
Abstract
The current study investigated the moderating effects of COVD-19 infection severity of region of residence, and the mediating effects of resilience and self-efficacy, on the relationship between mindfulness and mental distress during the COVID-19 pandemic. A total of 1,220 participants from 107 cities in China took part in a cross-sectional survey. The data were collected during the early stages of the COVID-19 pandemic (from April 10 to June 10, 2020). The final sample comprised of 1,201 participants with a mean age of 29.62 (SD = 12.72; Range = 18–78). Participants were categorized into high, moderate, and low infection-severity areas according to the numbers of infected people and deaths in their residential areas as of April 16, 2020. The findings showed that mindfulness, resilience, and self-efficacy were negatively associated with the mental distress indicators of stress, anxiety, and depression and that mindfulness, resilience, and self-efficacy positively correlated to one another. COVID-19 infection severity in one's region of residence did not moderate the negative associations between mindfulness and stress, anxiety and depression, while resilience and self-efficacy mediated the negative relationship between mindfulness and mental distress. This study therefore sheds light on some of the mechanisms by which mindfulness helps individuals maintain good mental health in times of adversity. The inclusion of mindfulness, resilience, and self-efficacy in the design and implementation of mental health intervention in response to the pandemic and future public health crisis may help mitigate some of the mental problems related to the COVID-19 and future pandemics.
Introduction
Mindfulness, mental distress, and infection severity of region during the COVID-19 pandemic
Over the past few decades, positive psychology has recognized mindfulness as important for enhancing awareness of the present moment and competently responding to mental distress (Bishop et al., 2004). According to Kabat-Zinn (2013), mindfulness refers to “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment” (p. 145). Mindfulness is a nonjudgmental practice, through which the ongoing movement of internal and external stimuli are observed as they arise (Baer, 2003). Mindfulness promotes adaptive coping to stressful events via self-regulation of attention and an open and accepting orientation toward present experience (Bishop et al., 2004). Although mindfulness is often conceptualized as a skill that can be enhanced through practice (Kabat-Zinn, 2003), it is also viewed as a dispositional trait; that is, even without mindful practice some people are dispositionally more mindful than others (Burzler et al., 2019). Dispositional mindfulness, which is employed in the current study, is associated with a flexible state of mind and openness to novelty seeking and production—a process of actively exploring various possible solutions (Li et al., 2020; Pirson et al., 2018).
The essential elements of mindfulness, such as awareness of one's body sensations, thoughts, and emotions, and nonjudgment of one's moment-to-moment experience (Kabat-Zinn, 2013), are potential buffers against common types of mental distress, including feelings of anxiety, depression, and stress (Keng et al., 2011; Li et al., 2023). Moreover, mindfulness encourages people to decrease automatic thoughts, emotions, and behaviors, and to respond (instead of reacting) to stress through the self-regulation of emotions and behaviors (Kabat-Zinn, 2013). Keng et al.'s (2011) review of empirical studies found that trait mindfulness is negatively correlated with depression, social anxiety, negative affect, difficulties in emotion regulation, and negative automatic thoughts. Evidence from systematic reviews suggests that mindfulness-based interventions are efficacious for reducing mental distress (e.g., stress, anxiety, depression, posttraumatic stress disorder [PTSD]) in a wide range of populations, including children and adolescents (Kallapiran et al., 2015), pregnant women (Hall et al., 2016), and diabetes patients (Fisher et al., 2023; Ni et al., 2020).
The COVID-19 pandemic has posed an unprecedented threat to people's mental health (Li et al., 2021a). A systematic review on the impact of the COVID-19 pandemic on mental health among the general population reported high prevalence of anxiety (6.33% to 50.9%), depression (14.6% to 48.3%), PTSD (7% to 53.8%), mental distress (34.43% to 38%), and stress (8.1% to 81.9%) in China, Spain, Italy, Iran, the USA, Turkey, Nepal, and Denmark (Xiong et al., 2020). Existing literature suggests that mindfulness is a protective factor against mental distress caused by the COVID-19 pandemic (Antonova et al., 2021; Chiesi et al., 2022; Conversano et al., 2020; Ju et al., 2022; Lekagul et al., 2022; Li et al., 2020). In their systematic review evaluating psychological interventions and their effectiveness mitigating pandemic distress, Lekagul et al. (2022) reported that across 13 randomized controlled trials (published between January 2020 and September 2021), mindfulness meditation significantly reduced symptoms of depression, anxiety, and stress. Later investigations (Antonova et al., 2021; Chiesi et al., 2022; Ju et al., 2022) lend support to the findings of this review, suggesting that mindfulness meditation is effective for promoting good mental health during the pandemic. Several studies also indicate that dispositional/trait mindfulness can protect against mental distress consequent to the pandemic (Conversano et al., 2020; Li et al., 2020). Conversano et al. (2020) reported that greater dispositional mindfulness corresponded to significantly lower levels of mental distress during the COVID-19 pandemic.
In their longitudinal study, Li et al. (2020) reported that novelty seeking—a component of the Langer Mindfulness Scale (Pirson et al., 2018), employed in the current study to measure dispositional mindfulness—negatively correlated with stress, anxiety, and depression at all study time points. Further, the study found that the growth trajectory for novelty seeking was negatively associated with growth trajectories for depression, anxiety, and stress (i.e., a longitudinal increase in novelty seeking was associated with a longitudinal decrease in depression, anxiety, and stress). Dispositional novelty seeking is comprised of the personal factors of self-beliefs, self-construal, and novelty-outcome expectations. These factors function collectively to regulate novelty-seeking behavior. High levels of novelty seeking are often associated with high levels of cognitive flexibility (Langer, 2015). When facing stressful situations, people with high levels of dispositional novelty seeking often can explore creative ideas, and various possible solutions. Cognitive flexibility permits individuals to actively process new information, and construct new meaning in a crisis, such as the COVID-19 pandemic. Consequently, novelty seeking may support people to be mindful of the pandemic context, investigate new activities that help overcome isolation caused by the public health measures, and learn from new challenges experienced during the pandemic. Through these novelty-seeking activities and experiences, people may enhance resilience and self-efficacy, and reconstruct a sense of optimism, leading to the maintenance and improvement of mental health (Li et al., 2020).
