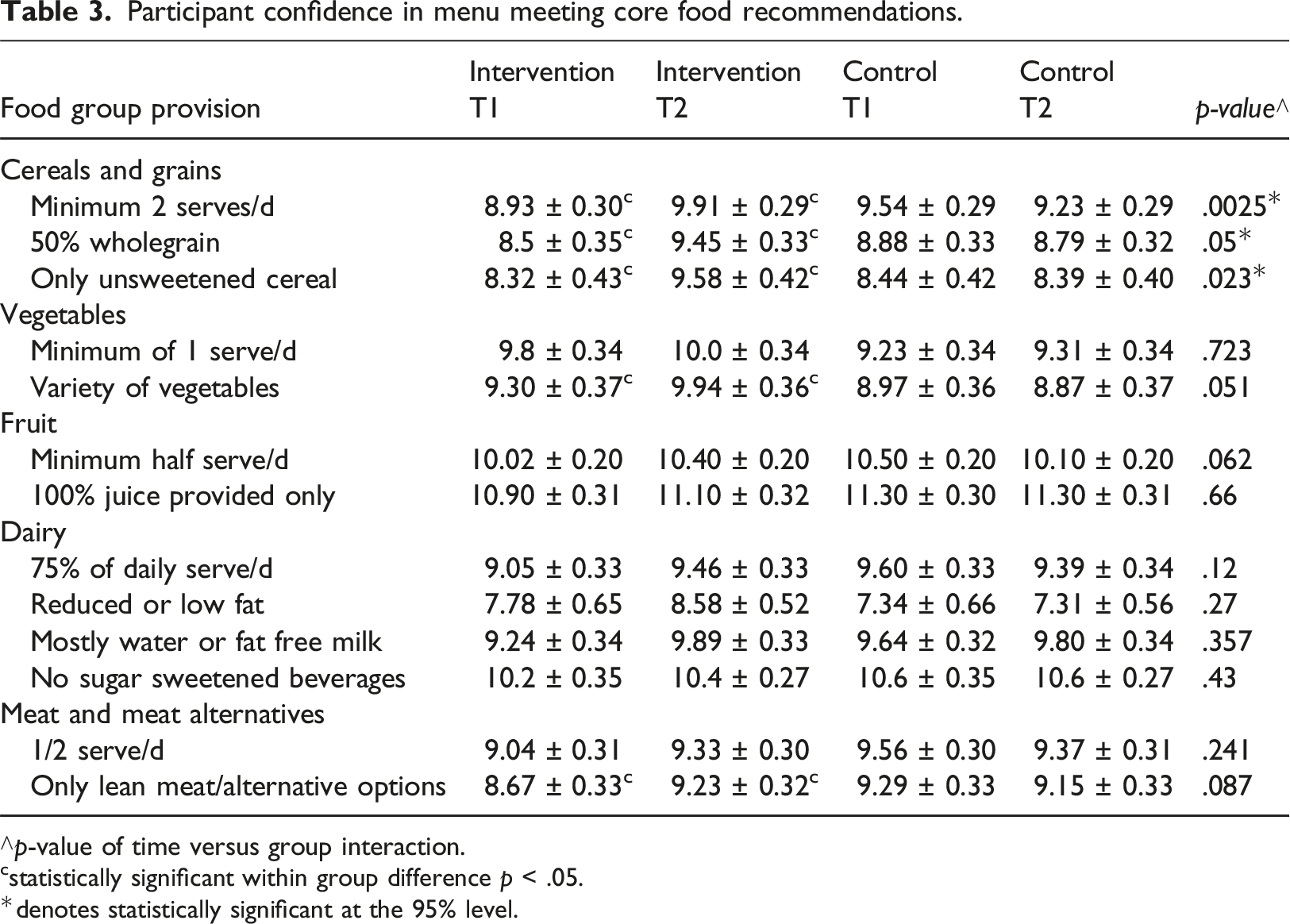
∧p-value of time versus group interaction.
cstatistically significant within group difference p < .05.
*denotes statistically significant at the 95% level.
Statistically significant improvements were observed for participant confidence that the menu provided the recommended serves of cereal/grains, vegetables and meat/meat alternatives food groups (NHMRC, 2013).
