
Abstract
Stress, an inevitable aspect of human existence, triggers complex physiological and behavioral responses aimed at maintaining internal equilibrium. It requires a multifaceted understanding encompassing its physiological, pathophysiological, and behavioral dimensions to inform effective treatment approaches. This narrative literature review attempts to understand the evolution of research on stress, from its historical roots to current physiological, pathophysiological, and conceptual understandings. Pathophysiological consequences of chronic stress, including cardiovascular disease and immune system dysregulation, highlight the need for comprehensive prevention and intervention strategies. The results demonstrate the importance of adopting a holistic approach to stress management, combining pharmacological interventions with psychological therapies such as cognitive-behavioral therapy and other third-wave approaches. For chronic stress, long-term strategies focusing on lifestyle modifications, social support, and coping skills enhancement are recommended, whereas acute stress may benefit from immediate pharmacological interventions to mitigate physiological arousal and promote relaxation. The review results also indicate the significance of the biopsychosocial framework in understanding stress by acknowledging its multifaceted nature, emphasizing the effectiveness and sustainability of diverse intervention strategies, and highlighting the role of societal factors in shaping stress experiences and treatment outcomes. Further research is warranted to clarify the mechanisms underlying stress responses and refine intervention strategies for optimal efficacy and sustainability.
Keywords
Introduction
Stress is an intrinsic characteristic of life that individuals encounter regularly, which includes a diverse range of physical, psychological, and contextual consequences. Its origins trace back to the fundamental need for organisms to maintain balance in their internal environment, a concept explicated as homeostasis by Claude Bernard. Stressors are factors that can disrupt this equilibrium and vary widely, ranging from acute stressors such as the fright of nearly having a serious accident to chronic stressors such as prolonged emotional strain. Stress manifests in response to various stimuli, including physical harm, biochemical imbalances, and exposure to pathogens (Charmandari et al., 2005). Initially, the stress response is adaptive by activating resources to confront the challenges posed by stressors, such as trauma or surgery, in order to alleviate further damage (Mifsud & Reul, 2018). However, by exposure to acute stressors that are repetitive (as in repeated acute stress) or prolonged (as in chronic stress), the stress response can become maladaptive, leading to detrimental impacts on physiology. Chronic stressors, in particular, can provoke maladaptive responses such as depression, anxiety, cognitive impairment, and cardiovascular diseases (Alexander et al., 2007; Beversdorf, 2019; Ketchesin et al., 2017).
As the field of stress research continues to expand, it has become increasingly apparent that the conventional conceptualization of stress presents significant threats. The developing volume of literature demonstrates the need for a critical reassessment of how the stress concept is traditionally employed and understood. As research progresses, it becomes obvious that the conventional understanding of stress may not fully capture its multidimensional nature or adequately address its complications for human health and well-being. Refining our understanding of stress could provide more refined perspectives, thereby facilitating more effective approaches to research, assessment, and intervention in this critical domain. While existing reviews have studied stress mechanisms and consequences (Koolhaas et al., 2011; Robinson, 2018; Romero, 2004; Ulrich-Lai & Herman, 2009), there are limited studies comprehensively examining diverse aspects of stress by providing updated views on recent developments. Specifically, there remains a significant gap in the literature regarding a comprehensive review that synthesizes current knowledge on diverse aspects of stress, from physiological mechanisms to psychological consequences. Addressing this gap is essential for advancing our understanding of stress and informing evidence-based intervention strategies.
This narrative literature review is an attempt to offer a comprehensive overview of research development and understanding of the multifaceted nature of stress by exploring its physiological foundations, pathophysiological consequences, and behavioral manifestations, as well as assessment, prevention, and intervention strategies. By synthesizing existing literature, this narrative review aims to bridge the gap in understanding stress from diverse and interdisciplinary perspectives. The synthesis of the findings can contribute to identifying critical gaps in current knowledge and provide insights into the complex interactions between diverse factors influencing stress. Thus, this review aims to inform future research directions and clinical practices for managing stress effectively, eventually contributing to the advancement of more targeted and holistic prevention and treatment programs that address both the root causes and manifestations of stress. In brief, this review has the potential to guide interdisciplinary approaches to stress management, promoting collaboration among researchers, clinicians, and policymakers to increase overall well-being.
Method
A thorough literature search was performed across multiple electronic databases, including PubMed, PsycINFO, and Web of Science. The search approach employed a combination of keywords related to stress physiology (i.e., stress, cortisol, hypothalamic–pituitary–adrenal axis, allostasis, sympathetic nervous system, stress biomarkers, adrenaline/epinephrine), stress response mechanisms (i.e., acute stress, chronic stress, homeostasis, behavioral responses to stress, stress adaptation, coping mechanisms, resilience), psychopathology (i.e., stress-induced psychopathology, anxiety, depression, burnout, post-traumatic stress disorder), and treatment interventions (i.e., cognitive-behavioral therapy [CBT], mindfulness-based stress reduction, resilience training, stress management, pharmacotherapy, psychotherapy, psychoeducation). We applied logical operators (i.e., “AND” and “OR”) to combine search terms, with searches limited to articles published in English. The search results almost yielded 3,800 research papers across the specified databases and keywords. We followed specific inclusion criteria to choose research studies investigating physiological mechanisms of stress, pathophysiological consequences, assessment strategies, prevention and intervention approaches, or the biopsychosocial framework of stress management. We excluded research studies lacking relevance to human stress physiology, studies without full-text availability, and non-peer-reviewed sources. Additionally, studies using animal models, reporting clinical trials, exploring molecular mechanisms, observational studies, and narrative reviews were considered. After removing duplicates and the screening titles and abstracts of the papers, we did a more detailed evaluation of methodological rigor and relevance to the study aims, which led to the final 134 research papers framing the results of this narrative review.
We attempted to extract the relevant data from included research studies with the following outline: information on stress-response pathways, physiological markers of stress, pathophysiological consequences of chronic stress, assessment methods, and intervention strategies. By synthesizing the extracted data, we attempted to offer a thorough picture of the physiological mechanisms underlying stress responses and their implications for health and illness. After spotting core themes and findings, as well as analyzing commonalities and discrepancies across studies, a coherent narrative review was developed.
Utilizing relevant criteria adapted from the established guidelines for narrative reviews (Green et al., 2006), we attempted to evaluate the quality of the included research studies based on the clarity of research objectives, methodological rigor, appropriateness of statistical analyses, and relevance to the study aims. Specifically, we examined the robustness of their research design, along with the validity and reliability of their measurement tools. To ensure a comprehensive assessment, the transparency of reporting and the replicability of the findings were also considered. While every effort was made to perform a thorough literature search and synthesize findings accurately, this review may be subject to publication bias due to including studies published only in English. Additionally, the complexity of stress physiology and the breadth of the literature may have resulted in some relevant studies being overlooked. Nevertheless, the authors aimed to enhance the credibility and reliability of the findings presented in this review by following quality-assessment criteria.
History of stress
Stress has long been a deep focus in neuroscience, with foundational contributions dating back to the late 19th century. Renowned French biologist Claude Bernard highlighted the importance of preserving internal equilibrium, or homeostasis, in the face of external challenges (Bernard, 1865; Cannon, 1929). Bernard noted that the body continuously works to maintain a steady, balanced interior environment. In particular, he identified the part of the nervous system that controls blood-vessel dilatation and constriction in response to internal temperature fluctuations. He is often considered the founding figure in experimental medicine. Although Claude Bernard pioneered the systematic exploration of regulatory mechanisms aimed at stabilizing the internal environment, it was not until Walter Cannon’s additional contributions to these processes that Bernard’s ideas gained wider recognition and appreciation.
Walter further underscored the vital role of the autonomic nervous system in establishing and preserving homeostasis, asserting that any inclination toward change is countered by the augmented effectiveness of the factors that oppose the change. Despite its significance in physiology and medicine, homeostasis was initially conceptualized as an entirely automatic process, remaining distant from the psychological notion of stress (Robinson, 2018). Combining his theory of emotion with his theory of homeostasis, Cannon advanced beyond investigating the physiological responses to physical emergencies and psychological stress. In the second edition of his book Bodily Changes in Pain, Hunger, Fear, and Rage, he proposed that the release of adrenaline (epinephrine) into the bloodstream serves multiple adaptive functions, enabling an organism to react to acute stress by preparing for fight or flight. He observed that adrenaline’s release exerts distinct effects on the body’s organs, collectively aiding in the maintenance of homeostasis.
