
Abstract
Keywords
Introduction
Health care in the 21st century has been transformed by the rapid uptake of health information-related technologies, advancements in bioinformatics, costing models and service and system integration. Health information is central to much of this change. The management and integrity of health data and information are reliant upon the specialist work of health information managers (HIMs) as the “expert informational and ethical gatekeepers” (Robinson and Lee, 2021: 4–5) whose “undisputed expertise in health data provenance, data integrity, confidentiality, privacy and access, applies equally to all health data and their uses.” Internationally, HIMs occupy a central role in the adoption and maintenance of health information technology in association with their knowledge of health informatics and the organisation of electronic healthcare data (Šendelj, 2020). The rapidly evolving health ecosystem has compelled HIMs to re-think and innovate their professional skill set to meet the anticipated future demands of the healthcare industry.
The recent peer-reviewed and professional practice literature have revealed focal shifts for the profession, including a re-balancing to accommodate the historical, generalist HIM roles and progressively greater specialisation in health informatics, health data modelling and analytics, and electronic health data governance, including security (Butler, 2017; Kwan et al., 2022; Robinson and Lee, 2021; Zhou et al., 2018). Importantly, complementary parallels between specialist health information management and health informatics fields have been identified (Valerius et al., 2015). By way of example, in Australia, the status of electronification of health information has transformed in the past 5 years with increased focus on electronic medical records (EMRs) (Bonello et al., 2021; Hendry, 2018) and digitisation (Bonello et al., 2021).
While health information privacy and the specialised custodial and curation responsibilities have historically been significant HIM roles, suggested new or extended roles present themselves in the areas of health literacy (Kyabaggu et al., 2022), mobile data associated with new digital technologies, patient-reported outcome measures and fitness-for-purpose of EMRs including for non-acute healthcare systems (Robinson and Lee, 2021). The evolving HIM roles also reflect the long-standing need for increased standardisation in all aspects of health information management. In parallel with these developments, demand is expected to increase significantly for HIMs’ expert health classificatory, interpretative and auditing skills, in response to the expanding functionalities and embeddedness of EMRs and the artificial intelligence (AI)-led shift from manual to automated clinical coding (Beesley et al., 2021; Robinson and Lee, 2021; Stanfill and Marc, 2019). Therefore, it is essential that graduates entering the profession are well prepared to meet the healthcare industry’s contemporary needs (Jackson et al., 2016). A previous survey of the 5-year (2012–2016) cohort of Australian HIM graduates from La Trobe University (LTU) revealed that they utilised professional skills and knowledge across four identified domains: health information management (including health information science); health classifi-cation (including clinical, and finance-related, knowledge); (health) data management and analytics; and health information systems (including health information and communication technologies (ICTs)) (Riley et al., 2020). The current study involved the subsequent 5-year (2017–2021) cohort of graduate HIMs’ early professional careers.
Aims and objectives
The study aims were to identify the early career employment characteristics and experiences of the recent, 5-year (2017–2021) cohort of graduate HIMs from LTU, Australia. The objectives were as follows:
To identify the employment roles and destinations of Australia-based, graduate HIMs from 2017 to 2021.
To investigate the primary knowledge and skill sets utilised by the 2017–2021 cohort of new graduate HIMs in the performance of their professional roles and as related to the previously identified professional knowledge–skill domains.
To compare the outcomes from (1) and (2) with those from the previous workforce study of 2012–2016 graduate HIMs (Riley et al., 2020).
Method
Study design and sample
A cross-sectional study design was utilised. The study population comprised 222 LTU graduates of the combined degree programmes (CPDs) comprising bachelor-master and double-bachelor degrees (n = 126, 56.7%), and the profession-entry, graduate-entry master (GEM) degree (n = 96, 43.2%) in health information management, who qualifi-ed at LTU in the 5-year period (2017–2021). All courses held external accreditation from the Health Information Management Association of Australia (HIMAA) and their curricula were compliant with HIMAA’s HIM profession-entry competency standards (HIMAA, 2017). The graduates were from the university’s Melbourne and Sydney campuses. Their names were obtained from a database held within LTU’s Discipline of Health Information Management and contact details were obtained via the researchers’ extensive professional networks, HIM practitioners and social media. Excluded from the study were graduates who were (a) practising outside Australia, (b) non-locatable or non-responsive to the researchers’ invitations and (c) members of the research team. The study sample of 200 eligible members was derived following the application of the exclusion criteria.
Survey instrument
The survey instrument was based on Ammenwerth and Hackl’s (2015) survey of biomedical informatics graduates and Riley et al.’s (2020) survey of health information management graduates. Feedback from the pilot study, which involved HIMs who graduated pre-2012, informed amendments to the survey instrument. The instrument was designed to elicit quantitative and qualitative data (see Supplemental Appendix S1). A forced response format sought the following: age, year and qualification(s) awarded, additional postgraduate education, the time elapsed between course completion (i.e. final examinations) and employment in the graduate’s first profession-related role, titles of up to three HIM positions held postgraduation, major duties performed in each role and non-HIM-related employment, postgraduation. Open-ended items sought information on career pathways and the use of knowledge–skills learned at university and on the job.
Data collection
The anonymous survey was distributed to members of the study sample in electronic form, via Research Electronic Data Capture. Non-respondents were followed up after 6 weeks, and non-response after two attempts at contact resulted in exclusion from the study.
Data analysis
Categorisation of respondents’ position titles into the previously established HIM knowledge–skill domains was undertaken independently by two of the researchers (MR and NP) (refer to Appendix A). The domains, shown in Box 1, were established by Robinson (2017) and adopted, with the addition of an “Other” category, in the earlier study (Riley et al., 2020). In discrepant cases where a broad-based position may have fitted two or more categories, resolution was achieved by the application of a hierarchy and allocation to the domain in which the respondent had identified the most skills. Inter-rater agreement was calculated using Kappa statistics. Data were analysed using SPSS version 26. Chi-square and p-values (α = 0.05) were used to determine any statistically significant differences (a) between CDP and GEM graduates within the 2017–2021 cohort and (b) in selected outcomes between the 2012–2016 and 2017–2021 cohorts. Items with missing responses were excluded from the analysis, resulting in variation in denominators.
Broad categories of position titles of HIMs.
