
Abstract
Background:
Professional practice placements (work-integrated learning (WIL)) enable practical application of essential knowledge and skills, from the health information management university curricula, aligned to profession entry-level competencies.
Objectives:
To (1) identify formal (explicit learning outcomes (ELOs)) and informal (derived learning outcomes (DLOs)) articulated in final-year, health information management WIL proposals, 2012–2021, at Australia’s La Trobe University; and (2) map these to the contemporaneous, national Health Information Manager (HIM) profession entry-level competency (sub-)domains.
Method:
A random sample (20%; n = 129) of 2012–2021 final-year placement proposals was interrogated using documentary analysis. ELOs and DLOs were extracted and categorised to the (sub-)domains of the Health Information Management Association of Australia’s (2017) HIM Professional Competency Standards; between-group comparisons were made.
Results:
Of the 129 proposals: 38 (29.5%) were absent ELOs; one had no project description; almost 74% were project-related. Predominant sub-domains in Domain A, “Generic professional skills”: communication (in 63.7% of ELOs; 61.2% of DLOs); teamwork (40.7% ELOs; 50.8% DLOs). Predominant sub-domains in the eight profession-specific competency domains: “Health information services organisation and management” (Domain I; 60.5% ELOs; 100% DLOs); “Health information and records management” (Domain B; 54.9% ELOs; 56.3% DLOs); “Research methods” (Domain E; 45.1% ELOs; 44.5% DLOs). ELOs were most commonly aligned to four discipline-specific domains; DLOs were distributed across five.
Conclusion:
Analysis of the knowledge-skills learning outcomes for final-year, student-HIM placements has generated recommendations to support agency supervisors in framing WIL project proposals.
Implications for health information management practice:
This research will support more robust WIL to complement student HIMs’ academic education for competent, postgraduation practice.
Keywords
Introduction
This is the second article reporting research on the work-integrated learning (WIL; professional practice) of final-year students in two health information manager (HIM) qualifying degree programs in Australia, following from Robinson et al. (2024). WIL is a tripartite approach to education that involves the student, the university and an external stakeholder (professional practice placement agency/organisation; Zegwaard et al., 2023). WIL comprises “authentic work-focused experiences as an intentional component of the curriculum” (Zegwaard et al., 2023: 38) and is a cornerstone of many university programs. Relating academic learning to practical, real-world experiences, it fosters in students the discipline-specific and transferable skills and competencies required by employers of career-ready graduates (Jackson and Cook, 2023) and is essential for navigating the modern work climate (Universities Australia, 2019). In the last 2 decades, universities have increasingly prioritised WIL to address the growing emphasis on employability (Small et al., 2018) and the demand for graduates who possess relevant competencies and skills (Sistermans, 2020).
Professional competencies: Guiding the curriculum
The clinical and other health disciplines’ placements are a key form of WIL. Grounded in experiential learning theory, they have long been integral to health profession-related university curricula (McCarthy, 2010; Robinson et al., 2020). This experiential learning process contributes to the development of key competencies needed for success in the workplace. The definition of competency, tendered by Frank et al. (2010b) in the context of medical education, arguably applies to the education of HIMs and other health professionals: An observable ability of a health professional, integrating multiple components such as knowledge, skills, values and attitudes. Since competencies are observable, they can be measured and assessed to ensure their acquisition. Competencies can be assembled like building blocks to facilitate progressive development. (Frank et al., 2010b: 641)
Discipline-specific competencies represent disciplinary expertise. “Generic” professional competencies, also known as “transferrable,” “employability” or “basic’ skills” (Caballero et al., 2011: 42), reflect broader, universal attributes and skills that facilitate meaningful interactions with people and technologies. Both discipline-specific and generic competencies are crucial to becoming a well-rounded healthcare professional (Van Der Vleuten, 2015), and it is essential that they are developed throughout a student’s education (Janssens et al., 2024). Competencies can be taught to students via competency-based education which, supported by WIL, emphasises the integration of knowledge, skills and attitudes in a specific context (Carraccio et al., 2016). The development of a competency-based curriculum begins with determining (a) the competencies required of the student at the end of the course and (b) how the student must demonstrate achievement of the required competencies, for example, by meeting pre-determined standards or benchmarks (Albanese et al., 2010; Frank et al., 2010b; Gruppen et al., 2012; Sistermans, 2020). The curriculum designers and academics work “backward” (Sistermans, 2020: 688) from the competency standards to design the curriculum. Curriculum content is therefore oriented to and driven by “graduate outcome abilities and organised around competencies” (Frank et al., 2010a: 636) derived from analysis of the needs of critical stakeholders. In the case of HIMs, the key stakeholders are society, patients, the members of the profession of health information management, and the healthcare sector including its government, private sector, clinician, employer and funding components. The focus on outcomes rather than chronological progression ensures that students meet their academic requirements and acquire the specialist expertise necessary to practice competently, post-graduation.
The profession’s competency standards
The health information management degree programs at La Trobe University (LTU), Australia, are designed to meet the Health Information Management Association of Australia’s (HIMAA’s) HIM professional competency standards at profession-entry level (see Box 1). The standards define the capabilities of the profession, specifically its knowledge, skills and ethical and professional practices. The model is a comprehensive, whole-of-career competency framework for HIMs that addresses the profession’s essential domains and sub-domains of knowledge. The matrix of domains (and their sub-domains) incorporates three, core sub-sets of competency standards that differentiate and articulate the key stages of professional maturity in HIMs’ life-long learning:
(a) Profession-entry competency standards: (i) Inform the HIM-qualifying university degree curricula, (ii) define the entry-level competencies required for graduates as they commence their professional careers and (iii) provide the benchmark for external course accreditation (by HIMAA) to ensure that these specialist university degrees are suitably rigorous, qualifying programs for HIMs.
(b) Intermediate level competency standards: (i) Guide individual HIMs’ professional development and (ii) inform employer and workplace/role-related expectations of qualified, experienced HIMs’ capabilities and knowledge.
(c) Advanced level competency standards: Relate to highly experienced or highly specialised HIMs and used for the same purposes as in (b), above.
