
Abstract
Background:
This study extended prior research on employment outcomes of the 2012–2016 and 2017–2021 health information manager (HIM) graduate cohorts from La Trobe University, Australia.
Objectives:
(1) To classify graduates’ early-career pathways, applying two classificatory methodologies, employing (a) position title (methodology 1), (b) self-reported knowledge and skills-based duties (methodology 2); (2) To compare outcomes of the methodologies; (3) To examine graduates’ duties within the profession’s established knowledge-skills domains and inform understanding of HIMs’ roles.
Method:
Residual data from prior cross-sectional studies were applied to early-career graduate HIM positions, using the two classificatory methodologies.
Results:
Methodology 1 showed a greater proportion of roles under the “Health Information Management” domain. Methodology 2 revealed more roles aligned with the “Health Information Systems” and “Data Management and Analytics” domains. A longitudinal increase in health systems implementation, system documentation development, database management, and IT system support and maintenance characterised increasing “technologisation” of HIM roles (“Health Information Systems” domain). Clinical coding of admitted episodes (“Health Classification” domain) was the most frequently reported skill utilised in HIMs’ first post-graduation position, offset by a slight, longitudinal decrease in clinical coding engagement. The 2017–2021 cohorts progressively reduced involvement in clinical coding roles, instead utilising more skills in the “Health Information Systems” and “Data Management and Analytics” domains. Methodology 1 showed a cohort 1 to cohort 2 increase in graduates assigned to the “Data Management and Analytics” domain (10.2–16.6%); Methodology 2 showed a simultaneous decrease (22.0–15.1%), arguably influenced by artefactual differences. The apparent decline in the “Data Management and Analytics” domain should be viewed cautiously owing to HIMs’ increasingly data-driven work.
Conclusion:
Reliance on job title may oversimplify or misrepresent the scope of HIMs’ duties. Choice of classificatory methodology significantly impacts upon the domain to which HIMs’ roles are categorised. The findings support a skill- and duty-based methodology for accurate capture of evolving HIM roles.
Implications for health information management practice:
This research provides valuable insights into HIM workforce trends, and foundations for (a) longitudinal career pathway and skills mapping and (b) a visual tool (career map) to support the profession’s visibility, promotion, and development of illustrative career trajectories.
Keywords
Introduction
Recent changes within the global healthcare sector include the introduction of patient-centric models of care, more sophisticated electronic health records (EHRs), increasing technogovernance requirements surrounding health information, and technologies for artificial intelligence (AI) and big data (Hoeyer, 2023; Houser et al., 2025a; Hoyle, 2017; Martin and Sinsky, 2016; Price and Cohen, 2019; Robinson and Lee, 2021). The healthcare system’s reliance on health data and information and, consequently, on the specialist expertise of health information managers (HIMs), is integral to much of this change. Notwithstanding this centrality, much of the work of HIMs is undertaken “behind-the-scenes” and is invisible to patients and the public (Robinson et al., 2025). There exists a perceived challenge in explicating the role of the HIM (Al Kiyumi et al., 2016; Nexhip et al., 2024); it has been suggested that this has contributed to worldwide shortages of qualified HIMs as limited public understanding of HIM job titles, functions and career pathways inhibits promotion of the profession, particularly to school leavers (Al Kiyumi et al., 2016).
Classificatory disparity between occupational classification frameworks impedes the capture, internationally and domestically, of the profession’s actual capacity and scope. For instance, the World Health Organization (WHO, 2019: 8) omits HIMs from its global classification of health workers and, instead, narrowly frames all health information workers within technician roles as Medical Records and Health Information Technicians. Within Australia, Health Workforce Australia (HWA, 2013) observed some years ago that, while the health information workforce was dispersed across the healthcare system, there was some perceived blurring of professional boundaries. The complexity of HIMs’ positioning in Australia is exemplified in the Australian Bureau of Statistics’ (ABS, 2024) Occupation Standard Classification. This categorises HIMs as Information and Organisation Professionals within the broader Business Professionals group, emphasising their expertise in health information governance, documentation practices, clinical coding, and data analysis for statistical and research purposes.
In North America, the Canadian Health Information Management Association (CHIMA, 2014) and the American Health Information Management Association (AHIMA, 2016) have developed career mapping tools using methodologies based on job advertisements or specialised focus groups (Gibson et al., 2015; Madlock-Brown et al., 2021). Similar methodological approaches have highlighted trends in the HIM workforce in the United States of America (USA) and elsewhere (Fenton et al., 2022; Marc et al., 2019), and a small body of literature has reported research, using various methodological approaches, on HIMs’ professional career circumstances or pathways in several countries (Beesley et al., 2020; Burns et al., 2025; Gibson et al., 2015; Gjorgioski et al., 2023; Lee et al., 2024; Riley et al., 2020; Robinson et al., 2025).
Riley et al. (2020) surveyed early-career HIM graduates in Australia and found “very high employability and demonstrate[d] job mobility consistent with the national trends” (p. 93). Building on the evidence-based work of Robinson et al. (2025) involving an Australia-wide cohort of HIMs drawn from across the healthcare sector, Riley et al. (2020) and Gjorgioski et al. (2023) categorised graduate positions – using HIM-respondents’ self-reported position titles – into four key “knowledge-skills domains” (hereinafter, “domain[s]”): health information management (including health information science), health classification (including clinical and finance-related knowledge), health data management and analytics, and health information systems (including information and communication technologies (ICTs)). These domains represent the specialised professional expertise of Australia’s HIMs. The domains provide a useful framework for examining employment outcomes. The approach adopted by Riley et al. (2020) and Gjorgioski et al. (2023) offered valuable insights into the employment destinations and sectoral locations of HIM graduates; however, reliance upon position title alone may not fully capture the depth or diversity of the skills and duties actually performed in these roles.
To better understand and communicate the diversity of HIM career pathways, it is useful to apply classification theory, which explicates the categorisation and definition of entities in social, technical and institutional systems. Bowker and Star (1999) observed that classification systems are never neutral; rather, they shape what is acknowledged and valued within professions and may inadvertently obscure roles that do not fit readily into domain categories. When applied in the case of HIMs, such obscurity can potentially contribute to role ambiguity and workforce underutilisation.
Aims
The current study was part of a wider program of research investigating the career trajectories of HIM graduates from La Trobe University (LTU), Australia. The LTU’s HIM curricula comprehensively address the aforementioned core domains, preparing graduates with appropriate skills for healthcare sector-wide employability in the health data and information arena. This component of the research has been derived from the prior work of Riley et al. (2020) and Gjorgioski et al. (2023) by applying a classification methodology that extended beyond using position title to infer the knowledge-skill domain of HIM graduate roles. This current study instead classified HIM-graduates’ roles according to self-reported knowledge, skills, and duties, the aims being to provide an accurate picture of HIMs’ early-career pathways and examine the alignment between job titles and work performed. There were three objectives:
To classify graduates’ early-career pathways using two distinct classification methodologies – one based on position titles and the other based on knowledge-skills domains derived from self-reported duties;
To compare the outcomes of these two classification methods; and
To examine the duties undertaken by graduates within each of the four knowledge-skills domains, in order to provide a better understanding of HIMs’ roles and responsibilities.
Method
Study design and sample
The methods underpinning this study have been described elsewhere (Gjorgioski et al., 2023; Riley et al., 2020). In summary, a cross-sectional study design was employed, involving two purposively selected samples of graduate HIM cohorts (2012–2016, 2017–2021) from LTU, Australia. The sample members had qualified with LTU’s profession-entry bachelor-master or double-bachelor degrees, or graduate-entry master degree, and were employed within Australia. All programs held external accreditation from the Health Information Management Association of Australia. Sample members were identified and located using LTU-owned databases and the research team’s professional networks, HIM-practitioner colleagues, and social media.