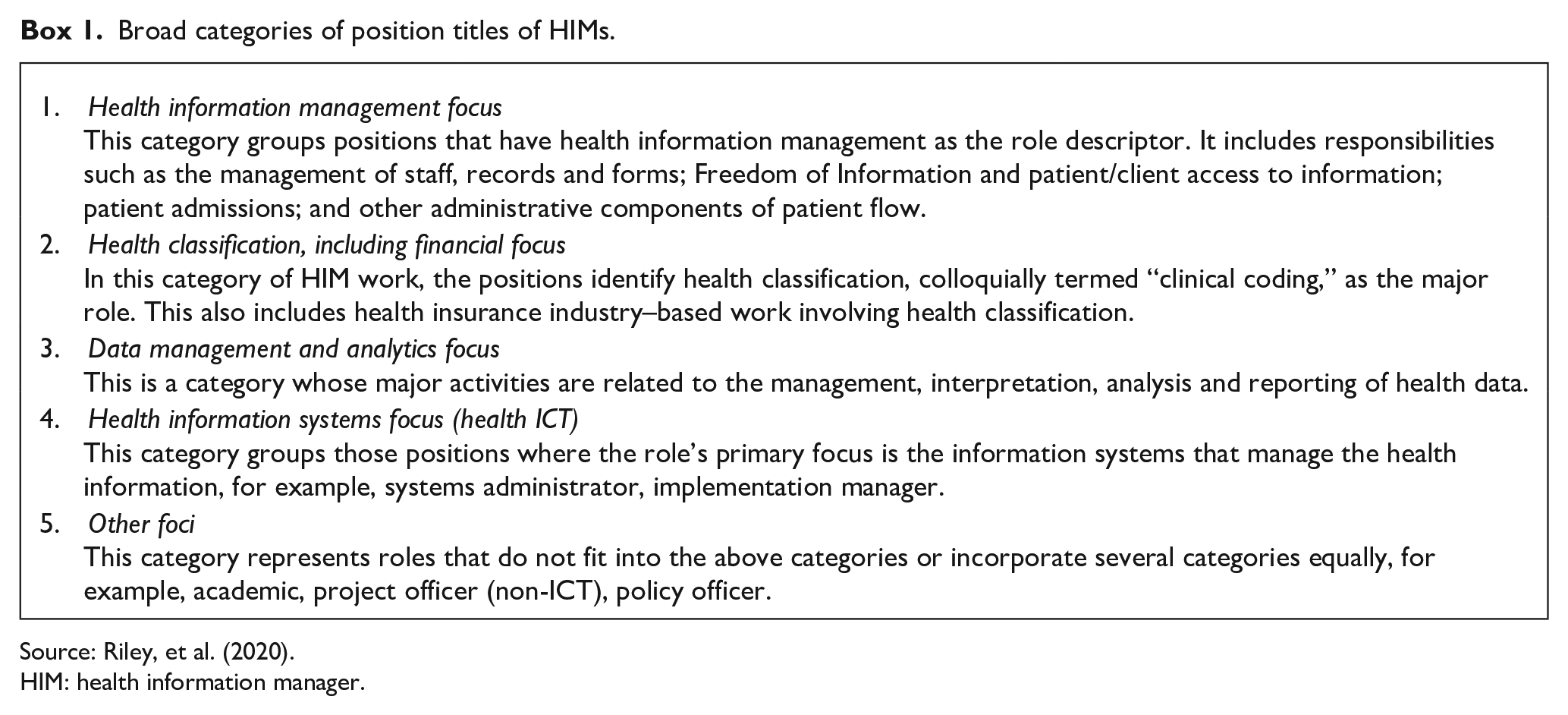
Source: Riley, et al. (2020).
HIM: health information manager.
Ethics approval
Ethics approval was granted by the LTU Human Research Ethics Committee (HREC22072).
Results
For convenience in reporting, the collective subjects of the current study (2017–2021) are referred to as cohort 2 and those in the 2012–2016 study (Riley et al., 2020) are referred to as cohort 1.
Response rate
In all, 47 of the 200 sample members did not respond; 21 (44.7%) of these had completed a CDP and 26 (55.3%) the GEM degree. The reasons for non-response were unknown. Three further participants commenced the survey but provided no data. Therefore, data were available from 150 sample members creating an effective response rate of 75% (Figure 1), slightly lower than the previous study’s 80% response rate.
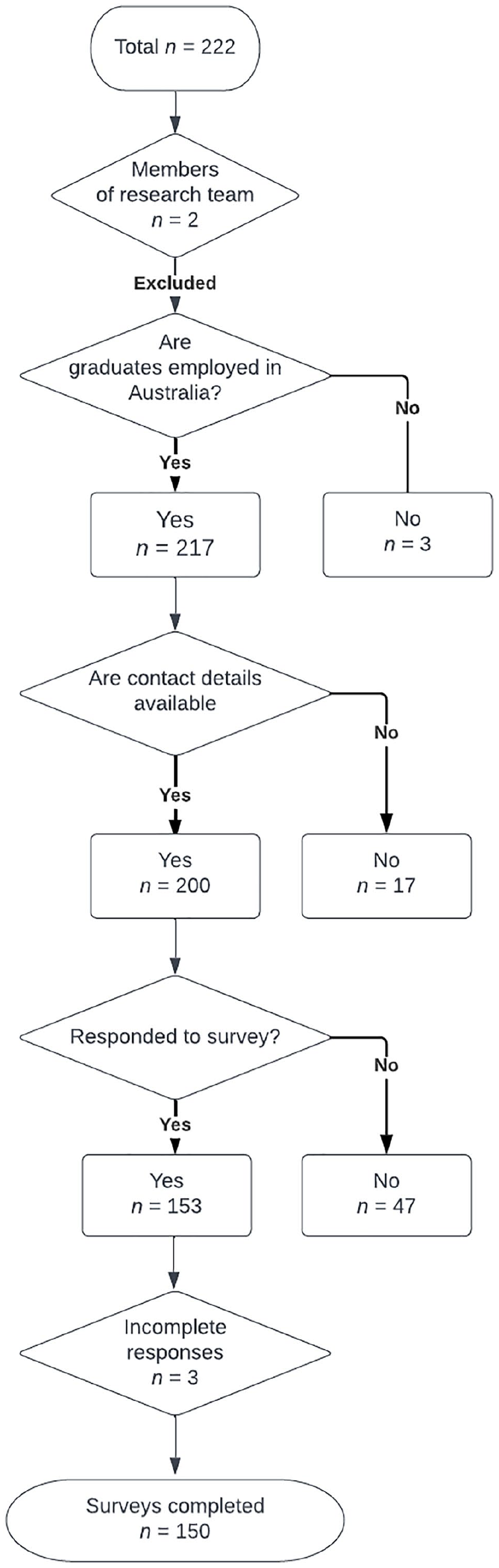
Response pathway to the LTU HIM graduate career survey, cohort 2 (2017–2021).
Demographic data
In total, 95 (63.5%) cohort 2 respondents had completed a CDP, and 55 (36.7%) had completed the GEM degree. Most were female (n = 125/150); 81% (n = 77/95) of CDP respondents were aged 20–29 years and 58.2% (n = 32/55) of the GEM respondents were over 30 years of age at the time of survey. Characteristics of the CDP-qualified respondents were similar in both cohorts, except for a 12% decrease in cohort 2 GEM graduates aged over 30.