While Cannon examined intense stress responses without explicitly using that term, Hans Selye observed distinct responses to chronic stress (Robinson, 2018). Building upon previous work, Hans Selye, an Austrian-American scientist, introduced the term “stress” and defined it as any threat that disrupts homeostasis. Selye’s (1956) seminal research laid the grounds for understanding stress as a physiological response to various stressors, including both physical and psychological stimuli. Selye successfully identified and isolated several hormones central to the stress response, with a particular emphasis on glucocorticoids (Selye, 1943). Through extensive investigation, Selye clarified that both humans and animals indicate similar physiological responses to stressors, including behavioral changes and activation of the endocrine and neuroendocrine systems (Carrasco & Van de Kar, 2003; Charmandari et al., 2005). His foundational research on the impact of chronic stress on the hypothalamic–pituitary–adrenal (HPA) axis paved the way for contemporary investigations into the causal link between chronic stress and HPA-axis hyperactivity (Robinson, 2018). Also, his pioneering work marked the scientific exploration of stress, establishing it as a multidimensional phenomenon with significant implications for health and well-being (Lupien et al., 2007).
Richard Lazarus was among the first to challenge Hans Selye’s general adaptation syndrome (GAS) theory. Unlike behaviorists, Lazarus introduced cognition and subsequent emotions as significant factors in the behavioral response to a stimulus. In an effort to incorporate various aspects of psychological and environmental interactions, he developed the transactional model of stress (Lazarus, 1966), by identifying that there are primary and secondary appraisals. Lazarus further advanced the field of stress research by introducing the efficacy of coping as one of the mediators of stress. Lazarus pioneered a new exploration of stress research by introducing cognitive appraisals and coping strategies as mediators of emotional outcomes. His work expanded stress research to consider the complex interactions between stimulus, appraisal, and responses (Robinson, 2018). By the early 1980s, stress research had blossomed, incorporating a wide variety of approaches. Within psychology, stress research became integral to nearly every sub-discipline, leading psychologists to differentiate various types of psychological stressors, including those related to mental illness.
Physiological mechanisms of stress
Stress represents a holistic physiological reaction to several external stressors, ranging from physical threats to psychological challenges, aimed at preserving the body’s internal equilibrium (Bernard, 2013; Cannon, 1929; Selye, 1956; Carrasco & Van de Kar, 2003). In other words, any disruption in the body’s internal equilibrium, whether physical or psychological, causes a stress response, characterized by a series of physiological and behavioral modifications. This intricate response mediated by a complex interaction of neurological, endocrine, and immunological processes is required for enhancing organismal survival by restoring balance within the internal context (Carrasco & Van de Kar, 2003). Activation of stress responses initiates the engagement of multiple key physiological systems, such as the sympathetic–adreno–medullary (SAM) axis, the HPA axis, the renin-angiotensin system (RAS), the immune system, and the autonomic nervous system (Carrasco & Van de Kar, 2003; Herman et al., 2003; Mifsud & Reul, 2018). Figure 1 represents the schematic demonstration of stress physiology. Notably, stress responses manifest in two different forms: (a) slower reactions predominantly mediated by the HPA axis and (b) fast reactions primarily mediated by the SAM axis (Schwabe et al., 2012). This dynamic interaction of physiological systems demonstrates the adaptive nature of the stress response, facilitating rapid adjustments to diverse environmental challenges (Bernard, 2013; Charmandari et al., 2005; Herman et al., 2003).
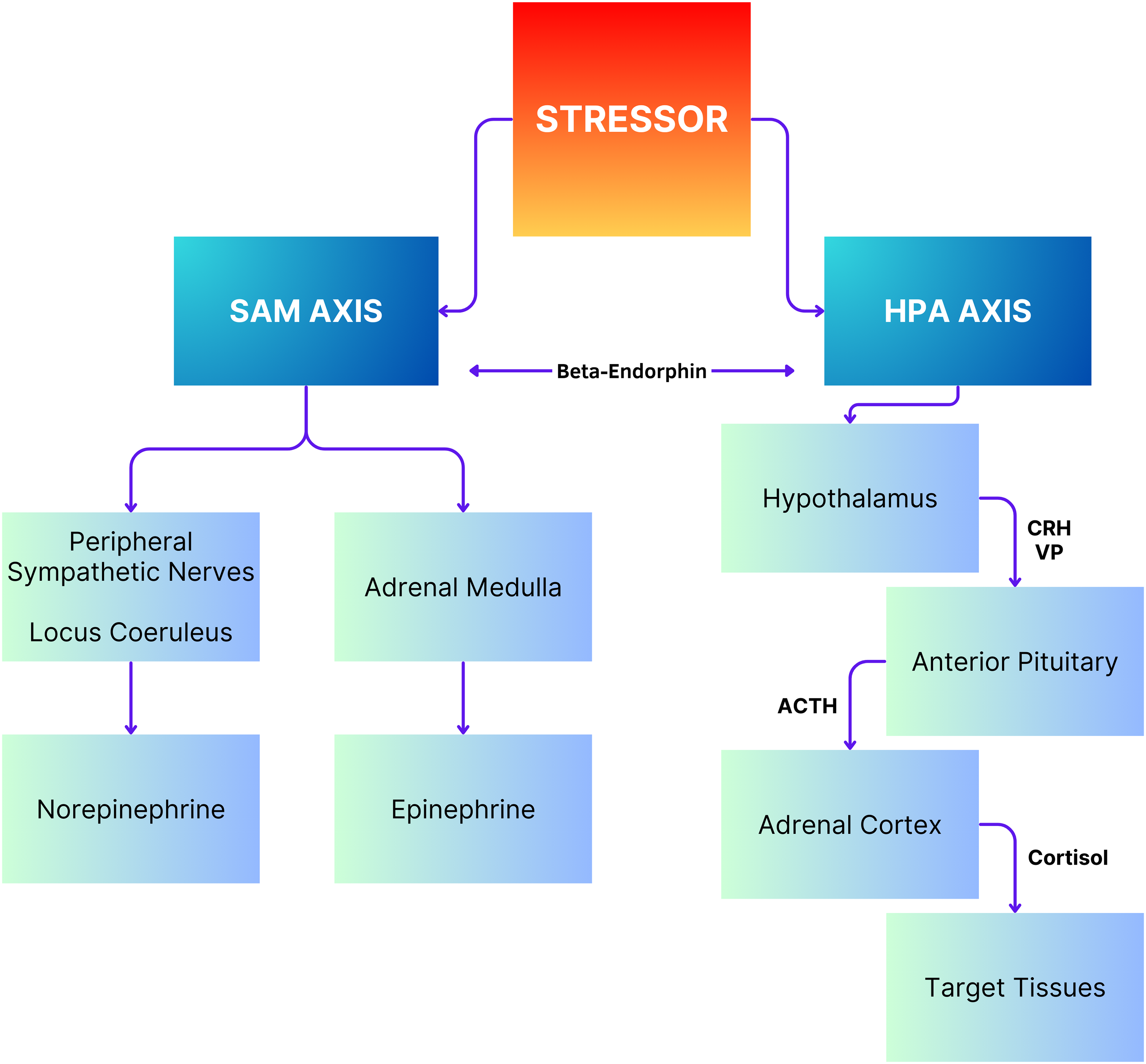
Schematic representation of stress physiology. Note: ACTH: Adrenocorticotrophic hormone; CRH: Corticotropin-releasing hormone; HPA: Hypothalamus-pituitary-adrenocortical; SAM: Sympathetic-adrenal-medullary; VP: Vassopresin.