Previous work by the current authors, based on the same dataset of the current study, revealed a link between the degree to which one's region of residence is being impacted by COVID-19 and mental distress among Chinese participants. That is, participants who lived in regions with a greater spread of COVID-19 (high infection severity) showed significantly higher levels of mental distress than those living in medium and low infection-severity areas, even when statistically controlling for group differences in demographic variables. Considering the positive effects of mindfulness when coping with stress, it may be possible that people with higher levels of mindfulness are able to maintain good mental health in the face of pandemic-related stressors. However, it is also possible that the buffering effects of mindfulness only work up to a point before acute stressors begin to overwhelm the individual's capacity to cope. In such a situation, we might expect to see a negative relationship between mindfulness and mental distress among those in low and moderate infection-severity areas, but not high infection-severity regions. In other words, infection severity may moderate the negative relationship between mindfulness and mental distress.
Possible mediating effect of resilience and self-efficacy on the relationship between mindfulness and mental distress
Resilience has also been identified as a psychological buffer against mental distress (Li & Miller, 2017). Resilience has been conceptualized as a trait, an outcome, or a process (Charbonneau, 2019). The trait approach defines resilience as a multidimensional psychological construct consisting of stable personality traits that help the individual to bounce back, recover, and thrive from adversity, challenges, and threats (Campbell-Sills et al., 2006). The outcome approach relates resilience to a set of good outcomes despite experiencing serious threats to adaptation or development (Masten, 2001). The process approach conceptualizes resilience as an active process that involves positive adaptation in the context of trauma, tragedy, threats, or significant sources of stress (American Psychological Association, 2014). Regardless of what approach is used to conceptualize resilience, the central theme is recovery and optimistic adaptation in the face of adversity. Trait resilience, which is concerned with “personal qualities that enable one to thrive in the face of adversity” (Connor & Davidson, 2003, p. 76), is employed in the current study.
Along the lines of these conceptual approaches, several scales have been standardized to measure resilience (Yu & Zhang, 2007). Among these scales, the Connor–Davidson Resilience Scale (CD–RISC; Connor & Davidson, 2003), used in the current study, was developed based on the biopsychosocial model of resilience. It consists of factors that reflect the notions of personal competence, high standards, and tenacity; trust in one's instincts, tolerance of negative affect, and strengthening effects of stress; the positive acceptance of change, and secure relationships; control; and spiritual influences (Connor & Davidson, 2003). Studies using CD–RISC have demonstrated that trait resilience can be regarded as a measure of stress coping ability and a critical target of treatment in anxiety, depression, and stress reactions (Campbell-Sills & Stein, 2007; Connor & Davidson, 2003; Yu & Zhang, 2007).
Aspects of resilience that may act to buffer mental distress include optimism, positive adjustment, effective coping strategies, self-regulation skills, self-efficacy, self-compassion, meaning of life, and supportive relationships (Li & Miller, 2017; Masten, 2019). These factors may function collectively to mitigate risks, promote better adaptation, and attenuate mental distress. The results of a meta-analysis on 76 studies showed a significantly weak, negative correlation between resilience and depression, anxiety and negative affect (Hu et al., 2015). Li and Miller (2017) reported a significantly weak, negative correlation between resilience and anxiety among older adults. During the COVID-19 pandemic, Chiesi et al. (2022) found a strong, negative relationship between resilience and psychological distress in breast cancer patients.
Research suggests the existence of moderate to strong positive correlations between mindfulness and resilience across various groups including university students (Keye & Pidgeon, 2013), prostate cancer patients (Walsh et al., 2018), and military college undergraduate students (Charbonneau, 2019). This would suggest that resilience and mindfulness share some of the same underlying factors. According to Masten (2019), resilience of an individual depends on adaptive systems that develop within the person (e.g., stress-regulation, self-regulation, and behavioral flexibility systems) when adapting to external contexts. Mindfulness may enhance the internal adaptive systems in that mindfulness training can reduce stress reactivity and increase emotional regulation and behavioral flexibility (Charbonneau, 2019). Hence, growths in mindfulness should be expected to increase resilience, which in turn would be associated with a decrease in mental distress. In other words, resilience may mediate the negative relationship between mindfulness and mental distress.
Research suggests that perceived self-efficacy plays a powerful role in regulation of emotional states (Bandura, 1997) and mental distress (Bandura, 1988; Clarke et al., 2014; Parto, 2011). Self-efficacy refers to a person's beliefs about his or her capabilities to perform specific behaviors through exercising influence over potentially threatening events (Bandura, 1994). Self-efficacy consists of specific self-efficacy and general self-efficacy. Specific self-efficacy is concerned with one's belief that one is capable to achieve good outcomes in a specific area of life (Bandura, 2012), such as in the areas of physical and mental health, academic performance, leadership, and memory (Schutte & Malouff, 2016). General self-efficacy, employed in the current study, is defined as one's overall sense of competence in tackling various life challenges across a wide range of situations (Schwarzer, 1992; Schwarzer et al., 1997).
Self-efficacious people believe in their abilities to exercise control over their thoughts, emotions, and behavior when encountering difficult situations (Schwarzer et al., 1997). According to Bandura (1988), being capable of managing and controlling threatening situations can reduce mental distress. In the cognitive and behavioral processes, it is the exercise of control, rather than the diminution of the threatening event itself, which reduces mental distress. That is, the effects of self-efficacy on mental distress are derived from a sense of control, rather than from the enhanced predictability of the adverse event. Empirical evidence supports that general/specific self-efficacy negatively correlates with mental distress. For example, Parto (2011) found a weak, negative correlation between general self-efficacy and mental distress. Clarke et al. (2014) reported weak to moderate negative correlation between mental health self-efficacy and depression, anxiety and stress. During the COVID-19 pandemic, researchers have found that self-efficacy negatively associated with COVID-19 anxiety (Bidzan et al., 2020), general anxiety (Mo et al., 2021; Zhou et al., 2021), PTSD (Bidzan et al., 2020), stress (Mo et al., 2021), and depression (Zhou et al., 2021) in various populations (e.g., healthcare professionals and community samples).