Employment
Of the cohort 2 respondents, 90% (n = 132/150) had worked in an HIM-related role, compared to 96% (n = 161/167) from cohort 1. This constituted a statistically significant difference (χ2 = 7.98, p = 0.005). Table 1 shows the time from course completion to securing professional employment. There was no inter-cohort difference between the proportions of respondents in each age group who obtained a position prior to course completion (Figure 2). A decreasing shift was seen in cohort 2 from the 20–29 years age group (n = 89/132) to the 40 years-plus age group (n = 11/132). The proportion of cohort 2 respondents employed prior to course completion was highest for the 40 years-plus category (54.5%) and lowest for the 30–39 years age group (46.9%). There was a slight increasein the relative proportion across all age groups of cohort 2 respondents who obtained a position prior to course completion when compared to cohort 1.
Time from course completion to securing employment, by qualification, cohort 2 (2017–2021) and cohort 1 (2012–2016).
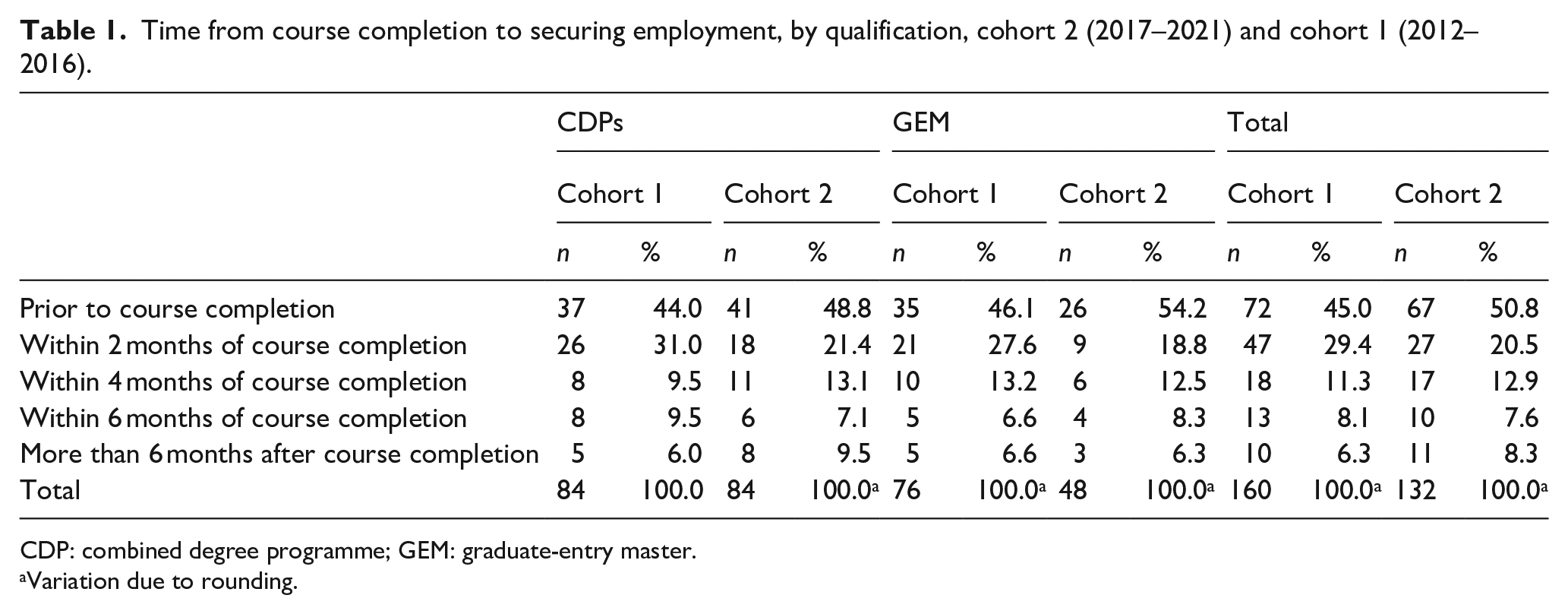
CDP: combined degree programme; GEM: graduate-entry master.
Variation due to rounding.
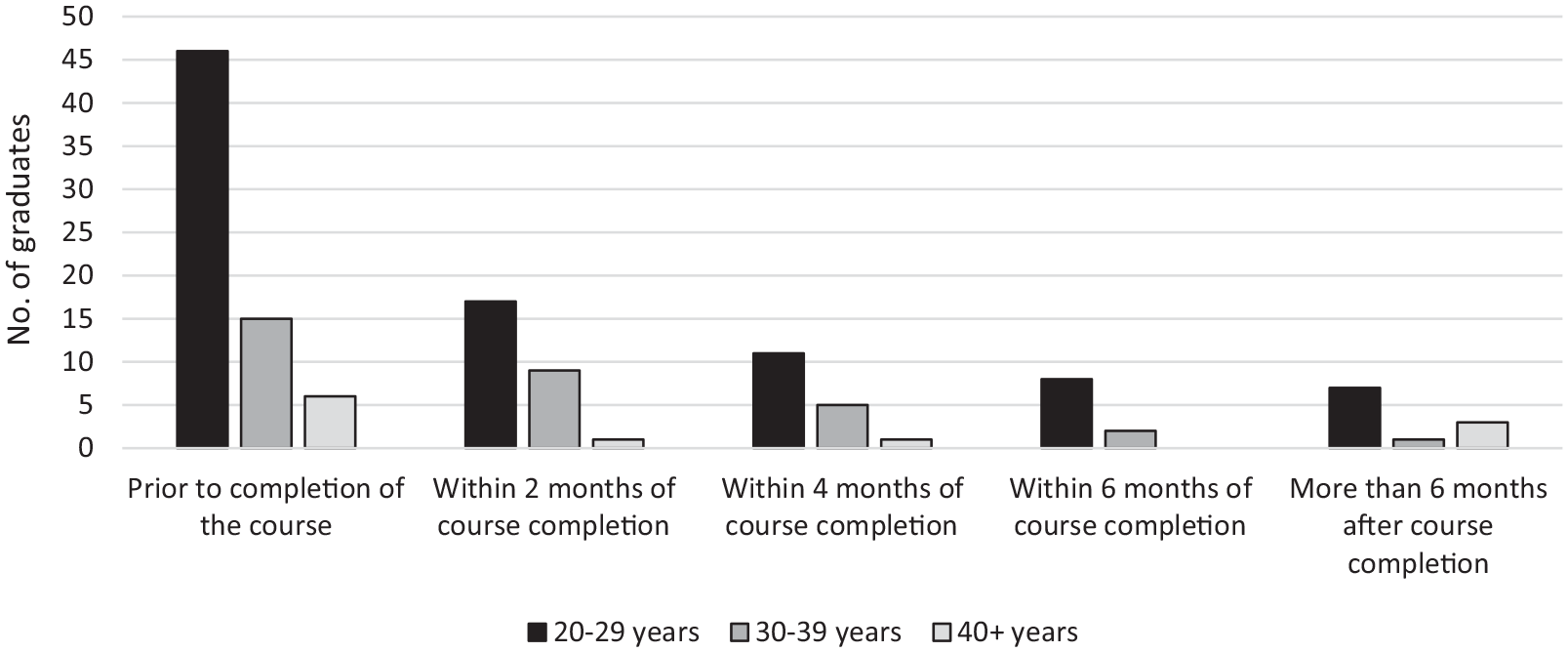
Time to employment by age group, cohort 2 (2017–2021).