HIM professional competency standards domains and sub-domains.*
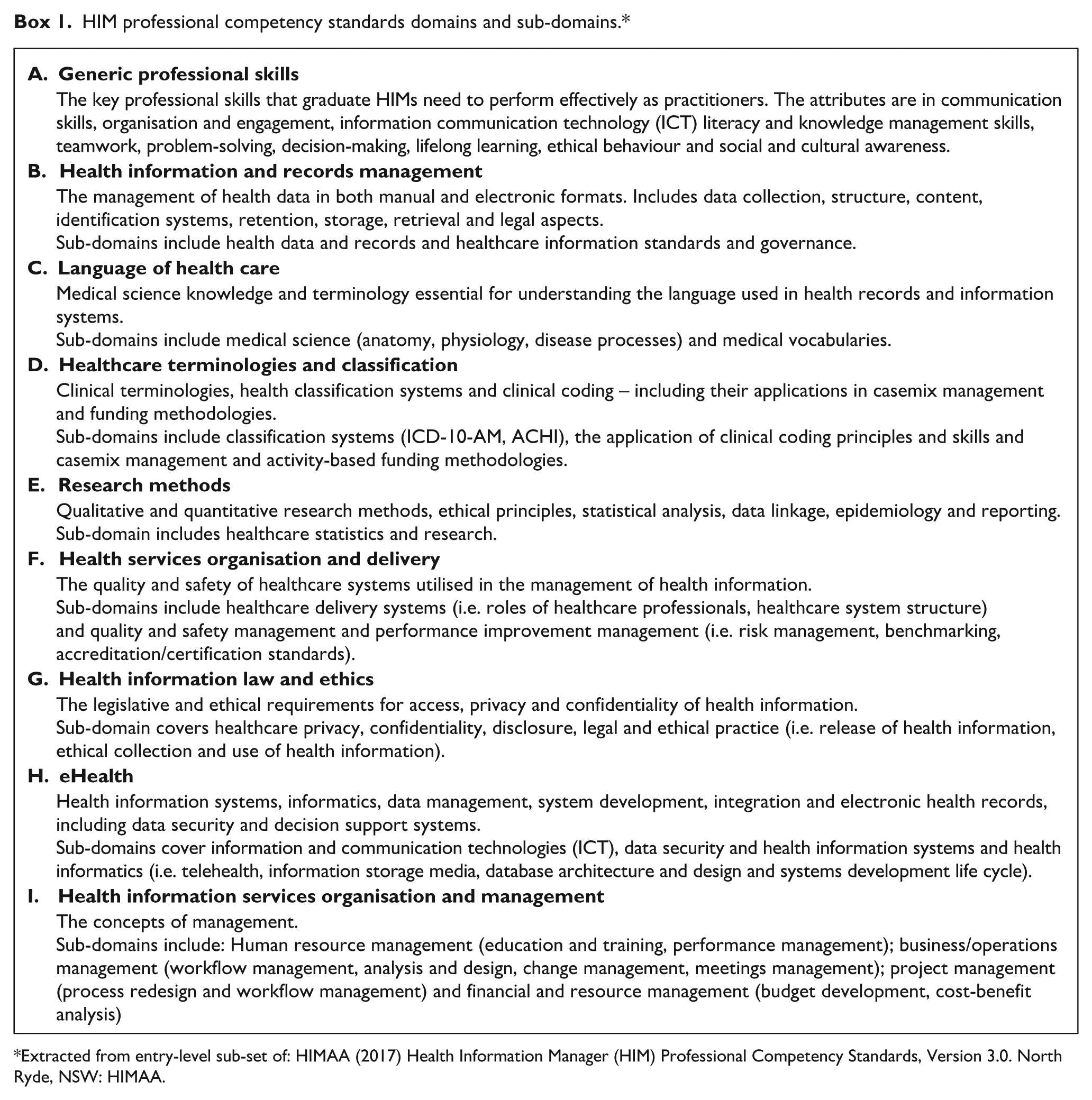
Extracted from entry-level sub-set of: HIMAA (2017) Health Information Manager (HIM) Professional Competency Standards, Version 3.0. North Ryde, NSW: HIMAA.
The 2017 version of the standards has been applied to the current research. It constituted one domain that incorporated eight sub-domains of “generic” (universal) skills, and eight domains of discipline-specific knowledge and skills that incorporated 17 sub-domains. Collectively, the sub-domains held 127 competency standards at each competency level (Entry, Intermediate and Advanced).
The WIL program
LTU offers profession-entry health information management degrees at both undergraduate and master’s levels. All students complete their introductory WIL in the health information services (HISs) of metropolitan and regional hospitals. The final-year WIL framework allows students to undertake placement at any healthcare agency, organisation or service (hereinafter, “agency”) across the whole-of-health including, but not limited to, public and private hospitals, government departments, clinical quality registries, medical research centres, health information and communication technology (ICT) companies, health insurance funds, and primary healthcare facilities (Robinson et al., 2024). The intentional exposure of students to real-life, contextually varied health information management environments from throughout the healthcare sector provides scaffolding to assist them in consolidating knowledge learned at university and in building upon a range of skills. Critically, students can apply their knowledge within a supervised setting in a real-world context to demonstrate their competence, by the conclusion of the placement, as workforce-ready, entry-level HIMs.
Several months prior to each final-year placement, university staff initiate contact with agencies to source the placements. Agencies assess their capacity to host a placement and confirm this by submitting a placement proposal (hereinafter, “proposal”) to the university. The proposal is the key document that outlines the agency’s profile and services, describes the project and activities in which the student will be involved, and specifies the intended learning outcomes. The proposal details the requisite skills and knowledge areas, and the meaningful opportunities with which the student will engage during the placement. It is a blueprint for how they may develop and demonstrate the competencies required for professional practice.
Aims
This research was part of a larger study that aimed to evaluate LTU’s health information management professional practice placement program and identify evidence to inform best practice guidelines for project-based, WIL placements. The categories, locales and foci of the 2012–2021, final-year (capstone) placements have been reported elsewhere (Robinson et al., 2024). The objectives of this component of the study were to:
Identify the formal (explicit) learning outcomes and skills articulated in final-year health information management placement proposals, 2012–2021, and map these to the contemporaneous, national HIM profession-entry competency (sub-)domains.
Identify and extract informal (derived) learning outcomes or opportunities from the body of the placement proposals and map these to the contemporaneous, national HIM profession entry-level competency (sub-)domains.
Method
Study design
This study involved the examination of LTU’s final-year, 2012–2021 professional practice placement proposals. A qualitative method, documentary analysis, was employed (Bowen, 2009; Gorsky and Mold, 2019; Dalglish et al., 2020; Morgan, 2021). The study design and methods were described by Robinson et al. (2024).