Data collection
As described by Gjorgioski et al. (2023) and Riley et al. (2020), quantitative and qualitative data were collected from participants using self-administered, online surveys. A forced response format elicited respondents’ demographic details, qualifications, employment type, titles of up to three positions held post-graduation, and the major duties performed in each role. Open-ended items sought information on career pathways and skills learned at university and on the job. In both studies, respondents self-identified the skills and knowledge applied in their current roles by selecting professional duties aligned with four previously established, core domains. Both surveys were published as Supplemental Material in Gjorgioski et al. (2023) and Riley et al. (2020), with the domains also described in these publications. The subset of duties associated with each domain corresponded to the typical scope of work performed within that area of practice; respondents could select all that applied to their role. While the core structure of the domains remained consistent, there were slight differences between the two studies in the specific skills and knowledge items available for selection in the survey. These changes were introduced to capture fully the tasks undertaken by HIM graduates, which had slightly evolved between cohort 1 (2012–2016) and cohort 2 (2017–2021); Box 1 shows the inter-survey, between-skills differences. This approach enabled the research team to identify alignment with and/or divergence between the skills and knowledge utilised by graduates and the roles implied by their position titles.
Skills and knowledge domains.
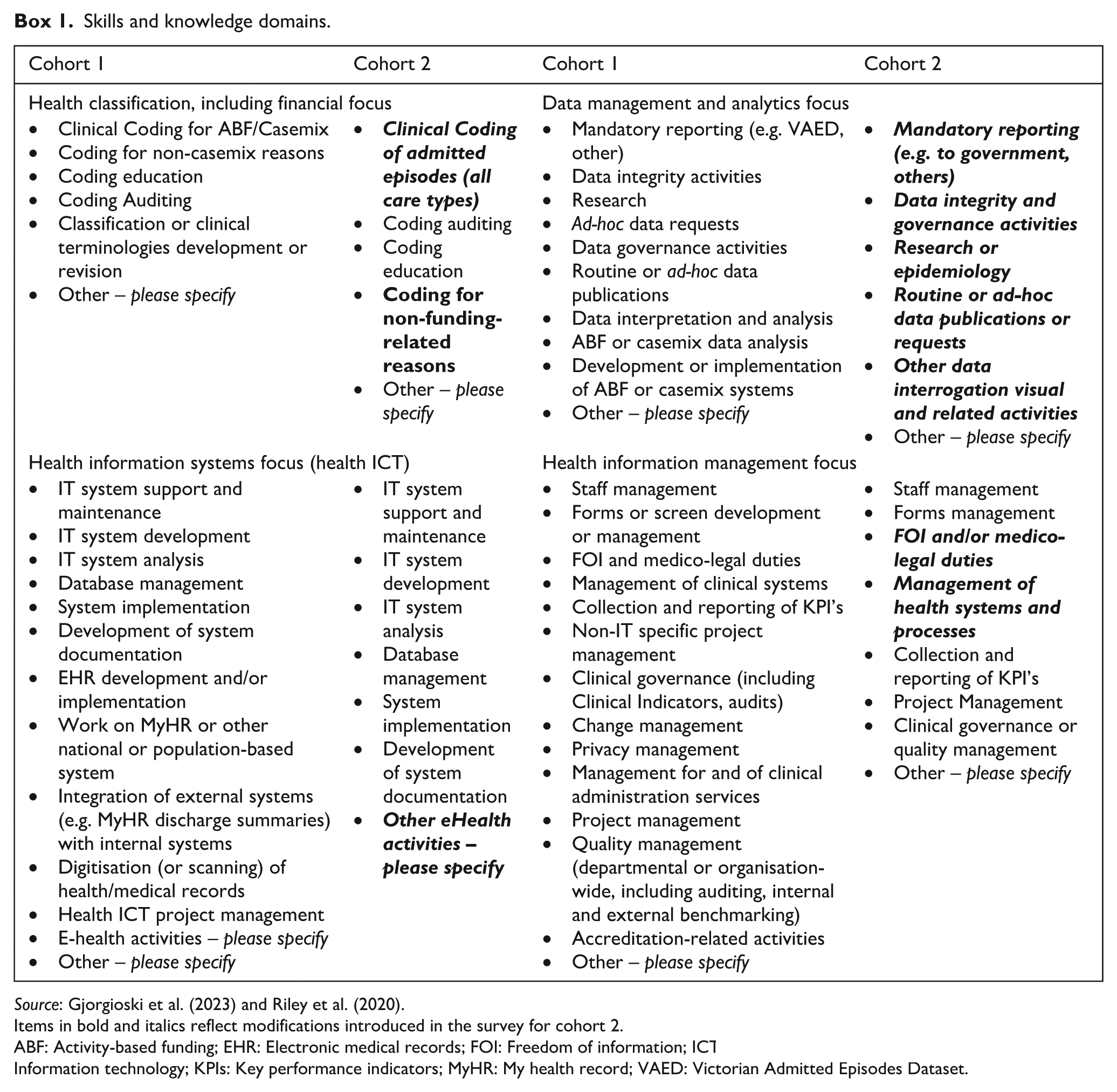
Source: Gjorgioski et al. (2023) and Riley et al. (2020).
Items in bold and italics reflect modifications introduced in the survey for cohort 2.
ABF: Activity-based funding; EHR: Electronic medical records; FOI: Freedom of information; ICT: Information and communication technologies; IT: Information technology; KPIs: Key performance indicators; MyHR: My health record; VAED: Victorian Admitted Episodes Dataset.
Classification methodology 1: Position title-based
In the current study, two distinct methodologies were used to classify early-career graduate HIM positions. The first, consistent with Gjorgioski et al. (2023) and Riley et al. (2020), relied upon the terminology of the position titles. In each of the previous studies, two researchers had independently reviewed each title and assigned it to one of the established domains. Following application of a hierarchical decision-making process, each position was classified into the domain most closely aligned to its primary function. Where the classification was unclear, titles lacked domain-specific indicators (e.g. “Academic,” “Project Officer”), or a title could reasonably fit into multiple domains, the position was allocated to a residual “Other” category to maintain consistency.
Classification methodology 2: Knowledge- and skill-based
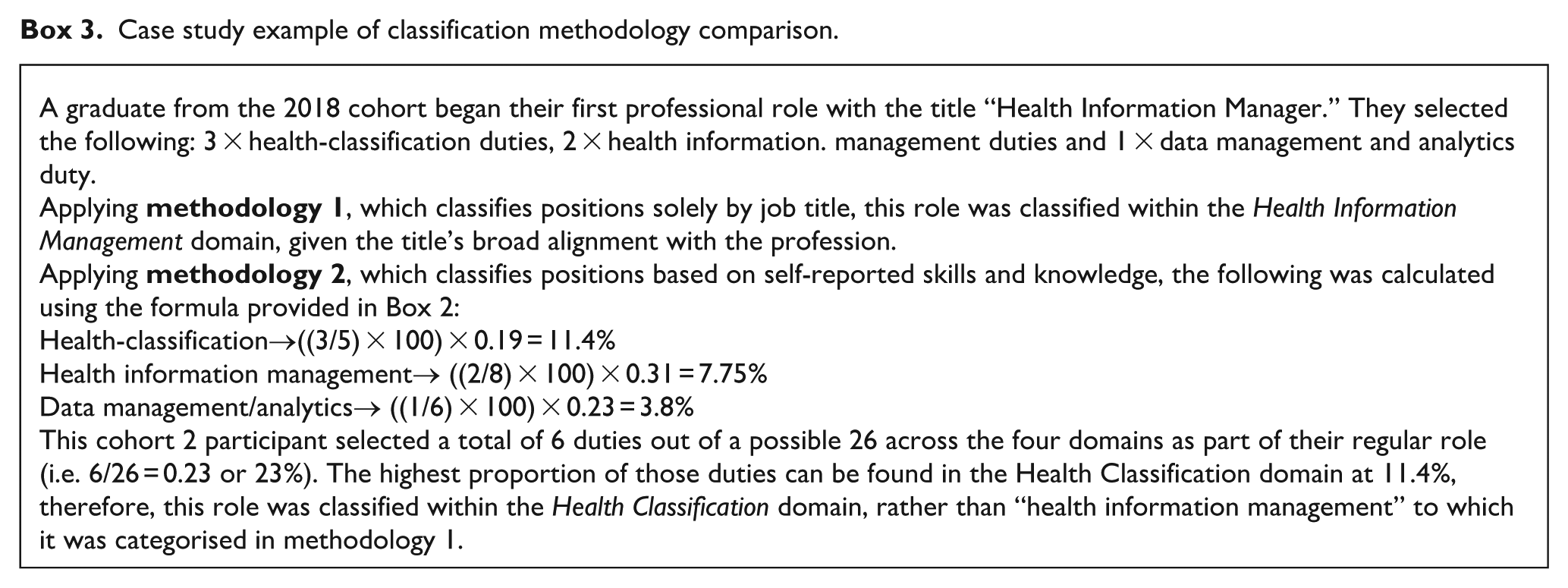
The second classification methodology focused on the knowledge and skills graduates reported using in their current roles, as opposed to position titles. Respondents identified the major duties they performed within each established domain (Box 2). Since the four domains varied in the number of selectable duties (e.g. participants could select from 5 duties under “health classification,” compared with 12 duties for “health information management”), a formula was developed to ensure equal, between-domain weighting and to prevent overrepresentation of domains with more listed duties. Where respondents’ duties were evenly distributed across multiple domains, or no clear dominant domain could be established, the position was classified into the “Other” category, consistent with the handling of ambiguous cases in methodology 1. Boxes 2 and 3 detail the weighting formula, and a case example illustrates the comparative applications of how the classification methodologies categorised the same graduate position.