The current survey offered a wider selection of employing agency types (Table 2) than the 2012–2016 survey instrument, which contained options only for “public” and “private” sector employment. In cohort 1, more graduates had been employed in the public sector than in the private sector in their first position (Riley et al., 2020). When the categories in Table 2 were collapsed into public and private only, 87% of the cohort 2 respondents were employed in public sector organisations in their first position, compared with 82% in cohort 1 (χ2 = 3.4, p = 0.065). There was no significant difference between cohort 2 CDP and GEM respondents concerning the type of employing agency for their first position (χ2 = 1.35, p = 0.25). Most (89.2%) cohort 2 respondents obtained positions in the state of Victoria, with the remainder distributed throughout New South Wales and the Australian Capital Territory, and a small number in Queensland and South Australia. This detail was not available for cohort 1.
Employing agency, first position, cohort 1 (2017–2021).
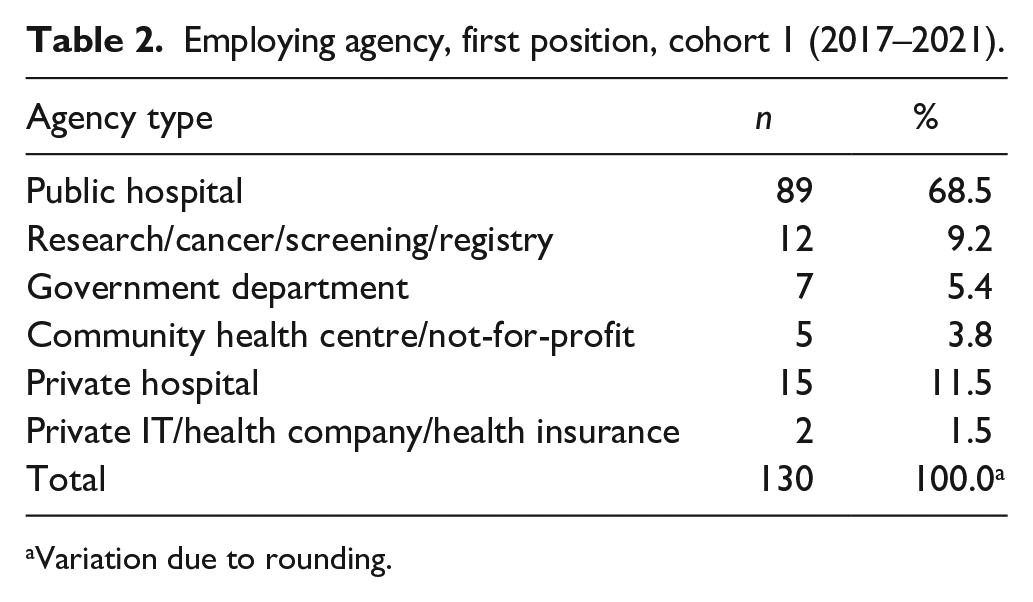
Variation due to rounding.
An examination of the employing agencies of cohort 2 members who obtained second positions within the study period showed an 11% (n = 35/61) decrease, from cohort 1, in those employed in public hospitals and, conversely, a 14.8% increase in those working for government departments (n = 9/61). Private hospitals employed only 11.5% of cohort 2 respondents in their second positions, and a comparative increase was observed in those moving to private ICT and health insurance companies (4.9%). Of the 16 respondents who had three positions within the study period, 93.8% were employed in the public health sector and one moved to a private hospital.
In total, 18 respondents (55.5% CDP, 44.5% GEM) had not worked in an HIM-related role. “Healthcare and medical” (n = 4) and “government and defence” (n = 5) were the industries most frequently selected by this group; other employing industries included “administration and office support,” “call centre and customer support,” “hospitality and tourism,” “information and communication technology,” “legal,” “retail and customer product,” “insurance and superannuation,” “transport and logistics” and no-employment. When prompted to comment on their non-HIM employment, four respondents described roles that could be classified as health information management related (e.g. “First year out of uni as Performance and Costing Analyst, currently management consultant in data and reporting” [Participant 24], and “. . . investor relations, finance, digital and technology” [Participant 89] for a large, national private health network).
Number of positions
Table 3 shows comparable percentages for cohorts 1 (55%) and 2 (53%) members’ occupancy of only one position. There was no statistically significant, between-cohort difference in the proportion of respondents who had held three or more positions during the respective study periods (χ2 = 0.62, p = 0.44). The cohort 2 respondents who had held three positions since course completion were more likely than those who had held one position to have graduated early in the study timeframe; this was consistent with the findings for cohort 1 (refer Figure 3); and 75% (n = 12/16) of cohort 2 respondents who had moved into a third position had completed an undergraduate degree (CDP). A comparison of the cohort 2 CPD (57.8%) and GEM (44.7%) respondents who held one position only showed no statistically significant differences (χ2 = 2.08, p = 0.15). By contrast, statistically significantly more GEM (46.8%; n = 22/47) than CPD (27.7%; n = 23/83) graduates had held two or more positions (χ2 = 4.83, p = 0.02). Overall, there were no significant differences between CDP and GEM graduates holding three or more positions postgraduation (χ2 = 0.98, p = 0.32).
Proportions of HIM graduates from cohort 2 (2017–2021) and cohort 1 (2012–2016) held one, two and three positions.
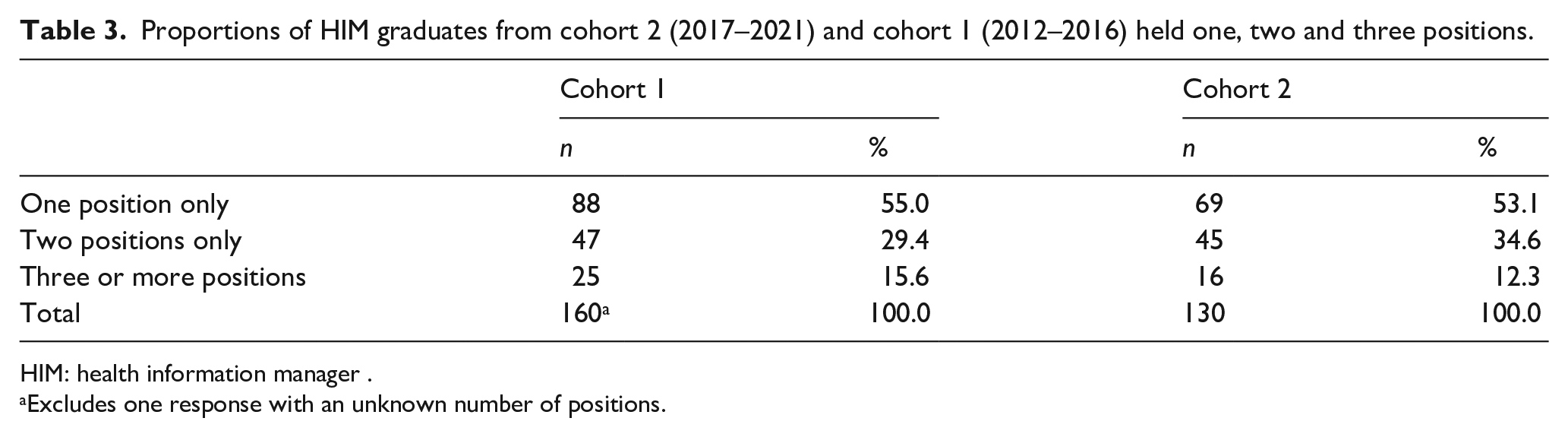
HIM: health information manager .