Sample
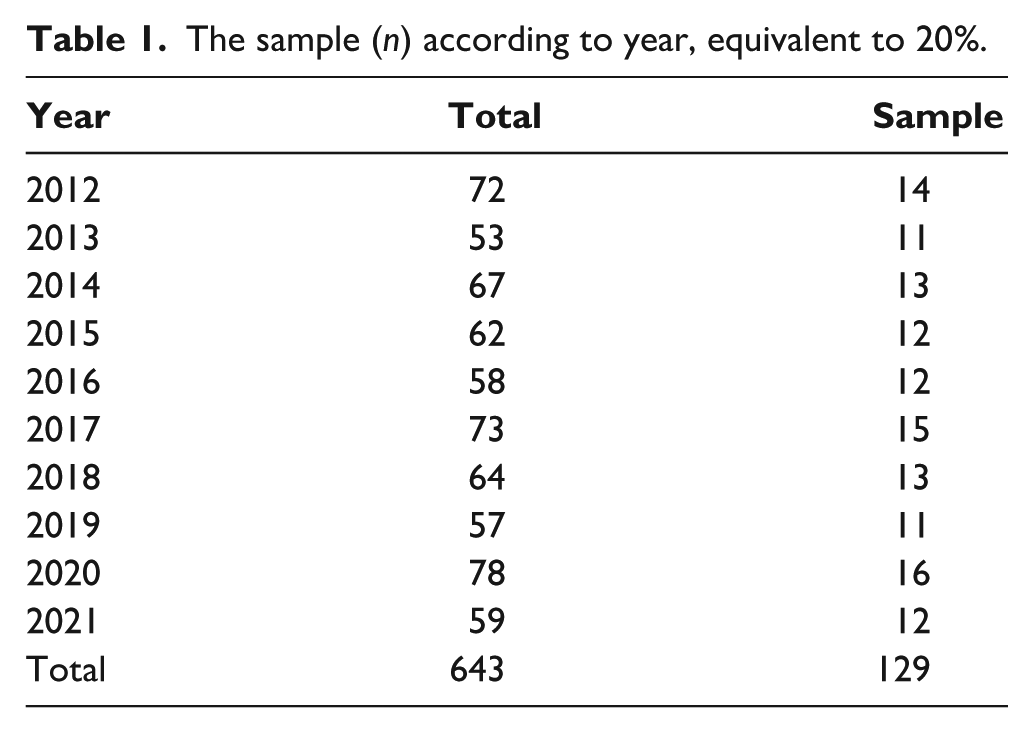
A total of 643 final-year proposals were received by the University from prospective placement agencies during the study period, 2012–2021, inclusive. Using the 2019 sub-set of proposals as a sample year, explicit learning outcomes (ELOs) were mapped against the domains and sub-domains of the entry-level sub-set of the HIMAA HIM Professional Competency Standards (HIMAA, 2017; Prasad et al., 2023). This process was also separately completed for the learning outcomes derived from the proposal description itself. The comprehensive mapping of all 2019 proposals yielded valuable insights into mapping processes, informed the mapping rules and justified the decision to include a sampling strategy to manage the large volume of data and extensive time required to analyse and map the proposals. A stratified random sample was selected, comprising 20% (n = 129) of the proposals submitted between 2012 and 2021. The sample size for each year was calculated proportionally using Microsoft Excel, based on the total number of proposals for each year. The random sample was then generated using the RANDARRAY function in Excel.
Data collection tool
Data were extracted from the sample of proposals and entered into a mapping document via Microsoft Excel, to capture the following elements.
Researcher ID: Identifying the research team member responsible for mapping.
Proposal ID: A unique identifier indicating the year and proposal number (e.g., 2017.15).
Source of data: Indicating whether the data were extracted from the ELOs or abstracted from the proposal description (derived learning outcomes (DLOs)); these elements were analysed separately.
Competency domain and sub-domain: Classification according to the HIMAA (2017) HIM profession entry-level competency standards.
Data extraction procedure
Two researchers (NP and AN) separately and independently undertook the data extraction which involved reviewing each proposal and extracting (a) the ELOs and (b) the DLOs. All learning outcomes (explicit and derived) were categorised according to the domains and sub-domains of the HIMAA (2017) HIM Professional Competency Standards (entry-level; summarised in Box 1) and entered into an Excel mapping document. There were no restrictions on the number of domains or sub-domains into which extracted data could be categorised. For example, a learning outcome that aligned with both the “medical science” and “clinical coding” sub-domains was categorised to both. This ensured that multi-faceted, explicit and DLOs were captured accurately. An example of the data extraction logic process is shown in Appendix A. The full research team progressively reviewed the data and resolved queries.
The 2017 version of the competency standards was used for this study because it was relevant for much of the study period and, particularly, because it bore close similarity to the previous, 2013, version (HIMAA, 2013, 2017). The most recent, 2023, version, which contains slightly compressed generic standards, more explicit data analytics standards and a professional practice standard addressing WIL, was not current for the study timeframe (HIMAA, 2023). An additional “other” category was included in the analytical process to capture data items that were not readily categorised into a domain or sub-domain of the competency standards, that is, did not reflect a health information management profession-specific competency.