Participants rated their confidence on a scale of 0 (strongly disagree) to 6 (strongly agree) when estimating the recommended food serve sizes for children (NHMRC, 2013). A statistically significant difference in confidence was observed between groups over time (p = .001). Intervention group confidence scores increased by an average of 0.94 (95% CI 0.59, 1.29), while no change was detected in the control group.
Participant knowledge of core food serve sizes.
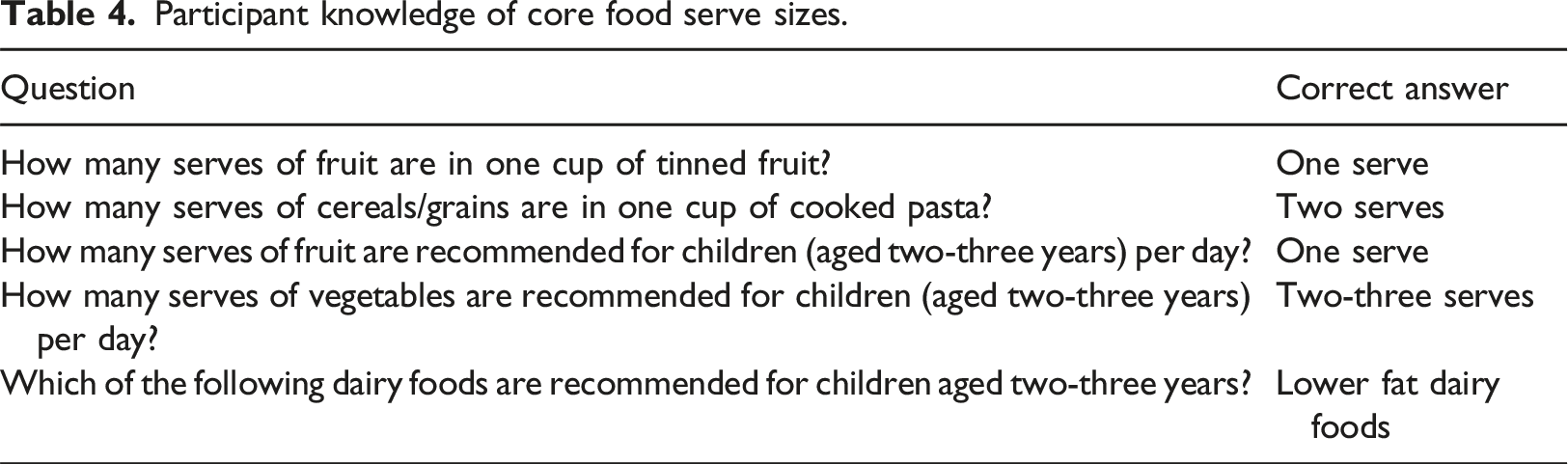
Participants answered a series of questions about fat, saturated fat, sugar, sodium, protein and fibre content of specific foods, selecting response options: high, low or unsure. Overall, knowledge about foods containing added sugar and fat was high across both groups and time points. Concerning sodium, the only statistically significant difference between groups related to sausages (p = .0082). Despite an increase in knowledge about sodium content among intervention participants (p = .013), they did not correctly identify cheese (42%), peanut butter (21%) and bread (82%) as typically high sodium foods. There was no difference in knowledge about protein or high-fibre foods between groups or time points. For saturated fatty acids, knowledge about salmon (a food low in saturated fat) changed significantly between groups (p = .0057). Among intervention participants, no change was detected, but control participants exhibited a decrease in knowledge (p = .01). Participants were asked to identify the healthiest choices for a variety of children’s snacks and meals. No differences were detected between groups and time points. Only half the intervention participants (50.9%) correctly identified a whole fresh orange as the healthiest snack when choosing from strawberry yogurt, muesli bar, and crackers and cheese.
Food package label information use.