Weak-to-medium positive correlations between mindfulness and self-efficacy have been observed in various populations, including university students (Keye & Pidgeon, 2013; Leppma & Darrah, 2022; Luberto et al., 2013), patients with lower back pain (Turner et al., 2016), breast cancer patients (Chiesi et al., 2022), and Indian adults (Chandna et al., 2022). According to Kabat-Zinn (2013), the sense and ability of control are central to coping with aversity and stress. Feeling unable to control threatening situations can lead to feelings of anger, anxiety, and aggression, all driven by a (conscious or unconscious) motivation to maintain a sense of control over a situation (Kabat-Zinn, 2013). Greater mindfulness can help individuals gain a greater sense of control of their thoughts, emotions, and behavior and enhance their self-efficacy (Hosseinzadeh et al., 2021), which in turn would be expected to reduce mental distress. In other words, self-efficacy may mediate the relationship between mindfulness and mental distress. To the authors’ knowledge, there is no research exploring the parallel mediating effects of resilience and self-efficacy on the relationship between mindfulness and mental distress, particularly within the context of the COVID-19 pandemic.
The present study
The present study aims to investigate the moderating effects of infection severity of region, and mediating effects of resilience and self-efficacy, on the relationship between mindfulness and mental distress. Understanding the role that positive psychological resources (e.g., mindfulness, resilience, and self-efficacy) play in maintaining and improving mental health during a public health crisis is important. Positive psychological resources are possibly less visible compared to the medical interventions (e.g., vaccinations) at play in the fight against COVID-19. However, positive psychological resources may contribute significantly to support individuals to maintain mental health during the COVID-19 pandemic. Mindfulness was chosen as the independent variable because systematic reviews and meta-analyses suggest a causal relationship between mindfulness-based interventions (MBIs) and mental health (particularly symptoms of depression, anxiety, and stress) during the COVID-19 pandemic (Duarte et al., 2022; Witarto et al., 2022). The findings of the present study will provide mindfulness researchers and practitioners with empirical evidence on the relationship between mindfulness and mental distress and potentially elucidate the underlying mechanism (e.g., the mediating effect of resilience and self-efficacy) of this relationship.
The conceptualization of mindfulness, resilience, and self-efficacy provide theoretical underpinnings that support the mediating roles of resilience and self-efficacy in the mediation model tested as part of the present study. As posited by Langer (2015) and Kabat-Zinn (2013), mindfulness is associated with positive emotions and psychological and behavioral flexibility. Positive emotions, and the psychological and behavioral flexibility to utilize these positive emotions, are regarded as integral to trait resilience. In turn, trait resilience enables individuals to exploit positive psychological resources (e.g., adaptive capacities), promoting flourishing from adversity and lowering the likelihood of mental distress (Davydov et al., 2010). Similarly, according to Bandura (1997), positive emotional states (e.g., calmness and stability of emotions) are among the sources of influence upon which self-efficacy develops. Positive emotions serve as markers of optimal well-being and mental health (Leppma & Darrah, 2022). Hence, trait resilience and self-efficacy may play mediating roles in the relationship between mindfulness and mental distress.
Due to the exploratory nature of the current study, instead of a priori hypotheses, two research questions (RQs) are proposed:
As depicted in Figure 1, does severity of infection in one's region of residence moderate the relationship between mindfulness and mental distress?

The theoretical model of the proposed moderation model.
As depicted in Figure 2, does resilience and self-efficacy mediate the relationship between mindfulness and mental distress?

The theoretical model of the proposed mediation model.
Methods
Participants
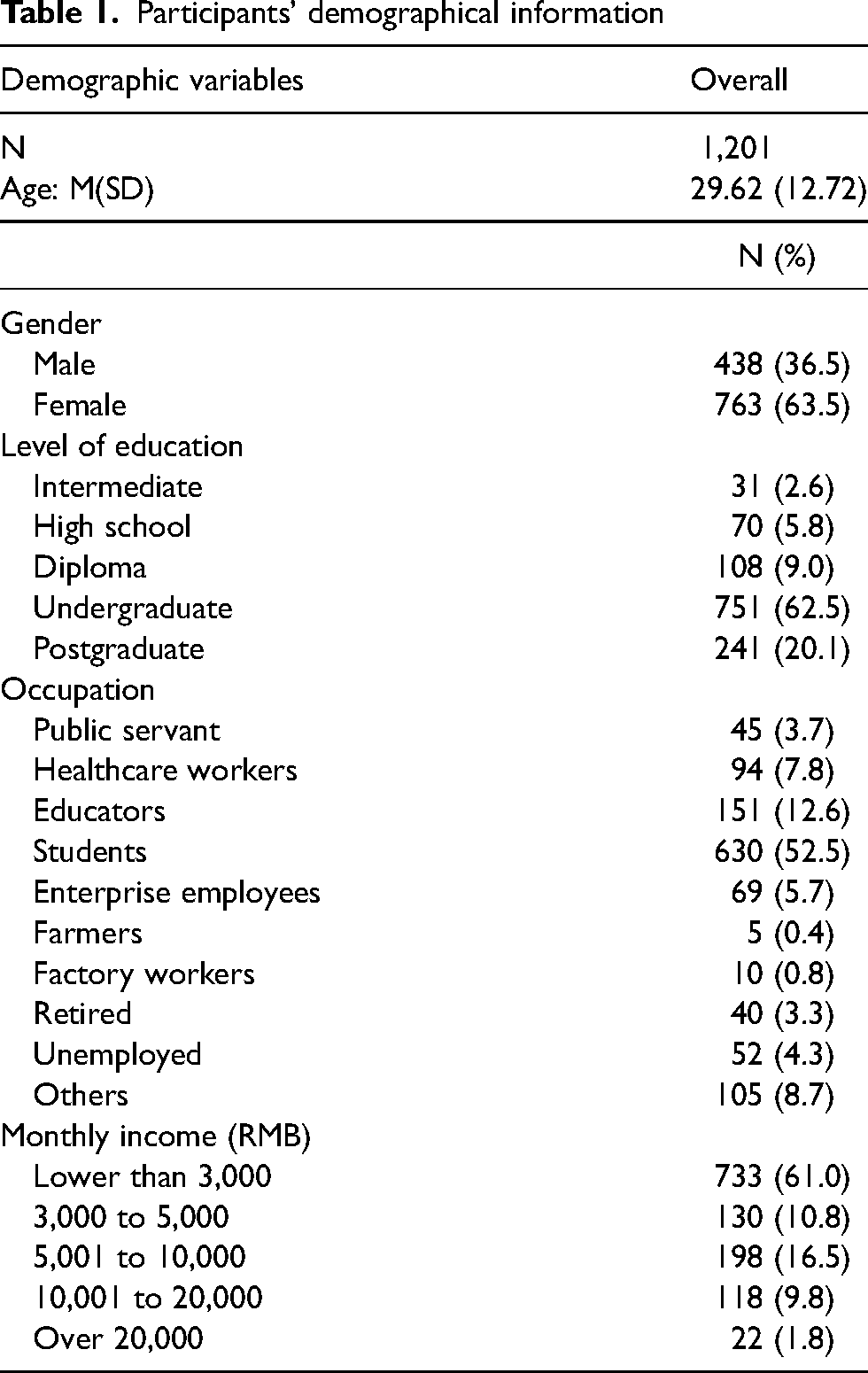
The inclusion criteria were Chinese residents aged 18 years and over who possessed the ability to read the questionnaire. The participants were residents (N = 1,220) of 107 cities in China. The data were collected over a period of two months (April 10 to June 10, 2020) during the spread of COVID-19 in China. Following data cleaning, the final sample comprised of 1,201 participants (females = 63.5%), with a mean age of 29.62 (SD = 12.72; Range = 18–78). As reported in previous work by the current authors (Li et al., 2021a), the final sample included 23.4% (n = 281) participants living in a high infection-severity area (Wuhan city), 13.4% (n = 162) in a moderate infection-severity area of nine cities in Hubei province outside of Wuhan, and 63.1% (758) in a low infection-severity area of 97 cities elsewhere in China. Table 1 shows the demographic characteristics of participants.