Quality control
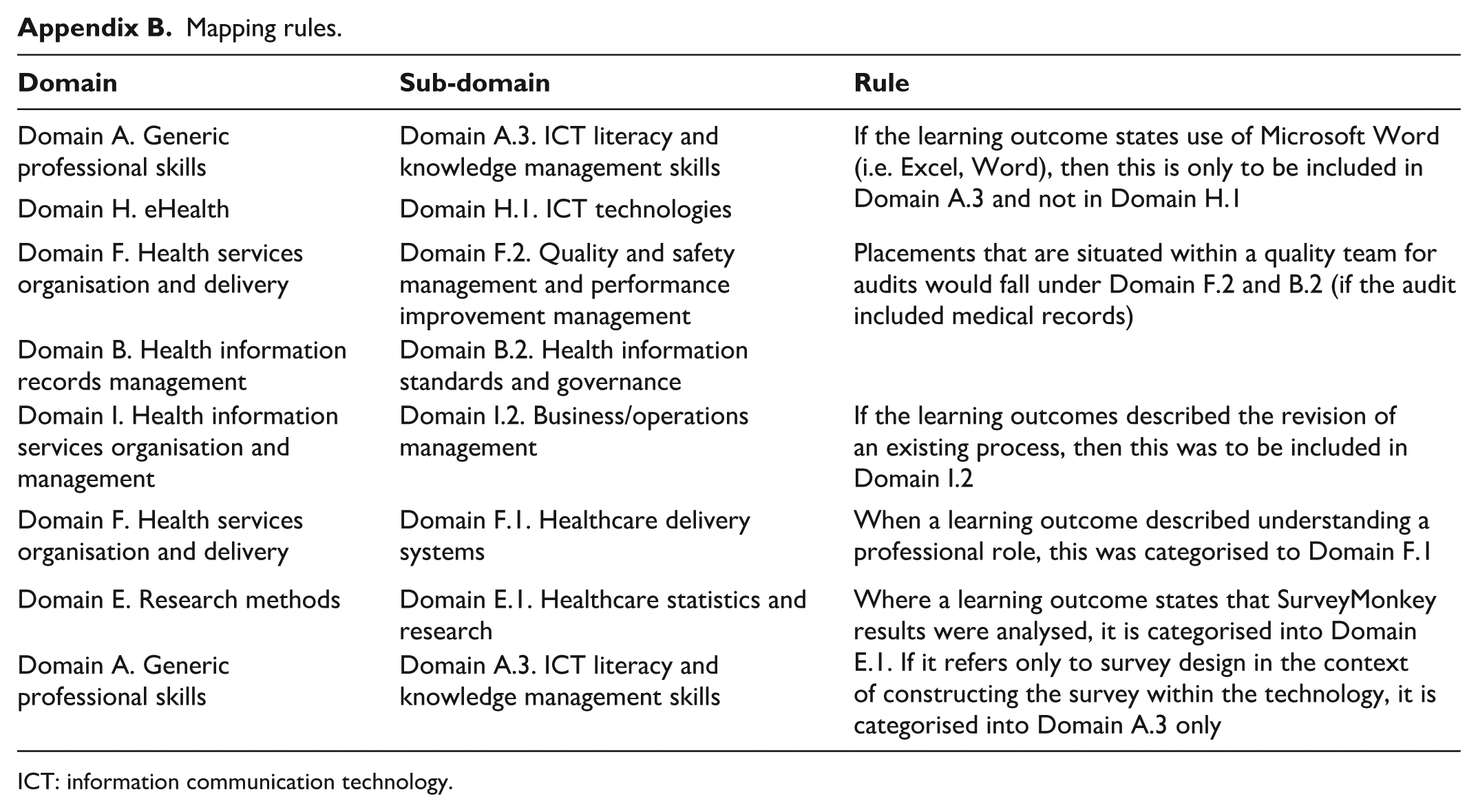
In order to minimise subjective bias, a set of mapping rules was developed iteratively (NP and AN) and reviewed, modified as necessary, and approved by the full research team (NP, AN, MR and KR; Appendix B). To ensure consistency, interpretive discrepancies that were irresolvable at the regular two-researcher (NP and AN) meetings were escalated to the full research team for further discussion and remediation. Some discrepancies necessitated reference to the HIMAA (2017) HIM profession entry-level competency standards, which contained further (sub-)domain-related contextual information.
Data analysis
Descriptive statistics were utilised to determine the proportions of explicit and DLOs that were mapped to each domain and sub-domain of the competency standards. Generic professional skills (Domain A) were analysed separately from the profession’s discipline-specific skills (Domains B–I). Statistically significant differences between ELOs and DLOs were calculated using Chi-square and p-values via MedCalc Software Ltd. (2025).
Ethics approval
The LTU Human Research Ethics Committee approved this study (HEC22060).
Results
The 20% stratified random sample, drawn from proposals from each year in the 2012 to 2021 timeframe, resulted in 129 proposals selected for analysis from the population of 643 proposals (Table 1). Almost 30% (n = 38/129) of the sample proposals were absent formal (explicitly) recorded learning outcomes and one proposal had no project description. Almost 74% (n = 95/129) of the sample comprised project-related proposals (Table 2). This compared to almost 65% of the population of proposals which were project-focused, indicating that project-based placements were slightly over-represented in the sample (Table 2). Within the sample, the highest proportion of projects related to a hospital HIS (n = 37/129, 28.7%), followed by “other” (n = 32/129, 24.8%) projects related to clinical quality registries or health/disease screening services. More of the internship placements were related to “other” placement categories (e.g. government departments) than to hospital HISs.
The sample (n) according to year, equivalent to 20%.
All placement categories (internship, project-based, research-based, other) in the sample, by year, 2012–2021.
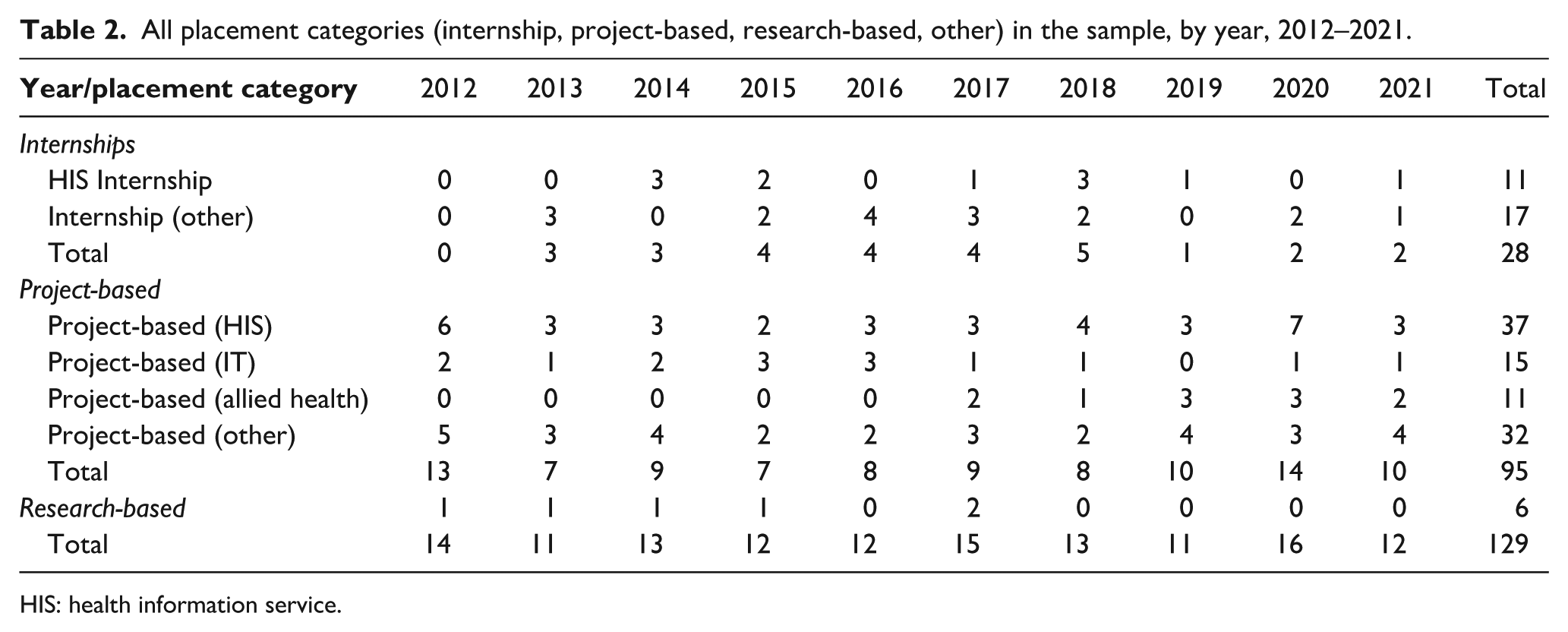
HIS: health information service.