Equal weighting formula.

Case study example of classification methodology comparison.
Data analysis
Categorisation of positions using methodology 2 was conducted independently using the re-weighting formula applied in Microsoft Excel (2025). All classifications were reviewed and verified independently by another member of the research team (AN) to ensure consistency and accuracy. Comparative analysis of the classification outcomes from methodologies 1 and 2 was also conducted in Microsoft Excel. Data on the skills and knowledge utilised by graduates from both cohorts were analysed using SPSS (Version 26; IBM Corp., 2024) predictive analytics software. Chi-square tests and p-values (α = 0.05) were undertaken using EpiInfo version 7.2 (Dean et al., 2011) and applied to identify any statistically significant differences (a) between the two classification methodologies and (b) in selected, inter-cohort outcomes.
Ethics approval
The LTU Human Research Ethics Committee (HREC22072) approved this research.
Results
Sample
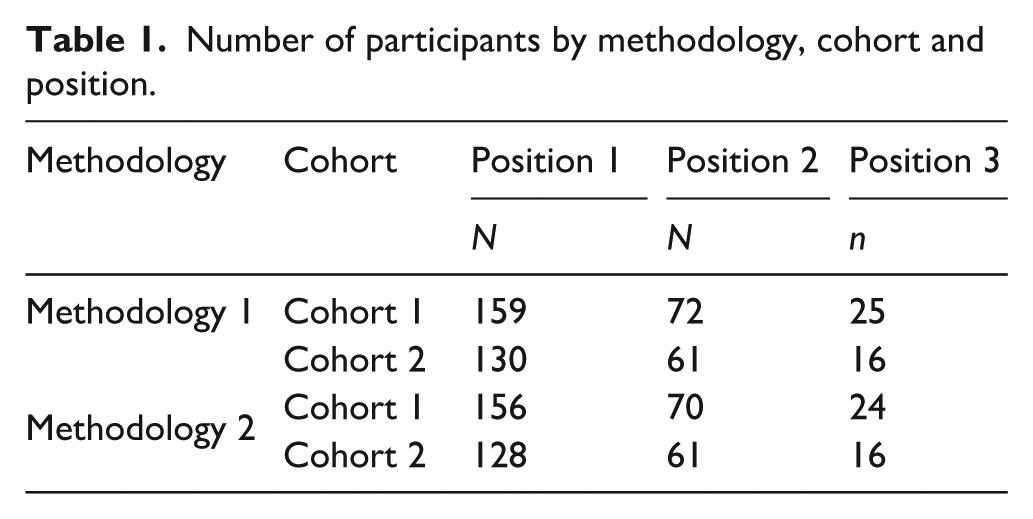
Under methodology 1, data were available for 159 participants in cohort 1 and 130 in cohort 2; methodology 2 included 156 and 128 participants, respectively (Table 1), reflecting minor differences in data completeness between the two approaches.
Number of participants by methodology, cohort and position.
Position title categorisation (methodology 1)
Under methodology 1, “Health Information Management” was the most frequently reported domain across both cohorts, comprising 44.1% of roles in cohort 1 and 40.0% in cohort 2 (χ² = 0.75, p = 0.35) (Figure 1). A statistically significant decline was observed in “Health Classification” roles between cohort 1 and cohort 2, decreasing from 28.1 to 14.9% (χ² = 11.5, p < 0.01). Conversely, “Health Information Systems” roles increased significantly between cohort 1 and cohort 2 from 6.3 to 17.4% (χ² = 14.13, p < 0.01). “Data Management and Analytics” showed a modest, statistically significant increase from 10.2 to 16.6% (χ²= 4.16, p = 0.04). Roles categorised as “Other” remained stable (11.3 and 11.1%, χ² = 0.037, p = 0.83).
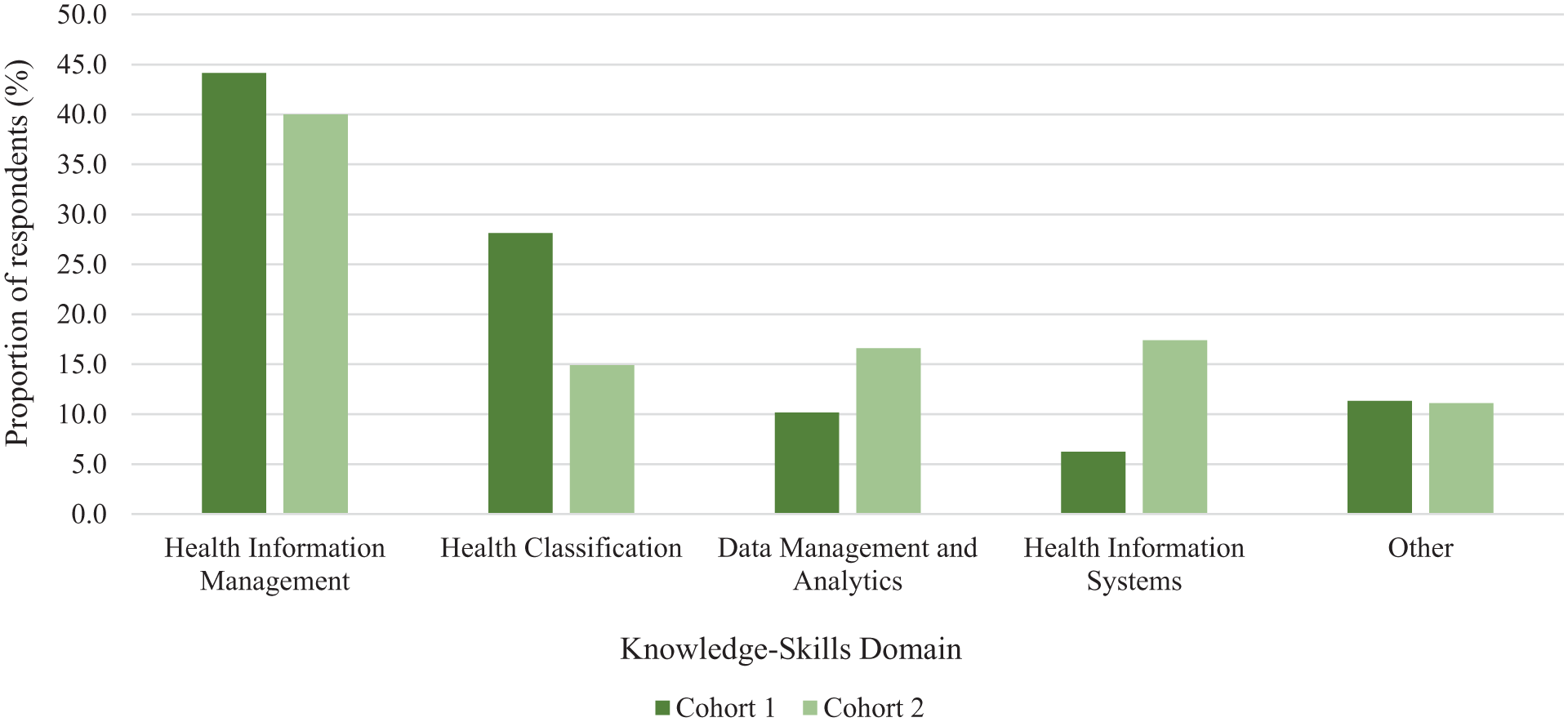
Classification of roles by position titles (all positions combined) by cohort, methodology 1.
