
Abstract
Background:
Increasing concern regarding long-term consequences of mild traumatic brain injury (mTBI; concussion) highlights the need for an accurate understanding of its epidemiological landscape. Current estimates of mTBI presentations to the emergency department (ED) are based on principal diagnosis International Classification of Diseases, Tenth Revision, Australian Modification (ICD-10-AM) S06.0~ concussive injury codes assigned by the treating ED clinician in the ED information system (EDIS). While mTBI is defined by absence of loss of consciousness (LOC) or LOC < 30 minutes, the S06.0~ codes include injuries associated with longer periods of LOC. To ensure reliable case estimates to inform healthcare resource allocation, it is essential to understand which S06.0~ codes most accurately capture mTBI and to minimise its misclassification.
Objective:
To identify the positive predictive value (PPV) of principal diagnosis S06.0~ codes for mTBI using information from EDIS and retrospective chart review.
Method:
All episodes of care assigned principal diagnosis S06.0~ codes between 1 July 2022 and 30 June 2023 at Royal Perth Hospital ED, Western Australia, were identified, and clinical diagnoses were confirmed via medical record review. PPVs were calculated for each S06.0~ code, and logistic regression models implemented (RStudio v4.3.3) to explore the influence of patient characteristics on coding.
Results:
Code S06.00 was most frequently assigned (n = 279, 51.7%). No cases were coded S06.04 or S06.05 (>24 hours LOC). For mTBI, the adjusted PPV of S06.0~ was 71.8% (95% confidence interval (CI) 66.85–76.22), increasing to 74.0% (95% CI 68.72–78.69) after excluding S06.03 (LOC 30 minutes to 24 hours). The highest PPV was observed for the four-digit S06.0 code (adjusted PPV = 87.0%; 95% CI 74.36–93.90). PPVs were lower among patients arriving via emergency transport, older adults (>65 years), and cases without a documented injury mechanism.
Conclusion:
There are limitations to using ICD-10-AM concussive injury codes to identify mTBI in ED settings, and patient characteristics influence coding accuracy. Reconsideration of current ED coding practices, including exploration of alternative models that reduce clinician burden and improve coding accuracy, is recommended.
Implications for health information management practice:
The introduction of electronic medical records provides an opportunity to standardise documentation of key clinical findings and develop artificial intelligence tools to improve coding of mTBI.
Keywords
Introduction
Mild traumatic brain injury (mTBI; concussion) is increasingly recognised as a cause of persisting functional impairment (Nelson et al., 2019; Theadom et al., 2016) and poorer socioeconomic outcomes (Lystad et al., 2023; Sariaslan et al., 2016; Theadom et al., 2023). As the initial point of contact for many experiencing mTBI (Thorne et al., 2022), the hospital emergency department (ED) has the potential to provide a rich data source covering diverse patient cohorts with differing mechanisms of injury and injury modes. However, inconsistent clinical practices and variability in documentation (Pozzato et al., 2020) results in episodes of care that may be misclassified when coded, hindering cohort identification.
mTBI is defined by a Glasgow Coma Scale (GCS) of 13–15, with an absence of or less than 30 minutes of loss of consciousness (LOC) and less than 24 hours of related post-traumatic amnesia (PTA; Silverberg et al., 2023). This diagnosis includes those with an absence of trauma-related intracranial abnormalities on neuroimaging (uncomplicated or non-complex) who would typically be provided with a clinical diagnosis of concussion but can also include those with trauma-related intracranial imaging abnormalities, a subgroup referred to as “complex mTBI” (Carroll et al., 2004).
Concussion (or non-complex mTBI), in particular sport-related concussion (SRC), has been defined as a traumatic brain injury (TBI) caused by a direct blow to the head, neck, or body resulting in an impulsive force transmitted to the brain (Patricios et al., 2023a). Symptoms and signs of concussion may present immediately or evolve over hours (Herring et al., 2021), and no abnormality is described on routinely available neuroimaging (Patricios et al., 2023a).
Globally, an estimated 50–60 million TBIs are reported annually (Maas et al., 2022). Of these, 74%–90% are classified as mild (GCS 13–15), corresponding to 45–54 million mTBIs. Rates of mTBI vary widely (James, 2019) with the Canadian annual incidence reported as 1153 per 100,000 (Langer et al., 2020) and New Zealand as 771 per 100,000 (Feigin et al., 2013) person-years. These variations likely reflect inconsistencies in classification and coding.