Table 3 outlines the proportion of each HIMAA competency standard domain and sub-domain addressed in the ELOs and DLOs. Among the eight sub-domains of Domain A (Generic professional skills), there were statistically significantly more ELOs than DLOs related to the sub-domains “Organisation and engagement” (Χ2 = 5.9, p = 0.015) and “ICT literacy and knowledge management skills” (Χ2 = 4.1, p = 0.042). There were no sub-domains within the “Generic professional skills” that were reported statistically significantly more in DLOs than ELOs.
Number and proportion of derived (DLOs) and explicit (ELOs) learning outcomes mapped to HIMAA HIM profession-entry level competency domains A–I, 2012–2021.
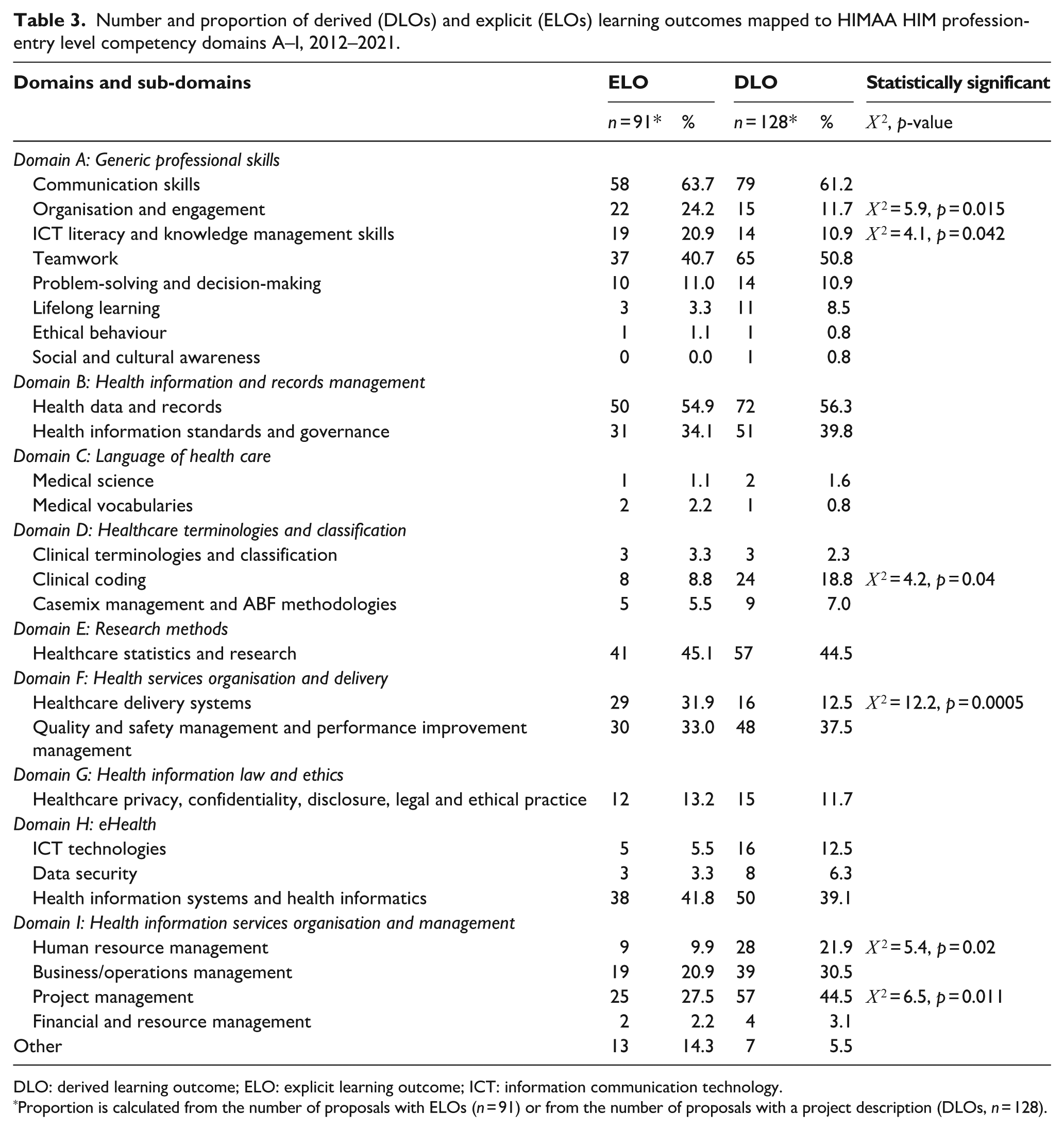
DLO: derived learning outcome; ELO: explicit learning outcome; ICT: information communication technology.
Proportion is calculated from the number of proposals with ELOs (n = 91) or from the number of proposals with a project description (DLOs, n = 128).
Overall, approximately 64% (n = 58/91) of proposals that contained ELOs included communication skills (written and verbal), making it the most commonly reported generic professional skill. This correlated with the DLOs, where 61.2% (n = 79/128) of project descriptions also highlighted communication skills as the most common generic professional learning outcome. The second most common generic professional learning outcome represented in both explicit and derived outcomes was teamwork (40.7% (ELOs) and 50.8% (DLOs)). There was negligible representation of the competency standards for ethical behaviour or social or cultural awareness in either explicit or DLOs.
