
Abstract
Introduction
Many educational disciplines, especially in health professions and clinical programs, must include informatics in their curricula as required by best practices and accreditation standards (Bichel-Findlay et al., 2023; Giddens and Mansfield, 2023; Lobach, 2004). With an ever-increasing volume of digital patient data, education programs (known in some countries as ‘courses’) in the health professions must embrace the use of health informatics (HI) to prepare graduates for busy practice environments where data from multiple sources must be quickly and efficiently synthesised (Cutrer et al., 2021).
In the United States, physical therapy (PT) education programs are accredited by the Commission on Accreditation in Physical Therapy Education (CAPTE). CPATE’s Standards and Required Elements for Accreditation of Physical Therapist Education Programs (CAPTE, 2020) include section 7D40 which simply requires programs to ‘Use health informatics in the health care environment’. A footnote on the page adds: As defined by the US National Library of Medicine, health informatics is the interdisciplinary study of the design, development, adoption, and application of IT-based innovations in healthcare services delivery, management, and planning. Medical Informatics, physician, HealthIT. Jan 7, 2014. (CAPTE, 2020: 32)
A 2023 draft incorporating proposed updates to the CAPTE standards retains the same requirement to ‘Use health informatics in the healthcare environment’ (CAPTE 2023b: 32). However, this newer version, renumbered to 7D19, includes a separate glossary with the following slightly expanded definition: Health informatics: the interdisciplinary study of the design, development, adoption, and application of IT-based innovations in health care services delivery, management, and planning. For the purpose of these standards, health informatics relates to using health information to make clinical decisions. It is not related to electronic medical records or electronic documentation. (CAPTE, 2023b: 4)
The draft definition indicates CAPTE does not consider the use of an electronic heath record system alone to meet the HI curriculum requirement. This definition also emphasises the need to utilise HI in clinical decision making, which includes various aspects of patient care (e.g. intervention, safety, quality, cost). Both definitions allow for a broad range of activities incorporating health information technology to achieve compliance with the standard. However, an excessively broad scope can result in uncertainty as to what should or could be included in PT curricula.
This study was inspired by a routine internal reaccreditation curriculum review of a 3-year entry-level Doctor of Physical Therapy (DPT) program at a large public university in the United States (the term ‘course’ may be more appropriate than ‘program’ in some countries). The Department’s review process revealed the need to educate faculty (academic staff) about the CAPTE-adopted definition of HI and to more deeply examine where and how this content was incorporated. It was anticipated that HI content had been taught in several courses (the term ‘subject’ may be more appropriate than ‘course’ in some countries), but faculty had not recognised the content as meeting HI standards or not fully represented the content in syllabus student learning objectives (SLOs). Just as in physiotherapy education, the primary focus of most healthcare faculty is the complex clinical interaction that must be applied in the treatment of patients (Pain et al., 2017) with the use of informatics being secondary, yet required. However, with increasing dependency on digital information and technology in health care, it is vital that faculty identify HI content so that students recognise when and how it should be used in clinical decision making (Wilkerson et al., 2010).
The aim of this project was to explore how the target DPT program, having recently and successfully achieved CAPTE reaccreditation, could more accurately represent compliance with HI accreditation requirements by identifying hidden instances of this content within the curriculum. To achieve this aim, one faculty researcher from PT who was extensively involved in the Department’s reaccreditation recruited two faculty researchers from the health information management (HIM) department for assistance. After a brief review of the reaccreditation process and discussion about the DPT curriculum and resources, the researchers anticipated this study would result in the revision of some existing objectives and the addition of new objectives to more accurately represent HI content already being taught in DPT courses.
Method
Study design
For this exploratory study, researchers felt mixed methods data collection was necessary to capture the rich, extemporaneous thoughts and beliefs of participants and to document changes in understanding of HI through participation in the study. Thus, quantitative and qualitative data collection methods were utilised to assess general knowledge of HI, determine whether HI content was already incorporated in courses, and if so, whether the content was accurately reflected in course SLOs. An action research approach was chosen as this methodology is widely used in higher education and health care to identify process improvements and initiate change (Baum et al., 2006; Saramunee, 2022).