Physiological stress responses
The slower response to stress is mediated by the activation of the HPA axis. The HPA axis organizes the body’s response to stress, comprising three key endocrine formations: the hypothalamus, pituitary (hypophysis), and adrenal glands (Tsigos & Chrousos, 2002; McCormick et al., 2010). Among these, only the adrenal glands possess a strictly endocrine structure. The hypothalamus manages the secretion of adrenocorticotropic hormone (ACTH) from the anterior pituitary by releasing corticotrophin-releasing hormone/factor (CRH or CRF) (Vale et al., 1981; Tsigos & Chrousos, 2002). In other words, the process of stress response begins with the release of CRH from the paraventricular nucleus of the hypothalamus into the circulation. The CRH released from the hypothalamus acts on two receptors: CRH-R1 and CRH-R2. While CRH-R1, which is widely expressed in the mammalian brain, serves as the key receptor for stress-induced ACTH release from the anterior pituitary, CRH-R2 is predominantly expressed in peripheral tissues, including skeletal muscles, the gastrointestinal tract, the heart, and subcortical structures of the brain. Cortisol-releasing hormone-binding protein (CRH-BP) demonstrates a higher affinity for CRH than its receptors and is expressed in diverse tissues such as the liver, pituitary gland, brain, and placenta (Westphal et al., 2005). Research studies confirming the role of CRH-BP as a controller of CRH bioavailability have found that CRH-BP binds 40 to 60% of the CRH present in the brain (Behan et al., 1995). During exposure to stress, the expression of CRH-BP increases in a time-dependent manner, likely serving as a negative-feedback mechanism to decrease the interaction of CRH with CRH-R1 (Ketchesin et al., 2017). Serum cortisol levels represent the total cortisol level in the body, with 80% bound to cortisol-binding globulin and 10% bound to albumin. Unbound cortisol is biologically active.
Acting as an enhancer, arginine-vasopressin (AVP) amplifies the stimulatory effect of CRH on ACTH secretion, although its individual impact is modest, suggesting a cooperative regulation with CRH (Tsigos & Chrousos, 2002). CRH and AVP, released from neurons within the parvicellular nuclei of the hypothalamus, cross axons to the median eminence, where they are released into the hypophyseal portal system’s first capillary network (Sawchenko, 1987). Within this network, CRH stimulates the anterior pituitary lobe to release ACTH and other biologically active substances, such as beta-endorphins (Grammatopoulos & Chrousos, 2002). In other words, following the release of CRH, the anterior pituitary gland is stimulated to release ACTH into the bloodstream. ACTH, in turn, prompts the adrenal cortex to secrete glucocorticoid hormones, including cortisol, into circulation. The inactive form of cortisol, cortisone, undergoes catalysis to its active form, cortisol, through the action of 11 beta-hydroxysteroid dehydrogenases.
In response to CRH binding, the synthesis of proopiomelanocortin (POMC) is triggered in the pituitary, serving as the key predecessor for biologically active peptides such as beta-endorphin and ACTH (Sawchenko, 1987). ACTH, circulating through the bloodstream, gets to the adrenal glands’ cortex, prompting the synthesis and secretion of adrenocorticosteroids (Cullinan et al., 1995; Sousa et al., 2014). The secretion pattern of CRH follows a circadian and pulsatile rhythm, with enhanced frequency and amplitude during stress states, ultimately elevating ACTH and cortisol levels (Cullinan et al., 1995). Different factors, including AVP, angiotensin II, and cytokines, modulate the HPA axis in reaction to diverse stressors (Tsigos & Chrousos, 2002).
As the third element of the HPA axis, the adrenal glands release glucocorticoids from their cortical layer, serving as the final effectors in stress responses (Sousa et al., 2014). Glucocorticoids play a crucial role in maintaining homeostasis and regulating stress responses, exerting a regulatory role in both basal HPA activity and stress termination. Negative-feedback mechanisms mediated by glucocorticoids limit the duration of exposure to these hormones, thereby mitigating their catabolic, anti-immune, and anti-reproductive effects (Tsigos & Chrousos, 2002). Glucocorticoids apply their effects through cytoplasmic receptors, which, upon hormone binding, translocate into the cell nucleus to change gene expression. This includes inhibiting transcription factors that are implicated in immunological responses. Additionally, glucocorticoids influence mRNA stability and protein synthesis, with both slow and relatively fast effects observed, suggesting the involvement of cell membrane receptors (Schumacher, 1990; Lupien & McEwen, 1997).
On the other hand, the fast reaction triggered by the activation of the SAM axis initiates a surge in the secretion of norepinephrine (NE) and epinephrine (E) from the adrenal medulla, as well as elevated NE secretion from sympathetic nerves and locus coeruleus (Carter & Goldstein, 2015; Giannakakis et al., 2019; Goldstein, 2010). This leads to elevated levels of NE in the brain, where these neurotransmitters interact with α-adrenergic and β-adrenergic receptors distributed throughout the central nervous system and on the cell membranes of various organs and smooth muscles (Kabir & Akter, 2023; Wong et al., 2012). Upon release, NE and E bind to specific membrane-bound G-protein receptors, initiating intracellular signaling pathways, particularly the cyclic-adenosine monophosphate (cAMP) pathway, which rapidly triggers cellular responses (Fuchs & Flügge, 2004). Activation of these receptors induces smooth and cardiac muscle cell contraction, resulting in vasoconstriction, increased blood pressure, heart rate, and cardiac output. Furthermore, it enhances blood flow to skeletal muscles while stimulating sodium retention, elevating glucose levels through glycogenolysis and gluconeogenesis, and stimulating lipolysis, oxygen consumption, and thermogenesis (Giannakakis et al., 2019; Jones et al., 2012). Furthermore, SAM activation results in reduced intestinal motility, cutaneous vasoconstriction, and bronchiolar dilation. Behaviorally, it prompts heightened arousal, alertness, vigilance, cognition, focused attention, and analgesia, collectively preparing the body for rapid and efficient responses to perceived threats or stressors (Giannakakis et al., 2019).
The RAS intricately regulates body fluids and electrolytes, responding rapidly to changes in blood volume, pressure, and plasma concentrations of certain substances (Boron & Boulpaep, 2003). At the heart of this system lies angiotensin II, a potent vasoconstrictor synthesized from its precursor, renin, through multiple enzymatic conversions. Angiotensin II further stimulates the adrenal cortex to release aldosterone, crucial for salt homeostasis, primarily governing sodium and potassium levels in the body (McCormick & Bradshaw, 2006). Acting through type 1 (AT1) and type 2 (AT2) receptors, aldosterone exerts its effects, with these receptors widely distributed across various brain regions, including the limbic system (Okuyama et al., 1999).
Activation of the RAS develops as a pivotal rapid reply during stress (McCormick & Bradshaw, 2006). However, its role seems dual, with evidence suggesting contrasting effects mediated by its receptors. Research studies in mice lacking AT2 receptors demonstrated abnormal aggression, hinting at their involvement in modulating stress responses (Okuyama et al., 1999). On the other hand, antagonism of AT1 receptors was found to decrease stress intensity and anxiety by impacting the central nervous system (Saavedra et al., 2005). While these receptors’ roles in stress may seem paradoxical, past studies have proposed that their respective antagonists can enhance cognitive function (Barnes et al., 1991). Despite conflicting observations (Shepherd et al., 1996), activation of the RAS remains crucial in stress responsiveness and behavioral control (Carola et al., 2002).
Overall, stress profoundly activates the autonomic nervous system, coordinating physiological responses crucial for coping with challenges (Carola et al., 2002; Lown & DeSilva, 1978; Sgoifo et al., 1999). However, this activation has its limits, beyond which it may become detrimental (Cacioppo et al., 1998). Stress can tilt the sympathovagal balance, either by bolstering the sympathetic nervous system, inducing inotropic and chronotropic effects, or by stimulating the parasympathetic nervous system, potentially triggering vasovagal responses or even cardiac arrest (Cacioppo et al., 1998; Ulrich-Lai & Herman, 2009).
Sympathetic responses, coordinated primarily through the medulla oblongata and presynaptic nodes of the spinal column, involve the release of catecholamines from the adrenal medulla (Purves et al., 2019), culminating in heightened heart rate, skeletal muscle blood flow, and the induction of a “fight or flight” state (Cannon & De La Paz, 1911). These metabolic responses mobilize essential substances to fuel muscular-nervous responses against stressors (Corr et al., 1986). Notably, under stress conditions, the concentrations of epinephrine and norepinephrine surge due to the SAM activation, increasing cardiac contractility and elevating blood pressure (Kandel et al., 2000; Pfeifer et al., 1983).
Parasympathetic reflexes typically counterbalance sympathetic responses in order to reestablish homeostasis (Ulrich-Lai & Herman, 2009). Activation of the nucleus ambiguous and dorsal motor nucleus of the vagus nerve drives parasympathetic actions, mainly decreasing cardiovascular parameters (Kandel et al., 2000). Although sympathetic reactions are relatively short-lived due to reflexive parasympathetic activation, modifications in parasympathetic activity modulate the duration of sympathetic effects, depending on stress conditions (Kandel et al., 2000). In brief, stress elicits a dynamic interplay between sympathetic and parasympathetic branches of the autonomic nervous system, crucial for adapting to and coping with environmental challenges.