In Australia, hospitals code diagnoses using the International Classification of Diseases, Tenth Revision, Australian Modification (ICD-10-AM) (Independent Health and Aged Care Pricing Authority, n.d.; Thomas et al., 2024). The four-digit S06.0~ concussion code includes the five-digit codes S06.00-S06.05; however, S06.03-S06.05 codes require an LOC of >30 minutes, which, by definition, should exclude patients with mTBI (Thomas et al., 2024). The previously utilised ICD-9 codes have shown the inaccuracies of using ICD coding for mTBI case ascertainment (Bazarian et al., 2006), and coding inaccuracies have been reported in relation to mTBI (Poloai et al., 2023). Therefore, clarification is required regarding which ICD-10-AM codes accurately represent a clinical diagnosis of mTBI in Australian hospitals. Given that ICD-10-AM concussion codes include LOC durations inconsistent with mTBI, published statistical data may be biased by coding protocols rather than reflecting true epidemiology. This challenge is further complicated by inconsistent terminology (e.g. mTBI; concussion; non-complex or uncomplicated mTBI; SRC; complex mTBI) associated with such injuries.
Current study
Before the epidemiology of all-cause mTBI can be established in Western Australia (WA), it is necessary to first identify which ICD-10-AM concussion codes reliably represent mTBI presentations in the ED setting. Five-digit codes are preferred for reporting episodes of care, as they provide more specific and detailed diagnoses (Australian Institute of Health and Welfare [AIHW], n.d.). Consistent with the Lancet Neurology Commission’s recommendation “to increase public health interest and establish a research focus on mTBI” (Maas et al., 2022), the study aimed to identify which ICD-10-AM S06.0~ codes are most indicative of a clinical diagnosis of mTBI. The objective was to identify the positive predictive value (PPV) of ICD-10-AM principal diagnosis concussive injury codes for mTBI using information from the emergency department information system (EDIS) from a Western Australian ED and retrospective chart review. We hypothesised that the five-digit ICD-10-AM codes S06.00–S06.02 are consistent with a clinical diagnosis of mTBI, while codes S06.03–S06.05 reflect alternative intracranial injuries.
Method
A retrospective chart review was performed on patient medical records corresponding to episodes of care coded with S06.0~ ICD-10-AM concussion codes. Ethical approval was received from Royal Perth Hospital (RPH) Human Research Ethics Committee (HREC) (RGS0000006733: 15 May 2024) including a waiver of consent, with East Metropolitan Health Service Governance Authorisation (RGS0000006733: 22 July 2024), and reciprocal HREC approval from Curtin University (HRE2024-0263: 29 May 2024).
Source of records
Records were sourced from a 450-bed adult hospital (RPH), which receives more than 84,000 ED presentations each year. EDIS was used to identify episodes of care with principal diagnosis codes S06.0~. From EDIS records, key patient and clinical information, including admission time, mode of arrival, treating clinician, outcome, discharge status, and departure date, was collected. Principal diagnosis is coded by the treating clinician prior to patient discharge for each presentation. Medical records corresponding with the relevant episode of care were requested from the RPH Health Information Management Services.
Identification of eligible episodes of care
All episodes of care between 1 July 2022 and 30 June 2023 coded with an S06.0~ code, in patients aged 14 years or older, were eligible for inclusion in the study. Episodes of care with an alternative principal diagnosis code and patients less than 14 years of age (due to the patient demographic seen at RPH) were excluded. Unavailable medical records were also excluded.
Data collection
Based on previous literature (Pozzato et al., 2017, 2020) estimating that mTBI accounts for 1.7% of ED presentations in Australia, an annual volume of ~1400 mTBI presentations to RPH was estimated. To estimate the PPV of ED mTBI coding with 95% confidence intervals (CIs) of ±5%, a conservative expected PPV of 50% was used, requiring 384 cases. However, 578 records for S06.0~ coded episodes of care were identified for the study period, and it was deemed feasible to analyse all records not used for piloting extraction and training. This allowed for 95% CIs of ±4.2%, and 10% subgroup PPV estimation with ±13.3% precision for secondary analysis.
Data from EDIS and the medical records were collected and managed using a data abstraction form ( Supplemental 1, online Supplemental ) developed in REDCap (Harris et al., 2009, 2019) to optimise consistency. Variables included date and time of ED presentation, age of patient, Australasian Triage Scale (ATS) score, arrival mode, documented presenting complaint, GCS at triage, evidence of PTA, recorded LOC, documentation of substance use, mode and mechanism of injury (Andelic et al., 2008; Maas et al., 2022; Silverberg et al., 2023; Voormolen et al., 2018) ( Table S1, online Supplemental ), presenting symptoms and signs (Davis et al., 2023a, 2023b; Echemendia et al., 2023; Patricios et al., 2023b) ( Figure S1, online Supplemental ), clinical assessment tool utilisation, neuroimaging result (if requested), and any documentation of a clinician’s diagnosis. Participant data were coded in a manner that prevented the identification of subjects.