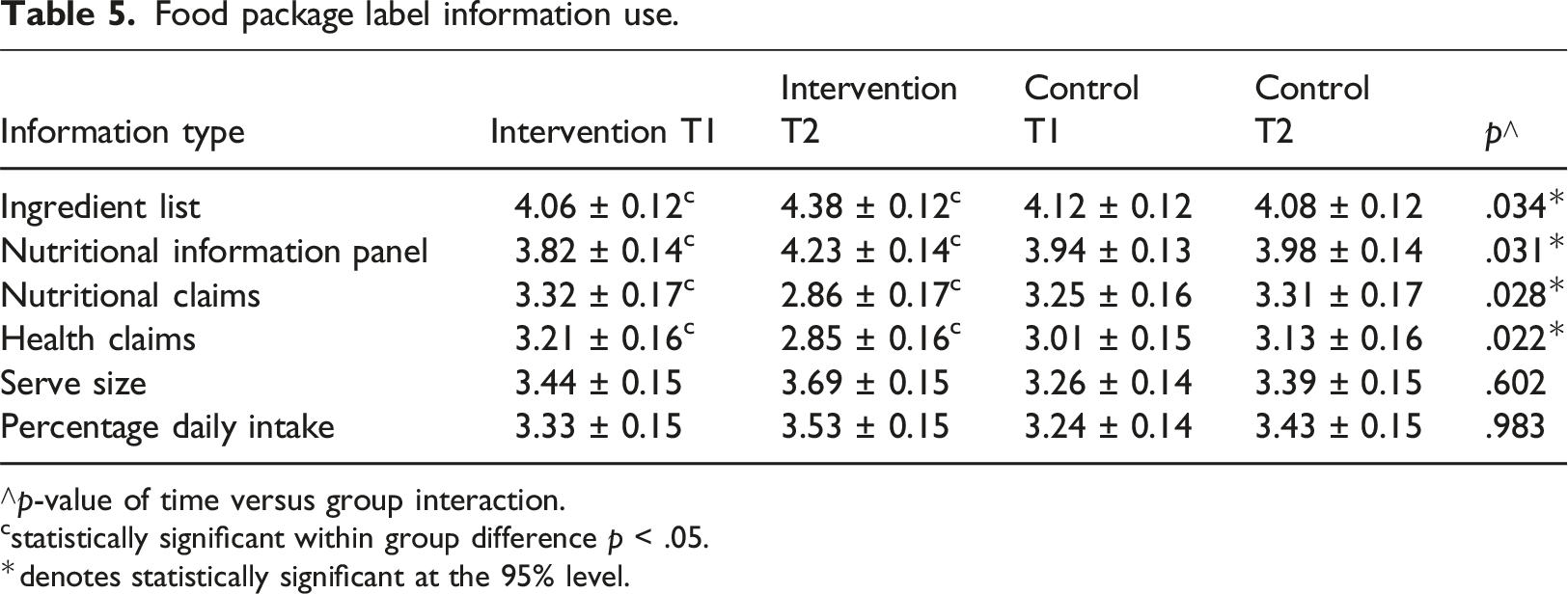
∧p-value of time versus group interaction.
cstatistically significant within group difference p < .05.
*denotes statistically significant at the 95% level.
Making good food choices
Participants ranked their confidence (1 = not at all; 12 = totally) to make nutritional recommendations to parents around limiting unhealthy snacks and drinks with added sugar, eating low-sodium foods, avoiding solid fats and eating lean meats/poultry. Both groups reported between 60%–80% confidence in making these dietary recommendations to parents. Statistically significant differences were observed between the groups over time for eating low sodium foods (p = .022) and avoiding solid fats (p = .0005). The intervention group showed an average increase of 1.03 (95% CI 0.26, 1.81) in the former and 1.43 (95% CI 0.64, 2.22) in the latter.
Perceptions of role legitimacy and adequacy.