Pathophysiological consequences
Chronic stress can cause dysfunctional responses that lead to various health problems such as heart disease, sleep dysregulation, stomach ulcers, and psychiatric disorders. Dysregulation or suppression of the HPA axis often occurs also due to chronic stress. Cardiovascular responses to stress include elevated blood pressure and heart rate, contributing significantly to cardiovascular disease incidence. Stress-related psychological disorders are associated with increased risk for coronary artery disease, stroke, and hypertension. Catecholamine release during stress can adversely affect the gastrointestinal tract by reducing local blood flow, potentially exacerbating H. pylori conditions (Budzyński & Kłopocka, 2014).
The quality and quantity of sleep also impact cortisol response to chronic stress. Higher sleep quality is correlated with a stronger cortisol stress response, particularly manifested in men. On the other hand, individuals reporting issues staying awake or challenges keeping enthusiasm indicate blunted cortisol reactions to stress (Bassett et al., 2015). Disorders of the adrenal system, such as Addison’s disease, Cushing syndrome, and pheochromocytoma, also disrupt the body’s stress processes by impacting cortisol and epinephrine release. Addison’s disease is associated with deficient glucocorticoid and/or mineralocorticoid hormones (Michels & Michels, 2014). Cushing syndrome manifests as hypercortisolism due to endogenous or exogenous sources (Reincke & Fleseriu, 2023), while pheochromocytomas are catecholamine-secreting adrenal tumors (Adler et al., 2008).
The general adaptation syndrome describes stress-induced physiological changes across three stages: alarm reaction, resistance, and exhaustion. Initially, the body goes through two phases in reaction to acute stress: the “fight or flight” response and the recovery phase. Prolonged periods of stress result in adaptation, which is marked by the continuous release of stress hormones and symptoms such as inability to concentrate and irritation. If stress persists, the body enters the exhaustion stage, which is characterized by lower stress tolerance, burnout, exhaustion, sadness, and anxiety (Selye, 1950).
Effect of stress system on immune system
The inflammatory response of the immune system is a normal and necessary response to hostile situations in order to protect the integrity of cells and organs. However, disease-related changes to the immune system can result in either deficiency or overactivity. Overactivity can result in autoimmune illnesses, while insufficient responses can cause immunodeficiency, which puts people at risk for infections and cancer (Kjekshus, 2015).
As cortisol inhibits all aspects of the immune response, activation of the HPA axis predominantly has inhibitory effects on the inflammatory and immunological response. Generated following stressful events, glucocorticoids influence immune responses by alleviating levels of chemoattractants that are essential for immune cell function, inhibiting leukocyte transmigration, and attenuating inflammatory signaling pathways (Ilchmann-Diounou & Menard, 2020). They also induce apoptosis of B and T lymphocytes, causing adaptive immune deficiency (Xu et al., 2020). Thus, at the cellular level, glucocorticoids apply their main anti-inflammatory impacts through various mechanisms, including modifications in leukocyte trafficking and function, decreased production of cytokines and other mediators of inflammation, and inhibition of pro-inflammatory signaling pathways in target organs and tissues (Chrousos, 2000). Consequently, glucocorticoids are used pharmacologically to treat immune-related disorders, particularly autoimmune diseases characterized by exaggerated immune responses (Ilchmann-Diounou & Menard, 2020). However, in cases of chronic stress, these immune alterations may contribute to chronic infections, inflammatory autoimmune diseases, or even cancer. Also, stress-induced sympathetic adrenergic signaling can inhibit immune responses in infectious diseases (Bae et al., 2019).
Recent studies suggest that stress can influence the immune response in an intricate manner. While stress hormones typically inhibit T helper-1 (Th1) pro-inflammatory responses and promote a Th2 shift systemically, they may induce pro-inflammatory cytokine production and activate the peripheral corticotropin-releasing hormone (CRH)–mast cell–histamine axis in certain local responses (Capelle et al., 2022). This additional mechanism implicates the stress system in the pathogenesis of chronic inflammation and immune-related illnesses. Also, glucocorticoids, a main element of the stress response, may impact Th17 differentiation and function through molecular mechanisms that are not yet fully understood. Th17 cells are a newer subset of effector T cells that secrete interleukin-17 (IL-17) and are implicated in autoimmune processes (Taves & Ashwell, 2021), further linking stress to autoimmune diseases.
Effect of stress system on the cardiovascular system
Chronic stress is linked to an increased risk of cardiovascular complications, mainly atherosclerosis or coronary artery disease, which entails lipid accumulation and inflammation of large arteries. This issue can lead to diverse cardiovascular conditions, such as stroke. Greater amygdala activity induced by stress is associated with carotid artery intima-media thickness, elevated blood pressure reactions, and inflammatory responses, contributing to the acceleration of atherosclerosis (Gharios et al., 2024). Furthermore, the maladaptation of neuroendocrine pathways involved in the stress response exacerbates this process. Stress stimulates the HPA axis, leading to increased secretion of glucocorticoids from the adrenal glands, which further accelerates atherosclerosis by reducing nitric oxide concentration and promoting vascular contractility. Intense stress triggers a rapid sympathetic nervous system response, resulting in the release of catecholamines into circulation, leading to increased heart rate, blood pressure, and peripheral microvascular constriction, which also contributes to the development of atherosclerosis (Liu et al., 2019; Macleod et al., 2021). Acute stress can precipitate cardiovascular events such as angina, arrhythmias, stress cardiomyopathy, myocardial infarction, stroke, or sudden death (Vancheri et al., 2022). These results demonstrate the significance of raising awareness about stress-related disorders, as they can influence individuals irrespective of their family history of diseases.
Behavioral manifestations
The acute response to danger and stressful events triggers a consistent series of physiological and behavioral adaptations to increase survival. These adaptations include increased heart rate and blood pressure, redirected blood flow to the brain and affected body areas, and the breakdown of tissues to provide immediate energy. Also, there is a suppression of diverse neurovegetative functions, such as eating, sleeping, sexual activity, and endocrine mechanisms linked to growth and reproduction. This suppression ensures that energy and resources are prioritized towards survival rather than maintenance or growth functions during life-threatening conditions (Gold, 2005).
Furthermore, fear-related behaviors dominate during stressful situations, playing a critical role in survival during emergencies. As a result, an extensive neural circuitry for generating and modulating fear has evolved. Depending on the context and individual factors such as gender and stress-system set points, fear can trigger defensive behaviors that protect from harm or initiate a fight for survival. Speed and simplicity are vital, resulting in the rapid deployment of straightforward, well-practiced behavioral and cognitive responses. Concurrently, there is a suppression of more complex, novel, or untested responses that would take longer to organize (Gold et al., 2015).
Other general behavioral manifestations of stress, such as crying, smoking, excessive eating, drinking alcohol, fast-talking, and trembling, are commonly reported (Ghasemi, 2022). Additionally, individuals often complain that stress negatively impacts their cognitive functioning and task performance (Beversdorf, 2019; Renner & Beversdorf, 2010). Enduring stress can be challenging to manage and can have adverse effects on various aspects of health, including appetite, mood, and sleep (Attia et al., 2022). Research findings demonstrate that physical and cognitive symptoms of stress can contribute to negative behaviors, perpetuating a cycle of stress (Curtiss et al., 2021). For instance, stress is often considered a significant risk factor for alcohol use disorder, as some individuals may turn to alcohol to cope with negative emotions and encounters (Ghasemi, 2022; Nehring et al., 2023). Common behavioral symptoms of stress also include modifications in alcohol and drug usage, changes in appetite, disruptions in sleep patterns, neglect of responsibilities, and nervous habits such as knuckle cracking, fidgeting, and nail-biting (Attia et al., 2022).
Assessment of stress
Several difficulties have been associated with stress evaluation due to individual variability in stress experiences (Hou et al., 2015). The reliability of stress-assessment methods depends on the chosen approach and analysis methods. Previously, subjective methods, such as self-report questionnaires, have been widely used in psychiatry, psychology, and the medical community, measuring mostly behavioral and cognitive skill changes (Holmes & Rahe, 1967; Monroe, 2008; Weiner & Craighead, 2010). However, these methods rely on individuals’ self-perception and are not designed for frequent applications, which may potentially lead to inaccuracies in stress-level measurement (Hou et al., 2015). The Perceived Stress Scale (PSS), developed by Cohen et al. in 1983, is the most widely used instrument for assessing stress. Despite its origins in the early 1980s, the PSS remains a popular instrument for understanding how various situations impact our feelings and perceived stress levels. Recent papers have also highlighted the potential of using single-item ratings of stress and coping and efficient measures that can be administered over time (Verster et al., 2021). In summarizing this literature, Woods and colleagues (2023) concluded that the “technical adequacy of the single-item stress and coping measures have been previously reported; in particular, these items have comparable correlations and predictive value as longer scales of the same construct” (p. 7).
