
Abstract
The Bougainville Crisis (1988–1997) was characterized by widespread human rights violations, civilian deaths, and displacement. In March 2017, a rapid qualitative assessment was conducted to better understand the major mental health and psychosocial (MHPS) problems of conflict-affected adults living in North Bougainville in order to contribute to the design of feasible interventions to address these problems and inform the development of culturally appropriate assessment instruments. We conducted 54 free-list interviews to gather information on the problems of people in local communities, and further explored five priority MHPS problems through 38 key-informant interviews. The major MHPS problems that emerged and were subsequently explored included alcohol use, drug use, arguments and fights, physical violence against women, and rape. Frequently reported indicators of these problems included anger, aggression, sadness, shame, worry, trauma, neglect, and fear. Findings highlight the highly interconnected relationship between substance use and violence in North Bougainville, as well as the set of emotional and behavioral problems that both contribute to and result from this relationship. The primacy of both drug and alcohol use in this setting is particularly notable, as is the role of these substances as individual coping mechanisms and instigators of violence. Overall, findings suggest the need for integrated strategies toward addressing MHPS issues in North Bougainville, with violence and substance use incorporated as both causes and consequences of psychological distress.
Introduction
Between 1988 and 1997, the population of Bougainville was subjected to intensive fighting between the armed forces of Papua New Guinea and local militias. Referred to as the Bougainville Crisis, this protracted civil war was accompanied by widespread human rights violations, including murder, torture, rape, arbitrary arrests and detentions, looting, and property destruction (Amnesty International, 1997; Boege, 2009; Havini, 1995, 1996). It is estimated that as many as 20,000 people lost their lives and over 60,000 were internally displaced (Braithwaite et al., 2010). Violence continued in the region through the commencement of the peace process in July 1997, which established Bougainville as an autonomous region within Papua New Guinea (Bougainville Peace Agreement, 2001), and laid the groundwork for a recent referendum on independence supported by 98% of the population (Bougainville Referendum Commission, 2020). While the peacebuilding process was largely hailed as a success and has brought notable political stability to the region (Reddy, 2008; Wallis, 2012), high levels of community and sexual violence remain, as do persistent localized conflicts in several areas of Bougainville (Fulu et al., 2013; Jewkes et al., 2013; Jewkes, Fulu et al., 2017; Kent & Barnett, 2012). In addition, the complete breakdown of the region's social, economic, and educational systems during the conflict has left Bougainville in an enduring state of fragility (Braithwaite et al., 2010).
There is substantial international evidence regarding the mental health and psychosocial (MHPS) impacts of armed conflict. War-related violence, deprivation, and displacement contribute to a range of short- and long-term mental health problems including depression, anxiety, and post-traumatic stress disorder (PTSD) (Bogic et al., 2015; Charlson et al., 2019; Jong et al., 2003; Steel et al., 2009). In particular, MHPS issues have consistently been associated with cumulative exposure to traumatic events including murder, torture, sexual violence, and forced displacement (Roberts & Browne, 2011; Steel et al., 2009). Beyond these direct impacts, mental health can also be influenced by prolonged disruptions to political, economic, sociocultural, and healthcare infrastructures (Mollica et al., 2004). Protracted violence produces or exacerbates stressful conditions such as social marginalization, family adversity, and inadequate housing, and this can profoundly affect the psychosocial well-being of individuals living in conflict-affected settings (Miller & Rasmussen, 2010). This may be a particular issue within the context of chronic poverty, with armed conflict contributing to intractable cycles of socioeconomic deprivation that can drive ongoing mental health disparities (Bwirire et al., 2022).
While there have been few systematic studies of MHPS problems in the wake of the Bougainville Crisis, existing assessments indicate that such issues are pervasive (Jewkes, Jama-Shai et al., 2017). In particular, it has been suggested that the conflict contributed to complex patterns of violence that can be seen among Bougainville's population (Jewkes, Jama-Shai et al., 2017). The United Nations Multi-Country Study on Men and Violence found very high rates of sexual and gender-based violence in Bougainville (Fulu et al., 2013; Jewkes et al., 2013) and considerable mental health and substance use problems including high rates of depressive symptoms (32% and 38% among men and women, respectively), PTSD symptoms (25% and 15%), suicidal ideation (3% and 8%), alcohol abuse (34% and 7%), and drug use (17% and 3%) (Jewkes, Jama-Shai et al., 2017). These findings align with those from another investigation, which found anecdotal evidence of substantial conflict-related trauma, grief, anger, substance use, and domestic violence in Bougainville (Tierney et al., 2016). This study also highlighted the unique MHPS issues of individuals who were children during the war, and who are now marginalized due to their lack of formal education, limited engagement with traditional social values, and deviant behaviors.