Skills and knowledge categorisation (methodology 2)
When methodology 2 was applied, “Health Information Management” was again the most frequently reported knowledge-skills domain in both cohorts (35.2% in cohort 1; 32.2% in cohort 2; χ² = 0.45, p = 0.50) (Figure 2). “Health Classification” declined slightly, but not significantly, from cohort 1 to cohort 2 (24.8–20.0%; χ² = 1.48, p = 0.22). In contrast, a statistically significant increase was observed in “Health Information Systems” roles (12.0–23.9%; χ² = 11.12, p = 0.001). “Data Management and Analytics” roles showed a non-significant decrease from 22.0 to 15.1% (χ² = 3.48, p = 0.06). Roles classified as “Other” remained low in both cohorts.
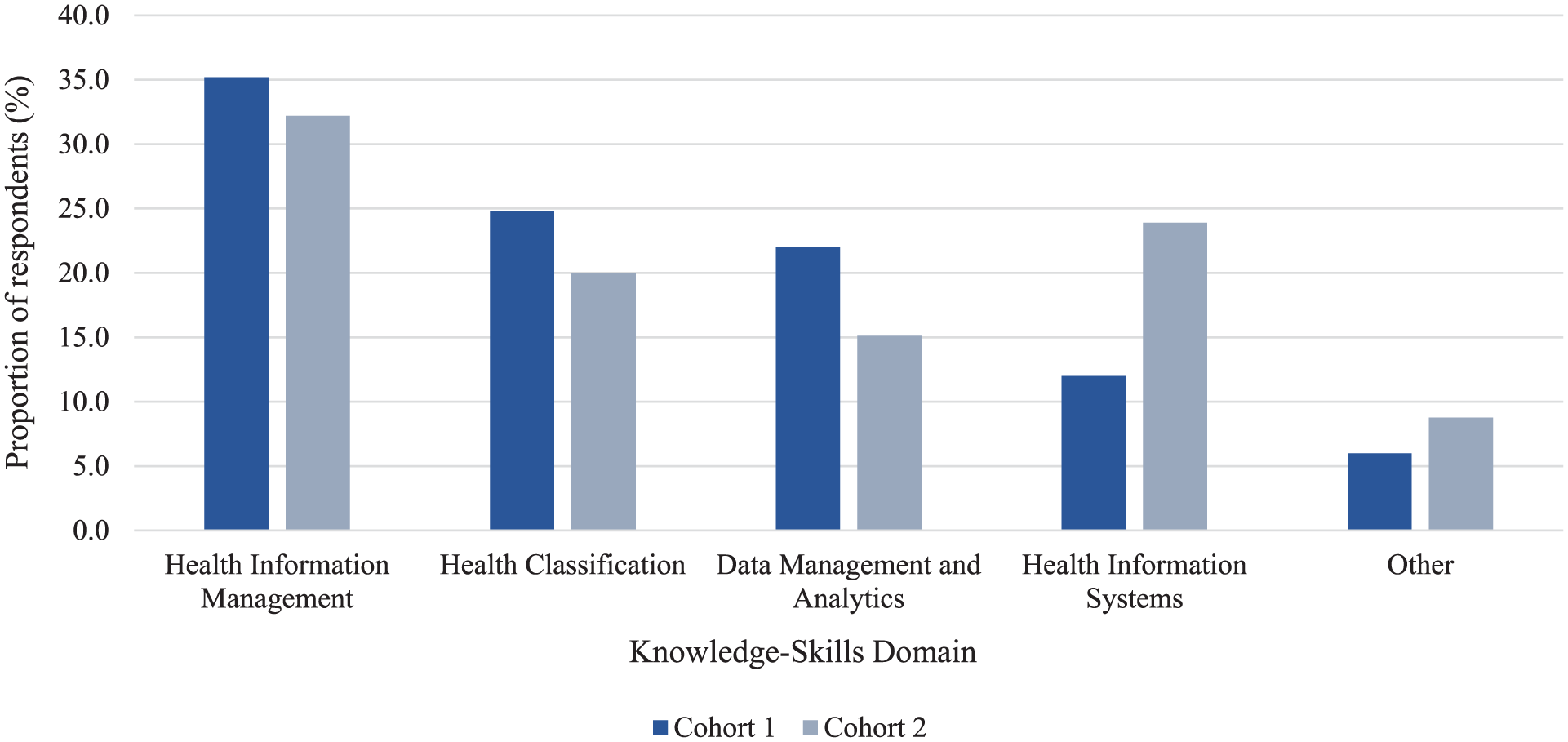
Skills and knowledge domain classification (all positions combined) by cohort, methodology 2.
Similar trends were observed across both methodologies, with decreases in the proportion of graduates classified in the “Health Information Management” and “Health Classification” domains between cohorts 1 and 2 and increases in the “Health Information Systems” domain. There were inter-methodology differences in the classification of roles in the “Data Management and Analytics” domain: methodology 1 showed an increase from cohort 1 to cohort 2 (10.2–16.6%), whereas methodology 2 showed a decrease (22.0–15.1%).
Domain classification of “Health Information Manager” position titles
Position titles may not always reflect the specific skills or knowledge applied in practice; therefore, further analysis was undertaken to explore the domain classification of graduates holding a generic Health Information Manager title (Table 2). Across both cohorts, 30% of graduates (n = 86/288) held this title in their first role, with a slightly higher proportion in cohort 1 (31.9%) than cohort 2 (27.3%). Despite this generic title, the largest proportion of these positions was classified into the “Health Classification” domain using methodology 2 (n = 32, 37.2%), followed by the “Health Information Management” domain (n = 26, 30.2%) and “Data Management and Analytics” (n = 15, 17.4%). A smaller number of Health Information Manager positions were classified under “Health Information Systems” (5.8%) or “Other” domains (9.3%).
Domain classification of generic “Health Information Manager” job titles across the first three positions post-graduation (methodology 2), cohorts 1 and 2 combined.