Physiological measurements propose another avenue of stress assessment, with diverse indicators such as heart rate variability, electrodermal activity, and salivary cortisol, providing valuable insights (Engert et al., 2011; Hanrahan et al., 2006; Kirschbaum & Hellhammer, 1994). In particular, assessment is done by measuring biochemical indicators such as cortisol, cortisol-awakening response, prolactin, dexamethasone suppression test, salivary α-amylase, plasma/urinary norepinephrine, norepinephrine spillover rate, and interleukins (Azra et al., 2019; Nater et al., 2013). Furthermore, stress-induced activation of the HPA axis is associated with a rise in plasma cortisol, while activation of the SAM system results in the secretion of catecholamines. Both of these can be easily measured in blood, urine, and saliva. Based on this direct association, cortisol and catecholamines have been utilized as valid biochemical indicators of stress in humans (Nater et al., 2007). The measurement of cortisol levels in the serum, saliva, and urine is routinely conducted to measure stress reactions. Free cortisol is metabolized in the liver, with about 70% of biologically inactive metabolites excreted in urine. Accordingly, the measurement of cortisol conjugates and metabolites in 24-hour urine samples has also been utilized as indicators of HPA-axis activation (Mason et al., 2002).
These markers can be influenced by various factors, including circadian rhythm and physical activity (Koibuchi & Suzuki, 2014; Zanetti et al., 2019). Despite their reliability, the limitations associated with some of these biochemical indicators include invasiveness and the impossibility of continuous stress-monitoring assessment. The link between the activation of biochemical indicators in the body and the perceived intensity of stress is complicated and not well-studied, making the use of these indicators less advantageous (Nater et al., 2013).
There is a wide range of techniques that monitor the physiological reactions of the stress response on the body using indicators extracted from biosignals, which are time-varying measurements of bodily functions with two major classes: physiological (e.g., cardiac activity and brain function) and physical (e.g., pupil size, eye movements, and respiration) signals (Giannakakis et al., 2019). The most widely used biosignals are electrocardiography (ECG), electromyography (EMG), and skin conductance (Attar, 2022; Zheng et al., 2015). Characteristics extracted from these biosignals, such as heart rate and its variations, are driven by the autonomic nervous system and constitute good stress indicators. Other biosignals include skin temperature, pulse photoplethysmography (PPG), respiration, pupil diameter, EMG, and blood pressure (Giannakakis et al., 2019; Zheng et al., 2015).
Neuroimaging techniques (e.g., functional magnetic resonance imaging[fMRI], magnetoencephalography [MEG], and electroencephalography [EEG]) provide alternative measurement tools for stress assessment by indirectly measuring brain activity (Attar, 2022). Developments in neuroimaging have transformed our understanding of brain function and have become a vital resource for researchers studying neurological problems. It has also revolutionized the diagnosis and treatment of neurological and psychiatric disorders by allowing for the identification of biomarkers, the monitoring of treatment responses, and the advancement of tailored and adapted therapies (Yen et al., 2023). Neuroimaging techniques offer researchers the capacity to visualize the brain’s structure and activity, providing insights into how various brain regions contribute to cognitive and behavioral processes such as perception, attention, memory, language, decision-making, and emotion regulation. Certain neuroimaging techniques offer researchers diverse levels of spatial and temporal resolution, permitting the examination of brain activity across diverse spatial scales and timeframes (Zhang et al.,2023).
A widely used noninvasive neuroimaging technique is EEG, which records the brain’s rhythmic electrical patterns with multiple electrodes positioned on specific sites on the scalp (Yen et al., 2023; Zhang et al., 2023). Due to its sensitivity to localized brain activity in areas implicated in the production of the stress response, or activity linked to elevated arousal or particular psycho-emotional states, EEG is valuable in psychophysiological research. EEG identifies diverse frequencies of brain activity, which signify different cognitive states such as stress, anxiety, and relaxation (Giannakakis et al., 2019). While the left anterior area of the brain appears to be associated with approach-type emotions (e.g., happiness, rage), the right anterior region is related to avoidance-type emotions (e.g., sadness, fear; Larsen et al., 2008). According to Giannakakis et al. (2019), evidence supports the idea that in a stressed condition, frontal right alpha activity is often higher than left alpha activity. In particular, individuals who fail to represent simplified alpha activity and have heightened beta asymmetry can experience stress and anxiety disorders (Attar, 2022). In other words, with a decrease in alpha activity and an increase in the beta-activity waves, one may experience stress (Giannakakis et al., 2019).
EEG demonstrates several advantages by standing out for its high temporal resolution, cost-effectiveness, and ease of use (Zhang et al.,2023). EEG analysis typically entails extracting characteristics from EEG signals and classifying stress levels based on these features (Ehrhardt et al., 2021). Various EEG features, including time-domain, frequency-domain, and synchronicity-domain features, provide valuable information about mental stress. Frequency-domain features, such as power spectral density and time-frequency features obtained through transforms like short-time Fourier transform or discrete wavelet transform, offer insights into stress-related brain rhythms (Movahed et al., 2021). While EEG analysis holds promise for stress assessment, conflicting findings in the literature highlight the need for further research to establish robust methods (Ehrhardt et al., 2021; Yen et al., 2023).
Recently, fMRI has also been utilized to examine the effects of stress, for example, revealing the impact of an imaging compatible stressor on network connectivity in the brain during verbal problem-solving and other verbal tasks (Nair et al, 2020a, 2020b). While fMRI provides significantly greater anatomical detail than EEG, the temporal sensitivity of EEG is significantly greater. Additionally, tasks often need to be modified to be compatible with the MRI environment, leading to imaging in a less naturalistic setting in this environment.
Despite these efforts, a scientifically supported, objective, reliable, repeatable, and easily usable measurement method remains unavailable. Up to now, there is no consensus among professionals or within the research community on a unique or standard stress assessment method. Thus, a single stress marker cannot globally assess the stress response of an individual (Azra et al., 2019). Therefore, a multimodal approach to stress measurement that considers the different stress-response reactions as a whole is requisite. Along with Azra et al. (2019), we propose to use physiological biomarkers that can be unobtrusively monitored, aiming to obtain a reliable description of the stress response that can be easily monitored in daily life.
Recent papers have highlighted the potential promise of using Wearable Biosensor Technology (WBT) to monitor stress biometrics with minimal burden or intrusiveness (Hernández-Mustieles et al., 2024). WBTs include smart wristbands, watches, and even glasses. These technologies and related sensitivities and algorithms continue to improve and will likely provide reliable, real-time, and continuous information about key stress biometrics.
One final important point related to the measurement of stress is the need for sophisticated data-integration strategies. Most measures of stress can produce enormous amounts of information especially when they include continuous or longitudinal data streams. Ecological Momentary Assessments (EMAs) have emerged as excellent data strategies for summarizing and analyzing these data streams (Song et al., 2023). EMAs have been successfully applied with self-report measures including single-item measures (Song et al., 2023) as well as physiological measures (Weber et al., 2022).
Intervention approaches for stress
Regarding intervention, the biopsychosocial framework (Engel, 1977) provides a comprehensive approach to stress management, indicating the interaction between biological, psychological, and social factors. This approach was originally developed at the University of Rochester by Drs. George Engel and John Romano. The biopsychosocial approach emphasizes the significance of understanding individual health and disease within their broader contexts, unlike traditional biomedical models that primarily focus on pathophysiology and biological aspects of disease. This model integrates insights from diverse fields to provide a holistic understanding of stress and its influences on individuals (Borrell-Carrió et al., 2004). It is adapted and expanded upon from existing studies to offer a robust framework for stress intervention and management. As illustrated in Figure 2, within this framework, different professionals, including psychiatrists, psychologists, and social workers, collaborate to address stress and its effect on individuals. Psychiatric interventions typically focus on mitigating emotional distress through medication, particularly targeting symptoms of Axis I mental disorders such as Major Depressive Episodes or Generalized Anxiety Disorder. The purpose of medications is to regulate neurochemical imbalances that cause negative emotional responses.