While these quantitative investigations have highlighted the prevalence of specific MHPS problems in Bougainville, no existing qualitative studies have explored local perceptions regarding these issues among conflict-affected individuals residing in the region. This is an important gap in evidence, as this type of information is essential for identifying locally relevant MHPS problems, selecting and implementing contextually feasible interventions, and designing culturally appropriate assessment instruments (Bolton & Tang, 2004). In addressing such gaps, rapid qualitative methods have been identified as a cost-effective technique for incorporating community perspectives and cultural understandings into health policies and programs (Chambers, 1981; Manderson & Aaby, 1992; Scrimshaw & Hurtado, 1987; Smith, 1989). While these methods do not provide in-depth ethnographic information, they are well-suited for ensuring that MHPS interventions in low-resource environments are acceptable to the target population and reflect their perspectives on priority MHPS problems (Bolton & Tang, 2004). As such, they have been used by our team for over two decades to identify and describe MHPS needs among a wide range of conflict-affected populations, including those living in Uganda, Rwanda, Zambia, Haiti, and Iraq (Betancourt et al., 2009; Bolton, 2001; Bolton et al., 2012, 2013; Murray et al., 2006; Nguyen et al., 2016).
The current study employed rapid qualitative methods in North Bougainville in order to explore the MHPS problems of concern to conflict-affected adults. Specifically, we aimed to gain an understanding of local descriptive terminology for MHPS problems, perceptions regarding their causes and effects, and strategies for addressing them. This work was undertaken as part of a broader initiative to build mental health capacity in Bougainville. In 2014, the Autonomous Bougainville Government (ABG) engaged technical advisors alongside a local steering committee to consult broader stakeholder groups and make recommendations for building capacity to address the continuing MHPS impacts of the Bougainville Crisis. On the basis of these efforts, the following recommendations were submitted to the ABG: (1) conduct systematic research on MHPS needs and available resources; (2) establish a comprehensive community-based model of mental health services; (3) develop and test strategies to raise awareness and promote advocacy around MHPS issues; and (4) develop an official mental health policy with the aim of providing accessible and sustainable services to the Bougainville population (Tierney et al., 2014). These recommendations were approved by the ABG, and subsequently incorporated into the Bougainville Mental Health Policy (Autonomous Bougainville Government, 2019). The current study served as an initial pilot activity in this mental health capacity-building initiative, known colloquially as the Bougainville Mental Health Project.
Methods
Study site
Located in the Solomon Sea, the Autonomous Region of Bougainville consists of a chain of islands, and is divided into three administrative regions known as North, Central, and South Bougainville. At its last census in 2011, Bougainville's total population was 249,358 with 42% of the population residing in North Bougainville (Autonomous Bougainville Government, 2018). Data were collected in North Bougainville over a three-week period in March 2017. This region includes Buka Town, located on Buka Island, which serves as Bougainville's capital and hosts the ABG's headquarters. The assessment was conducted in nine different sites selected to reflect major diversities in the region (e.g., differences in lifestyle and disparities in economic development between coastal and inland as well as urban and rural areas).
Data collection
We partnered with the ABG, with logistical and technical support provided by the Department of Health (DoH). Ethical approval for the study was given by the Johns Hopkins Bloomberg School of Public Health (BSPH) Institutional Review Board, with local approval from the ABG through the Secretary of Health. Over the study period, 16 local interviewers were drawn from the DoH and other ABG staff. All staff were trained in research ethics and qualitative research methods by the BSPH supervisors (SLF and JLA).
Two different rapid qualitative methods were used in this study: free-listing and key-informant interviews. Free-listing is a structured anthropological approach for eliciting information on categories, classes, or domains (Romney & D’Andrade, 1964; Weller & Romney, 1988). It has particular utility for rapidly generating relevant items within a specific semantic or cultural domain, which makes it a valuable tool for establishing priority issues (as well as associated terminology) from the perspective of local populations (Weller & Romney, 1988). In the current study, free-listing was used to gather information on the general problems of adults in local communities in order to obtain an overview of the most salient issues in North Bougainville. From this list, we were able to identify priority MHPS problems based on the frequency with which they were mentioned as well as their apparent severity. We then explored the priority MHPS problems in more depth through key-informant interviews. Key-informant interviews are in-depth discussions with individuals who have expert or specialized knowledge in a given area, which can be used to generate richer information around a particular topic than free-listing alone (Gilchrist, 1992). The rationale behind this sequence of qualitative methods is that it allows for a broad understanding of community problems through free-listing followed by a more detailed understanding of specific MHPS problems through key-informant interviews (Applied Mental Health Research Group, 2013; Bolton & Tang, 2004; Bolton & Weiss, 2001).
A total of 54 free-list interviews were conducted across nine sites. The sample was chosen to include approximately the same number of men (n = 26) and women (n = 28). In addition, the inclusion of both younger (ages 21–43; n = 26) and older (ages 45–71; n = 28) participants ensured that we captured the viewpoints of those who were both children and adults during the Bougainville Crisis. Interviewers worked in teams of two to conduct free-list interviews in Tok Pisin, a language commonly spoken throughout Bougainville and Papua New Guinea. During free-list interviews, participants were directed to generate a list of local issues by responding to the following question: “What are the problems of persons in this community?” The wording of this primary free-list question, which asked generally about “problems” rather than referring directly to “mental health problems,” was selected to avoid participants’ preconceptions of what “mental health” means (Bolton & Tang, 2004). Each problem was recorded by a dedicated note-taker using the exact language of the participant, and interviewers repeatedly probed participants until no new problems emerged. Once a final list of problems was compiled, interviewers asked for a brief description of each problem. After completing the free-list interview, interviewers reviewed the problems and their descriptions to identify potential MHPS issues, defined as those related to thinking, feeling, or relationships (Applied Mental Health Research Group, 2013). Free-list interview participants were then asked for the names and contact information of individuals in their local community whom they believed to be knowledgeable about the highlighted problems.