Data collection
Qualitative data were collected through open-ended interview questions, review of course syllabi and during individual and small group semi-structured interviews that occurred in-person or online. Quantitative data were collected via an electronic six-item pre- and an eight-item post-interview questionnaire administered through QualtricsXM (Qualtrics Software Company, Seattle, WA, USA). All semi-structured interviews involved at least two researchers collecting data with most interviews including all three.
Sample
Candidate participants were from a convenience sample of 16 full- and part-time faculty members in an entry-level PT department at a large public university in the United States that had recently undergone CAPTE reaccreditation. Participation in the survey was voluntary. Informed consent was indicated through submission of the survey.
Procedure
Faculty members were invited to participate in the study during a routine, in-person department faculty meeting and received a follow-up email invitation with a link to the pre-interview questionnaire. Informed consent to participate in the study was obtained in the first question with the following questions asking participants about their familiarity with and use of HI in their courses. The last pre-interview questionnaire item asked participants for permission to be contacted by the researchers to schedule an interview. If a participant answered ‘yes’, they were taken to a separate survey where they could enter their email address. This step separated survey data from the email address ensuring the anonymity of the data. If participants answered ‘no’, they were thanked for answering the pre-interview questionnaire and this ended their participation in the study.
Those agreeing to be interviewed were asked to submit electronic copies of their course syllabi. Researchers reviewed course descriptions, SLOs, assignments and learning activities prior to individual or small group interviews. Semi-structured interview questions are shown in Table A1. Researchers took notes during in-person interviews while online interviews were recorded. Notes were reviewed and responses were categorised and discussed. Within 6 days of completing the interview, participants were invited to complete the post-interview questionnaire. Quantitative data from the pre- and post-interview questionnaires were analysed with descriptive statistics (percentages) and before and after results were compared.
This study was approved by the Institutional Review Board of our home institution with Approval ID 8773.
Results