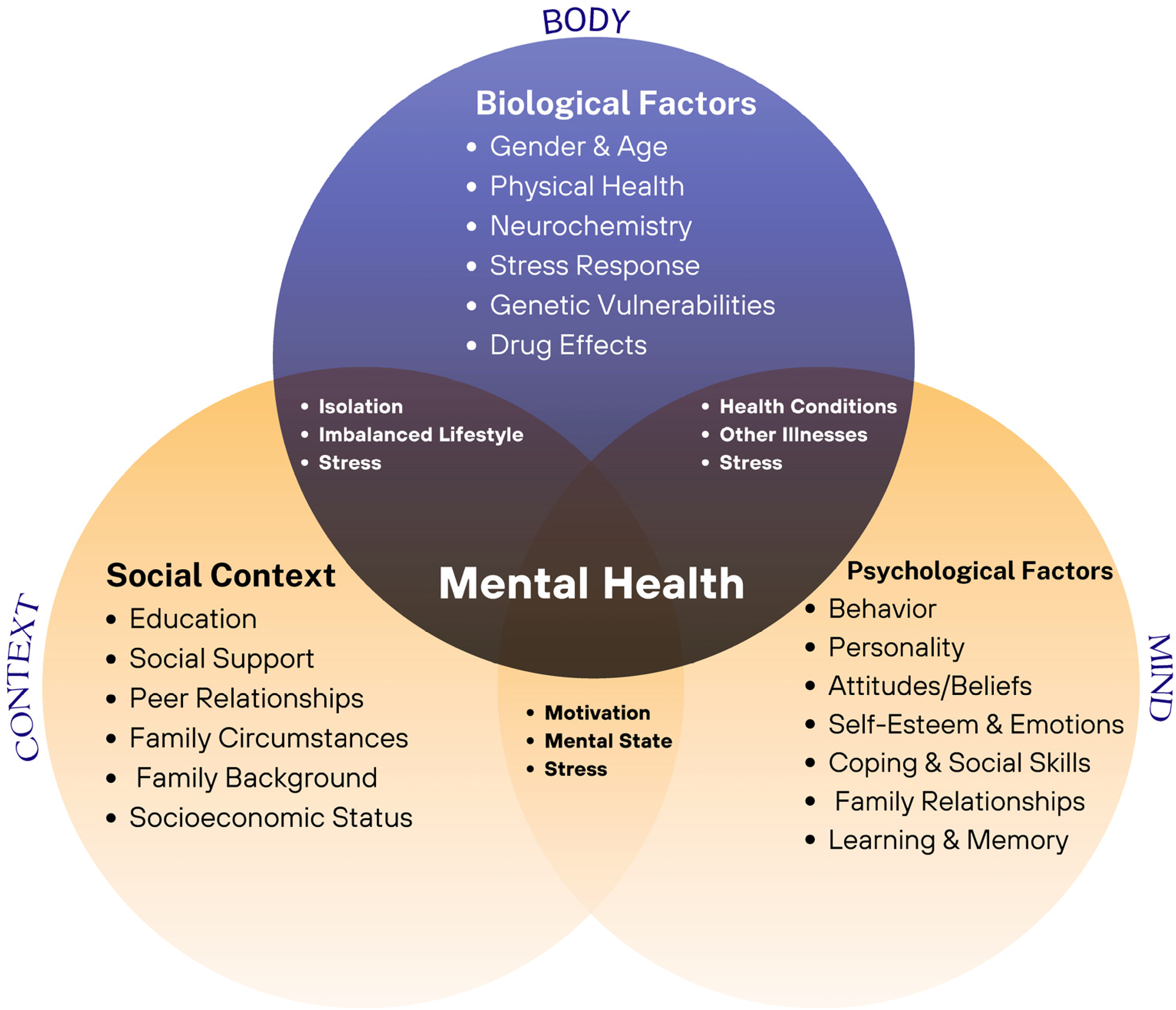
The biopsychosocial model of health.
Psychologists, on the other hand, focus on cognitive processes involved in translating life stress into emotional distress. Psychological interventions involve different psychotherapeutic programs such as CBT, which assists clients in identifying and challenging maladaptive thought patterns and developing more effective coping strategies. Social workers take a broader perspective, considering societal factors that affect stress and coping. They may address interpersonal functioning, occupational adjustment, and access to agency resources that can support clients in dealing with stressors. It is important to note that both psychologists and social workers may conceptualize and intervene in stress across these various domains.
Each approach has its strengths and limitations, and the effectiveness of treatments may differ based on the nature of the stressors and the individual’s unique circumstances and available resources. Evaluating these approaches in light of common stressful life events, economic hardships, and life changes can contribute to tailoring treatment programs to meet the various needs of individuals experiencing stress. By integrating biological, psychological, and social perspectives, professionals can offer holistic support to foster resilience and well-being.
Pharmacological interventions
Regarding pharmacological treatments, a significant issue in mental health care is the overreliance on psychotropic medications, such as antidepressants and anxiolytics (Olfson et al., 2002; Whitaker, 2007; Zito et al., 2000). Diverse factors have been identified contributing to the surge in prescription rates, including pharmaceutical industry advertising, cultural norms favoring quick fixes through medication, and healthcare system dynamics such as managed care and cost containment, and escalating time constraints imposed on physicians for clinic visits. Furthermore, the reliance on medication-based treatments might be unintentionally promoted through publication biases in scientific journals (Antonuccio et al., 2003; Turner et al., 2008). Psychopharmacological treatments may be utilized to mitigate the adverse emotional reactions that arise from stressors; nevertheless, it is important to acknowledge that these reactions can also be normal, even adaptive, responses to life experiences (Woolfolk et al., 2007). Sadness or anxiety are examples of negative emotions that might act as motivational cues to seek out social support or make lifestyle adjustments.
However, medications can be suitable when negative emotional responses become severe or persistent, disrupting adaptive functioning. For instance, antidepressants may be effective in treating severe depression that inhibits daily functioning. It is crucial to consider the role of coping strategies in managing stress. Effective coping involves confronting stressors or changing perceptions, while medications primarily suppress emotional reactions. Overreliance on medications to control stress may overlook the potential benefits of non-pharmacological treatments, which often yield better long-term results (Papp, 2007).
While medications may mitigate extreme stress reactions, non-pharmacological interventions typically provide better long-term outcomes (Papp, 2007). If a medication is needed in particularly extreme cases, it seems advisable to pair it with non-pharmacological interventions for longer-term impact. There are many challenges in the management of normal emotional responses to life experiences in the medical setting. Psychiatrists often rely on psychiatric diagnoses to lead treatment decisions and prescriptions (Horwitz & Wakefield, 2007). However, when clients are dealing with substantial life stressors, they may not meet the criteria for most psychiatric diagnoses beyond adjustment disorder. This can sometimes present a challenge. The patient often is expecting action by the psychiatrist, who has significant time limitations imposed on the duration of the patient encounter. The psychiatrist is forced to make a quick determination as to whether the severity of the reaction to the stressor might require supplemental pharmacotherapy, and an associated adjustment to the diagnostic code might be necessary to support this approach.
When initiating psychopharmacological interventions, patients may experience frustration because of delayed treatment response and may stop medication prematurely (Horowitz & Horowitz, 1993). Poor adherence to antidepressant medication regimens is associated with unfavorable results, including low proportions of remission from depressive episodes (Rush et al., 2004). The limitations imposed on time allowed with patients, particularly problematic in the primary-care setting, can limit the time allowed to discuss expectations with new medications to patients, which may contribute to poor adherence (Tarn et al., 2008). Moreover, there is evidence of over-prescription of psychotropic medications, even in cases where patients do not demonstrate symptoms of anxiety or depression (Coyne et al., 2004).
The financial cost and potential side effects of long-term pharmacological interventions can contribute to exacerbating stress. Sustained preservation of the pharmacological intervention increases costs and the risk of long-term side effects. Sudden termination of medications can give rise to withdrawal responses and recurrence of stress symptoms. Additionally, long-term application of certain anti-anxiety medications may lead to increased tolerance and physical dependency, with benefits often not continuing after discontinuation (Papp, 2007; Hollon et al., 2006). Although there is evidence criticizing the limitations of pharmacological treatments, it is important to acknowledge that these interventions can be highly effective, particularly for major psychiatric conditions such as severe depression and intense stress disorders. There have been many cases where medications successfully prevented and offered required relief from symptoms and improved the quality of life for individuals (Sijbrandij et al., 2015). However, it is also important to note that pharmacological interventions are not always effective and there may be a need for such treatments to be complemented by other psychotherapeutic interventions to address the multifaceted nature of mental health conditions. By integrating medication with psychotherapy, lifestyle modifications, and other holistic treatments, we can provide a more thorough and individualized approach to mental health care (Cuijpers et al., 2008).