We classified S06.0~ coded episodes of care as either mTBI “cases,” “non-cases,” or, if clinical diagnosis was unclear from the medical records, “unsure.” Mild TBI “cases” were defined as: a documented diagnosis of “Concussion” or “mTBI” by a clinician, or a biomechanically plausible mechanism of concussion injury with symptoms and/or signs consistent with concussion, or mTBI as defined by the American Congress of Rehabilitative Medicine (ACRM) ( Supplemental 2, online Supplemental ). Where multiple criteria were present, a documented clinician diagnosis was prioritised. “Non-cases” were defined as GCS <13 AND/OR LOC >30 minutes AND/OR PTA >24 hours, or an alternative documented intracranial diagnosis by a medical doctor or identified on neuroimaging.
Data abstraction was performed by three abstractors: (1) Medical Doctor and PhD candidate; (2) Occupational Therapy student and research group member with lived experience; and (3) Medical Doctor and PhD Supervisor. Abstractors were blinded to the S06.0~ code recorded in EDIS for each case during review. A trial of data abstraction was conducted by Abstractor 1 to confirm that the abstraction tool was fit for purpose, followed by training and cross-validation of six records with Abstractor 2, with the aim of mitigating errors and omissions identified within the medical records. This process guided completion of the abstraction procedures manual and accompanying flowchart ( Supplemental 3, online Supplemental ) for use by all abstractors.
Inter-rater reliability between Abstractors 1 and 2 was assessed using observed agreement of 25 randomly selected records and Cohen’s kappa (minimum acceptable k = 0.6; Vassar and Holzmann, 2013). Abstractor 1 reviewed all records; Abstractor 2 independently reviewed ⩾20% for reliability (n = 114); Abstractor 3 adjudicated unresolved cases. Final kappa was recalculated at study completion.
Independent variables
Independent variables included age (young adult [14–25 years]), adult [25–65 years], older adult [>65 years]), sex (male, female), mode of arrival (private transport, ambulance, helicopter, police, Royal Flying Doctor Service [RFDS]), arrival time (day, night), injury acuity (ATS 1–5), GCS at ED triage (13–15, 9–12, 3–8), whether substance use was documented (yes, no), injury mode (fall, traffic incident, inflicted injury [assault or deliberate self-harm], sport, other accident, unknown mechanism), injury mechanism (direct blow to head, head striking object, force transmitted from body, other unknown/unwitnessed), and patient disposition (admitted or discharged from ED). Reclassification was performed to increase the effective sample size. Age was grouped into two categories <65 years or >65 years. The arrival modes of ambulance, police, helicopter, and RFDS were combined as emergency services. ATS 1 and 2 became high acuity, ATS 3 moderate, and ATS 4–5 lower acuity. GCS on arrival was dichotomised into GCS <13 and GCS 13–15, and both injury mode and injury mechanism were categorised as known and unknown.
Outcomes
True positive cases of mTBI were defined as episodes of care with an S06.0~ code, which had been identified in medical record review as having a clinical diagnosis of mTBI (“case”). False positive cases were combined with those where a clinical diagnosis was unable to be confirmed from record review (“non-case” and “unsure”). Unadjusted and adjusted PPVs of the combined S06.0~ concussion codes, individual codes, and codes grouped by LOC were calculated for mTBI (95% CIs) (Paget et al., 2022; Warwick et al., 2020).
Statistical analysis
Analysis was performed in Rstudio v.4.3.3 (RStudio Team, 2025). Descriptive statistics were performed to describe the distribution of patient and episode characteristics using frequency and percentage (calculated among all episodes unless stated otherwise). Unadjusted PPVs were calculated with 95% CIs estimated using the Wilson score method to improve accuracy. Univariate assessment of true positive (TP) and total counts by independent variables was conducted using contingency tables and Chi-squared test. Adjusted PPVs were calculated using logistic regression models fitted with the “glm() function,” specifying a binomial family and logit link. Bias-reduced logistic regression (Firth, 1993) was applied for small cell sizes. The emmeans package, which allows for calculation of marginal means across the levels of independent variables, was used when estimating adjusted PPVs.
Results
A total of 578 episodes of care were recorded with an EDIS principal diagnosis code of S06.0~ over the data collection period. Medical records for 11 episodes were used in the development of the data abstraction tool and abstractor training, with 25 then used for pilot abstraction (Abstractor 1 and 2). After these 25 reviews, inter-abstractor observed agreement was 100.0% (k = 1). A total of 542 records remained available for inclusion in the study; 2 were excluded as they were unavailable (N = 540). At the end of the study, inter-abstractor observed agreement was 88.6% (k = 0.78).