The knowledgeable persons identified during the free-list interviews were later contacted as potential key informants, and were also asked to refer the research team to additional key informants. A total of 38 key informants were ultimately interviewed across seven sites, including 17 men and 21 women. This included village chiefs, religious leaders, community-based organization staff members, village health workers, teachers, and community police. As before, key-informant interviews were conducted in Tok Pisin by two interviewers, with one interviewer responsible for taking detailed notes that captured informants’ verbatim responses. Key-informant interviews were used to explore five priority MHPS problems. For each of the selected MHPS problems, key informants were asked to describe the nature of the problem, its causes, its effects, what communities currently do to address the problem, and what communities should be doing. After reaching saturation on these initial topics, a subsequent set of interviews with different key informants focused on the signs and symptoms of six common mental and emotional states that had emerged during the interviews with the first set of key informants. Throughout the data-collection process, follow-up interviews were conducted with those key informants who were found to be knowledgeable on the selected topics in order to elicit as much information as possible. In addition, detailed notes were reviewed soon after each interview by the BSPH supervisors, and suggestions were provided on whether to follow up with a particular key informant, as well as the proposed focus of the subsequent interview.
Data analysis
Qualitative data from the free-list and key-informant interviews were coded and analyzed in Tok Pisin by the local research team, with guidance from the BSPH supervisors. During the analysis of the free-list interviews, the research team condensed the individual free-lists into a composite list of problems, which included a tally of how many participants had mentioned each problem. Problems were listed exactly as they had originally been recorded in Tok Pisin, with items that used different wording but were considered the same concept combined using whichever language was thought to be most representative. The composite list was reviewed by the study investigators, in collaboration with the local research team and partners from the DoH, in order to select which MHPS problems to explore in more depth. This choice was based on which issues were most frequently mentioned, our team's perceptions of their severity, and their amenability to feasible interventions based on existing methods and available resources.
A similar procedure was followed for the analysis of the detailed notes from the key-informant interviews. During key-informant interview analysis, the research team was divided into six groups: one group for each of the selected MHPS problems identified during free-listing and one group for the signs and symptoms of psychological distress. Each of the groups reviewed all of the relevant notes, and compiled lists of the causes, effects, current community responses, and suggested community responses for their assigned topic in Tok Pisin. Responses considered to be the same were again combined using the most representative language. At the end of this process, responses were ranked and sorted according to how many key informants had mentioned each item.
Results
Free-list interviews
The summary of problem free-lists is presented in Table 1, including 32 problems that were listed by three or more participants. Upon review of these general problems, six related themes emerged: (1) substance use, including both alcohol and drugs; (2) family and intimate relationship issues; (3) lack of community infrastructure and government services; (4) violence, including both gender-based violence and generalized violence in the community; (5) lack of resources, including water, food, land, and money shortages; and (6) lack of harmony in the community, encompassing disrespectful behavior, disobedience to community norms, and an unwillingness to cooperate.