Profession-specific competency domains
In relation to the discipline-specific domains of knowledge as articulated in the HIMAA competency standards, the most commonly occurring domain represented in the 91 ELOs was “Health information and records management” (n = 81) followed by “Health services organisation and delivery” (n = 59) and “HISs organisation and management” (n = 55). With DLOs, both “Health information and records management” and “HISs organisation and management” domains had approximately the same number of knowledge-standard sub-domains identified (n = 123 and n = 128, respectively).
Profession-specific competency sub-domains
The most frequently identified knowledge-standard sub-domain addressed by both ELOs and DLOs was “Health data and records” (a component of the “Health information and records management” domain), represented in 54.9% of ELOs and 56.3% of DLOs. The second most common discipline-specific sub-domain addressed by both ELOs and DLOs was “Healthcare statistics and research,” which showed similar results of 45.1% (ELOs) and 44.5% (DLOs). The third most commonly occurring sub-domain in the ELOs was “Health information systems and health informatics” (n = 38; 41.8%) which was part of the “eHealth” domain. “Project management,” part of the “HISs organisation and management” domain, was the third most frequently represented sub-domain in the DLOs (n = 57; 44.5%).
Review of all learning outcomes mapped to the competency standards revealed that there were almost 50% (48.5%) more DLOs (n = 707) than ELOs (n = 476; Table 4); these statistics exclude learning outcomes that were mapped to the “other” category. Table 4 shows that the proportion of generic professional skills (Domain A) were reflected similarly in the ELOs and DLOs: 32.4% and 28.6%, respectively. These results were independent of whether the person completing the abstraction of the outcomes was informed about the study aims (i.e. the researchers) or were agency supervisors who completed the proposals well before this research commenced.
Number and proportion of derived (DLOs) and explicit (ELOs) learning outcomes by “generic” (Domain A) and discipline-specific (Domains B–I) knowledge-skills, 2012–2021.
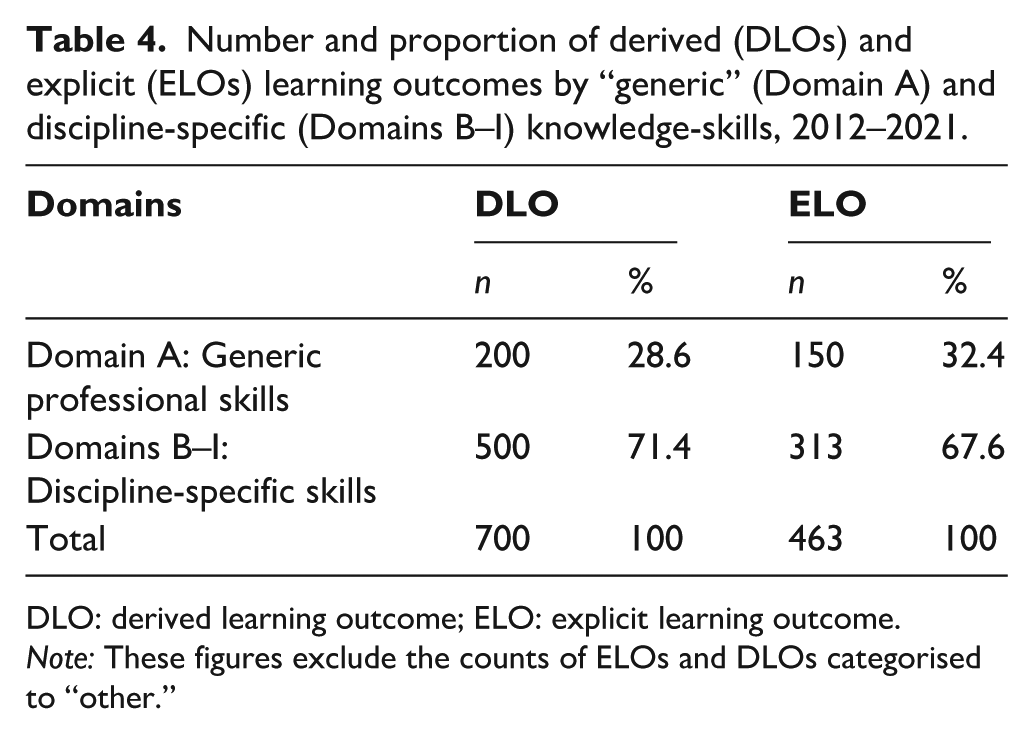
DLO: derived learning outcome; ELO: explicit learning outcome.
Note: These figures exclude the counts of ELOs and DLOs categorised to “other.”
Figure 1 shows the frequency of domains incorporated in individual proposals, categorised by ELOs, DLOs or both combined. The most competency domains (A–I) addressed by any single placement was seven, derived from the project descriptions in two proposals (1.6% of DLOs). The most commonly occurring number of HIM competency domains addressed by individual proposals that contained ELOs was four (22.5%), followed closely by three domains (20.2%). The most common number of HIM competency domains addressed by individual proposals that contained DLOs was also four (33.3%), followed by three domains (24.8%). However, the combined proportion of proposals with four or five domains for ELOs was 35.7%, compared to 55.8% of DLOs. When learning outcomes from either ELOs and/or DLOs were examined, the most common proportion of domains addressed in individual proposals was five (31.8%).