The mean patient age was 40.1 years (standard deviation = 19.0, range 14–94 years). In addition to GCS 13–15 (n = 492, 91.1%), other clinical information abstracted to assist in identification of mTBI cases included documentation of LOC (n = 218, 40.4%) and time frames of this (unspecified n = 63, 11.7%; <30 minutes n = 137, 25.4%), and documentation of the presence of PTA <24 hours (n = 62, 11.5%). Computed tomography (CT) brain was performed in 365 (67.6%) episodes of care, of which 260 demonstrated an absence of trauma-related intracranial abnormalities, or “normal” results. Only nine episodes resulted in magnetic resonance imaging brain (1.5%), with one returning a “normal” result. Formal head injury assessment tools were used in 111 (20.6%) episodes of care. ED clinicians documented any diagnosis in the medical record 71.9% of the time (n = 388), which included a diagnosis of concussion for 176 episodes of care (32.6%) and mTBI for 1 episode (0.2%). Of those with a documented mode of injury, the most common was falls (n = 162, 30.0%). Of those where mechanism of injury was documented (n = 423, 78.3%), the majority had sustained an impact to the head (n = 394, 73.0%) rather than a transmitted force from the body (n = 29, 5.4%).
S06.00 (Concussion) was the most used S06.0~ code (n = 279, 51.7%). No episodes of care were coded with S06.04 or S06.05 (LOC > 24 hours). Despite five-digit-coding being preferred, 10.6% of episodes were coded with the four-digit-code S06.0 (Concussive Injury, n = 57). Other demographic and clinical characteristics of the cohort are presented in Table 1.
Demographic, injury-related, and clinical characteristics utilised as independent variables, and their crude associations with TP assessment for mTBI.
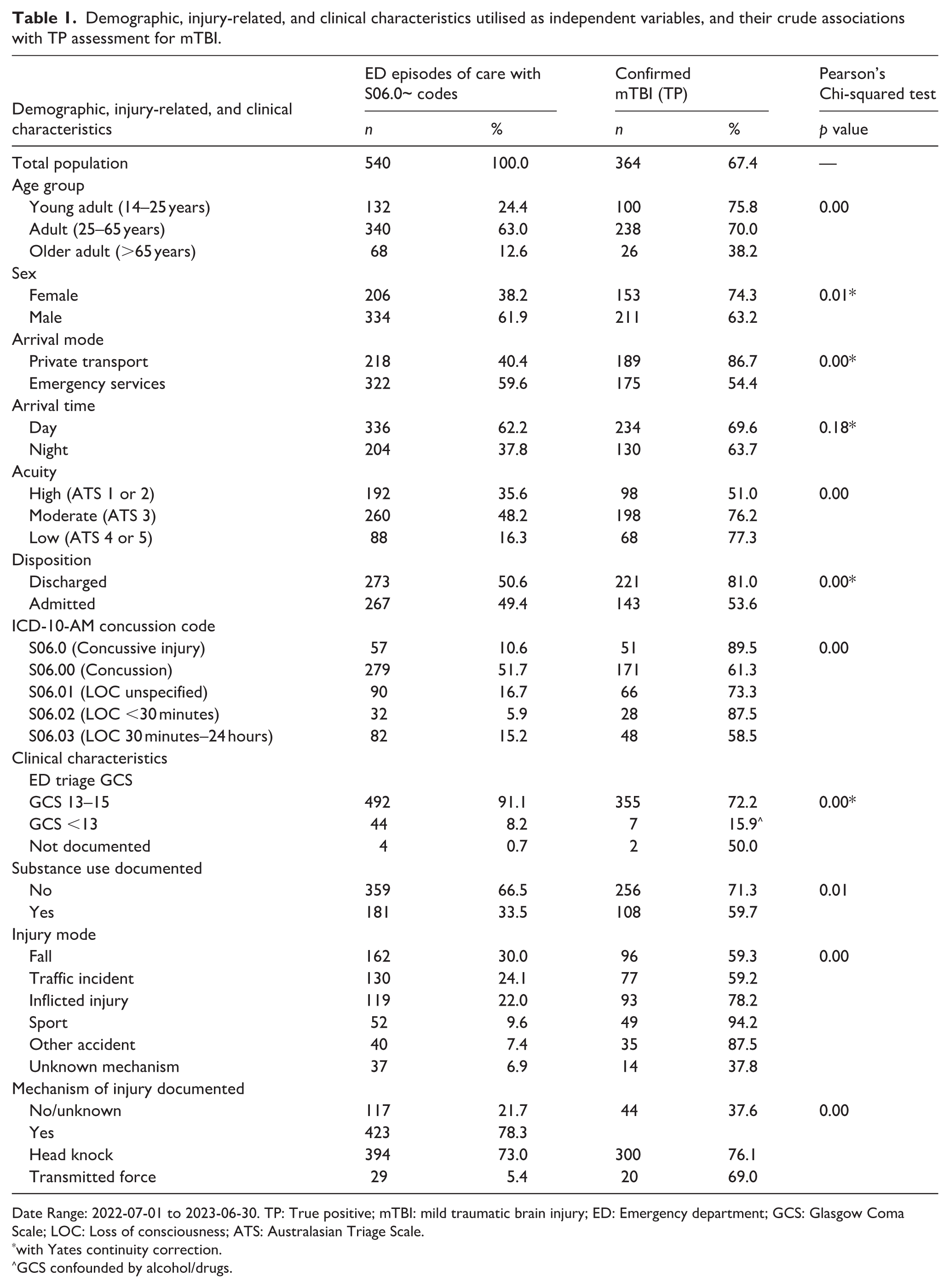
Date Range: 2022-07-01 to 2023-06-30. TP: True positive; mTBI: mild traumatic brain injury; ED: Emergency department; GCS: Glasgow Coma Scale; LOC: Loss of consciousness; ATS: Australasian Triage Scale.
with Yates continuity correction.