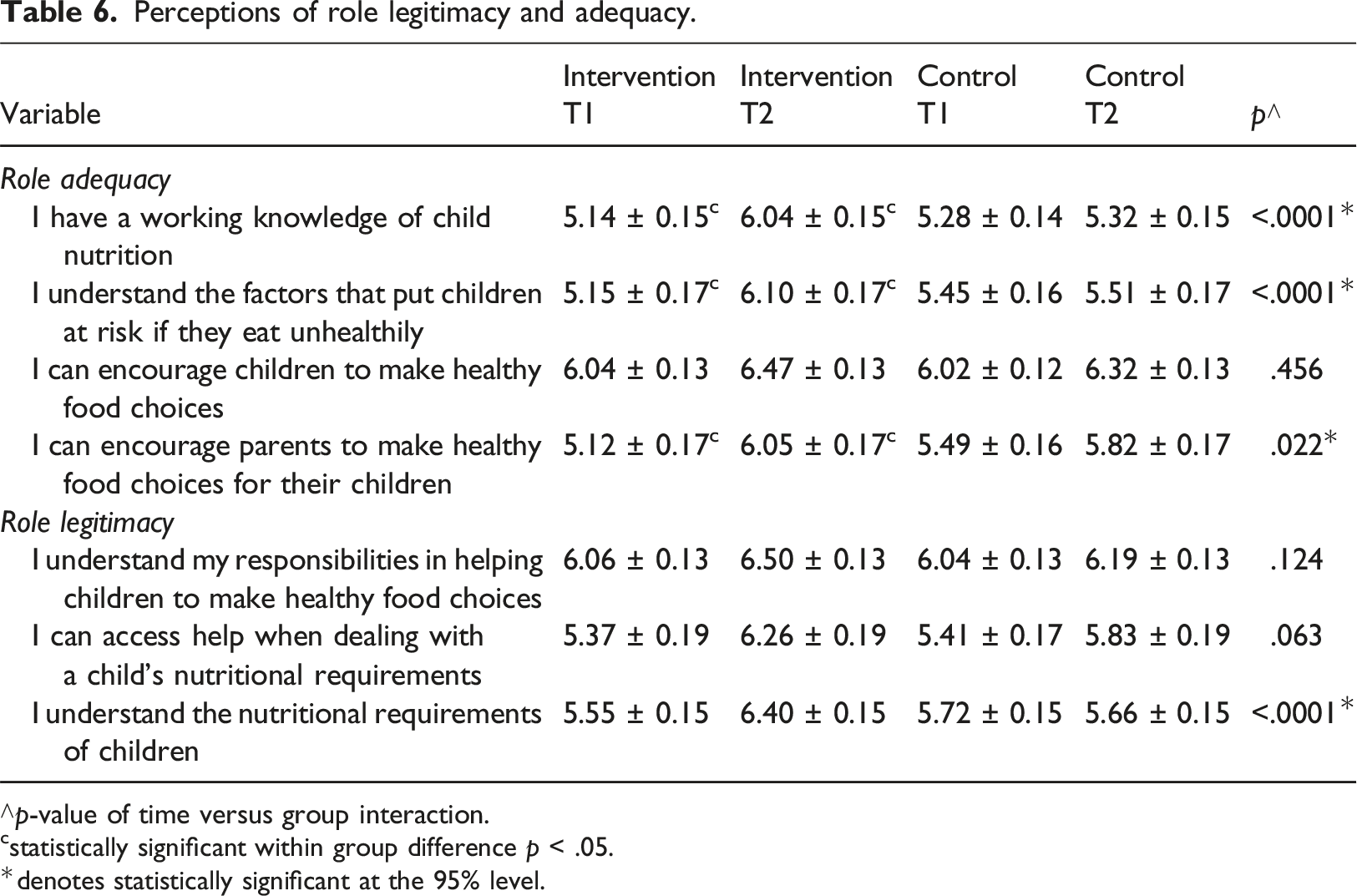
∧p-value of time versus group interaction.
cstatistically significant within group difference p < .05.
*denotes statistically significant at the 95% level.
There was a positive effect on three of the four role adequacy indicators for the intervention group (Table 6). For role legitimacy, only one indicator, understanding the nutritional requirements of children, was statistically significant between time and group (Table 6).
Food choices made for children.