Problem free-list items mentioned by at least three respondents (N = 54)
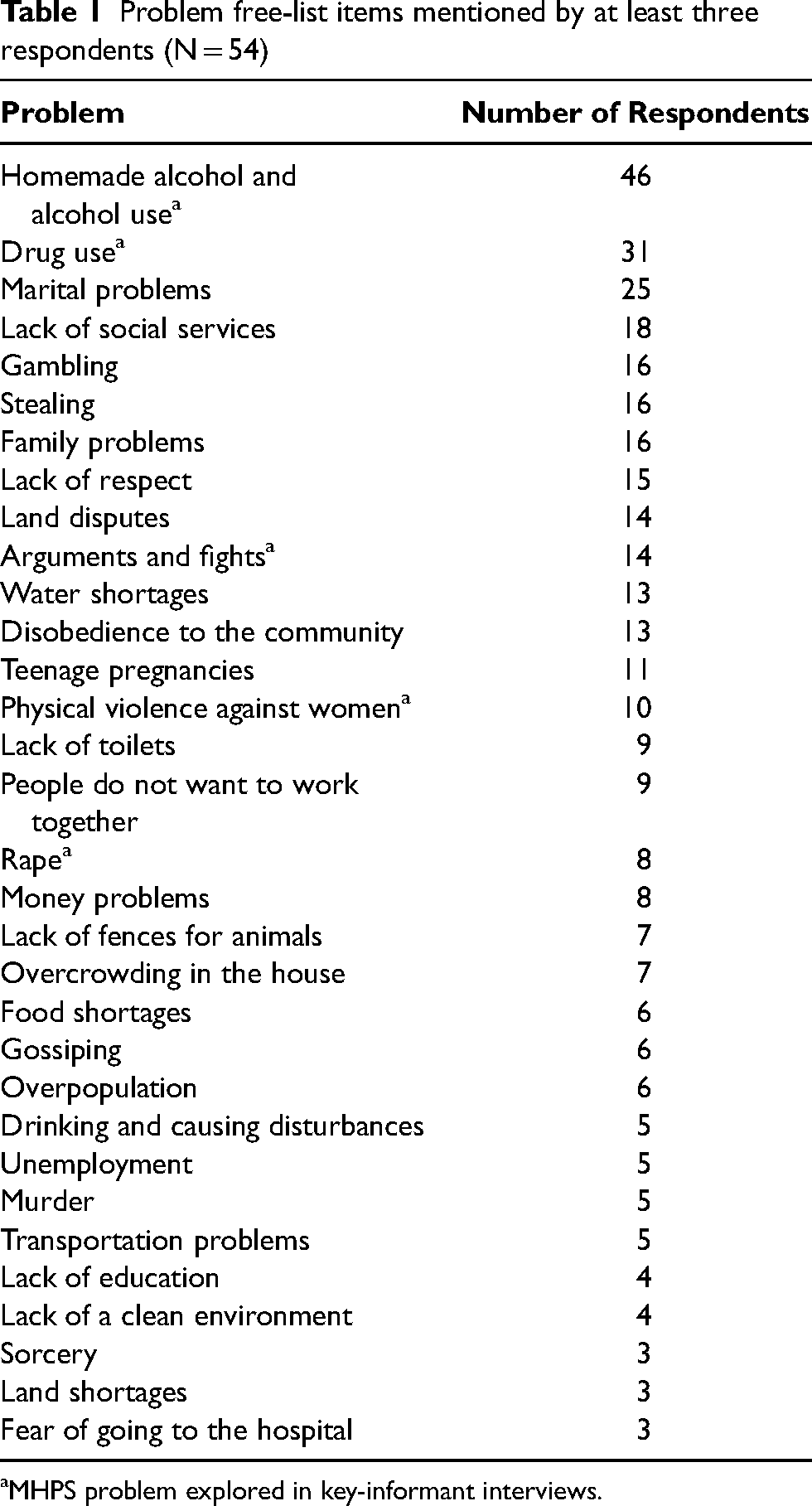
MHPS problem explored in key-informant interviews.
Key-informant interviews
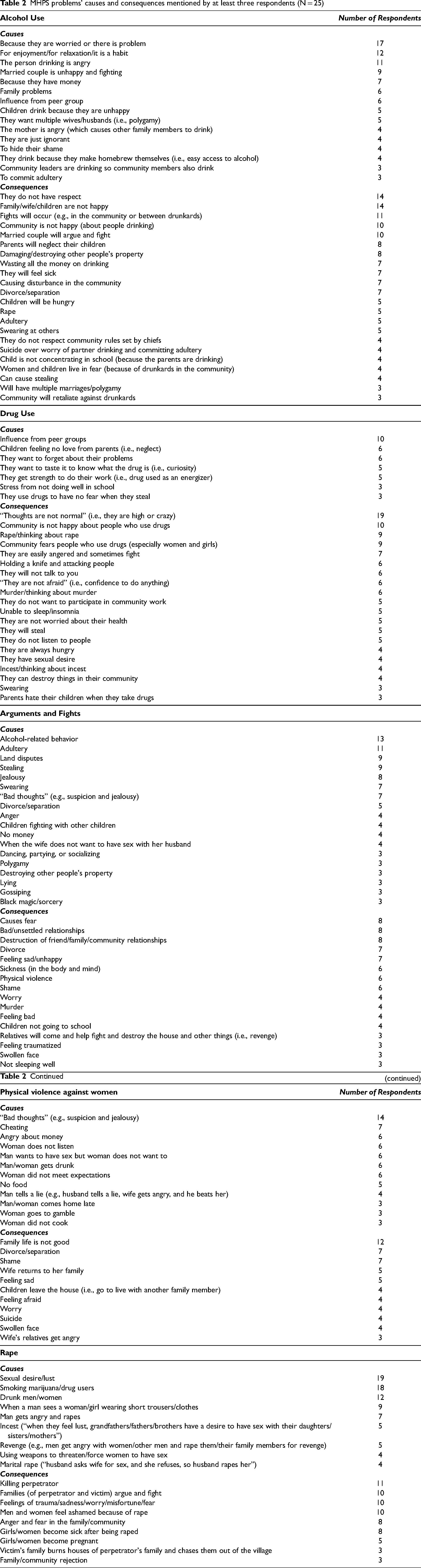
Five problems identified in the free-lists as being related to MHPS issues formed the basis for key-informant interviews. These included alcohol use by men and women (spak man/meri), drug use (plenti drug bodi), arguments and fights (koros na pait), physical violence against women (paitim meri), and rape (rape). The perceived causes and effects of these problems according to the key informants are listed in Table 2 and summarized below.