Participants’ demographical information
Measures
Demographic variables
Participants completed demographic questions about potential covariates (i.e., age, gender, educational attainment, occupation, and income).
Infection severity of region of residence
In contrast to individual infection severity, infection severity of region of residence concerns the severity of infection in the specific geographic locale in which a person lives. As reported in the previous work by the current authors (Li et al., 2021a), infection severity in region of residence was assigned based on the number of COVID-19 infections and deaths in the participant's geographic area as of April 16, 2020, in the current study. According to The National Health Commission of China (2020), as of April 16, 2020, the number of infected people and deaths were 50,333 and 3,869, respectively, in Wuhan (located in Hubei province); 17,795 and 643, respectively, in Hubei province excluding Wuhan; and 14,564 and 120, respectively, elsewhere in China. Hence, we categorized Wuhan, Hubei province excluding Wuhan, and elsewhere in China, as high, moderate, and low infection-severity areas, respectively.
Mental distress
Mental distress was measured using the 21-item standardized Chinese version of the Depression Anxiety Stress Scale (C-DASS21; Taouk et al., 2001) to evaluate participants symptoms of depression (e.g., “I could not seem to experience any positive feeling at all”), anxiety (e.g., “I was aware of the dryness of my mouth”), and stress (e.g., “I found it hard to wind down”). Participants rated each item on a four-point Likert scale from 0 = did not apply to me at all to 3 = applied to me very much, most of the time. Scores were summed where higher scores indicate greater level of depression, anxiety, and stress symptoms. Several recent studies have demonstrated that the Chinese version of the DASS has good internal consistency: depression (Cronbach's alpha = 0.83 to 0.88), anxiety (0.78 to 0.87) and stress (0.83 to 0.87) (e.g., Jiang et al., 2020; Li et al., 2020; Li et al., 2021a; Li et al., 2020b; Xie et al., 2021). Confirmatory factor analysis (CFA) using maximum likelihood estimation with three first-order factors (stress, anxiety, and depression) employing the IBM SPSS Amos Graphics v28 was performed to test the model fit of the C-DASS. After modifying the model based on the modification indexes, model fit indexes suggested an adequate-fitting model—χ2(178) = 1,491.78, p < .001, Comparative Fit Index (CFI) = .93, Tucker–Lewis Index (TLI) = .91, Goodness of Fit Index (GFI) = .88, Root Mean Square Error of Approximation (RMSEA) = .08, 90% CI [.07, .08], Standardized Root Mean Square Residual (SRMR) = .04—supporting the proposed factor structure of the C-DASS.
Mindfulness
Mindfulness was measured by the 12-item Chinese version of the Langer Mindfulness Scale (C-LMS). The C-LMS was translated from the 14-item English LMS (Pirson et al., 2018). To ensure the quality of the translated scale and equivalence between English and Chinese versions, translation and back translation were applied by the research team. This involved four steps: (1) a professional bilingual translator translated the English scale into Chinese; (2) a second professional bilingual translator translated this Chinese version back into English; (3) the original English version and the translated English version were compared by the research team; and (4) for items where substantial differences existed between the two English versions, another Chinese translation was prepared containing modifications designed to eliminate discrepancies. The process was repeated until the two English versions were identical or contained only minor differences. This resulted in a pre-final version of the C-LMS ready for pilot testing. The pre-final version was pilot-tested among 20 university students in China to evaluate the clarity of instructions and items. Each participant was asked to rate the instructions and each item of the scale using a dichotomous scale (clear or unclear). Thirteen items were rated as clear by 95% of the participants and one reverse item was rated as unclear by over 20% of the participants. In a focus-group setting, the 20 students who participated in the pilot testing were asked to provide suggestions as to how to rewrite this item to make the phrasing clearer. The item was translated and back-translated again.