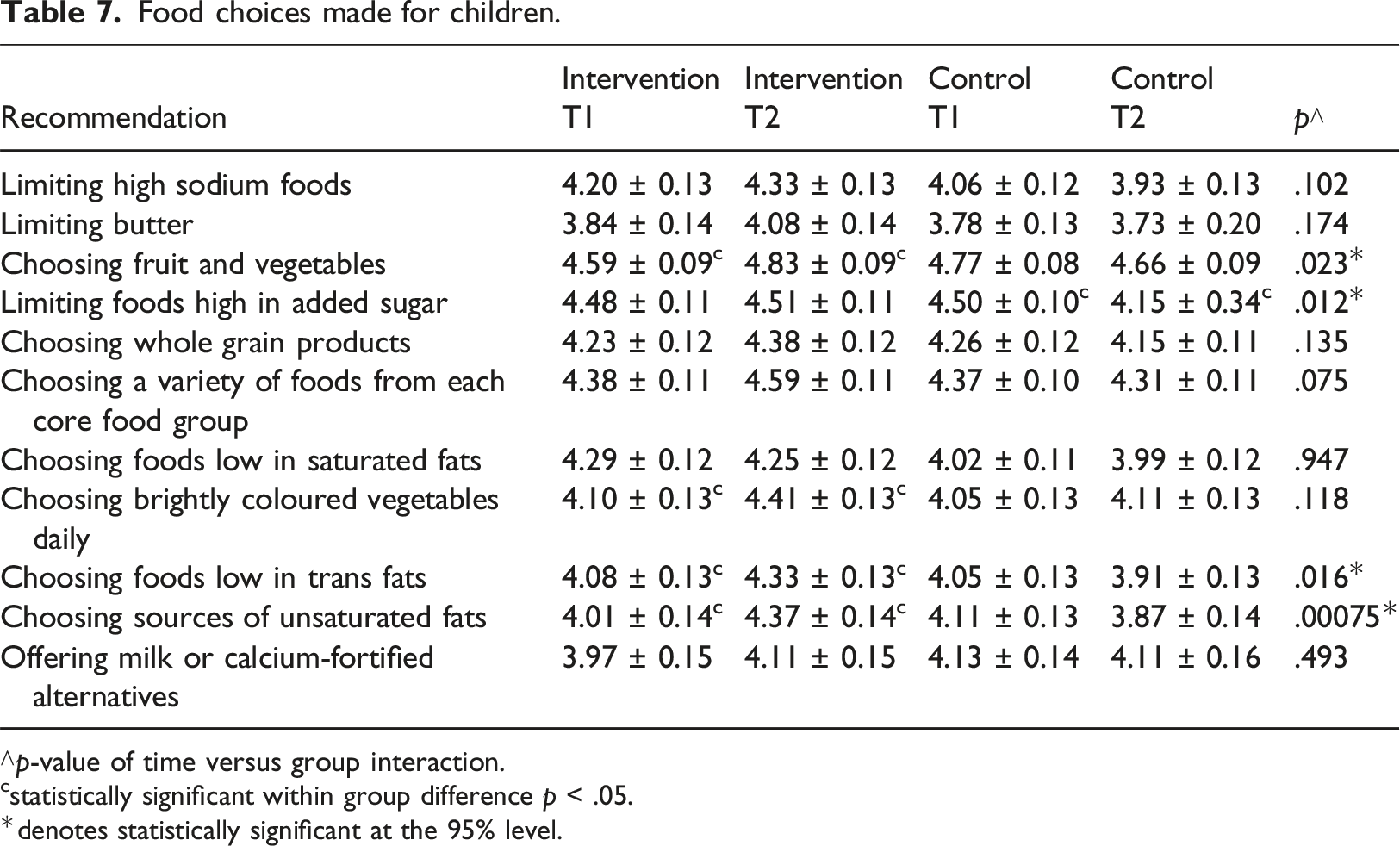
∧p-value of time versus group interaction.
cstatistically significant within group difference p < .05.
*denotes statistically significant at the 95% level.
At your service
Participant beliefs about healthy eating and food choices.
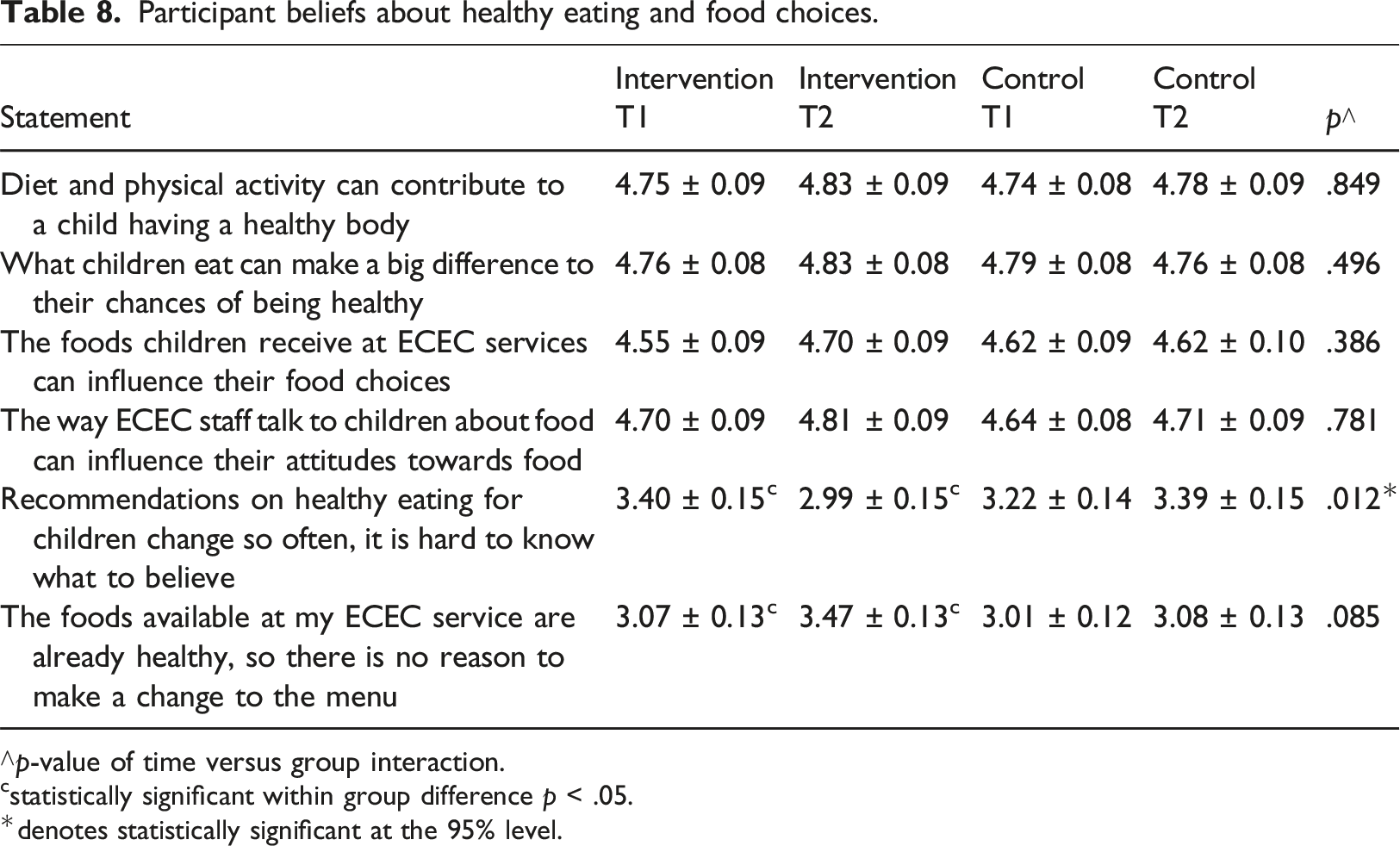
∧p-value of time versus group interaction.
cstatistically significant within group difference p < .05.
*denotes statistically significant at the 95% level.
Post-course completion, intervention participants rated the useability and likeability of the online short course, from 1 (Strongly disagree) to 7 (Strongly agree). Most reported the course was engaging (>90%), adequate (>92%) and easy to understand (94%). The downloadable resources were deemed informative by 98% of respondents, 90% felt that the course improved their confidence in making changes at their service and 94% believed it enhanced their nutrition knowledge.
Discussion
This study demonstrated that an online short course could improve ECEC professionals’ role adequacy and legitimacy, confidence to make dietary recommendations to parents and ability to understand food packaging labels. However, high levels of confidence contrasted apparent gaps in nutrition knowledge, highlighting the need for multilevel approaches to ensure healthy eating environments are promoted at services. This discussion is organised according to the three course modules.
Food foundations