MHPS problems’ causes and consequences mentioned by at least three respondents (N = 25)
Mental health and psychosocial problems
Strategies for addressing problems
Several general suggestions were made for how communities should respond to these MHPS problems. Participants frequently suggested strengthening existing community awareness activities (e.g., community-wide meetings and trainings) as a key component to addressing these issues. Churches, village leadership, local organizations, and non-governmental organizations (NGOs) were mentioned as potential implementers of such activities. In addition, individual counseling and facilitated mediation were recurrent recommendations for addressing all of these problems. In the case of facilitated mediation, participants discussed intervention by village leadership or church elders, as well as traditional reconciliation practices. There were also multiple recommendations to build community-based projects targeting MHPS problems, whether through partnerships with existing NGOs, churches, youth programs, or welfare programs. Participants often mentioned bolstering law and order approaches for dealing with concerns around violence and substance use, including greater involvement by the police, stronger penalties for perpetrators, and increased reliance on the prison system for punishment. Finally, with regards to both alcohol and drug use, participants made several recommendations to target both supply- and demand-side issues, including halting production and sale, increasing licensing procedures, and imposing government bans. Collectively, the participant suggestions recommend a multi-sectoral approach to addressing MHPS problems in North Bougainville.
Signs and symptoms of distress
From the initial round of key-informant interviews, six frequently described mental and emotional states were chosen for further exploration in order to gain a better sense of psychosocial distress in this population. These included sadness (sori), feeling bad (pilim nogut), anger (belhat), feeling shame (pilim sem), feeling traumatized (pilim traumatised), and thinking a lot (tingting plenti). The most commonly mentioned signs and symptoms of these mental and emotional states are presented in Table 3.
Mental and emotional state signs and symptoms mentioned by at least four respondents (N = 13)
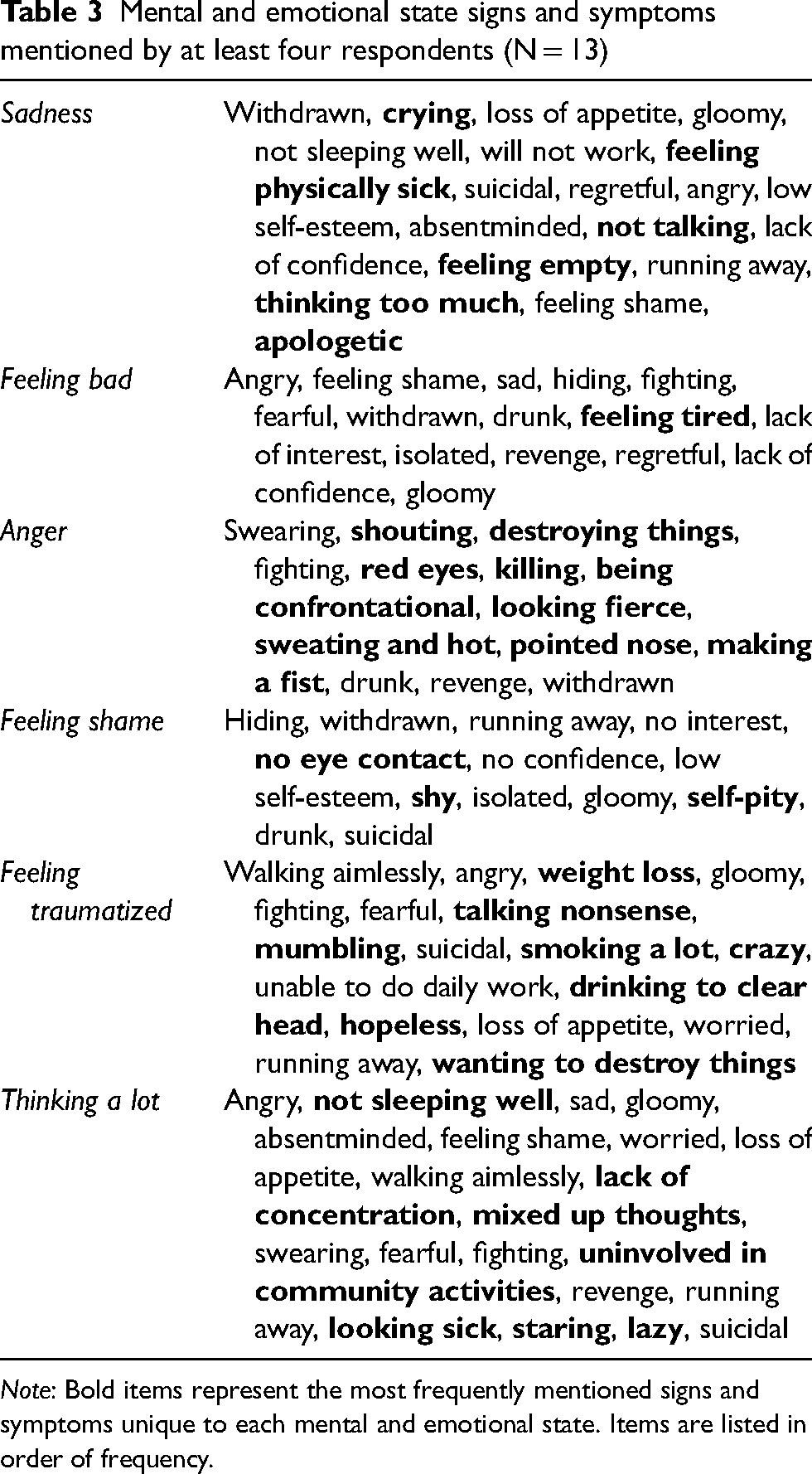
Note: Bold items represent the most frequently mentioned signs and symptoms unique to each mental and emotional state. Items are listed in order of frequency.