Excludes one response with an unknown number of positions.
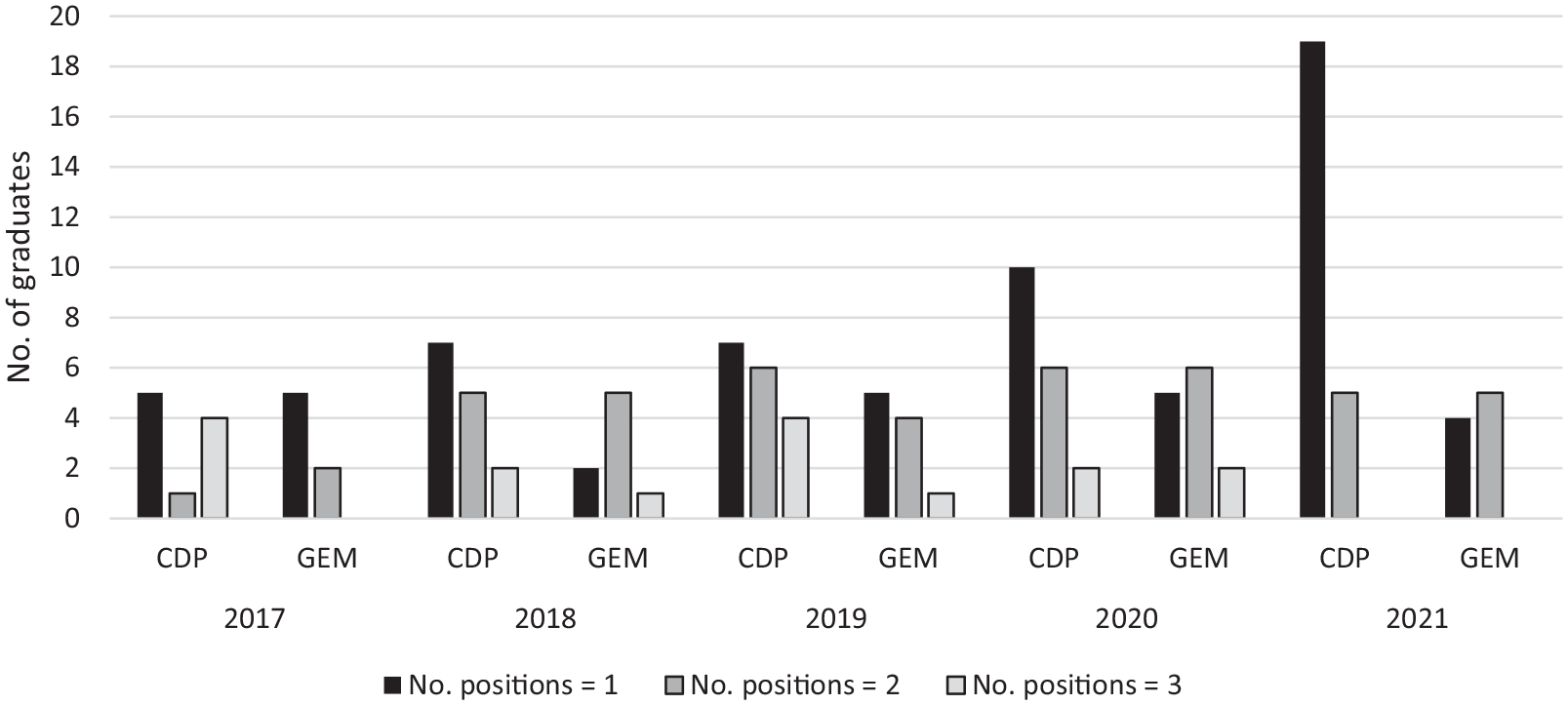
Number of HIM-related positions held since graduation, by qualification and year of graduation, cohort 2 (2017–2021).
Position titles
Table 4 shows the proportion of position titles from all (first, second and third) positions combined, categorised into the four HIM knowledge–skill domains and the additional “Other” category. High inter-rater agreement (K = 0.875) was achieved following independent categorisation of position titles. There was no significant between-cohort difference in the proportions of graduates filling roles titled “Health Information Manager” or in the “Other” category. However, there were statistically significantly fewer graduates from cohort 2 than cohort 1 employed in “Health Classification” roles, and statistically significantly more employed in “Data Management and Analytics” and “Health Information Systems” roles.
Comparison of categorisation of position titles (all positions combined) of health information graduates between cohort 1 (2012–2016) and cohort 2 (2017–2021).
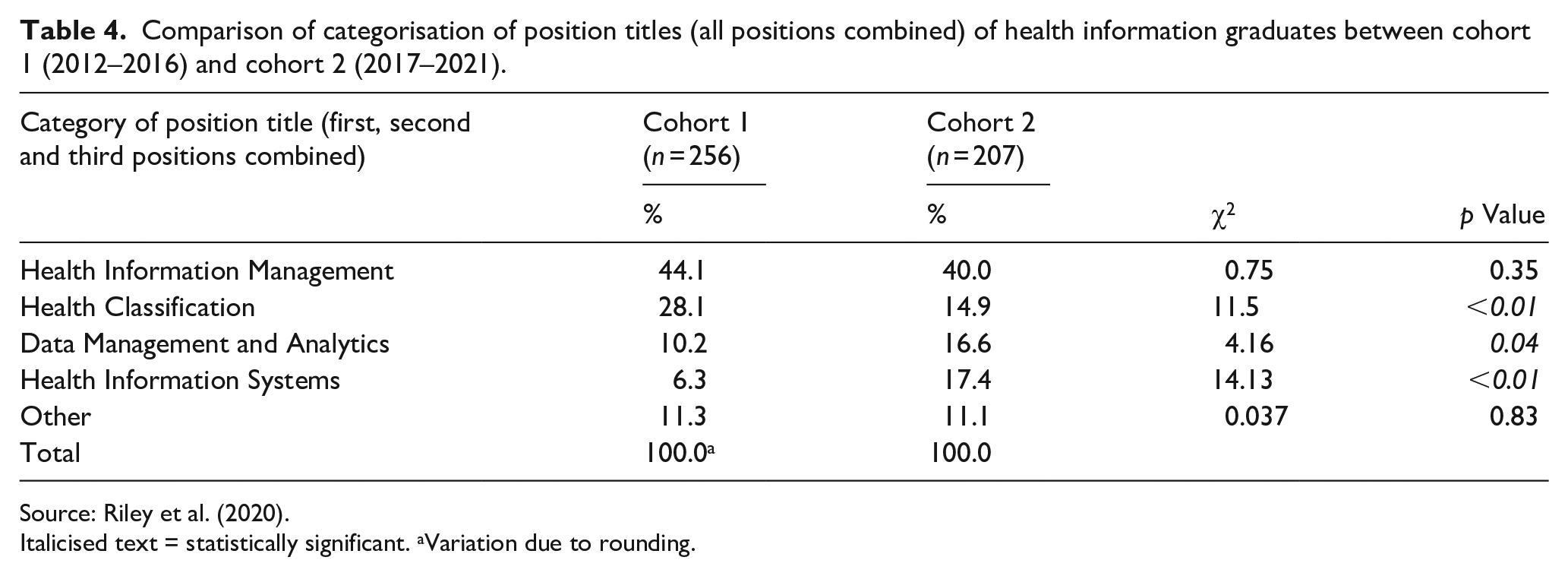
Source: Riley et al. (2020).