Of the 16 possible participants, 13 PT faculty members completed the informed consent and pre-interview questionnaire. Of those, 12 agreed to continue to the interview and course syllabus review phase of the study. One of the 12 was unexpectedly placed on special assignment outside the department and was removed from the study. Of the remaining 11 participants, 8 responded to the follow-up emailed request to submit their course syllabi for review and schedule an interview. Since the majority of courses were co-taught, these eight participants represented 22/39 courses (56%) in the PT program and 50% (8/16) of the department faculty. Table 1 shows pre- and post-interview questions and quantitative results. Table 2 lists reviewed courses along with the number of faculty interviewed in each course.
Pre- and post-interview survey questions and results.
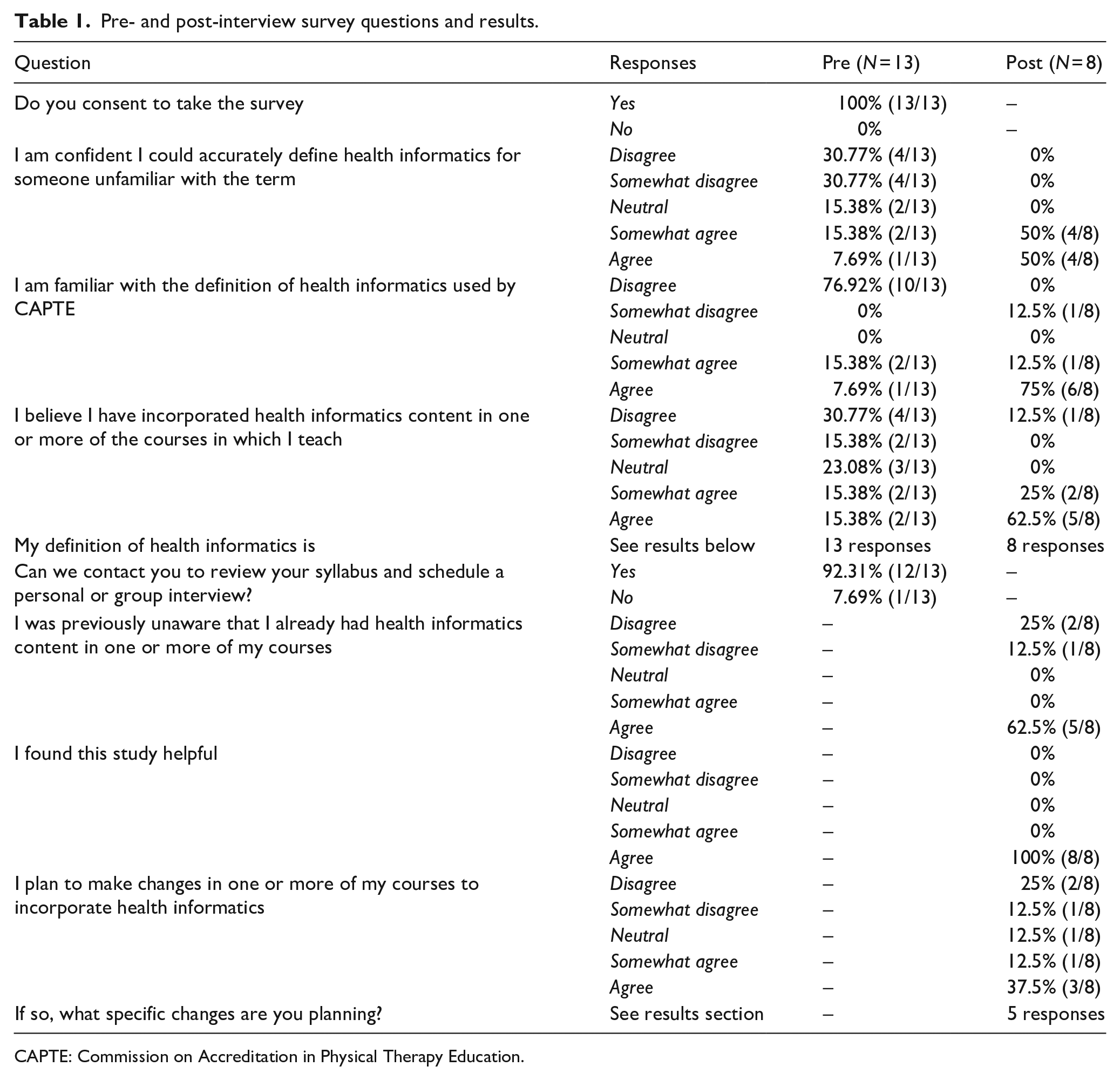
CAPTE: Commission on Accreditation in Physical Therapy Education.
Courses reviewed.
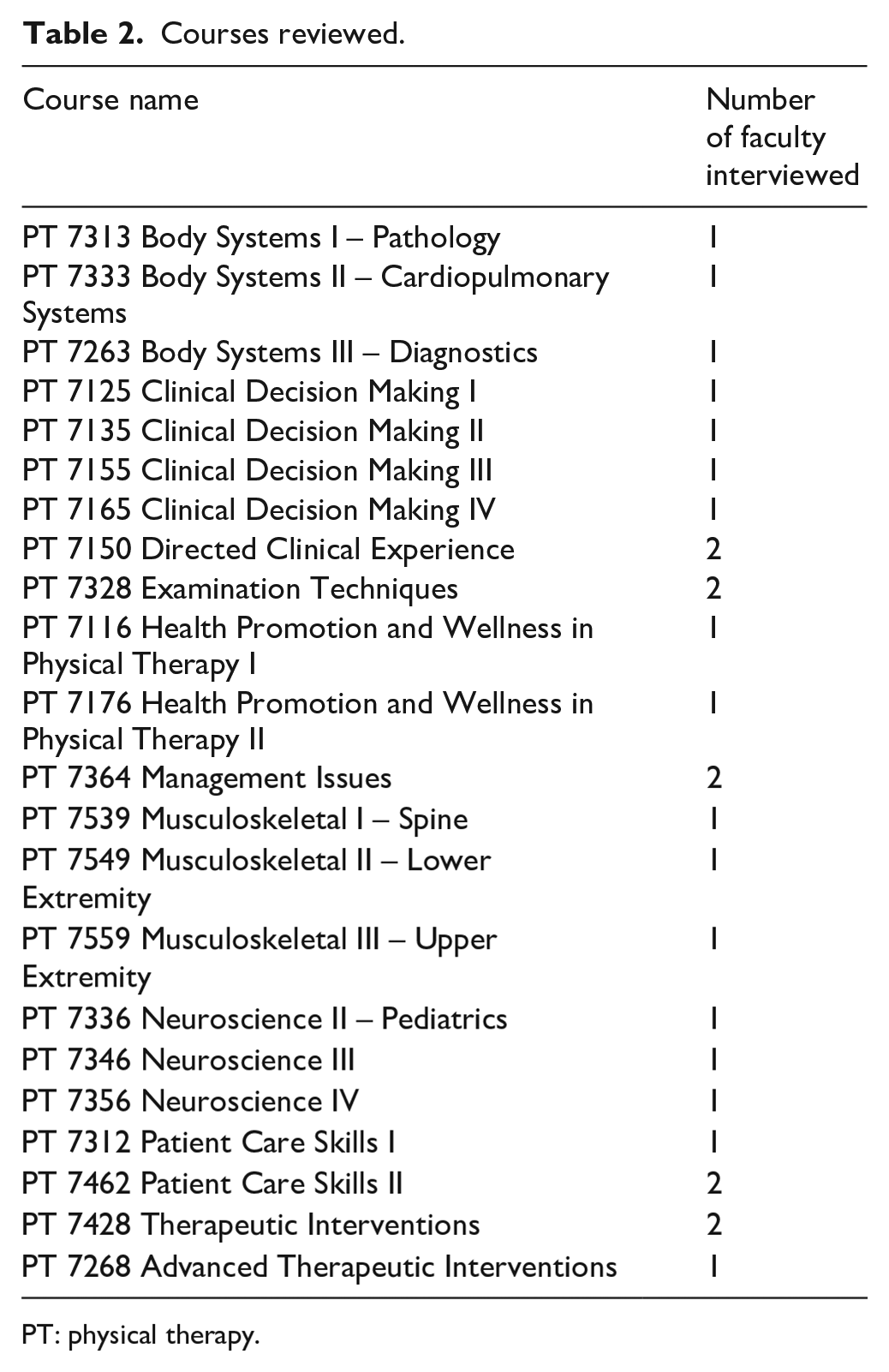
PT: physical therapy.
The pre-interview questionnaire included the prompt ‘My definition of health informatics is. . .’ with an open text box response. Slightly less than half (46%, 6/13) provided definitions that included an element of clinical decision making or words to that effect. Other responses indicated unfamiliarity with the term or focused on digital data but not its use to inform clinical decisions. Researchers agreed that 6 of 13 total definition responses in the pre-interview questionnaire included clinical decision making:
Use of health-related data to guide practice, clinical decision making and observe trends in health care and different populations
HI uses technology to improve health care and health care access
Use of technology for the collection and application of data to inform decision making in health care
The collection and use of health-related data for the purpose of providing health interventions/services or to understand disease/pathology processes or to conduct research
Using ‘big’ data as a way of making decisions about health for individuals, communities and society
Informatics involve the clinician’s use of technical data to improve the diagnosis, treatment and safety of patient care using evidence informed practice.
The remaining 7 of the 13 total responses (54%) did not clearly mention clinical decision making as an element of the definition for HI:
No idea
I do not know what this term means
Information provided regarding healthcare
Not sure
Collecting and using health-related data pertaining to support the health of patients
Use of health data to answer questions, solve problems, identify problems
Health-related data