While interviewers asked the participants about the signs and symptoms of each mental and emotional state separately, it is clear that many signs and symptoms are common across most or all of these states. Anger, sadness, gloominess (described as having a “dry face”), and acting withdrawn (including running away, hiding, not talking, not making eye contact, and lack of confidence) were mentioned in relation to almost every state. Of these mental and emotional states, anger was characterized by the most distinctive profile, with signs and symptoms primarily related to externalizing behaviors such as swearing, shouting, destroying things, and fighting. By contrast, feelings of shame were largely associated with behaviors of social isolation, including hiding, acting withdrawn, and running away. Given the pressing concerns with substance use in this population, it is not surprising that drunkenness was connected to a number of these states. Finally, while suicide did not come up frequently in the free-list or preliminary key-informant interviews, it arose consistently across these interviews.
Discussion
The aim of this exploratory study was to elucidate local understandings of MHPS problems described by conflict-affected adults living in North Bougainville in order to contribute to the development of relevant and culturally appropriate services. These data can be used to inform the selection and targeting of problems in accordance with local priorities, the construction of suitable MHPS assessment instruments, and the design of acceptable and feasible interventions (Bolton et al., 2013; Bolton & Weiss, 2001; Murray et al., 2006; Nguyen et al., 2016). This preliminary research activity, among others, will contribute to mental health capacity-building efforts in Bougainville.
Throughout our data-collection activities, the immense burden of substance use in this population was palpable. It is not surprising that substance use arose in the initial free-list interviews: indeed, studies have highlighted the elevated prevalence of substance use among conflict-affected civilian populations in general (Lo et al., 2015, 2017), and it has previously been noted as a concern within Bougainville (Howley, 2002; Jewkes, Jama-Shai et al., 2017; Tierney et al., 2016; United Nations, 2011). The primacy of both alcohol and drug use, however, is particularly notable. Exploration of these issues in key-informant interviews exposed their pervasive use in multiple facets of daily life: individuals may brew alcohol at home, use substances socially within peer groups, take drugs as an energizer to help them work, or rely on substances to overcome inhibitions. While it is clear that not all substance use in this context is pathological – indeed, one of the most frequently cited causes of alcohol use was for enjoyment or relaxation – at their most harmful, drugs and alcohol were viewed as instigators of physical and sexual violence, aggressive behavior, destructiveness, parental neglect, and wasteful spending. Notably, prior investigations in Bougainville have drawn ties between substance use and sexual violence, interpersonal conflict, and criminal behavior, and have also suggested that substance use may stem from difficulties coping with unresolved trauma (Howley, 2002; Project, 2004; Tierney et al., 2016; United Nations, 2011).
These findings align with a growing body of evidence regarding harmful substance use in other post-conflict environments, where it has been found to contribute to interpersonal violence, economic problems, and non-communicable diseases (Ezard, 2012; Roberts & Ezard, 2015). In the absence of health and social services, it has been suggested that substance use may be a form of self-medication to ameliorate symptoms of psychological distress, or a coping strategy for dealing with emergent social and economic hardships (Ertl et al., 2016; Khantzian, 1997; Prust et al., 2017; Rhodes & Jason, 1990). Our results are consistent with this hypothesis, with participants describing substance use as a mechanism for coping with social stressors and emotional issues, and with drunkenness included as a key sign of several mental and emotional states. It has also been noted in other post-conflict settings that weak alcohol policies may limit effective enforcement and provide opportunities for national and transnational companies to expand their marketing activities, thereby contributing to increased alcohol-related harm (Wallace & Roberts, 2014). While we did not explore the regulation of alcohol in Bougainville, participants’ recommendations of the need for supply- and demand-side approaches to curbing substance use, as well as their emphasis on the widespread consumption, brewing, and selling of “home brew,” indicate that this may indeed be a contributing factor in this region.