The 14-item LMS has three subscales: novelty seeking (5 items), novelty production (5 items), and engagement (4 items). All items of the scale were rated using 7-point Likert-type formats (where 1 = Strongly disagree and 7 = Strongly agree). Authors of the scale suggested that it is permissible to sum all items for a total score of overall mindfulness, with higher scores indicating higher levels of mindfulness (Pirson et al., 2018). Examples of items include “I like to investigate things,” “I make many novel contributions,” “I am very creative,” and “I am very curious.” There were six reverse coded items. The LMS has demonstrated good internal consistency with Cronbach's alphas ranging from .83 to .90 across samples (Pirson et al., 2018). A CFA with three first-order factors was conducted. The standardized factor loadings of two items (items 2 [“I generate few novel ideas”] and 14 [“I am not an original thinker”]) were lower than 0.20. These two items are negatively worded, which may have contributed to their low-factor loadings. Negatively worded items may be interpreted differently across cultures (Salazar, 2015; Tsang et al., 2017). In many cultures, answers to negatively worded items differ from answers to positively worded items, which may lead to a “negative item bias” (Lindwall et al., 2012, p. 197). For example, Wong et al. reported that recognition of negative items among US participants is more viable than among Asian participants (Wong et al., 2003). After removing these two items, model-fit indexes indicated that the model showed a good fit to the data: χ2(51) = 338.19, p < .001, CFI = .95, TLI = .94, GFI = .96, RMSEA = .07, 90% CI [.06, .08], SRMR = .05. Consequently, the 12-item C-LMS was used in the current study. Both the 12-item and 14-item C-LMS are presented in S1 in the Online Supplemental Materials.
Resilience
Resilience was measured by the standardized Chinese version of the short-from CD–RISC (Campbell-Sills & Stein, 2007; Connor & Davidson, 2003; Yu & Zhang, 2007). The CD–RISC consists of 10 items, each of which is self-rated on a 5-point scale (where 0 = Not true at all and 4 = True nearly all of the time), with higher total scores indicating more resilience. Example items include: “I am able to adapt when changes occur,” “I can deal with whatever comes my way,” “Having to cope with stress can make me stronger,” “I believe I can achieve my goals, even if there are obstacles,” and “Under pressure, I stay focused and think clearly.” The CD–RISC has good internal consistency with Cronbach's alpha of .91 being reported (Yu & Zhang, 2007). The results of a CFA suggested good model fit: χ2(29) = 171.43, p < .001, CFI = .99, TLI = .98, GFI = .97, RMSEA = .06, 90% CI [.06, .07], SRMR = .02.
Self-efficacy
The Chinese General Self-Efficacy Scale (C-GSE; Leung & Leung, 2011; Schwarzer et al., 1997) was used to measure perceived self-efficacy. The measure consists of 10 items self-rated on a 4-point format (where 1 = Not at all true and 4 = Exactly true). Higher total scores indicate greater self-efficacy. Example items include: “I can always manage to solve difficult problems if I try hard enough,” “If someone opposes me, I can find means and ways to get what I want,” and “It is easy for me to stick to my aims and accomplish my goals.” The C-GSE has sound reliability with Cronbach's alpha of .89 reported in Leung and Leung's (2011) study. The results of a CFA suggested good model fit: χ2(29) = 237.26, p < .001, CFI = .98, TLI = .96, GFI = .96, RMSEA = .08, 90% CI [.07, .14], SRMR = .02.
Cronbach alphas for each scale in the current dataset are presented in Table 2. The models of the CFA analyses of all scales are presented in S2 in the Online Supplemental Materials.
Zero-order correlations between continuous variables and Cronbach alphas
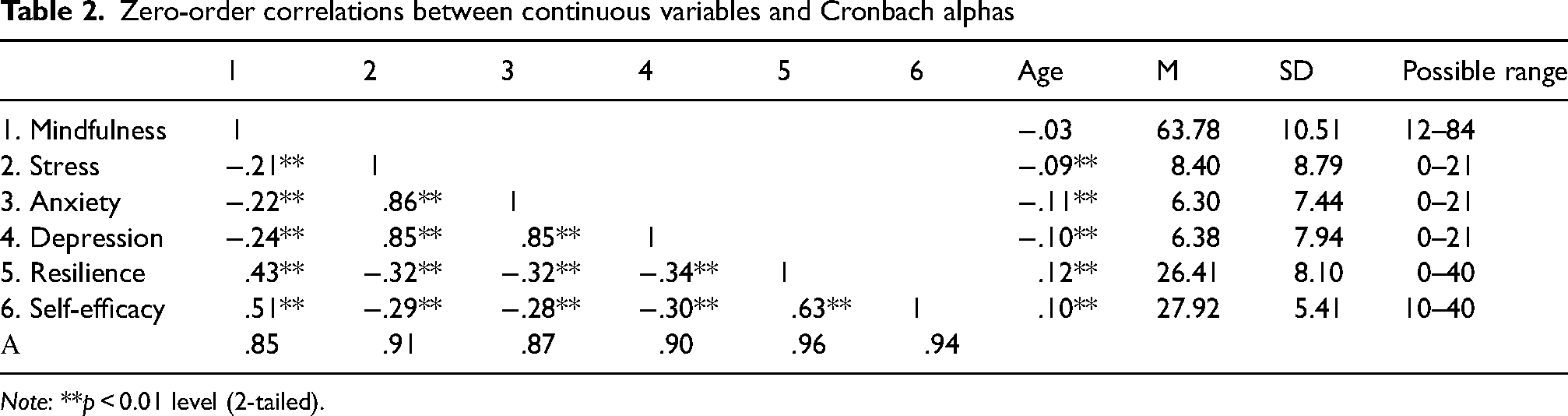
Note: **p < 0.01 level (2-tailed).
Procedure
Data collection was conducted online using Wenjuanxing (https://www.wjx.cn), a survey portal for Chinese respondents (Mei & Brown, 2018). The link was distributed to potential participants who were recruited via the social media app WeChat and through various professional and personal networks of the researchers using convenience sampling. The data collection did not commence until ethics approval was issued by the Human Research Ethics Committee of the Department of Social Work, Foshan University, China (ref. 2020001).