Results from the post-interview survey revealed improvement in understanding. In the post-interview survey, 75% (6/8) of faculty participants included an element of clinical decision making in their definition of HI:
Using (big) data and best evidence to make clinical decisions
Use of technology to collect data for the purposes of analysis and decision making for clinical care and clinical system management/operations
The use of data generated electronically through the use of technology that can be used to guide clinical decision making
HI involves digital data and technology related to patient health care and community care to improve health outcomes
Any technology used in the clinic to drive clinical decision making
Use of electronic information in health professions to assist with assessment and intervention of patient/clients
Two (2/8) participants did not clearly mention clinical decision making in their definition of HI a few days after the interview on the post-interview questionnaire. One reported the definition as ‘The use of electronic methods to capture information for teaching or research purposed’ and the other reported ‘The utilisation of technology to collect, store, or analyse health data’. During interviews, the CAPTE definition of HI was reviewed followed by discussions focused on course SLOs and details of actual learning activities. After thorough review and discussion, researchers agreed with faculty that HI content was appropriately not included in two courses. For example, PT 7313 Body Systems I – Pathology was a lecture-based course with straightforward coverage of body system pathologies, symptoms and pain referral patterns with no clear need for HI. However, discussion of other courses generated several ideas for changes to some existing SLOs to better represent existing HI content and the creation of new SLOs to document previously unrecognised HI content (see Table 3). Several participants indicated they planned to make changes to their course(s) and some included ideas for changes in the post-interview questionnaire:
To be more mindful in the informatics that are currently used in the clinic and make informed decisions on use of material captured for future use
Incorporate movement analysis lab to teach typical and atypical gait patterns
I plan to update some of the course objectives in the courses I co-teach to reflect the true nature of the learning and assessment that takes place regarding HI course content
New objective for the class: 9. Collect, analyse and apply electronic examination data in clinical decision making for determining appropriate interventions (7D40).