This study also uncovered the variable nature of violence in North Bougainville, as well as the role that violence plays across multiple socio-ecological contexts. Anger and aggression were widely described, and participants reported the ways in which they may impel individuals toward acts of verbal and physical violence. Among families, it is apparent that both physical and sexual violence are of deep concern, and can contribute to the splintering of interpersonal relationships. In communities, violence can arise in relation to disputes between individuals or families, and may also manifest through such disruptive acts as stealing and destroying property. These patterns of violence mirror those in other post-conflict settings, where it has been suggested that elevated rates of interpersonal violence are tied to deepening economic stressors, disrupted family life, diminished functioning of the police and justice systems, and increased acceptability regarding the use of violence (Annan & Brier, 2010; Cardoso et al., 2016; Horn et al., 2014; Igreja et al., 2006). Research has also found that exposure to high levels of war-related violence can lead to elevated levels of interpersonal violence within families and communities (Catani et al., 2008; Hecker et al., 2015), with frustrations in the post-conflict environment triggering episodes of extreme anger and aggression among individuals who have experienced gross human rights violations (Silove, 1999; Silove et al., 2009). Recent quantitative findings from Bougainville corroborate this evidence, with enduring conflict-related social, emotional, and physical issues associated with a higher likelihood of rape and intimate partner violence perpetration (Jewkes, Jama-Shai et al., 2017).
Our exploration of mental and emotional distress in this population aligns with these patterns of violence. In particular, it is apparent that anger and resultant aggression are especially salient in North Bougainville. Anger arose frequently in relation to all of the MHPS problems that we investigated: individuals may drink alcohol when they are angry, or to cope with someone else's anger; those who use drugs may be easily angered and provoked into fighting; anger was described as both a cause and consequence of fighting in communities, intimate partner violence, and rape. In addition, anger emerged as a symptom of nearly every mental and emotional state that we explored. Pathological forms of anger have received relatively little attention in post-conflict environments compared to such mental disorders as PTSD, depression, and anxiety. One notable exception is the work of Silove and colleagues on explosive anger in Timor Leste, defined as sudden spells of intense anger that are triggered by minor environmental events, are difficult to control, and commonly result in acts of aggression (Silove et al., 2009, 2017). Not only was explosive anger highly prevalent among both men (38%) and women (44%) in Timor Leste, but it was also strongly associated with exposure to war-related trauma (Silove et al., 2009). A longitudinal study conducted among the same population found that recurrent violence, as well as associated feelings of injustice, contributed to continued patterns of explosive anger over a six-year follow-up period (Silove et al., 2017).
In addition to anger, participants described a number of depression- and anxiety-like symptoms related to existing MHPS problems. These included sadness, lack of interest, excessive worry, lack of concentration, low self-esteem, appetite loss, fatigue, sleep disturbances, and suicidality. We do not have sufficient information to determine whether these symptoms can be meaningfully grouped into distinct syndromes, or whether they comprise a unified domain of general psychological distress. The substantial overlap in symptoms revealed by our targeted exploration of mental and emotional states supports the hypothesis of general psychological distress, with a single individual frequently experiencing multiple facets of this distress. It remains possible, however, that these mental and emotional states truly are unique, despite sharing a number of key signs and symptoms. The latter interpretation is consistent with existing research from Bougainville, which found that depression, PTSD, and suicidality are pervasive among both men and women (Jewkes, Jama-Shai et al., 2017). It is important to note, however, that the mental health assessment instruments utilized in the above-mentioned study were not validated for use in Bougainville, and may therefore not appropriately capture local experiences of psychological distress.
Taken together, our findings highlight the highly interconnected relationship between substance use and violence that exists in this setting, as well as the variable psychological distress that both contributes to and results from this relationship. While qualitative data cannot be used to make statements about causality in these relationships, participants’ descriptions suggest the ways in which they are intertangled. For example, participants reported that the excessive use of drugs and alcohol may spur individuals toward such acts of violence as rape, physical abuse, fighting, murder, and destructiveness. Violence was portrayed as causing further violence: rape may be used as retaliation in response to a dispute over resources, murder may be used to avenge rape, fighting in the home can incite fighting in the community. Finally, participants described the regularity with which individuals turn to drugs and alcohol to cope with issues stemming from widespread violence in their homes and communities. While the precise connections between substance use and violence in Bougainville require further investigation, it seems clear that these issues should not be considered in isolation. Interviewees’ responses also suggest a high burden of psychological distress related to such instances of substance use and violence, with symptoms of anger and aggression particularly relevant within this population. This suggests the need for the selection and adaptation of interventions that incorporate these issues as key components of psychological distress. In addition, it warrants a more targeted exploration around manifestations of anger and aggression in North Bougainville.
Limitations
North Bougainville was chosen as the setting for this assessment due to its relative accessibility and infrastructure, which improved study feasibility and increases the likelihood of the subsequent implementation of an intervention based on these findings. Stakeholders report substantial heterogeneity across the different regions in Bougainville, however, and these findings may not be generalizable. As such, there are plans to replicate this study using the same rapid qualitative methods in other regions of Bougainville.