Italicised text = statistically significant. aVariation due to rounding.
A cross-cohort comparison of titles of respondents’ first, second and third positions showed consistency in the proportions employed in roles in the “Health Information Management” category (Table 5). The “Health Classification” category showed the greatest difference, both between-cohort and across the study timeframes. While 25% of the cohort 2 respondents commenced in a “Health Classification” role, by the end of the study period, 6.3% of those who moved to a third position had assumed a classification role. By contrast, 30.8% of the cohort 1 respondents had obtained a first position in “Health Classification” and 24% of those who moved to a third position assumed a “Health Classification” role. The difference in number of respondents from each cohort whose first position was a “Data Management and Analytics” role was not statistically significant (χ2 = 3.57, p = 0.59). There was a marked increase in respondents in cohort 2 who assumed a “Data Management and Analytics” role in their first, second and/or third position when compared to the cohort 1 respondents. Table 5 shows increases in the percentages of graduates who moved to a “Health Information Systems” role by their second and/or third position. The cohort 2 graduates showed a comparative increase in uptake of “Health Information Systems” roles in their second (14.8%, 12% increase) and third (31.3%, 15.3% increase) roles. Contrastingly, the cohort 1 graduates were in a “Health Information Systems” role in their second (2.8%) and third (16%) positions, respectively.
Comparison of categorisation of position titles of health information management graduates between cohort 1 (2012–2016) and cohort 2 (2017–2021).
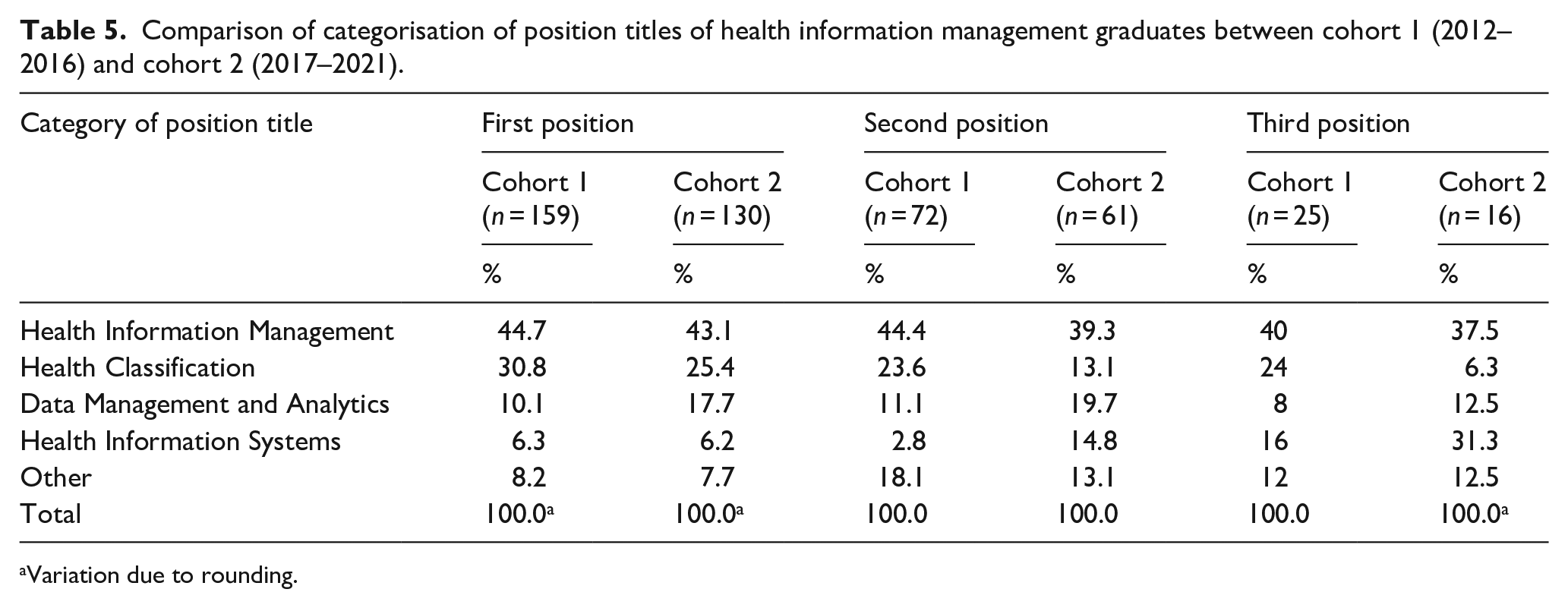
Variation due to rounding.
Knowledge–skill domains used by health information management graduates
Utilisation of all knowledge–skills domains was reported by almost the same proportion of respondents in both cohorts (26.4%, 2012–2016; 25%, 2017–2021). There were no statistically significant differences between the cohort 2 CDP and GEM respondents’ use of all four domains of knowledge–skills in their first position (χ2 = 0.54, p = 0.45). Most respondents were undertaking roles that required them to utilise three (39.1%) or four (25%) of the four core HIM knowledge–skills domains (Table 6); this was consistent with the experience of the cohort 1 graduates. Where cohort 2 graduates used three knowledge–skill domains, the most common combination was “Health Information Systems, Data Management and Analytics and Health Information Management” (25%). While more GEM (31.9%) than CPD (21%) respondents reported using this combination, the difference was not significant (χ2 = 1.89, p = 0.17).
Number and type of knowledge–skills competency domains utilised in the graduates’ first position, stratified by qualification, cohort 1 (2012–2016) and cohort 2 (2017–2021).