Data cleaning
After removing 11 unengaged responses (e.g., selecting the same values for all questions), univariate outliers were identified using boxplots, whereas Mahalanobis distances values were used to identify multivariate outliers (using an alpha of .001; see Tabachnick & Fidell, 2013, p. 99). There were nine univariate outliers that were replaced with the highest values that were not outliers. Eight multivariate outliers were detected and removed. The data cleaning process results in a final sample of 1,201.
Analysis
Data analysis was performed using IBM's SPSS version 28. Bootstrapped Analysis of variance (ANOVA; number of samples = 5,000 with 95% confidence intervals) and chi-square tests were employed to determine whether demographic variables differed in the sample and whether mindfulness, resilience, and self-efficacy differed across the three infection-severity groups. Three moderation models (using Model 1 of PROCESS V4.0 macro for SPSS; Hayes, 2018) and three parallel multiple mediator models (using Model 4 of PROCESS V4.0 macro for SPSS; Hayes, 2018)—one for each mental distress variable—were used to test RQ1 and RQ2, respectively. In the moderation models, infection severity was entered as a categorical variable using the using simple indicator coding with the reference group being the low infection-severity group.
Results
Preliminary analysis
Existing literature suggests statistically significant difference in mindfulness between age, gender, and income groups (Cheung et al., 2020; Jensen et al., 2019). Education and occupation are often positively associated with income. In other words, age, gender, education, occupation, and income may affect mindfulness and in turn have an impact on the outcome variable of mental distress. Hence, these were considered as potential covariates. Small but significant zero-order correlation was observed between age and all continuous study variables (Table 2). A chi-square test revealed that infection-severity groups differed with respect to gender, χ2 = (2, N = 1,201) = 42.40, p < .001, Cramer's V = .19; educational attainment, χ2 = (8, N = 1,201) = 183.21, p < .001, Cramer's V = .28; occupation, χ2 = (18, N = 1,201) = 463.06, p < .001, Cramer's V = .44; and monthly income, χ2 = (8, N = 1,201) = 141.75, p < .001, Cramer's V = .24. Consequently, age, gender, education, occupation, and monthly income were entered as covariates in the moderation (RQ1) and mediation (RQ2) models.
One-way between-groups ANOVAs were used to determine if mindfulness, resilience, and self-efficacy differed across the three COVID-19 infection-severity groups. Mindfulness was not found to significantly differ across the three infection groups, F(2, 1,198) = 1.66, p = .19, η2 = .003: Mild (M = 63.37, SD = 10.33); Moderate (M = 64.82, SD = 11.09); and Severe (M = 64.27, SD = 10.64). Similarly, no significant differences were observed for resilience—F(2, 1,198) = .76, p = .47, η2 = .001; Mild (M = 26.19, SD = 7.93); Moderate (M = 26.77, SD = 9.55); and Severe (M = 26.80, SD = 7.67)—or self-efficacy—F(2, 1,198) = 1.62, p = .20, η2 = .003; Mild (M = 27.71, SD = 5.13); Moderate (M = 28.40, SD = 6.75); and Severe (M = 28.22, SD = 5.28). Thus, infection severity was not entered as a covariate in the mediation models.
As shown in Table 2, mindfulness, resilience, and self-efficacy all exhibited small, negative correlations with stress, anxiety, and depression. Table 2 also shows small-to-medium positive correlations between mindfulness, resilience, and self-efficacy.
Test of RQ1
The moderation models explained 10.02% of the variance in stress, F(8, 1,192) = 16.60, p < .001; 8.69% of the variance in anxiety, F(8,1,192) = 14.17, p, .001; and 9.96% of the variance in depression, F(9, 1,191) = 16.48, p < .001. Even when controlling for age, gender, education, occupation, and income, mindfulness remained a negative predictor of stress, B = −0.13, t = −4.61, p < .001, 95% CI [−.13, −.07]; anxiety, B = −0.10, t = −4.03, p = .001, 95% CI [−.15, −.05]; and depression, B = −0.12, t = −4.64, p < .001, 95% CI [−.17, −.07].
In all models, the Mindfulness × Infection Severity interaction terms were nonsignificant: stress, ΔR2 = .008, F(1, 1,192) = 1.11, p = .29 with B = 0.02, t = 1.05, 95% CI [−.01, .05]; anxiety, ΔR2 = 0, F(1, 1,192) = .03, p = .87 with B = 0.002, t = 1.63, 95% CI [−.02, .03]; and depression, ΔR2 = .0001, F(1, 1,192) = .09, p = .77 with B = 0.004, t = .30, 95% CI [−.02, .03]. That is, the negative associations between mindfulness and stress, anxiety and depression were not moderated by infection severity of the region of residence. Thus, RQ1 was not affirmed.
Test of RQ2
Mediation models were specified in which mindfulness was the predictor variable and stress (Model 1 in Table 3), anxiety (Model 2 in Table 3), and depression (Model 3 in Table 3) were outcome variables, with resilience and self-efficacy being parallel mediators. Demographic variables (e.g., age, education, gender, income, and occupation) were entered into the models as covariates.
Path coefficients, effects, and 95%CI of the mediation models

Note: ***p < .001, **p < .01, *p < .05; X: Mindfulness; M1: Resilience; M2: Self-efficacy; Y: Model 1—stress, Model 2—Anxiety, Model 3—Depression; values in parentheses refer to pathways in the mediation diagram (Figure 2); effect size: standardized coefficient; indirect effect: completely standardized indirect effects of X on Y.
With regard to Model 1 (depicted in Figure 3), together mindfulness, resilience, and self-efficacy explained a significant portion of the variance in stress, R2 = .22, F(6, 1,194) = 55.68, p < .001. The indirect effect of mindfulness on stress through resilience (a1b1) was found to be significant (as indicated by the bootstrapped 95% CI around this indirect effect being entirely below 0) as was the indirect effect of mindfulness on stress through self-efficacy (a2b2). The direction of the path coefficients (reported in Table 3) and significant indirect effects are consistent with a model in which mindfulness bolsters resilience and self-efficacy, which then work to reduce feelings of stress.

The statistical model of the mediating effects of resilience and self-efficacy on the relationship between mindfulness and stress.