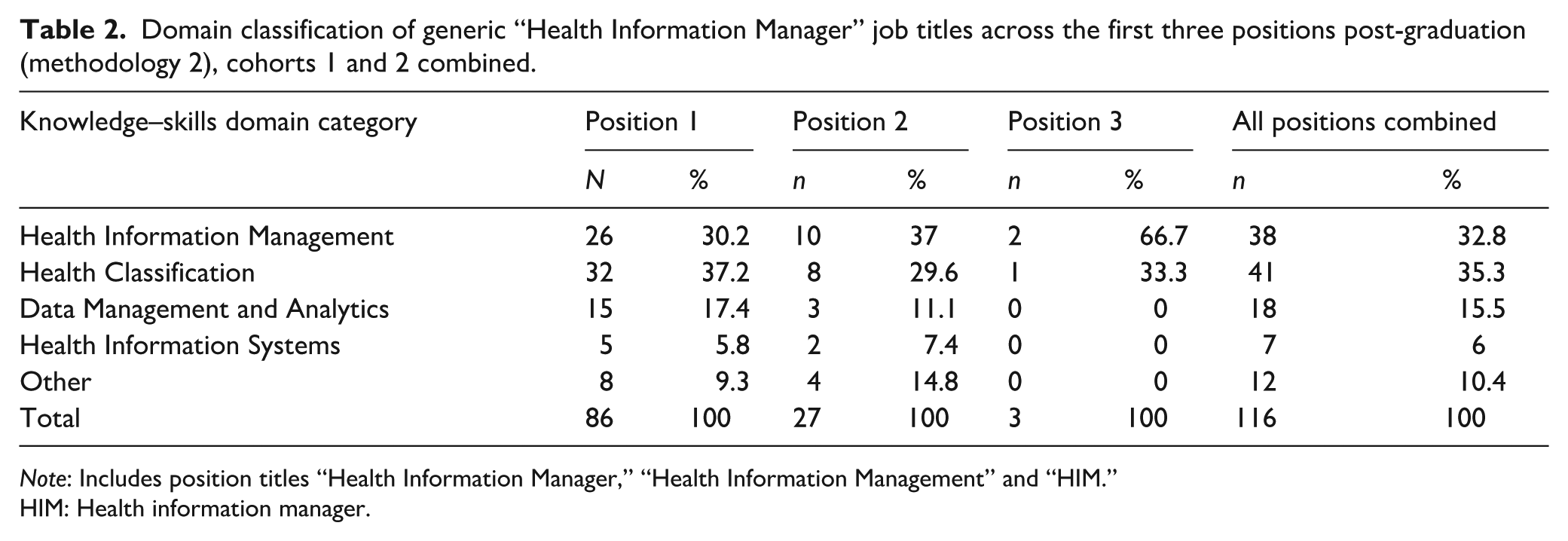
Note: Includes position titles “Health Information Manager,” “Health Information Management” and “HIM.”
HIM: Health information manager.
A similar trend was observed in roles titled Health Information Manager/Clinical Coder, with 48.8% (n = 21) classified to the “Health Classification” domain, 27.9% (n = 12) to “Health Information Management,” and 18.6% (n = 8) to “Data Management and Analytics” using methodology 2. Using the hierarchical system of methodology 1, those in a Health Information Manager/Clinical Coder role were classified to the “Other” category, as they fitted across the two domains of “Health Information Management” and “Health Classification.”
Comparison of classification methodologies
When comparing the categorisation of first position titles using methodology 1 and methodology 2, several statistically significant inter-cohort differences were observed (Table 3). For cohort 1, a significantly higher proportion of roles were categorised under “Health Information Management” using methodology 1 (44.7%) compared to methodology 2 (31.4%; χ² = 5.86, p = 0.02). Similarly, the proportion of roles categorised as “Data Management and Analytics” was significantly greater under methodology 2 (21.8%) than methodology 1 (10.1%; χ² = 8.12, p = 0.004). No significant differences were found for “Health Classification,” “Health Information Systems” or “Other” in cohort 1.
Comparison of the proportion of graduate positions assigned to knowledge–skills domains according to the two classification methods by cohort for position 1.
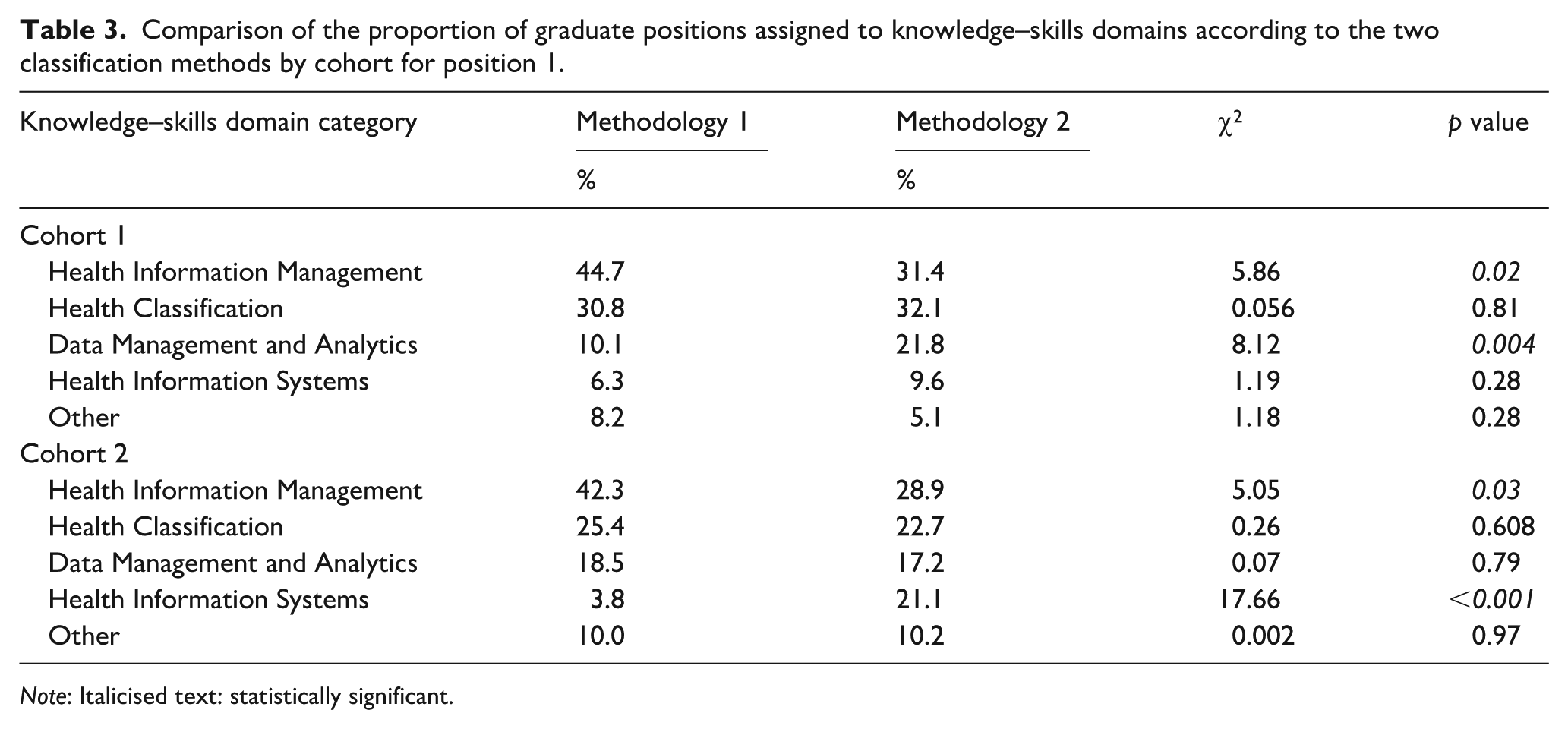
Note: Italicised text: statistically significant.
For cohort 2, “Health Information Management” was again more commonly assigned using methodology 1 (42.3%) compared to methodology 2 (28.9%; χ² = 5.05, p = 0.03). A marked difference was also found in the classification of “Health Information Systems” roles, which were significantly more likely to be identified under methodology 2 (21.1%) than methodology 1 (3.8%; χ² = 17.66, p < 0.001). No significant inter-methodology differences emerged for the domains of “Health Classification,” “Data Management and Analytics” or “Other” roles in cohort 2.
Professional duties
Figure 3 illustrates the breadth of professional duties undertaken by graduates in their first post-graduation role. Respondents could select multiple applicable duties: cohort 1 reported an average of 7.6/37 (20.5%) of the selectable duties, and cohort 2 reported an average of 5.9/26 (22.7%). While the majority of graduates reported undertaking a mix of activities, a small subset (n = 42/284, 14.7%) indicated that their role involved a single duty, most commonly clinical coding for casemix-related funding purposes.