GCS confounded by alcohol/drugs.
After adjusting for independent variables, of the 540 episodes with S06.0~ codes, 71.8% (95% CI 66.85–76.22) had evidence of mTBI based on medical record review. The concussion code with the highest PPV was S06.0 (the four-digit code for Concussive Injury). Only 64.5% of the most frequently used code, S06.00, had mTBI on medical chart review (95% CI 57.44–70.89). The PPVs for other individual codes and combined S06.0~ codes where LOC < 30 minutes are shown in Table 2. Of episodes coded S06.0~, those arriving at ED by private transport, those under 65 years of age, those with GCS 13–15, those where injury mode was reported (and sport specifically as a mode of injury), and those where mechanism of injury was documented were less likely to be misclassified for mTBI. Those coded S06.0~ who were triaged on arrival as high acuity were more likely to be misclassified as mTBI (Table 3).
Positive predictive values of ICD-10-AM S06.0~ concussion codes for mTBI.
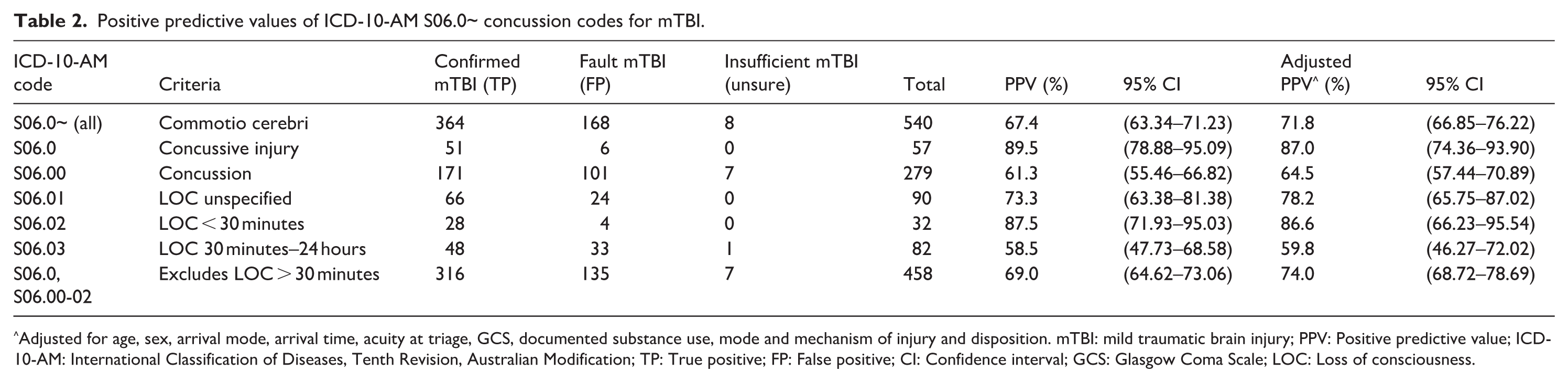
Adjusted for age, sex, arrival mode, arrival time, acuity at triage, GCS, documented substance use, mode and mechanism of injury and disposition. mTBI: mild traumatic brain injury; PPV: Positive predictive value; ICD-10-AM: International Classification of Diseases, Tenth Revision, Australian Modification; TP: True positive; FP: False positive; CI: Confidence interval; GCS: Glasgow Coma Scale; LOC: Loss of consciousness.
Positive predictive value of code S06.0~ with distribution by clinical characteristics.