In Model 2 (Figure 4), mindfulness, resilience, and self-efficacy were again found to explain a significant portion of the variance in anxiety, R2 = .14, F(8, 1,192) = 23.81, p < .001. As in Model 1, both indirect effects were significant and the direction of pathways was consistent with a model in which mindfulness bolsters resilience and self-efficacy, which then acts to reduce symptoms of anxiety.
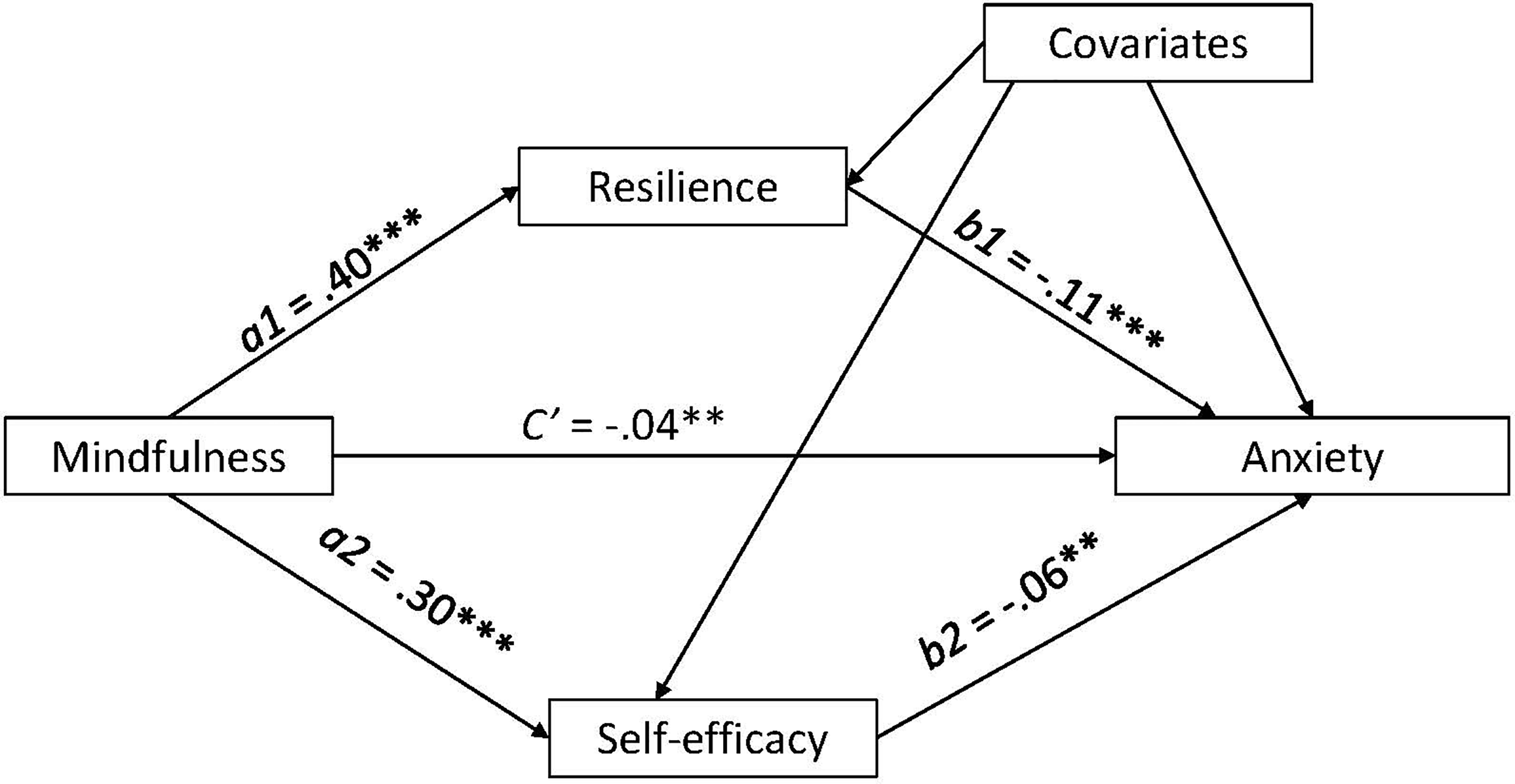
The statistical model of the mediating effects of resilience and self-efficacy on the relationship between mindfulness and anxiety.
The findings for Model 3 (Figure 5) were mirrored those for Models 1 and 2. Together mindfulness, resilience, and self-efficacy explained a significant portion of the variance in depression, R2 = .16, F(8, 1,192) = 27.40, p < .001, and both indirect effects were significant, and the direction of path coefficients were consistent with the casual model specified as part of RQ2. Overall, the mediation models supported RQ2.

The statistical model of the mediating effects of resilience and self-efficacy on the relationship between mindfulness and depression.
Discussion
This study aimed to explore the moderating effects of infection severity of region of residence, and the mediating effects of resilience and self-efficacy on the relationship between mindfulness and mental distress during the COVID-19 pandemic. The preliminary analysis showed that mindfulness, resilience, and self-efficacy were negatively associated with the mental distress indicators of stress, anxiety, and depression. These findings are consistent with existing literature (Bandura, 1988; Chiesi et al., 2022; Clarke et al., 2014; Hall et al., 2016; Hu et al., 2015; Kabat-Zinn, 2013; Kallapiran et al., 2015; Keng et al., 2011; Li & Miller, 2017; Ni et al., 2020; Parto, 2011). The preliminary analysis also showed that mindfulness, resilience, and self-efficacy positively correlated to one another, which is again consistent with prior research (Chandna et al., 2022; Charbonneau, 2019; Chiesi et al., 2022; Keye & Pidgeon, 2013; Leppma & Darrah, 2022; Luberto et al., 2013; Turner et al., 2016; Walsh et al., 2018).