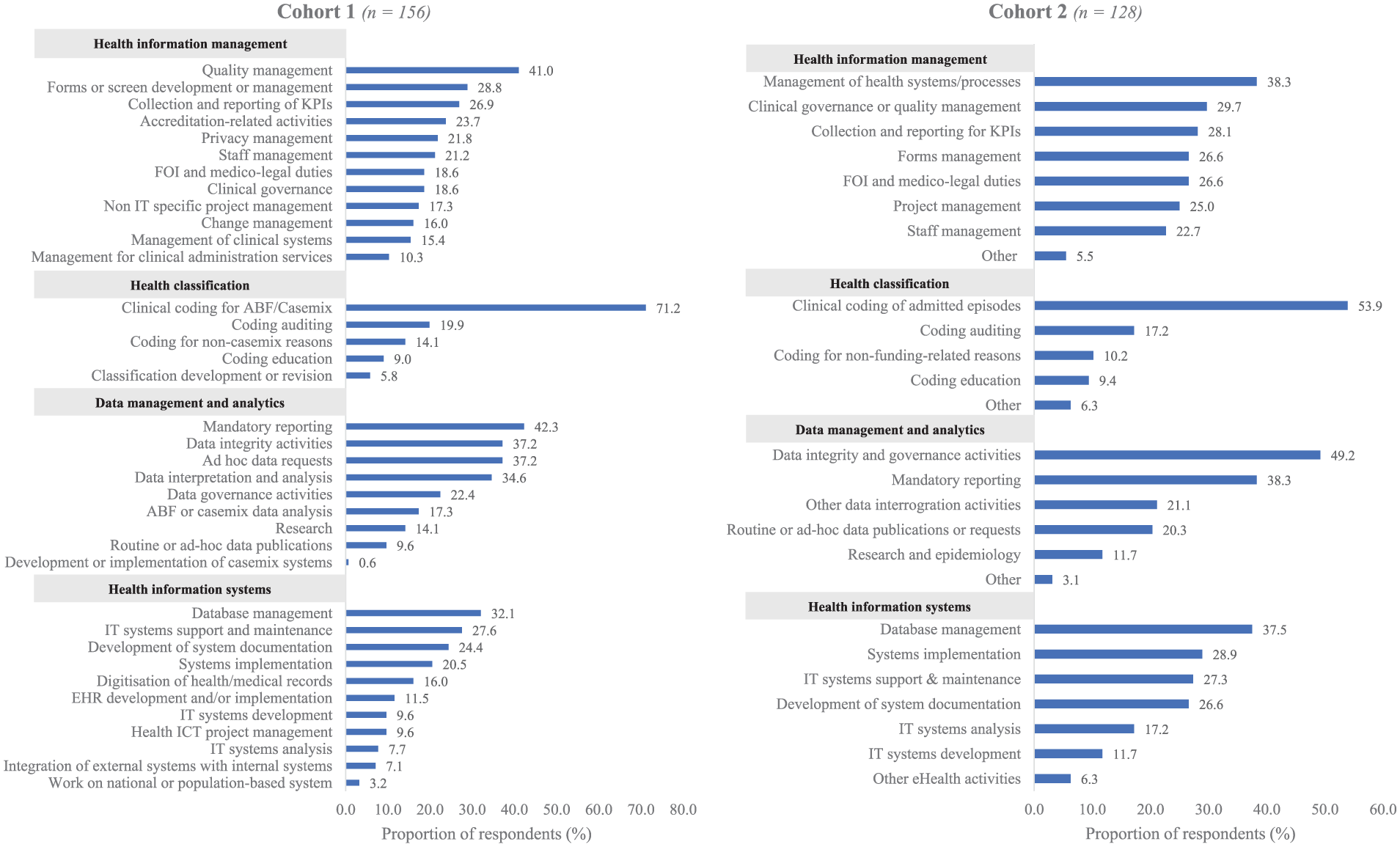
Major duties self-reported by graduates in position 1, grouped by domain (cohort 1 and cohort 2).
Correspondingly, clinical coding remained the most commonly reported activity across both cohorts, with 71.2% (n = 111/156) of cohort 1 graduates and 53.9% (n = 69/128) of cohort 2 graduates in coding-focused roles indicating they performed clinical coding of admitted episodes. Smaller proportions reported other coding-related duties: coding for non-funding purposes (14.1% in cohort 1; 10.2% in cohort 2); coding auditing (19.9%; 17.2%); and coding education (9.0%; 9.4%). Examination of the major duties performed across post-graduation positions 2 and 3 showed a decrease in the number of graduates undertaking clinical coding of admitted episodes in both cohorts, and a slight increase in those moving into clinical coding for other, non-funding related reasons, auditing and education (See Tables S1 and S2, online Supplement).
Many graduates also engaged in information systems and digital health-related duties. Across both cohorts, database management was a frequently reported task (32.1% in cohort 1; 37.5% in cohort 2) alongside systems implementation (20.5%; 28.9%), IT systems support and maintenance (27.6%; 27.3%), and development of system documentation (24.4%; 26.6%). Cohort 1 graduates reported a broader array of digital initiatives such as EHR development (11.5%) and digitisation of medical records (16.0%), which were less frequently noted by cohort 2 graduates.
Respondents reporting duties in data management and analytics often cited mandatory reporting such as to the state Department of Health’s Victorian Admitted Episodes Dataset (42.3% in cohort 1; 38.3% in cohort 2), and data integrity and governance activities (37.2%; 49.2%). Duties related to data analysis and interpretation were also common (34.6%; 21.1%), and 17.3% of cohort 1 respondents reported involvement in Activity-Based Funding (ABF) or casemix data analysis. While this category was not captured directly in cohort 2, other data management and analytic activities such as research and epidemiology (11.7%) were noted. Respondents also reported strong engagement in health information management functions, including quality or clinical governance activities (e.g. 41.0% in cohort 1 for quality management and 23.7% for accreditation; 29.7% in cohort 2 for governance or quality management). Management of health systems and processes was commonly reported by cohort 2 (38.3%) and reflected in a more specific form in cohort 1 (15.4%, clinical systems management). Other consistently reported activities included forms management (28.8%; 26.6%), Freedom of Information (FOI) and medico-legal duties (18.6%; 26.6%), and staff management (21.2%; 22.7%).
Analysis of post-graduation positions two and three revealed a broadening of duties undertaken by HIM graduates as they progressed beyond their first professional role (Table S5 and S6, online Supplement). While position one was often characterised largely by clinical coding, the subsequent roles demonstrated increased diversification via across-domain duties. This trend was evident in both cohorts, although more pronounced in cohort 2. For example, in cohort 2, among respondents reporting on their second position, the two most frequently performed duties were data integrity and governance activities (n = 32/68, 52.5%) and management of health systems/processes (n = 27/68, 44.3%), aligning with the “Data Management and Analytics” and “Health Information Management” domains, respectively. Similarly, in post-graduation position three, the top duties performed were data integrity and governance activities, systems implementation, and development of system documentation, selected by 68.8% (n = 11/16) of respondents who had held a third position. These duties aligned with the “Data Management and Analytics” and “Health Information Systems” domains, highlighting strong emphases on data and systems-focused responsibilities in later career progression.
Domain-specific skill patterns in graduates’ first position (per methodology 2)
Table 4 details how major duties varied by domain in cohort 2. Cohort 2 was selected for this scrutiny as it represented the most recent 5-year period under study, providing a view of contemporary graduate roles. Respondents classified within the “Health Classification” domain (n = 29) predominantly reported coding-related responsibilities. A large proportion (93.1%) undertook clinical coding of admitted episodes, with smaller groups engaged in coding: auditing (37.9%); for non-funding-related reasons (24.1%); and education (20.7%). These roles appeared largely specialised, with minimal crossover into broader data, governance, or IT activities.