No statistically significant changes were seen in nutrition knowledge for either group. Almost half of the intervention group did not correctly identify the recommended serves of core foods for children and were unable to identify the ‘healthiest’ snack, indicating a lack of understanding regarding the key nutrient content of foods/meals (Bhawra et al., 2023). These findings are consistent with a previous study that provided online nutrition curriculum resources to ECEC professionals (Devine et al., 2019). Kang (2016) suggests professionals may require repeated sessions over time to enhance learning outcomes, memory retention, problem-solving skills and the transfer of learning to new contexts. Furthermore, a moderated online community of support in addition to online nutrition curriculum resources (Devine et al., 2019) as part of a multilevel strategy, could better support healthy eating at ECEC services (Wallace, 2016).
Despite gaps in nutrition knowledge, participants demonstrated high levels of confidence regarding core food provision and estimation for children, highlighting disparities in these professionals’ knowledge, confidence and practices. This finding aligns with Devine et al.’s (2019) study, which reported a concerning lack of knowledge among ECEC professionals about the nutritional requirements of young children. Wallace and Mills (2019) similarly reported poor nutrition knowledge among family daycare educators about core food serve sizes for children. Wallace (2016) also noted high levels of participant confidence around the provision of food that meets nutrition guidelines for children after receiving nutrition education, which did not align with participants lower levels of nutrition knowledge.