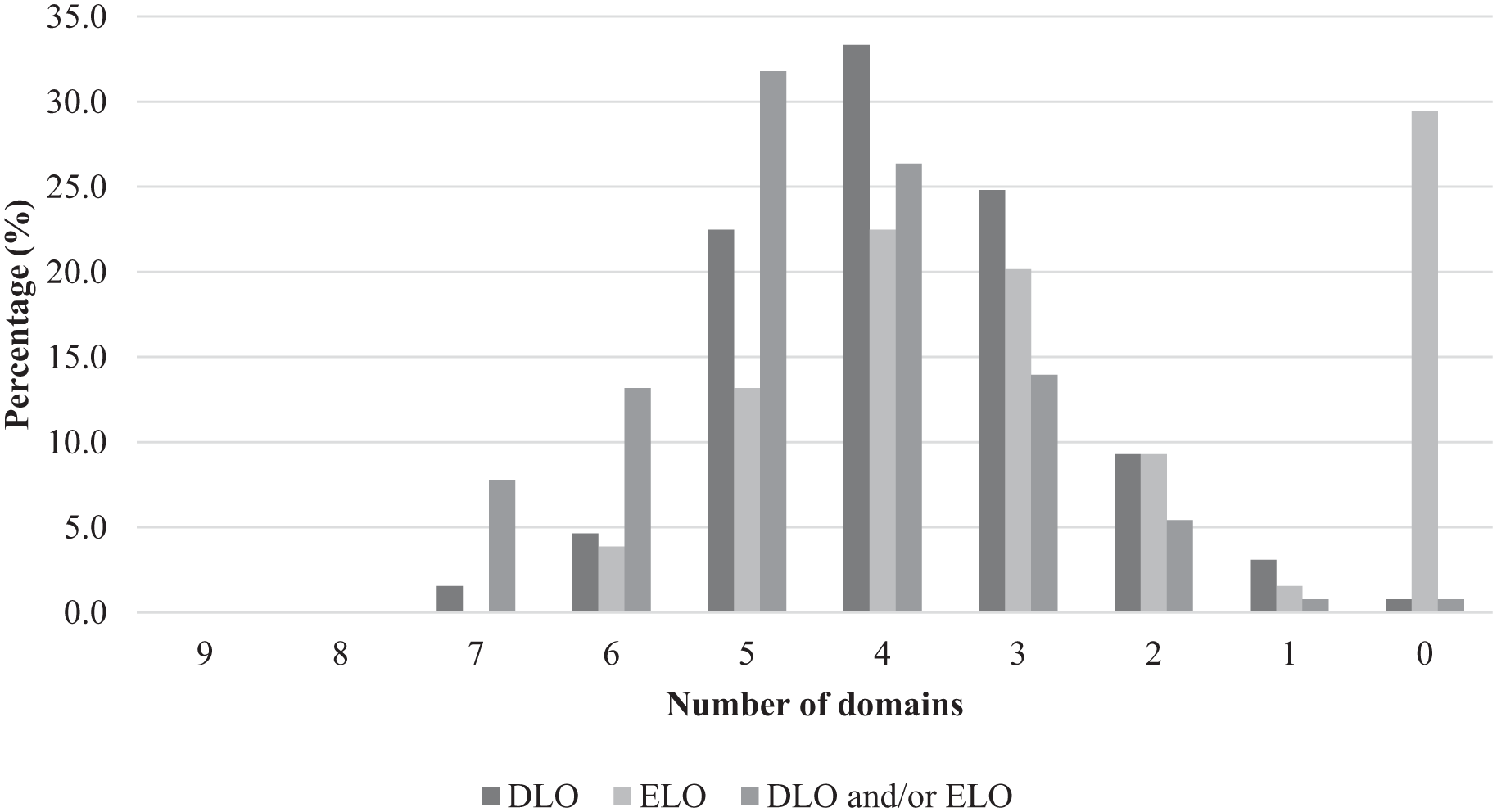
Percentage of proposals (derived and explicit learning outcomes) mapped against number of HIMAA competency domains (A–I) met.
Discussion
The component of the study reported herein aimed to examine final-year, HIM student WIL proposals and identify the learning outcomes explicitly stated by the placement agencies and those derived by the researchers from the project description, and subsequently, to map these to the knowledge-skills domains of HIMAA’s HIM professional competency standards at profession-entry level. This analysis has enabled us to (a) identify the most frequently occurring generic professional skills learning outcomes (Domain A), and discipline-specific skills learning outcomes (Domains B–I) and (b) develop recommendations to support agency supervisors in their future development of WIL project proposals.
By their nature and generality, the generic competencies are necessary adjuncts to the specialist HIM professional competencies. They support graduate HIMs’ multifaceted human and technological communications and facilitate their actioning and leverage of their specialist professional knowledge. As might be expected in a professional degree program, they constitute a relatively small component (single domain) of the body of HIM graduate competencies; however, this domain appears to be over-represented by volume of standards when compared to the profession-specific domains.
The generic skills and attributes required for new graduates’ work-readiness have been widely researched (Orr et al., 2023). For example, only 6 of the 16 in-scope studies in Orr et al.’s (2023) systematic review of work-readiness related articles referred to discipline-specific competencies along with generic professional skills, while all 16 studies referred to generic professional skills such as communication. None of these studies focussed only on discipline-specific competencies. Orr et al. (2023: 1714) confirmed that most studies adopted a “multi-dimensional approach [to conceptualising work-readiness], comprising discipline-specific and generic skills.” This supports the approach taken by our study.
Caballero et al. (2011) developed a “work-readiness scale (WRS)”; however, Walker et al. (2015) reported that nursing clinicians needed to adapt the scale with nursing-specific items to ensure its usability in evaluating graduate nurses’ work-readiness. An adaptation of the WRS was also made to assess the work-readiness of pharmacy students in the Kingdom of Saudi Arabia (Almarzoky Abuhussain et al., 2021). These adaptations highlight the limitations of using generic skill frameworks alone and underscore the importance of discipline-specific competencies in evaluating work-readiness.
The profession’s discipline-specific competency standards were reflected overwhelmingly more in the DLOs, abstracted by the researchers, than in the ELOs completed by agency supervisors. The over-representation of the generic standards was arguably associated with agency supervisors’ reasonable expectation that final-year students would commence their last WIL placement having acquired virtually full knowledge of the academic curriculum (e.g. relevant legislation, data reporting requirements, classification standards, database design, health records management best practice, etcetera). The emphasis in the ELOs and DLOs on generic competency standards reflects one of the key purposes of WIL, specifically to facilitate students’ professional practice in a real-world environment which inevitably demands demonstration of effective verbal and written communications, teamwork and other skills required in professional workplaces.
In our research on HIM competencies, the representation of competency domains in the proposals under study (including both generic and profession-specific) supports Gjorgioski et al.’s (2023) conclusions that most new graduate HIMs (64.1%) utilised, in their workplace, 75% or more of the overarching professional knowledge–skill domains described in that research as health classification, health data analytics, health informatics, and health information management. Results from Gjorgioski et al. (2023), and the current study have demonstrated that new graduates and final-year WIL students, respectively, are expected to utilise a very substantial component of the knowledge-skills acquired in the HIMs’ academic curriculum.