The test of RQ1 indicates that the COVID-19 infection severity of the region of residence did not moderate the negative associations between mindfulness and stress, anxiety and depression. That is, it was not the case that a negative correlation between mindfulness and mental health was observed in low infection-severity group, but not in the more severely groups. Rather, greater mindfulness predicted lower levels of mental distress across all three infection-severity groups. These findings suggest the generalized benefit of mindfulness to Chinese people's mental health, even for those who lived in the highly infected areas and were likely to experience extreme COVID-19-related adversity. This finding is consistent with existing literature indicating that greater mindfulness is associated with less mental distress in the time of the COVID-19 pandemic (Li et al., 2023). A recent systematic review showed that mindfulness is negatively correlated with anxiety and depression (Xu et al., 2023). According to Langer (2015), dispositional mindfulness is associated with greater cognitive flexibility. Cognitive flexibility may allow people to actively adjust to challenging situations during the COVID-19 pandemic through restructuring mental resources and balancing competing needs between public health measures (e.g., social isolation and lockdown) and personal freedom (Li et al., 2020). As such, people are likely to gain new perspectives related to the COVID-19 crisis, even when they live in a high COVID-19 infection-severity areas.
The test of RQ2 shows that resilience and self-efficacy mediated the negative relationship between mindfulness and mental distress. That is, greater mindfulness was associated with higher levels of resilience and self-efficacy, which in turn were associated with lower levels of stress, anxiety, and depression. To the authors’ knowledge, this study is the first investigating the parallel mediating effects of resilience and self-efficacy on the relationship between mindfulness and mental distress. Mindfulness can be built upon the process of bringing a person's attention to the present moment (including the pleasant and unpleasant), without judgement and with acceptance (Kabat-Zinn, 2013). The willingness and skills to attend to pleasant and unpleasant stimuli and situations may be associated with positive appraisal, growth from adversity, and psychological and behavioral flexibility, which are the fundamental elements of resilience (Richardson, 2002). The ability to positively appraise stressful events and to grow from adversity, and the psychological and behavioral flexibility in turn may be associated with lower levels of stress, anxiety, and depression when facing crisis situations, such as the public health crisis of the COVID-19 pandemic. Moreover, mindfulness promotes the beliefs that feelings are constantly changing and transitory. This belief may prevent the psychological tendency to extend adversity into the future and encourage individuals to believe in one's ability to successfully manage stressful situations and emotions (Luberto et al., 2013), which may be in turn be associated with better mental health.
There are several limitations in the current study. First, the current study employed a cross-sectional design. As such, it is not possible to determine that certainty increases in resilience and self-efficacy are caused by mindfulness. Rather, we can only safely conclude that the finding reflects such a causal model. Second, the sample was relatively highly educated, with 83% participants completing undergraduate and postgraduate education. Moreover, participants were predominately employed in skilled occupations. Consequently, apart from positive personal resources of mindfulness, resilience and self-efficacy, the participants might have more social resources to cope with the COVID-19 pandemic and be less likely to experience financial difficulties caused by the COVID-19 quarantine measures, compared to their counterparts who may have lower levels of education and fewer social resources to draw on. Third, the removal of two items from the 14-item C-LMS is an alert that the results of the current study may not be comparable with the literature. Further research into the psychometrics of the 14-item C-LMS in other Chinese population groups is needed. Fourth, resilience and self-efficacy were correlated, and thus it is possible that self-efficacy is an antecedent factor of resilience. This possibility warrants future research to investigate the possible serial mediating effects of general self-efficacy and resilience on the relationship between mindfulness and mental distress.
Despite these limitations, the current study identifies some potential mechanisms by which mindfulness influences mental health during the COVID-19 pandemic. In this way, the study is a timely effort to advance theoretical understandings of mindfulness and clinical practice and research in supporting people to utilize mindfulness along with resilience and self-efficacy to cope with pandemic-related stressors. Considering no previous studies have examined the impact of infection severity of region on the relationship between mindfulness and mental distress, the present study enhances knowledge in this research area. Specifically, it adds valuable contribution to the work of Li et al. (2021a) that found the negative association between filial piety and mental distress is relatively consistent across regions with low, medium, and high infection severity. Along with filial piety, mindfulness practice can be integrated into public health programs as a strategy to help Chinese people maintain good mental health when facing future pandemic crises (Li et al., 2021a).
The current finding of the parallel mediating effects of resilience and self-efficacy on the relationship between mindfulness and mental distress also contributes to the theoretical knowledge in this area of research. The present study indicates that one of the mechanisms through which mindfulness bolsters mental health during crises such as pandemics is via its influence on resilience and self-efficacy. These findings suggest that in future public health crises, screening mindfulness, resilience, and self-efficacy may be beneficial to identify people early who have lower levels of each, and thus are more vulnerable to developing psychological distress. During public health crises and future pandemics, these people will likely benefit from psychological interventions that enhance mindfulness, resilience, and self-efficacy to effectively reduce psychological distress. For example, mindfulness-based interventions (MBIs) have been proven to be effective in enhancing mindfulness and reducing mental distress (Fisher et al., 2023; Kabat-Zinn, 2003, 2013). The inclusion of mindfulness, resilience, and self-efficacy in the design and implementation of mental health intervention in response to future public health crisis may help mitigate some of the mental problems related to future pandemics.
Supplemental Material
sj-docx-1-pac-10.1177_18344909231192765 - Supplemental material for The relationship between mindfulness and mental distress in Chinese people during the COVID-19 pandemic: Moderating effects of infection severity of region and mediating effects of resilience and self-efficacy
Supplemental material, sj-docx-1-pac-10.1177_18344909231192765 for The relationship between mindfulness and mental distress in Chinese people during the COVID-19 pandemic: Moderating effects of infection severity of region and mediating effects of resilience and self-efficacy by Wendy Wen Li, Daniel Miller, Timothy Leow, Carolyn Heward, Yahong Li, Fang Yang and Huizhen Yu in Journal of Pacific Rim Psychology
Footnotes
Acknowledgements
The authors sincerely thank Professors Jonathan Davidson and Kathryn Connor granted permission for the use of the Chinese CD–RISC-10 in this COVID-19-related project.
Authors’ contributions
WL contributed to study design, data collection, data analysis, data interpretation, and writing. DM contributed to study design, data analysis, data interpretation, and writing. TL contributed to study design, data interpretation, and writing. CH contributed to study design, data interpretation, and the revision of the manuscript. YL and FY contributed to study design, data collection, and project administration. HY contributed to study design and data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.