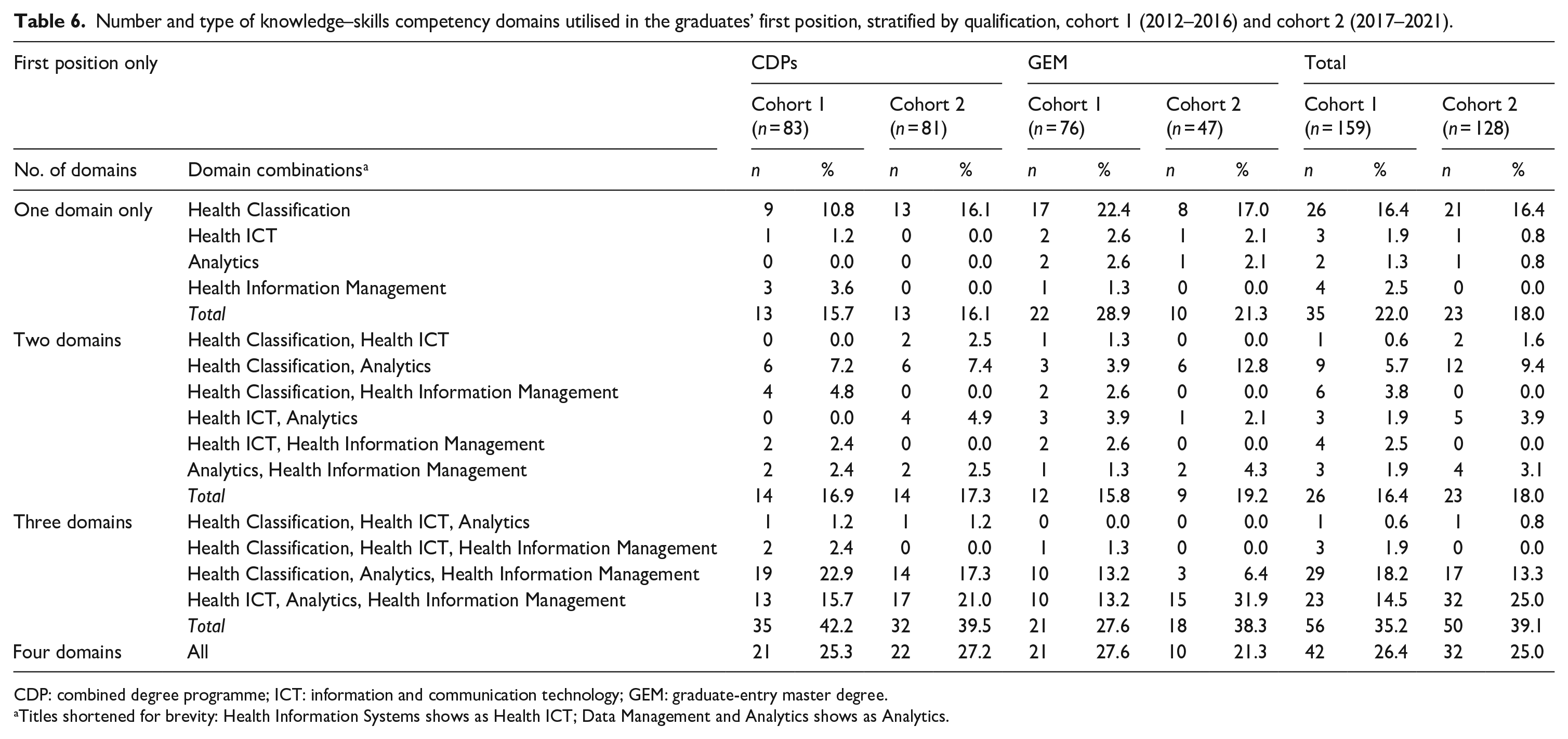
CDP: combined degree programme; ICT: information and communication technology; GEM: graduate-entry master degree.
Titles shortened for brevity: Health Information Systems shows as Health ICT; Data Management and Analytics shows as Analytics.
Only 18% of the cohort 2 respondents were using a single knowledge–skill domain; this was not statistically significantly different from the 22% reported for cohort 1 (χ2 = 0.72, p = 0.40). In cohort 2, there were statistically significantly more GEM than CDP respondents who used only one domain of knowledge in their first position (χ2 = 14.16, p = 0.0001). Consistent with the findings from the earlier study, the most common knowledge–skills domain for those who used only one domain was “Health Classification” (reported by 16.4% of respondents in each cohort). There were no statistically significant differences between CPD and GEM respondents who used “Health Classification” only (χ2 = 0.02, p = 0.88). The findings relating to (a) further study undertaken by the respondents and (b) the free-text (qualitative) responses will be reported in detail in a separate paper.
Discussion
This study of a second, 5-year cohort (2017–2021) of LTU graduate HIMs investigated their employability, employment destinations and knowledge and skills used in the workplace, and compared these with the experiences of the immediately preceding cohort (2012–2016) (Riley et al., 2020). The response rate suggested that the results were representative and may be generalised to other new graduates of HIMAA-accredited health information management courses in Australia.
HIM graduates’ roles
Our findings demonstrated consistently high employability of HIM graduates in first positions categorised within the “Health information Management” and “Health Information System” domains. New graduate-HIMs are increasingly acquiring roles in the EMR environment, with enhanced foci on the following: analysis of these electronic data, health business analysis, health digital product specialisation, clinical systems management and health information governance. This shift in the graduates’ first roles was seen in the statistically significant decrease, from cohort 1 to cohort 2, in those entering classification-coding roles and an increased uptake of health data analysis roles. The shift in recent graduates’ second and third positions, to roles primarily focused on health information systems and technology, also reflected a pattern of change. This finding may be artefactual or, alternatively, an early reflection in Australia of Stanfill and Marc’s (2019: 63) observation that the US HIMs needed to be active in supporting AI technology, including the development of practice standards for the “management of healthcare data and information in an AI-enabled world.” It is important also to acknowledge the “sometimes blurred” boundaries between health classification and data analytics, including where analytics roles involve applications of HIMs’ specialist knowledge of health classification and activity-based funding models. We postulate that these shifts reflect the influences of the rising prominence of digital technologies and the acceleration of the ongoing digitisation of health information across health care. Our assessment is supported by the Australian Government, National Skills Commission’s (2021: 125) recent identification of “data and digital skills” as “the fastest growing emerging skills” required by employers, based on job advertisements. When contextualised internationally, our findings reflect a greater need for data analysis and health information technology expertise in the workforce (Goldacre et al., 2020) and the marked increase in healthcare bureaucratic and regulatory rules (Martin and Sinsky, 2016).
Knowledge–skill domains
Our previous research revealed that new graduates were well prepared for workforce entry and, in their professional practice, “utilise[d] most or all of the specialised domains of professional knowledge and skills studied at university” (Riley et al., 2020: 93). These findings were repeated in the current study, with almost two-thirds of graduates utilising three-quarters of all of the professional knowledge–skill domains in their early career role(s). The decrease, since the earlier study, in the number of graduates utilising only one knowledge–skill domain (predominantly health classification), aligns with the decrease in graduates who are undertaking coding-related roles.