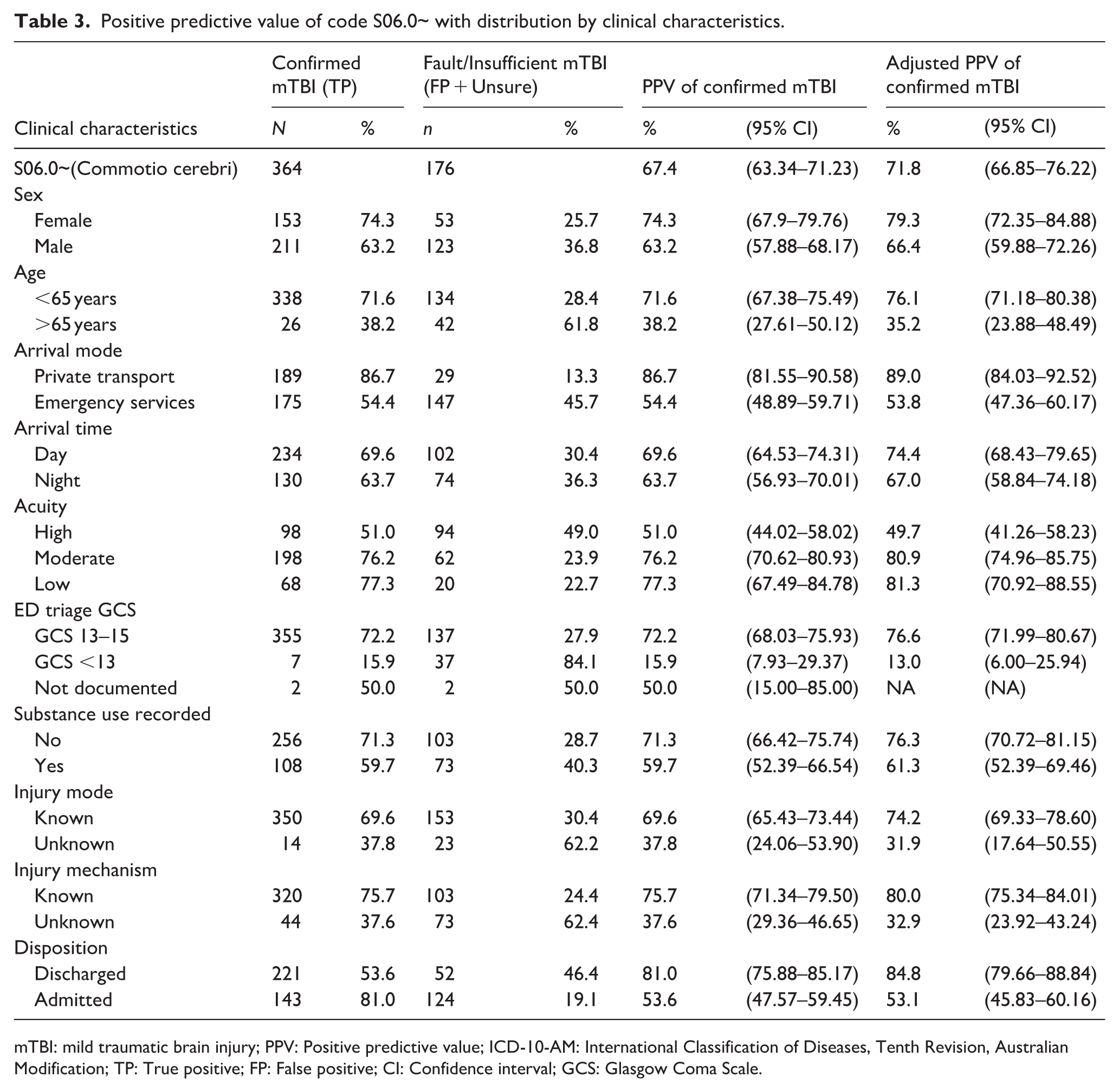
mTBI: mild traumatic brain injury; PPV: Positive predictive value; ICD-10-AM: International Classification of Diseases, Tenth Revision, Australian Modification; TP: True positive; FP: False positive; CI: Confidence interval; GCS: Glasgow Coma Scale.
Further analysis was performed excluding the S06.03 code (LOC > 30 minutes but <24 hours), which is inconsistent with clinical definitions of mTBI. This exclusion did not change which independent variables showed statistical significance ( Table S2 , online Supplemental ).
When independent variables were held constant, the adjusted PPV for S06.0~ was 71.8% (95% CI 66.85–76.22). For combined S06.0 and S06.00–S06.02 codes (excluding LOC >30 minutes), PPV was 74.0% (95% CI 68.72–78.69), for combined S06.0 and S06.00 codes (Concussive Injury and Concussion) 70.4% (95% CI 64.19–76.01), and for combined S06.01 and S06.02 codes (brief LOC or LOC <30 minutes) 86.1% (95% CI 75.50–92.51). The adjusted PPV for S06.03 (LOC >30 minutes to 24 hours) was suboptimal (59.8%, 95% CI 46.27–72.02) (Table S3, online Supplemental).
Discussion
This study provides insight into how ICD-10-AM S06.0~ principal diagnosis coding influences mTBI reporting in ED data. Approximately 206,000 mTBI cases occur annually in Australia (extrapolated (Feigin et al., 2013)). However, literature suggests that all S06.0~ concussion codes are typically included when identifying mTBI episodes (AIWH, 2021, 2024; Fouquet et al., 2024; Langer et al., 2020; Thomas et al., 2024) despite some codes having LOC time frames beyond clinical definitions of mTBI. This research clarifies how S06.0~ codes in ED predict a clinical diagnosis of mTBI and highlights implications for accurate reporting.