Psychological interventions
Psychological approaches typically integrate clinical assessment, psychological theory, common-sense views of etiology, and practical stress-management guidelines. Stress-reduction strategies in psychology frequently contribute to promoting functional coping mechanisms. A vast range of coping techniques can alleviate the adverse impacts of stressful life events (Herman & Reinke, 2014). Psychological treatment programs include but are not limited to, rational emotive behavior therapy (REBT; Ellis et al., 1997), CBT (Beck, 1970), mindfulness-based stress reduction (MBSR; Kabat-Zinn & Hanh, 2009), inquiry-based stress reduction (IBSR; Katie & Mitchell, 2021), stress inoculation training, problem-solving approaches, meditation, relaxation techniques, and behavioral lifestyle changes targeting nutrition, sleep, and exercise (Selhub, 2007; Yusufov et al., 2019). Developed by Albert Ellis in the late 1950s, REBT is a cognitive-behavioral approach to counseling and psychotherapy that addresses psychological challenges by altering cognitions and resulting emotional reactions. REBT presumes that stress is directed not primarily by the challenging life experiences or stressors individuals encounter, but by their irrational cognitions about these experiences (Ellis et al., 1997). The purpose of REBT is to replace irrational cognitions, which are solid and fixed, inconsistent with reality, and illogical, with rational cognitions that are flexible and non-extreme. In other words, it assists one learn to challenge his/her own irrational beliefs and develop habits of thinking in more rational ways. This cognitive shift lets individuals behave more effectively and experience healthier feelings (Dryden & David, 2008). There is also evidence promoting the use of REBT for mitigating negative feelings such as anxiety, stress, and depression, as well as improving stress-coping strategies with a medium effect size (for a review, see David et al., 2018).
Similar to REBT, the basic model of CBT uses therapeutic strategies to modify maladaptive beliefs and assists patients in adopting a calm and rational approach and perspective toward stressful life experiences. These modifications in thought patterns are presumed to result in positive emotional and behavioral changes (Beck, 2011). This therapy was developed in the 1970s by Aaron Beck who considered stress as arising from the interpretation of life experiences, with negative attitudes underlying most stressors and emotional disturbances. Stress responses originate from patients’ perceived capacity to cope with life experiences, which therapy attempts to modify alongside refining coping skills. CBT, focusing on changing beliefs and bolstering coping skills, effectively manages occupational stress, especially in individuals with less severe depression (Richardson & Rothstein, 2008). These strategies also increase physical responses to stress and diminish the perception of situations as stressful. Cognitive therapy inspires clients to view cognitions as temporary interpretations rather than factual representations of reality. CBT is widely considered the gold standard for evidence-based psychological interventions and has proven effective and practical in addressing a broad range of psychological conditions (Barrett & Stewart, 2021; Ghasemi, 2023; Ghasemi, Herman, & Reinke, 2023; Yusufov et al., 2019).
In recent years, there has been a shift in the prospect of cognitive and behavioral therapy with the advent of “third-wave” cognitive-behavioral approaches, which are founded in an empirical, principle-focused approach. According to Hayes (2016), the third wave of behavioral and cognitive therapy is particularly sensitive to the context and functions of psychological phenomena, not just their form, and thus tends to emphasize contextual and experiential change strategies in addition to more direct and didactic ones. These treatments tend to seek the construction of broad, flexible, and effective repertoires over an eliminative approach to narrowly defined problems, and to emphasize the relevance of the issues they examine for clinicians as well as clients. The third wave reformulates and synthesizes previous generations of behavioral and cognitive therapy and carries them forward into questions, issues, and domains previously addressed primarily by other traditions, in hopes of improving both understanding and outcomes. (p. 880)
These third-wave cognitive-behavioral approaches still place notable importance on beliefs but emphasize more on individuals’ relationship with their cognitions rather than on the content of the thoughts themselves. These approaches, which include, among others, acceptance and commitment therapy (ACT) and mindfulness-based interventions (MBI), focus on mindfulness, acceptance, values, goals, and meta-cognition (Hayes & Hofmann, 2017). Specifically, there has been substantial research in recent years supporting the efficacy of ACT in alleviating stress and improving overall psychological well-being (Barrett & Stewart, 2021; Ghasemi et al., 2023). The major aim of ACT is to increase psychological flexibility, including six core processes: acceptance, cognitive defusion, flexible attention to the present moment, self-as-context, values, and committed action. Regarding beliefs, ACT does not aim to change the content of one’s beliefs but emphasizes modifying how individuals associate with their thoughts through cognitive defusion techniques (Hayes et al., 2016). It proposes that the problem lies not in the content of the cognition itself but in one’s tendency to fuse with the thought or perceive it as objectively true. Cognitive defusion lets one observe his/her cognitions in a more detached manner. This shift assists individuals in viewing thoughts as mere life experiences in the mind, diminishing their effect and promoting greater psychological resilience.
IBSR, also known as “The Work,” is another known third-wave behavioral approach developed by Byron Katie in 1986 in response to her own mental health struggles. This technique is associated with a process of self-inquiry that assists individuals in detecting and questioning the stressful cognitions causing their suffering, whether related to relationships, work, body image, or other areas. IBSR consists of two phases: (a) systematically identifying stressful cognitions and (b) studying these cognitions through a meditative process using four particular questions and turnarounds. This self-inquiry can reveal that stressful cognitions are not entirely factual, thereby diminishing negative feelings by assisting individuals to adopt a less judgmental perspective, regulate their stress levels, and cope better with distress. The strategy requires no intellectual, religious, or spiritual preparation, only a commitment to deepening self-awareness (Katie & Mitchell, 2021).
Similar to classical CBT, IBSR indicates that dysfunctional beliefs are the primary cause of distress and problematic behaviors. However, while CBT challenges these cognitions through rational and objective methods, such as reasoning and argumentation, IBSR taps into inner wisdom. This approach integrates different types of knowing, including observation, logical analysis, kinesthetic and sensory experiences, behavioral learning, and intuition. IBSR has been widely studied and promising outcomes have been found for stress, anxiety, and well-being among a range of clinical and nonclinical populations (for a review, see Hook et al., 2021).
MBSR complements the approaches by teaching clients to notice situations and cognitions in a nonjudgmental manner without responding impulsively. This technique helps them advance a more automatic awareness of experiences, potentially mitigating stress and fostering emotional regulation. It is a method developed by Jon Kabat-Zinn in 1979 and was primarily advanced for stress management, but has since expanded to address diverse health-related conditions, such as anxiety, depression, pain, and immune disorders (Sharma & Rush, 2014). MBSR programs entail training in formal mindfulness practices, including body scan, sitting meditation, and Hatha yoga. The core of MBSR is training attention through simple, secular meditation techniques in an attempt to alter our relationship with stressful cognitions and life experiences by reducing emotional reactivity and increasing cognitive appraisal. From a Western psychological viewpoint, applying mindfulness both during formal meditation and in everyday activities can result in an awakening process (Kabat-Zinn & Hanh, 2009). MBSR has been widely studied, with promising results reported across a broad spectrum of clinical and nonclinical populations (Ma et al., 2022; Sharma & Rush, 2014). The program’s capacity to promote mindfulness helps clients manage stress more effectively, promoting overall well-being and resilience. Therefore, mindfulness strategies can contribute to mitigating emotional distress by diminishing distracting behaviors and ruminative cognitions, as well as contributing individuals to adopting a detached view toward their cognitions, emotions, and bodily sensations (de Abreu Costa et al., 2019). These techniques demonstrate self-directed attention and sustained focus on cognitions, feelings, and sensations (Baer, 2003).
Stress inoculation training also provides a valuable framework for assisting clients in dealing with stressors. It confirms that stressful life events cannot always be foreseen or controlled, advocating for adapting to problems as they arise. Stress inoculation training teaches clients to regard stressors as challenges and opportunities for growth, enhancing their problem-solving skills. These skills can be tailored to various stressful life events and have been beneficial for managing medical conditions and stressful occupations (Meichenbaum, 2019). Many depressed clients find benefit in acquiring problem-solving skills. When stressful life events are perceived as problems to solve, clients can learn to pause, devise a plan of action, and engage in constructive coping strategies. Similarly, relaxation and meditation techniques have been shown to assist clients in reducing subjective distress and lowering blood pressure (Schneider et al., 2005; Yusufov et al., 2019).