Proportionally, there has been a small shift in the focus of the knowledge–skill domains taught to undergraduates between cohort 1 and cohort 2. During the 4-year cohort 1 course, the proportion of each of the four knowledge–skill domain subjects within the 32 subjects offered was as follows: health information management (37.5%) (includes health information science and professional practice); health classification (25%) (includes clinical, and finance-related, knowledge), (health) data management and analytics (12.5%), and health information systems (includes health ICTs) (12.5%). There were an additional four subjects comprised of either elective or core university-based first-year subjects. For cohort 2, the proportion of both (health) data management and analytics subjects and health information systems subjects had increased to 15.6% following the addition of one subject to each of these domains, to replace two of the core first-year subjects. There was no intra-cohort change in the proportion of knowledge–skill domain subjects taught to profession-entry master of HIM students.
The curricula are continually reviewed for currency and relevance, although the implementation of course changes is lengthy owing to mandatory approval processes (i.e. approximately 2 years for major subject changes to occur). Our courses teach to the national HIMAA graduate-entry competency standards and if any professional-based knowledge–skill domain content is amended due to industry requirements, the curriculum is changed in response.
Lead time: Course completion to employment
The current study confirmed the previous findings that HIM graduates are in demand. The high employability, based on the securement of a position before the completion of final examinations, showed an increase from 45% (cohort 1) to 51%; albeit not statistically significant, this demonstrated continuing, very strong industry demand. A converse finding that statistically significantly more cohort 2 than cohort 1 graduates did not obtain an HIM-related position within 6 months of course completion may relate to the fact that some completed studies in 2020 and 2021, during the COVID-19 pandemic and in the state that experienced the most prolonged lockdowns. This is consistent with Smallwood et al.’s (2021b: 1) findings from their late 2020 national survey of frontline Australian health workers, that “occupational disruptions during the COVID-19 pandemic occurred commonly in health organisations” including 27% of healthcare workers have changed work roles; approximately 17% of healthcare workers had experienced redeployment, a significant predictor of which was less than 5 years of work experience. It is feasible that some new graduate HIMs may have opted for a less stressful workplace than what Smallwood et al. (2021a) described elsewhere as the high-pressured healthcare environment during the pandemic. Our analysis of the roles of graduates who had not obtained an HIM-related position within 6 months of course completion included some that the researchers would identify as HIM related. If these were re-classified as such, there would be no statistically significant, intra-cohort difference in this variable.
Number of positions
Almost half of the graduates under study had worked in two or more positions since graduating, consistent with the findings for cohort 1. Correspondingly, over half of both cohorts remained in their first position at the time of the survey. Unsurprisingly, graduates from the earlier years of both study periods were more likely to have held multiple positions.
Graduates of the CPDs are typically younger than the GEM graduates. Our finding, that 75% of the graduates who had moved into a third position had completed an undergraduate degree (CDP), approximates the average national job tenure of 1 year and 3 months for workers aged under 25 years (Wilkins et al., 2021). Furthermore, the Australian Bureau of Statistics (ABS) (2022) national data on job mobility showed that between February 2019 and February 2022, 34–37% of the Australian workforce had been employed in their current role for less than 5 years. In this context, the ABS reported that the health sector had the newest entrants and the most job changes within the immediate past 12 months (i.e. the latter part of the cohort 2 study period). Our findings that (a) 60% of new graduate HIMs were aged 20–29 years, (b) half remained in their first graduate position during the study period and (c) half moved positions, demonstrated that the patterns of early career HIM workforce mobility were similar to those for the national workforce over the past decade.
Employing agencies
Most graduates worked in a public sector agency in their first position, public hospitals being the predominant employer. In comparison, new graduates were less likely to obtain a position in private hospitals. This shift was also seen in graduates’ second and third positions, which tended to be within the public setting; however, the main employer in these subsequent positions shifted from public hospitals to government departments. This suggested that graduates in both cohorts, even in their second and third roles, were largely opting to work in the public sector.
Examination of the private sector trends showed that the graduates were more likely to be employed in private hospitals than by private ICT or health insurance firms; however, only one respondent out of those in their third position was employed privately. The increase in new graduate employment in the public sector, and the corresponding decrease in the private sector, may be attributable to increased demand for HIMs in public health sector agencies such as government departments and disease registries that utilise their health classification and data analytics skills. Furthermore, HIMs could be working in extended or non-traditional roles in public hospitals; for example, on EMR projects and in decision support teams (data analytics). This would be consistent with Butler’s (2017) description of the increased specialisation, in health informatics and data analytics, of their American counterparts.
Limitations
Limitations of the study included the potential impact of the COVID-19 pandemic on the work world (e.g. interpretations of skills learned “on the job” may have been different, post-pandemic, from the era of the pre-pandemic cohort 1 survey). There was also evidence of confusion by a small number of respondents in interpreting what constituted an HIM-related role; arguably, this concerned their understanding of the profession’s specialisation and dissemination beyond the historical generalist, hospital-based roles. Finally, there was an inherent limitation concerning within-cohort uniformity (i.e. that those who graduated later in the study period had fewer opportunities, than those who completed in the earlier years, to gain comparable experience or demonstrate mobility).
Conclusion
Findings from the current study have reinforced those from the previous study by demonstrating the ongoing employability and mobility of new graduate HIMs in the health workforce. They confirm their consistent utilisation of the professional knowledge and skill set learned at university. The significant decrease in those pursuing a specialisation in health classification may be attributable to environmental and technological factors. The statistically significant increase in the recent graduate HIMs’ work roles in the areas of data analytics and health ICT informatics affirms findings and commentaries from the profession’s literature. They reflect the (a) changing context of health information management, (b) relevance of HIMAA’s profession-entry competency standards and (c) the importance to the healthcare ecosystem of HIM graduates’ professional capabilities. The findings will (a) inform future health information management curricula and (b) address a gap in knowledge of the health information management workforce. Certain findings that revealed no inter-cohort change may present opportunities for separate, future research, such as the impact of the persistent gender imbalance among new HIM graduates, and the age and educational backgrounds of the profession-entry master graduates. A follow-up study of the current (third, 2022–2026) cohort is planned for 2027.
Supplemental Material
sj-docx-1-him-10.1177_18333583231197936 – Supplemental material for Workforce survey of Australian health information management graduates, 2017–2021: A 5-year follow-on study
Supplemental material, sj-docx-1-him-10.1177_18333583231197936 for Workforce survey of Australian health information management graduates, 2017–2021: A 5-year follow-on study by Stephanie Gjorgioski, Merilyn Riley, Jenn Lee, Natasha Prasad, Melanie Tassos, Abbey Nexhip, Sally Richardson and Kerin Robinson in Health Information Management Journal
Footnotes
Appendix
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.