In our study, the most commonly occurring discipline-specific learning outcome for both ELOs and DLOs was mapped to the “Health data and records” sub-domain. Competency in this and other specialist discipline-specific knowledge for all graduates is the cornerstone of the profession; hence, the long-standing professional identity as HIMs. This resonates with findings of Australian-based workforce studies (Gjorgioski et al., 2023; Riley et al., 2020) which demonstrated that “HIM” was the most frequent title of first positions occupied by new graduate HIMs, reflecting their expected expertise in the health information science and other specialty areas within health records and health data and information management.
The importance of the second most common sub-domain identified in our project proposals, “Healthcare statistics and research,” is also unsurprising. The role of health data analytics skills (mapped to this domain in the 2017 HIMAA professional competency standards) was shown by Gjorgioski et al. (2023) to increase in the proportion of HIM graduates from the 2017 to 2021 LTU cohorts undertaking data management and analytics roles, when compared to the 2012–2016 graduate cohorts. The importance of this work has been recognised by HIMAA via inclusion of a separate domain in the most recent version of its professional competency standards (HIMAA, 2023): the “Health data analytics” domain includes emerging skills and some pre-existing competencies.
The third most prevalent sub-domain reflected in the ELOs, “Health information systems and health informatics,” is indicative of HIMs’ implementation and management of diverse medical record technologies including electronic medical records (Bonello et al., 2021). The fourth most prevalent sub-domain of “Project management,” significantly represented in the DLOs, suggests a growing emphasis on preparing students to lead or contribute to various project initiatives. This reflects the focus of our intent for final-year placements to characterise project models as opposed to internships. Therefore, generic project management skills, including strategic planning, stakeholder collaboration and critical thinking, are an essential requirement in final-year placements.
Analysis of the narrative content revealed a clear distinction between the number of HIM discipline-specific skills and generic professional skills explicitly stated in or derived from the proposals. Robinson et al. (2024) reported that strong abilities in the generic competencies of autonomy, communication skills, teamwork, self-motivation and organisational and time management skills were expected by agency supervisors of these same cohorts of final-year WIL students.
Variability of competency demonstration
Final-year health information management students have the opportunity to demonstrate a range of competencies, to varying extents, during their formal WIL experiences. Variability in placement agencies’ requirements for competency demonstration can be influenced by factors such as the complexity of the tasks assigned, the student’s experience and professional knowledge maturity, and the WIL environment. Therefore, it is important for universities and placement agencies to consider these variations when assessing student performance. It is also necessary to ensure that placement projects are structured to allow students to develop and demonstrate a broad spectrum of competencies to the greatest extent possible. While it may appear that a small number of proposals lacked sufficient coverage of competencies for final-year student learning outcomes and work-readiness (e.g. three or less domains), it is probable that agency supervisors assumed the presence of certain knowledge and skills and, therefore, did not see the need to designate them in the ELOs or project descriptions. For example, Domains C and G, “Language of medicine and health care” and “Health information law and ethics,” respectively, represent fundamental skills of HIMs and are usually assumed prior knowledge of final-year students undertaking placement. For this reason, agency supervisors might not consider the need to incorporate them as learning outcomes. This reasoning may also be applied to other sub-domains.
Limitations
This study faced limitations concerning data completeness and interpretation. The dynamic nature of placements suggests that actual student experiences may have deviated in some way from what was described in the proposals. Furthermore, early-year proposals (2012–2013) were less likely to include ELOs, thereby limiting comparative analysis across time. There is also inherent subjectivity in extracting learning outcomes from project descriptions, and no additional validation was undertaken to compare ELOs with what might have been expected based on the project descriptions. To mitigate these effects, harmonisation of between-reviewer differences was undertaken. Another limitation was that the higher proportion of DLOs with more domains covered in their content may have reflected the researchers’ familiarity with creating learning outcomes, compared to that of the agency supervisors. In some instances, the proposal description could be clearly mapped to a specific HIM competency domain (DLOs), but the associated learning outcomes (ELOs) did not align with the competencies in that domain – or vice versa. These discrepancies likely arose because the learning outcomes did not fully reflect or support the content of the proposal description, resulting in the ELOs and DLOs not necessarily being complementary within the proposal.
Recommendations
Our findings support the following recommendations.
That universities should actively educate and support placement agencies in the creation of students’ WIL learning outcomes.
That agency supervisors should be encouraged to prioritise the inclusion of discipline-specific skills and knowledge in final-year WIL outcomes.
That agencies should be guided to refer to the contemporaneous HIMAA HIM professional competency standards when designing final-year placement projects and framing proposals, ensuring that the substance of the project aligns with competencies expected of graduate HIMs upon entry to the professional workforce.
That further investigation is warranted on the structures that optimally support the “project management” experiences in student HIMs’ WIL.
Conclusion
Findings from this research will provide valuable guidance to healthcare agency supervisors in crafting well-structured, focused project proposals for final-year health information management students’ WIL. Improved proposals containing more targeted learning outcomes will better support students’ demonstration of the application of core HIM knowledge domains and skillsets in real-world settings. The findings will also inform the intentional formulation and delivery of professional practice programs in the health information management, professional degree curricula. This research will contribute to the development of more robust and effective WIL which will support the academic education of student HIMs in their journey to graduate, fully equipped, to meet the demands of the healthcare industry.
Footnotes
Appendix
Mapping rules.
|
|
|
|
|---|---|---|
| Domain A. Generic professional skills | Domain A.3. ICT literacy and knowledge management skills | If the learning outcome states use of Microsoft Word (i.e. Excel, Word), then this is only to be included in Domain A.3 and not in Domain H.1 |
| Domain H. eHealth | Domain H.1. ICT technologies | |
| Domain F. Health services organisation and delivery | Domain F.2. Quality and safety management and performance improvement management | Placements that are situated within a quality team for audits would fall under Domain F.2 and B.2 (if the audit included medical records) |
| Domain B. Health information records management | Domain B.2. Health information standards and governance | |
| Domain I. Health information services organisation and management | Domain I.2. Business/operations management | If the learning outcomes described the revision of an existing process, then this was to be included in Domain I.2 |
| Domain F. Health services organisation and delivery | Domain F.1. Healthcare delivery systems | When a learning outcome described understanding a professional role, this was categorised to Domain F.1 |
| Domain E. Research methods | Domain E.1. Healthcare statistics and research | Where a learning outcome states that SurveyMonkey results were analysed, it is categorised into Domain E.1. If it refers only to survey design in the context of constructing the survey within the technology, it is categorised into Domain A.3 only |
| Domain A. Generic professional skills | Domain A.3. ICT literacy and knowledge management skills |
ICT: information communication technology.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.