As mentioned previously, our approach was much briefer than that used in more intensive qualitative or ethnographic studies, and thus did not yield in-depth findings regarding MHPS issues in this population. While these data are suitable for general descriptions of some of the most prominent MHPS problems in this context, we recognize that these methods preclude a truly detailed understanding of these issues because of their limited engagement with local viewpoints. Further, due to time and budget limitations, key-informant interviews were not audio-recorded and transcribed verbatim. Instead, a dedicated note-taker was responsible for capturing informants’ responses through detailed notes, which were used during analysis. In addition, we did not explore all of the MHPS problems affecting adults in North Bougainville, and instead focused only on the most commonly mentioned problems that we perceived to be potentially amenable to intervention. Further, while this analysis relied on frequency counts of the number of free-list and key-informant respondents who gave each response, these frequencies cannot be interpreted beyond a general indicator of item saliency. As such, rather than stressing exact numerical frequency, we have instead focused more broadly on items that were reported repeatedly compared to those that were only reported by one or two participants.
Finally, there are likely topics that individuals in this context were less willing to discuss, even if these topics represent real issues with serious MHPS implications. For instance, although sorcery rarely came up in the context of our free-list and key-informant interviews, others have identified it as an important issue in Bougainville (Evenhuis, 2015; Jewkes et al., 2015). Anecdotally, we were informed that there is extreme reluctance within communities to discuss this issue. This example highlights the fact that while rapid qualitative assessments are effective in learning about topics that are important, they cannot be relied upon exclusively to provide an exhaustive list of salient issues.
Conclusions
Results from this rapid qualitative assessment suggest that violence, substance use, and psychological distress are inextricably linked in North Bougainville. In particular, findings indicate that any intervention strategy aimed toward addressing mental health in this environment should incorporate violence and substance use as both causes and consequences of psychological distress. While a number of interventions have focused separately on each of these issues, there are relatively few that have utilized an integrated approach to addressing violence, substance use, and mental health. Existing studies, conducted largely in high-income countries, have suggested that Cognitive Behavioral Therapy (CBT) approaches that combine violence and substance use may have an impact on both outcomes (Chermack et al., 2015; Easton et al., 2007; Kraanen et al., 2013; Murray et al., 2020; Satyanarayana et al., 2016). In one particularly promising example, Murray et al. (2020) used a CBT-based transdiagnostic intervention, the Common Elements Treatment Approach (CETA), to address women's experiences of intimate partner violence and men's hazardous alcohol use among couples in Zambia. Not only was CETA highly effective for both outcomes (Murray et al., 2020), but these effect sizes were largest among those who reported more severe depressive symptoms at baseline (Fine et al., 2021), suggesting the promise of integrated approaches for tackling both mental and behavioral health problems. Notably, similar CBT-based transdiagnostic interventions have been used in a number of post-conflict settings to effectively address a range of mental health issues, including anxiety, depression, and PTSD (Bolton et al., 2014; Weiss et al., 2015). This speaks to the overall potential for integrating violence and substance use components into existing evidence-based mental health strategies within the context of armed conflict.
Beyond such individual psychotherapeutic interventions, the published literature also generally supports the use of community-based structural approaches to reduce or prevent violence- and mental health-related issues in low-resource settings (Bourey et al., 2015; Williams & Thompson, 2011). For example, according to one systematic review, social and economic interventions such as microfinance programs, cash transfers, livelihoods training, community mobilization, and media campaigns were associated with decreased intimate partner violence and enhanced relationship quality in low- and middle-income countries. Together, such findings suggest that a potential strategy for addressing MHPS problems in North Bougainville could rely on structural approaches for the primary prevention of violence and substance use, as well as integrated CBT-based transdiagnostic interventions for targeting those at the highest risk. This aligns with study participants’ recommendations, with broad support for both community-based and individually focused strategies for addressing these pressing MHPS issues. These findings will be vital in contributing to subsequent activities of the Bougainville Mental Health Project, with data utilized to shape intervention planning, inform service delivery, bolster advocacy efforts, and build mental health capacity.
Footnotes
Acknowledgements
We would first like to acknowledge Sr. Essah Barnabas for her tremendous contributions toward improving mental health in Bougainville. An essential research partner and co-author of this manuscript, Sr. Barnabas sadly passed away during the publication process. We are also grateful to the Autonomous Bougainville Government for the approval of this project, with particular thanks to Secretary of Health Clement Totavun for his support of this study and review of the manuscript. We would also like to acknowledge the Bougainville Department of Health for their assistance in the implementation of this study. In particular, we would like to thank Alois Pukienei and Roselyn Gatana for providing project oversight. We are grateful to Cameron Darragh of the Australian Department of Foreign Affairs and Trade and Brett Kirkwood of Health and HIV Implementation Services Provider for their support. Finally, we would like to acknowledge the tireless efforts of the research team, without whom this study would not have been possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the United States Agency for International Development Victims of Torture Fund (Cooperative Agreement No. GHS-A-00-09-00004-00), and the Australian Department of Foreign Affairs and Trade working in partnership with the Government of Papua New Guinea and the Autonomous Bougainville Government. SF's involvement was supported by the National Institute of Mental Health's Global Mental Health Training Program (T32MH10321).