A lack of nutrition knowledge (and potentially overconfidence in their skills) may result in the provision of food that does not meet nutrition guidelines – as reported elsewhere (Yoong et al., 2014) – impacting children’s weight status and risk of chronic disease (Wood et al., 2020). Nutrition is a complex topic and we cannot expect ECEC professionals to be nutrition experts (Boyd, 2015). Therefore, we should consider a range of options to embed nutrition education, like support from a ‘mentor or nutrition specialist’ (Kirkegaard et al., 2023), and implement these multilevel and holistic approaches (Wallace, 2016) to address complex health issues (Forde et al., 2021).
Regarding food label reading, findings indicated intervention participants relied on credible ingredient lists and nutrition information to make healthy food choices for children, rather than manufacturers claims about nutrition and health, highlighting the value of the course to teach professionals how to discern credible nutrition information. This finding is important because previous research showed that ECEC professionals searched the internet even though they acknowledged the validity and reliability of the information sourced could not be assured (Wallace et al., 2017b). Therefore, the inclusion of evidence-based resources to build sound nutrition knowledge should be a basic feature in any nutrition education and training.
Making good food choices
Participants reported confidence in making dietary recommendations to parents about their children’s food choices, particularly for foods containing sodium and solid fat. However, they demonstrated a lack of knowledge about high sodium foods. This knowledge gap has implications for the nutritional quality of foods offered at ECEC services and the potential accuracy of information provided by ECEC professionals to parents. Given reports that children consume 38.5% of their daily energy needs from discretionary foods (often high in sodium) that could impact their long-term health (Jakobsen et al., 2023), this finding is concerning and underscores the need for ongoing ECEC professional nutrition education.
For role adequacy, participants demonstrated a significant increase in confidence regarding nutrition knowledge, awareness of the health risks of unhealthy diets for children and confidence to encourage parents to make healthy choices for their children. For role legitimacy, there was a significant improvement in participants understanding children’s nutritional requirements. These findings show that online nutrition education, just like face-to-face (Branscum & Sharma, 2012; Forde et al., 2021), can increase the role adequacy and legitimacy of ECEC professionals. Importantly, online education may be more feasible for the ECEC workforce than face-to-face, and could enable scalability, which aligns with Love et al.’s (2020) recommendation for systemic, rather than individual level change, potentially also at a reduced cost for the sector.
Participants responses showed statistically significant improvements in choosing plenty of fruit and vegetables and limiting foods high in added sugar (Table 7), suggesting the course had a positive effect on participants’ awareness of healthy food choices. There were, however, no statistically significant changes in the reported provision of discretionary foods typically high in sugar and saturated fat, despite the course emphasising avoiding such foods as stipulated in the National Quality Standards (ACECQA, 2017, 2023), which align with the Australian Dietary Guidelines (NHMRC, 2013). These guidelines advocate for menu planning that excludes discretionary foods and includes core foods in each meal. Considering the impact of discretionary foods on overweight/obesity prevalence among Australian children (Jakobsen et al., 2023) and the influential role of ECEC services in shaping eating preferences (Walker & Littlewood, 2018), these findings highlight an urgent need to challenge professionals’ existing beliefs and practices regarding discretionary foods. As the cost of quality food provision is related to the use of discretionary foods at ECEC services (Sambell et al., 2020), financial support could help reduce food insecurity, while also improving child developmental outcomes (Thorpe et al., 2022). As Spence et al. (2020) suggest, policy changes may need to be promoted across organisational and governmental levels to help create enabling environments for healthier food practices, in addition to supporting services to develop and implement sound nutrition policy (Kirkegaard et al., 2024).
At your service
Overall, participant beliefs about establishing a healthy eating environment at their services scored positively. Only one statement, recommendations on healthy eating for children change so often, it is hard to know what to believe, showed a statistically significant difference between time and groups. This finding corroborates with a previous study (Devine et al., 2019) in which educators expressed similar concerns about recommendations being “changeable and hard to follow” (p. 10). Confusion could be attributed to the different ECEC nutrition guidelines present across Australian jurisdictions, which also creates challenges for service accreditation, resource provision and support (Spence et al., 2020). As such, nutrition experts have called for the harmonisation of nutrition guidelines to ensure consistent support and education is available across Australia. Implementing such changes would reduce confusion and encourage healthy eating environments, while enabling ECEC professionals to work across jurisdictions without the need for additional training.