Updates and additions of student learning objectives.
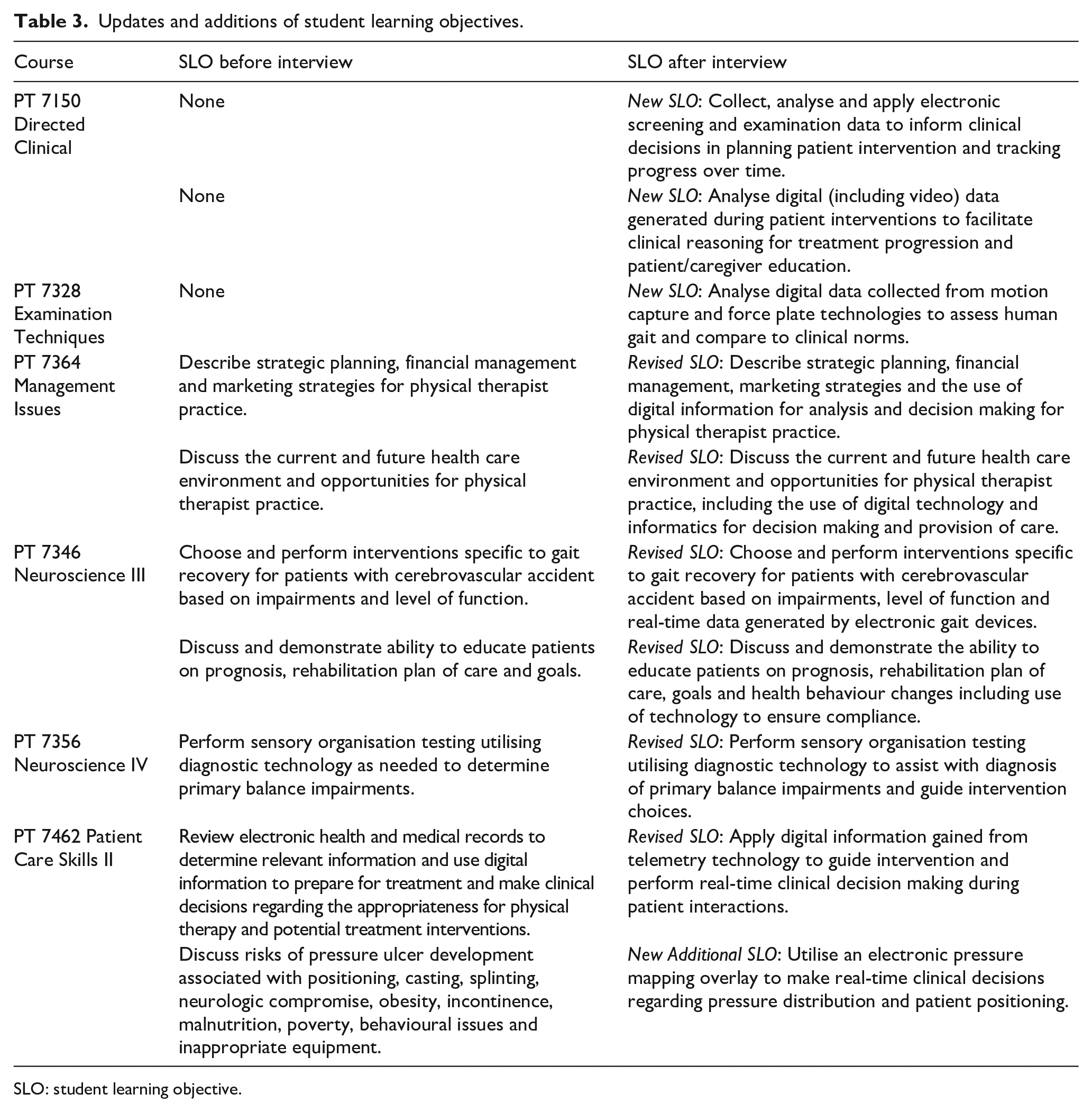
SLO: student learning objective.