Distribution of professional duties by knowledge-skills domain: position 1, cohort 2.
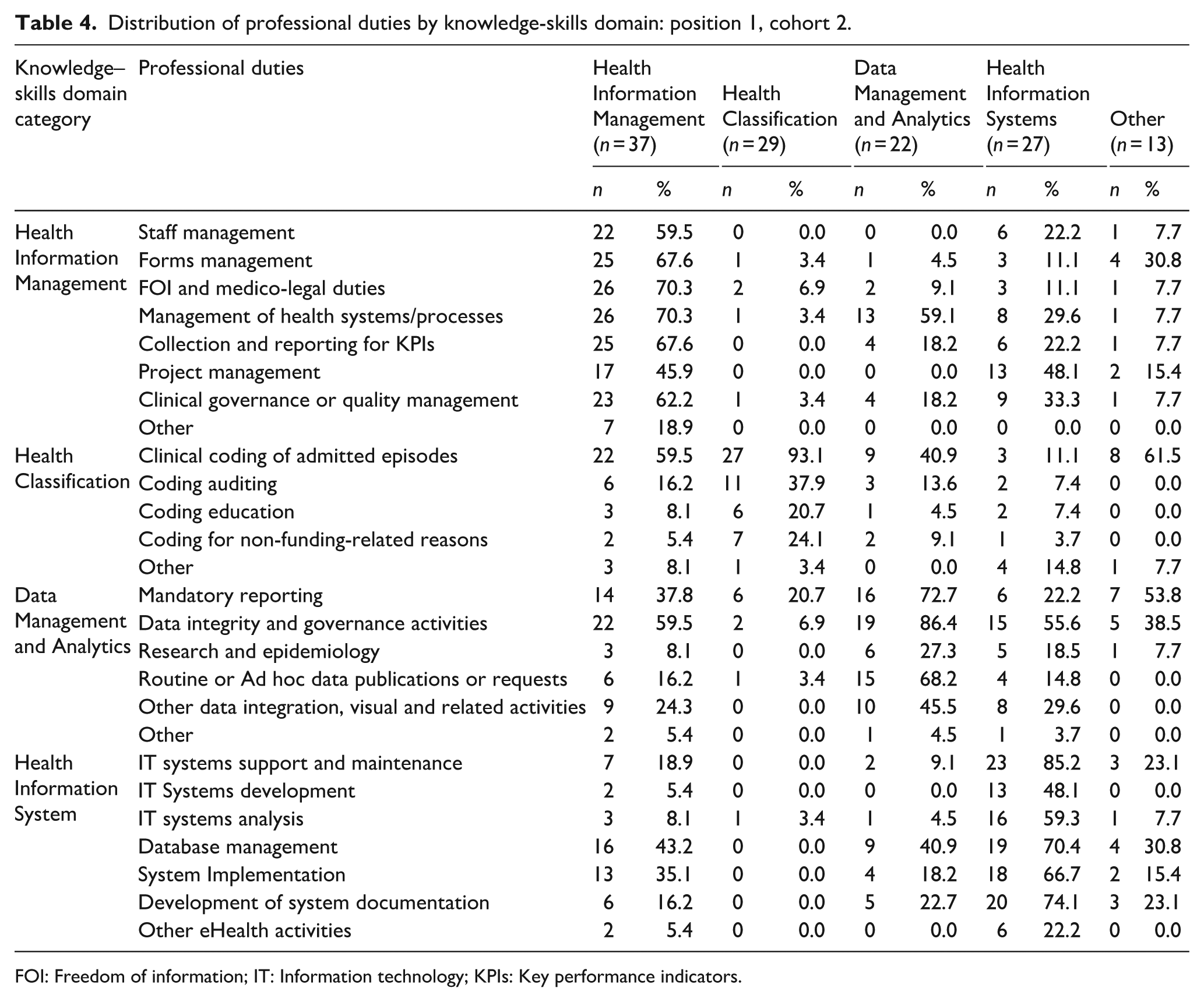
FOI: Freedom of information; IT: Information technology; KPIs: Key performance indicators.
In contrast, respondents in the “Health Information Systems” domain (n = 27) demonstrated a concentrated focus on IT-related functions. High proportions of graduates reported tasks such as IT systems support and maintenance (85.2%), development of system documentation (74.1%), database management (70.4%), and system implementation (66.7%). Some crossover into data integrity and governance (55.6%) and project management (48.1%) was evident. In addition, those classified under “Data Management and Analytics” (n = 22) reported a strong emphasis on data stewardship and reporting. The most commonly reported skills included data integrity and governance activities (86.4%), mandatory reporting (72.7%), and routine or ad hoc data publications or requests (68.2%). Engagement in clinical coding or IT support roles was rare.
Graduates in the “Health Information Management” domain (n = 37) reported the widest range of skills. Commonly reported tasks included FOI and medico-legal duties (70.3%), management of health systems/processes (70.3%), forms management (67.6%), collection and reporting on Key performance indicators (67.6%), and clinical governance or quality management (62.2%). In addition, a substantial proportion reported involvement in clinical coding (59.5%), and data integrity and governance (59.5%). Finally, those in the “Other” category (n = 13), often representing hybrid or emerging roles, demonstrated a more diverse skills profile. Common duties included clinical coding (61.5%), mandatory reporting (53.8%), and database management (30.8%), although fewer respondents reported involvement in more specialised functions such as research, project management, or system development (see Table 4).
Discussion
This study has extended the work of Riley et al. (2020) and Gjorgioski et al. (2023) by providing a contemporary analysis of the professional duties and career trajectories of Australian HIM new graduates. Riley et al. (2020) and Gjorgioski et al. (2023) found that nearly two-thirds of early-career HIM graduates utilised skills spanning at least three of the four core professional domains. The current analysis of a decadal sample of graduate workforce data compared position title-based, and skill-based, classificatory methodologies. Congruent with Bowker and Star’s (1999) theory, the findings show that classification methodology significantly impacts upon how HIM roles are categorised into the four core professional knowledge–skill domains. This underscores the importance of adopting nuanced, skills-based approaches to capture and accurately reflect the evolving complexity of these roles.
Health Information Management domain
Notably, across both cohorts, a greater proportion of roles were categorised as “Health Information Management” when classified by position title alone. Contrastingly, when categorised according to self-reported skills and knowledge (methodology 2), more roles aligned with the “Health Information Systems” and “Data Management and Analytics” domains, indicating that reliance on job titles may oversimplify or misrepresent the scope of duties performed by HIMs. While positions such as Health Information Manager/Clinical Coder consistently matched clinical coding expectations, with minimal crossover into other skill areas, more “generic” titles such as Health Information Manager often concealed significant variations in practice. Roles bearing this title frequently involved activities spanning multiple domains and incorporated clinical coding, analytics, data governance and systems management. This supports the findings of Burns et al. (2025), that even within non-hospital clinical registry settings approximately one in three positions occupied by HIMs retained profession-specific titles such as Health Information Manager or Clinical Coder. The endurance of these position titles, suggested Burns et al. (2025), reflects recognition of HIM graduates’ versatile skills and knowledge in roles across the healthcare sector, highlighting the profession’s adaptability and scope.