Strengths and limitations
Participants were randomly allocated to either group, with outcomes measured, ensuring methodological rigour (Wagle, 2018). Recruitment based on participant interest in healthy eating minimised selection bias. However, there was potential for participant bias. For example, participants may have joined the study to improve their nutrition knowledge and, thus, were motivated to learn, while others with entrenched habits and paradigms may have opted not to participate, potentially influencing the results. The extent of self-selection bias and its impact on generalisability should be carefully considered when interpreting the findings, as well as the relatively small sample size compared to the sampling frame and power calculation.
In addition, there is variation in how food is provided at ECEC services across Australia (National Nutrition Network - Early Childhood Education and Care, 2022). For example, some services prepare food on the premises, while others request food from parents, potentially influencing participants’ responses. More recently, it has become increasingly common for services to source food from a commercial catering company, so researchers must consider the sources of food provided at services when designing studies. We did not collect data on how the food was sourced because commercial sources were uncommon at the time of this study.
While the online course included nutrition policy information in Module 1, this was brief, and we did not test participants’ knowledge of nutrition policy in the pre and post surveys. Given that Lum’s (2023) review found only 37% of 523 participating ECEC services reported fully implementing nutrition policies, and system-wide change is recommended (Love et al., 2020), future nutrition education interventions in ECEC settings should include learning activities about nutrition policy, measuring participants understanding and assessing their ability to apply policy across all aspects of their practice (Kirkgaarde et al., 2024), as per the Health Promoting Schools Framework (Figure 1).
Conclusion
This study followed recommended best practices (Matwiejczyk et al., 2018) by developing and testing a comprehensive online short course, called ‘SNACing_101’, specifically designed to help ECEC professionals promote healthy eating across all aspects of their service - curriculum, partnerships and environment (Gillies et al., 2011).
Our findings demonstrate that online training can be effective (just like face-to-face) as positive outcomes were seen for some aspects of participants’ nutrition knowledge, their confidence in making recommendations to parents and awareness of their responsibilities in child nutrition. However, participants’ variable knowledge regarding the specific nutrition content of foods/meals highlights that training should target potential misconceptions and preconceived ideas, in addition to providing specific details about nutrition content of commonly used foods/meals. We also raised the issue of incorporating nutrition policy into education and, subsequently, enforcing it in practice, preferably supported by a harmonsed national approach.
Considering the complexity of nutrition topics, it is not surprising that one three-hour course could not address all misconceptions and knowledge gaps. Thus, it is important to explore how comprehensive training can be delivered across all levels of ECEC and embedded across each professionals’ career as part of their ongoing development to ensure enduring improvements to knowledge and practice. While such training options may present challenges, especially in an overcrowded ECEC agenda (Kirkegaard et al., 2023), the substantial influence of nutrition on child growth, development and future outcomes necessitates prioritising such strategies as part of a broader solution. Integrating child nutrition into ECEC tertiary education is also essential, given its integral role in a whole-service-approach and evidence that isolated, one-off programs yield limited impact (Yoong et al., 2023). It is vital to keep the needs of ECEC firmly in the sights of government and to advocate for multi-level solutions to enhance professionals’ nutrition knowledge, role adequacy and legitimacy. By doing so, we can work toward ensuring healthier environments for young children and better overall future health outcomes.
Footnotes
Acknowledgements
Ainslie Sartori (Research Assistant).
Author contributions
Ruth Wallace: Conceptualization, Funding Acquisition, Investigation, Methodology, Project Administration, Writing – original draft; Ros Sambell: Conceptualization, Funding Acquisition, Methodology, Writing – review and editing; Shih Ching Fu: Formal analysis, Validation, Writing – review and editing; Johnny Lo: Formal analysis, Validation, Writing – review and editing; Elizabeth J. Cook: Visualisation, Writing – review and editing; Amanda Devine: Conceptualization, Funding Acquisition, Investigation, Methodology, Supervision, Writing – review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Edith Cowan University Early Career Researcher Grant G1003434 awarded to Dr. Ruth Wallace (lead author).