In comparison with the influences of various psychotherapeutic interventions discussed above, the results of recent randomized controlled trials (e.g., Barrett & Stewart, 2021; Ghasemi, 2023; Ghasemi et al., 2023) have indicated that both ACT and CBT significantly improve stress, burnout, and mental health outcomes. Additionally, no significant differences have been found between the impacts of ACT and CBT in such trials. In particular, meta-analyses (e.g., Ma et al., 2022) assessing the combined effects of mindfulness-informed (e.g., ACT) and mindfulness-based interventions (e.g., MBSR and MBCT) on depressive and anxiety symptoms found modest impacts in mitigating depressive symptoms and moderate effects in reducing anxiety symptoms. In a similar vein, de Abreu Costa et al. (2019) examined the efficacy of CBT and mindfulness-based therapies in reducing internalizing symptoms in clients with anxiety- and stress-related conditions. Their results did not indicate the superiority of CBT over mindfulness-based treatments for decreasing internalizing symptoms and distress. However, the authors emphasized the need for additional research studies before mindfulness-based intervention programs can be suggested as first-line treatments.
In a more thorough meta-analytic evaluation study, Yusufov et al. (2019) examined the effectiveness of stress-reduction intervention programs for undergraduate and graduate students. The outcomes indicated that CBT, coping skills training, and social support interventions are particularly effective in decreasing perceived stress. On the other hand, techniques such as relaxation training, MBSR, and psychoeducation are more effective in mitigating anxiety symptoms. Unfortunately, these crude conclusions are of limited use because various types of intervention programs, delivery formats, and populations get lumped together. Overall, each of these approaches—CBT, IBSR, and MBSR—offers unique strategies for addressing stress and cognitive distortions, leading to a comprehensive understanding and treatment of psychological distress.
Social interventions
Because stress is typically conceptualized and measured at the level of the individual, interventions for stress may ignore the contextual contributions to stress. Some circumstances may exceed the human capacity to cope (e.g., repetitive traumatic events endured during war or settings with high levels of violence), thus relying solely on within-person interventions risks pathologizing the individual for not adapting to a pathological environment. As one example, employment circumstances are a common contextual stressor that may contribute to high stress levels, and some aspects of the employment context are beyond the individuals’ ability to alter (Herman et al., 2020). Thus, comprehensive strategies to reduce stress-related illnesses will give attention to creating more nurturing environments that reduce contextual stressors for both children and adults (Biglan et al., 2012).
When effective, social agencies and societal interventions often aim to address the source causes of stress. Thus, social-service interventions typically follow one of two major approaches: (a) addressing interpersonal conflicts and increasing the patient’s social support network, or (b) providing tangible support such as employment training, subsidized housing, or legal assistance to explore challenging circumstances. Patients may need help in getting over the complications associated with poverty, unemployment, and discrimination. A systematic review by Nagy and Moore (2017) classifying reports on social interventions targeting depression in adults indicates that almost all studies employed multiple approaches to facilitate social interaction among participants. The most common approach was a peer-based method involving information sharing and empathizing with others. Conversely, linking individuals to community resources was the least common approach. Most interventions were conducted in community or urban settings, though some group-based activities took place in nature, including group walks, horticultural activities, and trust-building tasks at remote retreats.
Examining the impacts of social support interventions on various stressful life experiences, Hogan et al. (2002) found generally encouraging results across diverse forms of support. The research recommends that support offered by friends, family members, and peers is beneficial. Furthermore, social-support skills training appears particularly useful. These positive results align with Yusufov et al.’s (2019) meta-analytic assessment of stress reduction interventions, the results of which demonstrated social support is an effective approach to mitigating perceived stress.
In brief, a thorough approach to stress management should incorporate a range of interventions adapted to individual needs and circumstances. While psychotropic medications can be helpful in managing acute symptoms, they should be used judiciously and complemented by non-pharmacological strategies for optimal results. Psychological interventions offer effective ways to alter maladaptive thought patterns and behaviors, enhancing emotional regulation and resilience. Social interventions, which leverage the power of social-support networks and community resources, can also significantly mitigate the impact of stress by fostering a sense of belonging, reducing direct contextual causes of stress, and offering practical and emotional assistance. Together, these pharmacological, psychological, and social strategies form a holistic, biopsychosocial approach to stress management that can address the multifaceted nature of stress and encourage overall well-being.
Discussion and conclusion
The purpose of this narrative literature review was to investigate the multifaceted nature of stress, spanning physiological, psychological, and social dimensions, and to explore assessment and intervention strategies aimed at mitigating its effects. Throughout the study, key topics associated with stress physiology and pathology were introduced. Each of these topics represents a vast field of study, extending far beyond the scope of this review, and they remain focal points of ongoing research within the field of neuroscience.
Furthermore, different facets of stress were addressed, including the activation of the HPA axis and SAM axis, the role of glucocorticoids and catecholamines in modulating physiological reactions, and the influence of chronic stress on cardiovascular, immune, and gastrointestinal systems. This review also explored diverse techniques for evaluating stress, ranging from subjective self-report questionnaires to objective physiological measurements and neuroimaging methods. Intervention strategies discussed within the biopsychosocial framework included psychiatric treatments, psychological therapies concentrating on cognitive restructuring and coping skills, and social interventions targeting interpersonal conflicts and societal stressors. By including a wide range of stress-related topics, this narrative literature review was an attempt to offer a thorough understanding of stress and equip readers with insights into effective approaches and strategies for managing its adverse impacts.
It would be crucial to understand the physiological processes of stress in order to identify the source causes of diverse illnesses and inform both pharmaceutical and psychiatric interventions. By revealing the intricate pathways through which stress affects the body, researchers can explicate the underlying processes driving illnesses such as cardiovascular conditions, gastrointestinal problems, psychiatric disorders, and immune system dysregulation (Azra et al., 2019; Ferguson et al., 2016; Gold et al., 2015; Vancheri et al., 2022). This understanding not only assists the progress of targeted pharmacological treatments but informs the application of psychotherapeutic intervention programs for mitigating the adverse impacts of stress on mental health (Gold, 2015). Additional studies are required to examine deeper the molecular and cellular processes underlying stress reactions, particularly in the environment with chronic and intricate stressors. Furthermore, examining the interaction between genetic predispositions and contextual factors in stress-related conditions can offer valuable insights into individual susceptibility and resilience. Interdisciplinary collaborations integrating fields such as neuroscience, immunology, endocrinology, and psychology are critical for achieving a thorough understanding of the multifaceted nature of stress and its influence on mental health and well-being. By increasing our understanding of these aspects, we can pave the way for more effective preventive measures, personalized treatments, and holistic approaches to stress management.
Briefly, the review’s findings underline the significance of using a biopsychosocial framework in understanding and treating stress-related conditions. Healthcare practitioners can advance more holistic approaches to prevention and intervention by understanding the complicated interaction between biological, psychological, and social factors (Borrell-Carrió et al., 2004). In order to effectively control the acute symptoms of conditions associated with stress, it is crucial to use pharmacological treatments to address neurochemical imbalances and physiological dysregulation (Olfson et al., 2002). However, the overreliance on psychotropic medications requires careful contemplation of the potential risks and benefits, demonstrating the necessity for individualized treatment plans (Whitaker, 2007). Psychological interventions, particularly CBT, provide valuable approaches for changing maladaptive cognition patterns and enhancing coping skills (Richardson & Rothstein, 2008; Yusufov et al., 2019). Furthermore, evidence suggested that implementing social interventions to address systemic stressors such as poverty, discrimination, and social support networks can significantly influence individuals’ resilience and general well-being (Nagy & Moore, 2017; Selhub, 2007).
Based on the presented research literature, future research efforts may concentrate on explicating the fundamental processes associating stress with disease pathology, investigating innovative therapeutic targets, and advancing tailored treatments that consider individual variations in stress response and coping strategies. Furthermore, longitudinal research examining the long-term efficacy and sustainability of biopsychosocial treatments is warranted to inform evidence-based practice and optimize intervention results. By integrating biological, psychological, and social perspectives, future research endeavors can contribute to the development of more comprehensive and effective strategies for prevention and stress management.