Discussion
The aim of this study was achieved as unrecognised HI content was, in fact, hidden and identified in multiple courses across the DPT curriculum. The six revised and four new SLOs reported in Table 3 reflected newly identified HI content in six courses. As shown in the literature (Cutrer et al., 2021; Wilkerson et al., 2010), it is important to familiarise students with HI, so they specifically recognise how electronic data are used to improve clinical decision making. These revised and new objectives will facilitate the use of intentional HI-related terminology and instruction techniques in these courses and likely other courses taught by these same faculty members as they gain comfort and confidence with incorporating HI content. Post-interview results support that overall understanding of HI improved with full participation in the study with 100% (8/8) of participants indicating they somewhat agreed (4/8) or agreed (4/8) with feeling confident they could accurately define HI (CAPTE, 2020, 2023a) compared to less than 10% reported in the pre-interview questionnaire.
Additionally, individual and small group interviews resulted in many generative discussions that will likely lead to more changes as faculty plan their next iteration of courses. For example, PT 7263 Body Systems III – Diag-nostics covers diagnostic imaging (e.g. magnetic resonance imaging, computed tomography, X-rays and pharmacology). While only the pharmacology faculty member participated in the study, the interview raised awareness that electronic diagnostic imaging SLOs should be reviewed and discussed with appropriate faculty prior to next year’s delivery. Also, faculty in the neuroscience courses indicated the interview triggered initial ideas for additional learning activities utilising computer-based equipment in the program’s on-site clinic. The researchers were pleasantly surprised by the high level of faculty engagement in the study with interview discussions unintentionally inspiring the creation of new learning activities and associated SLOs in some courses.
The on-site PT 7150 Directed Clinical course delivered in the program’s on-site PT clinic had by far the most significant hidden HI content. In PT 7150, second year students engage in 6–8 weeks of faculty-supervised clinical practice in the campus-based clinic. Through direct patient care, students collect, analyse, track and base clinical decisions on electronic data from multiple sources, including: computer-assisted robotic arm; digital video gait recordings; multi-camera motion capture, balance and gait technologies; body weight support treadmills and a split-track treadmill. As noted in Table 3, two new SLOs were added to this course to represent the significant and broad scope of HI (Wilkerson et al., 2010) utilised by students in general PT practice.
Lastly, the research collaboration between PT and HIM was an important component in the overall success of the study. The PT researcher had a good understanding of PT education and CAPTE standards but was not an expert in HI. With expertise in HI, the HIM researchers were able to recognise hidden HI-related content and learning activities during syllabi review and faculty interviews. The HIM researchers also provided valuable guidance to participants who wanted to revise existing and/or add new SLOs during discussions.
Limitations
The small sample of convenience was a limiting factor in this study. Increasing the sample size by including PT faculty from multiple DPT programs would be a good next step. Additionally, the faculty involved having recently undergone CAPTE reaccreditation could have been a complicating factor as some faculty may have become more aware of HI through the process. Data from DPT programs that were further removed from reaccreditation might provide a better representation of day-to-day, typical faculty knowledge and understanding of HI. Another limitation is that not all courses in the DPT curriculum were represented in this study as not all faculty participated. It would be interesting to explore how HI might be represented in the cardiopulmonary, off-site clinical experience and research courses.
Conclusion
Results of this study revealed multiple instances of hidden HI content across the DPT curriculum. While the DPT program met HI standards during the recent reaccreditation, identifying these previously unrecognised, additional instances of HI instruction provided a much more accurate representation of how the program incorporated HI into the curriculum. The revised and newly added SLOs as well as those that will likely follow due to this study will assist faculty in preparing graduates to more fully utilise HI in today’s digital healthcare environments. Collaboration between PT and HIM faculty identified previously unidentified HI activities hiding in plain sight.
Footnotes
Appendix
Semi-structured interview questions.