Health Information Systems domain
Our analysis has demonstrated that temporal shifts in workforce roles are best captured through detailed investigation of the skills and knowledge used in practice, rather than via position titles; for example, while position titles suggested modest changes, skill-based analysis highlighted a significant shift towards technology-oriented roles. This “technologisation” of HIM roles was particularly evident in the substantial increase, from cohorts 1 to 2, in positions classified under the “Health Information Systems” domain. There was a marked, longitudinal increase in the proportions of graduates undertaking health system implementation, system documentation development, database management, and IT system support and maintenance. These findings mirror global healthcare technology transformations associated with increased digitisation of hospital systems, telehealth, mobile health applications, patient portals, wider EHR adoption, and the expansion of data-driven healthcare – which are gradually reshaping the role of HIMs and expanding their responsibilities (Abdelhak and Händel, 2022; Madlock-Brown et al., 2021). The findings also align with Stanfill and Marc’s (2019) observation of the profession’s adaptation, in the USA, to technological advancement including increasing engagement with AI technologies and input to practice standards for managing healthcare data in an AI-enabled world. Consistent with these shifts, Robinson et al. (2024) reported that over the same timeframe, 12.7% of final-year HIM student professional practice placement proposals at LTU, Australia, were specifically informatics- or health ICT-focused. This prominence reflects other evidence of progressively increasing educational emphases on digital health competencies expected of HIM graduates entering the workforce (Branda, 2021; Flite et al., 2023; Houser et al., 2025b).
Health classification domain
Clinical coding of admitted episodes remained the most frequently reported skill utilised by HIMs in their first post-graduation position. This underscores its foundational importance and relevance within the profession, despite increasing diversification of the workforce (Shepheard and Groom, 2020). There was, however, a slight decrease, from cohort 1 to cohort 2, in the proportion of graduates engaging in clinical coding activities. By their second and third post-graduation positions, the 2017–2021 graduates were less likely to undertake clinical coding roles, instead utilising more skills associated with the “Health Information Systems” and “Data Management and Analytics” domains. The emergence of computer-assisted coding foreshadows a reshaping of the HIM-Clinical Coder roles from direct coding to greater involvement with data analysis, coding auditing and system management (Campbell and Giadresco, 2020). Graduates’ increasing use of non-health classification domains’ skillsets reflects the changing healthcare landscape and technological competencies required for future career development (Madlock-Brown et al., 2021).
Health data management and analytics domain
A key point of divergence between the two methodologies was evident in the classification of roles within the “Data Management and Analytics” domain. Methodology 1 demonstrated an increase in the proportion of graduates assigned to this domain between cohort 1 and cohort 2 (10.2–16.6%), whereas methodology 2 showed a simultaneous decrease (22.0–15.1%). These findings may be partly attributable to an artefactual difference arising from minor inter-survey instrument changes. In the survey administered to cohort 1, the “Data Management and Analytics” domain included a detailed, disaggregated list of duties, for example, data governance and data integrity showed as separate activities, whereas in the cohort 2 survey these showed as a single item (data integrity and governance activities), potentially reducing the specificity with which respondents could align their roles to this domain.
Additionally, the cohort 1 survey included distinct options (e.g. analysis of data for ABF or casemix and casemix system development), which were omitted or collapsed into other categories in the second survey. These changes may have led to underreporting or reclassification of relevant tasks by cohort 2, particularly when applying methodology 2, which relies on mapping the actual duties performed to the domains. The observed decrease in the “Data Management and Analytics” domain under methodology 2 may reflect structural differences in survey design rather than a substantive shift in graduates” professional activities.
These structural differences offer an explanation for the apparent decline in the “Data Management and Analytics” domain; however, broad contextual influences that shape HIMs” perceptions and reporting of their work need to be considered. HIM roles have become more data-driven, yet this shift may not have been fully captured via survey if graduates did not recognise or classify their tasks as aligning with data analytics. HIM professionals in the USA have been urged, given the close HIM-data relationship, to deepen their understanding of data analytics as a core component of practice (Sandefer and Marc, 2019). In Australia, Burns et al. (2025) observed that expanding HIM functions, particularly in clinical registries, require robust skills in data governance, analytics and system interoperability. As such roles proliferate, research opportunities are expected to follow (Nunn, 2018). Australia’s HIMs do not always identify research as a central component of their professional scope: Henderson et al. (2025) found that while many supported research via data access and analysis, they often did not view these activities as part of a formal research remit. This practice–perception disconnection may have contributed to underreporting of analytics-related work in the current study, compounding the methodological artefacts already noted and potentially clouding the true extent to which data analytics is embedded in the contemporary HIM role.
Career mapping
Structured career maps are a beneficial tool for visualising and understanding the breadth of a profession’s roles. The AHIMA’s interactive career map illustrates the profession’s diverse career pathways in the USA. Designed to accommodate a rapidly changing workforce landscape and increasing demand for qualified HIMs, it categorises positions across the profession’s AHIMA-established (2016) core domains and showcases roles using position titles, salaries and descriptors of responsibilities and skills (Madlock-Brown et al., 2021). The membership-centric approach to developing the career map using AHIMA members and subject matter experts, but excluding frequency data, has been critiqued as limiting its generalisability (Madlock-Brown et al., 2021). Nonetheless, it is valuable for comparative analyses.
The CHIMA’s (2014) career matrix offers another perspective on structuring of HIM career pathways. The Canadian matrix visually represents HIM positions classified to the profession’s core domains established by CHIMA. Positions are mapped to entry, intermediate, advanced and master levels of education and experience; further role descriptions are intended for future iterations.
Rafes et al. (2014) highlighted career mapping as a strategic tool for workforce planning, and profession promotion and recruitment. Career maps can raise awareness of professional opportunities among potential entrants, motivate current students, and alleviate attrition, facilitating clearer career goal-setting and highlighting potential trajectories. As the AHIMA map exemplifies, the inclusion of required skills and education enhances transparency and assists in aligning workforce preparedness with emerging industry needs. These principles have direct applicability to the Australian HIM context and the findings of the current study.
Recommendations
Recruiting school leavers into HIM university courses can present obstacles for universities, despite evidence of HIMs’ high employability (Gjorgioski et al., 2023; Riley et al., 2020) and the long-term, Australia-wide shortage of qualified HIMs (HWA, 2013). This presents a critical need for innovative strategies to attract school leavers to the profession’s degree programs. Our findings prompt the recommendations that (a) a career map showcasing opportunities for early career graduates be developed within the Australian context, and (b) research be undertaken on the mobility of mid- and late-career HIMs to illustrate progressive development of the profession’s skill sets.
Limitations
Minor inter-survey differences, and reliance on self-reported data may, respectively, have limited the cohesion of between-cohort analyses and introduced reporting bias. The surveys’ inductive approach to capture pre-defined duties potentially excluded additional activities performed by graduates in practice. Additionally, the comparatively smaller sample sizes of graduates in second and third post-graduation positions somewhat inhibited meaningful conclusions concerning these groups. Finally, the focus on a single university’s graduates prevented examination of cross-jurisdictional differences, a limitation muted by the number of LTU graduates employed in other states/territories.
Conclusion
This research has demonstrated that the methodology applied to classify HIM positions significantly impacts upon the domain in which roles are categorised, underscoring the need for a skill- and duty-based approach to capture accurately the evolving nature of HIM roles. The findings offer valuable insights into HIM workforce trends including greater “technologisation” of HIM roles and provide the foundations for the longitudinal mapping of career pathways and associated skills of HIMs in Australia, and a visual tool (career map). The latter will potentially enhance the profession’s visibility, inform marketing strategies, and showcase career trajectories to current and potential HIM students.
Supplemental Material
sj-docx-1-him-10.1177_18333583251393401 – Supplemental material for Early-career pathways in health information management: A comparison of graduates’ position titles and knowledge-skill domains using two classificatory methodologies
Supplemental material, sj-docx-1-him-10.1177_18333583251393401 for Early-career pathways in health information management: A comparison of graduates’ position titles and knowledge-skill domains using two classificatory methodologies by Stephanie Gjorgioski, Abbey Nexhip, Kerin Robinson and Merilyn Riley in Health Information Management Journal
Footnotes
Acknowledgements
The authors acknowledge Jennifer Muresan for her contribution to the initial classification of graduate position titles, undertaken as part of her final-year health information management project at La Trobe University, Australia. The authors would also like to acknowledge the Discipline of Digital Health and Information Management, Department of Public Health, La Trobe University for their support.
Authors’ note
All authors had full access to the data in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.