In Australia, coding practices differ between inpatient and ED settings. Inpatient hospital coding is performed by qualified and trained clinical coders, allocating both principal and additional codes. In contrast, ED presentations are coded in EDIS using only a principal diagnosis, defined as “the diagnosis established at the conclusion of the emergency care episode that is mainly responsible for occasioning the attendance, following consideration of clinical assessment” (Independent Aged Care Pricing Authority, n.d.). The coding decision is made by the treating clinician prior to patient disposition, with the patient remaining recorded as present in the department until this has been finalised. Clinician coding requires the clinician to understand ICD-10-AM codes and coding requirements and appropriately code the episode of care. Similarity between codes (e.g. S06.0 Concussive Injury and S06.00 Concussion) and a busy ED environment increases the risk of suboptimal coding. If the treating clinician who has the best knowledge of the patient history is unable to perform the task due to shift changes or clinical demands on time taking precedence, this may result in a proxy with limited knowledge of the relevant patient completing the coding.
Under-reporting of concussion in ED settings has been documented (Pozzato et al., 2020), which can be attributed in part to the limitation of only recording the principal diagnosis code in what may be complex presentations, and inaccuracies in coding (McKenzie et al., 2009; Wharton et al., 2025). Given these limitations of the current ICD-10-AM coding system in ED, this study provides valuable information regarding the PPVs for S06.0~ concussion coding for mTBI.
While the predictive ability of ICD-10 codes to capture true TBI cases has been previously reported (Warwick et al., 2020), to the authors’ knowledge, this is the first study to assess the ability of S06.0~ codes to capture true mTBI cases in Australia. Adjusted PPVs for S06.0~ concussive injury codes ranged from 59.2% to 87.0% for mTBI, consistent with PPVs for external injury codes (58.0%–96.5% (Paleczny et al., 2024)) but higher than the PPV for concussion in ICD-9 coding previously reported (Bazarian et al., 2006). Grouping concussion codes to reflect the clinical descriptions of LOC associated with mTBI (i.e. excluding codes reflecting a LOC >30 minutes) did not significantly change PPVs. When codes were grouped into “concussion” (S06.0 and S06.00), “brief LOC” (S06.01 and S06.02), and “LOC > 30 minutes” (S06.03), the adjusted PPV for concussion code S06.03 was 59.8%, which is suboptimal compared to thresholds considered acceptable for epidemiological studies using administrative data (Tonelli et al., 2015). Given the requirement for an LOC between 30 minutes and 24 hours, S06.03 should theoretically never represent mTBI; its observed PPV > 0 reflects misclassification within ED coding. Excluding this code improves conceptual validity but may reduce sensitivity in real-world datasets.
Unexpectedly, the four-digit S06.0 “Concussive Injury” code had a higher PPV than the five-digit S06.00 “Concussion” (Table S4, online Supplemental) for mTBI. This may reflect that despite five-digit codes being preferred in coding, the process of choosing the best code descriptor from an electronic system may result in some clinicians choosing the first appropriate, rather than the most appropriate diagnostic code they identify. It is also possible that clinicians perceive the term “Concussive Injury” as a more accurate clinical descriptor for mTBI, whereas “Concussion” may be viewed as a less precise lay term potentially explaining its lower PPV. Across groups without documented LOC, with LOC of unspecified time (assumed to be brief for the analysis), and LOC < 30 minutes, misclassification also occurred. Therefore, over-reporting should also be considered in these groups when using ED data to identify mTBI.
S06.0~ codes were less predictive for mTBI among certain characteristics. These included being over 65 years of age, arriving by emergency service vehicle, having higher acuity at triage (ATS 1 or 2), GCS less than 13 at triage, being admitted to hospital, and those without documentation of mode or mechanism of injury in the medical records. These findings may reflect several factors. These include clinician training, where a clinical diagnosis of mTBI is not considered despite symptoms and signs being identified, and clinician coding choices where, although considered as a diagnosis, it is not deemed the principal diagnosis (such as in complex cases or cases with confounding factors). Additionally, a lack of clarity in medical documentation, where there is an absence of documentation of negative findings and missed information, may lead to inaccurate coding by a proxy.
Limitations
Medical record review has been described as clumsy and imprecise, and in the absence of documentation reflecting comprehensive clinical assessment or a documented clinical diagnosis, classification was uncertain in some instances. In addition, the possibility of inaccurate or insufficient documentation, for example, when a scribe was utilised during assessment or when medical notes were written in retrospect, requires consideration. Despite this, written records have prima facie value. This study was conducted in the ED of a major trauma centre, and findings may not be directly generalisable to other ED settings. However, the increasing complexity of presentations across EDs suggests that similar patterns may be observed more broadly.