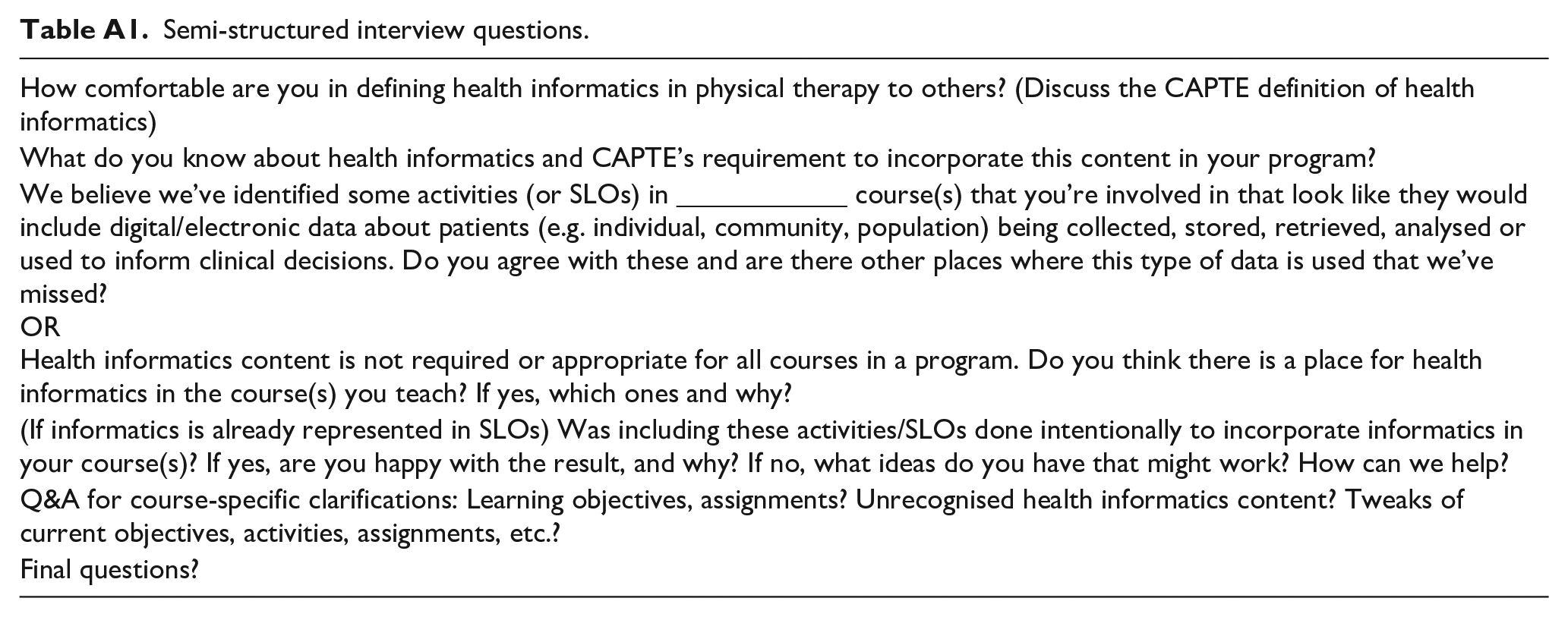
| How comfortable are you in defining health informatics in physical therapy to others? (Discuss the CAPTE definition of health informatics) |
| What do you know about health informatics and CAPTE’s requirement to incorporate this content in your program? |
| We believe we’ve identified some activities (or SLOs) in ____________ course(s) that you’re involved in that look like they would include digital/electronic data about patients (e.g. individual, community, population) being collected, stored, retrieved, analysed or used to inform clinical decisions. Do you agree with these and are there other places where this type of data is used that we’ve missed? OR Health informatics content is not required or appropriate for all courses in a program. Do you think there is a place for health informatics in the course(s) you teach? If yes, which ones and why? |
| (If informatics is already represented in SLOs) Was including these activities/SLOs done intentionally to incorporate informatics in your course(s)? If yes, are you happy with the result, and why? If no, what ideas do you have that might work? How can we help? |
| Q&A for course-specific clarifications: Learning objectives, assignments? Unrecognised health informatics content? Tweaks of current objectives, activities, assignments, etc.? |
| Final questions? |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.