The absence of S06.04 and S06.05 codes in the EDIS data is not unexpected, as both codes represent LOC > 24 hours. National Emergency Access Targets, which aim for most patients to be admitted, discharged or transferred within 4 hours, further limit the likelihood of these codes being recorded in the ED setting. Similarly, signs and symptoms of mTBI may evolve over time, but information captured by, and the principal diagnosis recorded in, EDIS reflects only the time spent in ED. While the entire episode of care for an S06.0~ principal diagnosis coded in EDIS was reviewed in the associated medical record to improve diagnostic clarification, this documentation may contain more information than was available at the time of original EDIS coding. Also, among patients discharged directly from the ED with S06.0~ codes, some may have experienced ongoing symptoms or evolving signs (e.g. PTA > 24 hours) that would ultimately have been better coded with an alternative code.
Given that the abstractors were part of the research team, the inherent risk of abstractor bias was mitigated through the development of an explicit protocol, a pilot phase, standardised abstraction tools, and training. Abstractors were also blinded to S06.0~ coding, and inter-abstractor agreement was monitored. If a better alternative diagnosis was identified, episodes were classified as “non-cases”; as such, episodes of care that fulfilled the ACRM criteria for complex mTBI but with CT findings that provided a more specific diagnosis, for example, cerebral contusion, were excluded from mTBI “cases” ( Figure S2, online Supplemental ). Finally, combining “unsure” with non-cases biased PPV estimates downward ( Table S5, online Supplemental ); however, this conservative approach was chosen to avoid overestimation in administrative data validation.
Recommendations
When using ED S06.0~ principal diagnosis codes to identify mTBI cases in ED, consideration should be given to the impact of misclassification. Researchers may improve accuracy by stratifying results by clinical characteristics, for example, reporting separately for patients 14–65 years versus those >65 years, or distinguishing those arriving by private transport and emergency service vehicles. Further research identifying the predictive value of S06.0~ codes in inpatient settings will assist in better understanding how concussion coding predicts mTBI in the inpatient setting and provide insight into ED-coded S06.0~ episodes that result in admission.
In the absence of a national TBI registry that captures mTBI, and pending the identification of a definitive biomarker panel for concussion, ICD-10-AM coding will remain the most accessible way to establish mTBI epidemiology in Australia. It is recommended that the responsibility of clinical coding in ED is removed from time-poor clinicians who do, and must, prioritise clinical care, and are inadequately trained in clinical coding. Instead, artificial intelligence (AI) tools, trained and validated by qualified clinical coders, could be developed to assign objective and appropriate codes. The increasing use of electronic medical records presents an opportunity to improve the documentation of mTBI presentations. By utilising prompts and preloaded concussion assessment tools to capture both positive and negative clinical findings, the information available for coding can be significantly increased. Additionally, machine-learning-based natural language processing approaches (McNamara et al., 2026) can extract free text from health data to help identify mTBI-related ED presentations. This is particularly useful for surveillance when mTBI is not the principal diagnosis, as it reduces reliance on standard ICD-10-AM coding for epidemiological research.
Conclusion
These findings demonstrate the limitations of using ICD-10-AM concussion codes for identifying mTBI in ED settings, revealing patient characteristics that influence coding accuracy within administrative data. To improve the positive predictive capacity of S06.0~ codes for mTBI, coding responsibility should be removed from frontline ED clinicians. Leveraging electronic medical records and developing AI-driven coding systems guided by expert clinical coders offers a practical pathway to improve the reliability of administrative data for mTBI surveillance.
Supplemental Material
sj-docx-1-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-1-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-10-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-10-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-2-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-2-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-3-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-3-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-4-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-4-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-5-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-5-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-6-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-6-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-7-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-7-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-8-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-8-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Supplemental Material
sj-docx-9-him-10.1177_18333583261447482 – Supplemental material for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury
Supplemental material, sj-docx-9-him-10.1177_18333583261447482 for The positive predictive value of ICD-10-AM S06.0~ concussion codes for mild traumatic brain injury by Gill Cowen, Thomas Bergin, Samantha Carey, Elizabeth Thomas, Ninh Ha, Sharmani Barnard, Daniel Fatovich, Melinda Fitzgerald and Delia Hendrie in Health Information Management Journal
Footnotes
Acknowledgements
Mrs Sophie Damianopoulos, Royal Perth Hospital Emergency Department, for medical record recall coordination and access. Ms Sharon Linton, Area Manager Clinical Coding, East Metropolitan Health Service, for information and advice regarding hospital coding practices.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Curtin Medical School Seed Funding Grant. The primary author (GC) is also the recipient of financial support through the Australian Government Research Training Program (RTP) scholarship via Curtin University. Publication was funded through Curtin University’s Open Access Publishing Agreement with SAGE.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof M Fitzgerald is CEO for Connectivity TBI Australia, Dr G Cowen is a member of Connectivity TBI Australia and has provided paid consultancy work to this organisation. She is also a Founding Member of the Western Australian Concussion Network (WACN).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.