
Abstract
Background:
Health information management (HIM) is at the core of health organisations, providing essential information. In Malawi, there is a substantial deficit of qualified personnel, specifically health information managers, who can properly manage health information in electronic and paper-based formats. The nation has no higher education institution offering an academic programme in HIM.
Objective:
To investigate the need for HIM professionals in Malawi government health facilities, to determine the kinds of data managed by data users; competencies of HIM workers and challenges associated with the current HIM system.
Method:
A cross-sectional research design was adopted, with a qualitative approach to gather data from data users and key informants, using two focused interview guides. Data were collected from 13 participants from 6 government health facilities representing the primary, secondary and tertiary healthcare delivery levels. Data were analysed thematically.
Results:
Data users handled a diverse range of data, the majority having moderate skills in HIM. Both data users and key informants reported experiencing challenges in dealing with the existing HIM system. Findings also revealed key challenges associated with the absence, or inadequacy, of a well-trained HIM professional workforce in Malawi health facilities.
Conclusion:
Introducing a training programme in HIM would improve data management in health facilities in Malawi. Well-managed data would improve the delivery of health care services.
Keywords
Introduction
Malawi is a landlocked country located in south-eastern Africa. It borders Tanzania to the north, Mozambique to the east and south and Zambia to the west. Malawi spans an area of 118,500 sq. km, of which one-fifth is water surface, largely dominated by Lake Malawi. The projected national population for 2023 was around 20.9 million people (World Population Review, 2022) and expected to reach approximately 25 million by 2030 (World Population Review, 2022). An estimated 85% of the population lives in rural areas. The country has three geographical regions: Northern, Central and Southern regions, which include 29 health districts (The Republic of Malawi, 2018, 2020).
In Malawi, healthcare services are delivered by both the public and the private sectors. The public sector includes all facilities under the Ministry of Health (MoH), Ministry of Local Government and Rural Development, the Ministry of Forestry, the Police, the Prisons and the Army. The private sector consists of private-for-profit and private-not-for-profit providers, mainly Christian Health Association of Malawi (CHAM), an example of the latter (Malawi Ministry of Health, 2021). The Malawi government, through the MoH is the largest provider of health care. CHAM is the second largest provider, offering complimentary services to the government and private-for-profit providers cover the small proportion remaining (CHAM, 2022).
Malawi’s health system is organised at primary, secondary and tertiary levels, linked through an elaborate referral system. Primary services are delivered through health posts, dispensaries, maternity, health centres and community, rural hospitals, while secondary services comprise district hospitals, the referral facilities for health centres and community and rural hospitals. They also service local town populations, offering both inpatient and out-patient services. CHAM hospitals also provide secondary level health care (Republic of Malawi, Department of Disaster Management Affairs, 2020). Tertiary level services comprise four central hospitals, which provide specialist referral health services for their respective regions and offer very specific services. There are 977 health facilities in Malawi, comprising 113 hospitals, 466 health centres, 48 dispensaries, 327 clinics and 23 health posts. These are managed by the government (472), complementary and alternative medicine (CHAM) (163), private (214), non-governmental organisations (NGOs) (58) and private companies (69) (Malawi Ministry of Health, 2021).
Health information is a critical and strategic resource for the management and monitoring of health sector performance (World Health Organization (WHO), 2010). Modern health care is heavily reliant on information (Al Kiyumi et al., 2016; Kitsios et al. 2020). Huge volumes of hospital data have created a large and growing demand for trained experts who can administer the systems effectively and support better health outcomes. Those who manage data in hospitals must be experts in health information management (HIM). The WHO promotes strengthening the six building blocks of a health system: (1) governance and policy; (2) service delivery; (3) human resources; (4) health commodities; (5) health financing and (6) health information systems (HIS) (MEASURE Evaluation and WHO, 2017, 2010).
A synthesis of the literature at international level revealed that HIM associations play significant roles in the overall promotion and support of HIM professionals. For instance, in Australia, the Health Information Management Association of Australia (HIMAA) promotes and supports HIM professionals as the universally recognised specialists in information management at all levels of the healthcare system (HIMAA, 2017; Riley et al., 2020). In Canada, the Canadian Health Information Management Association (CHIMA) is the certifying body and national association for almost 5000 HIM professionals across the country. In addition, CHIMA sets out HIM training curricula, accredits HIM educational programmes at colleges and universities and provides continuing education for HIM professionals in the workplace (Gibson et al., 2015). In the United States, the American Health Information Management Association (AHIMA) has helped in defining HIM professionals’ roles proactively and in investigating emerging themes in health information technologies (IFHIMA, 2022; Sandefer et al., 2015). In India, the Health Information Management Association’s (HIMA) goal is to provide the knowledge, resources and tools to advance health information professional practice and standards for the quality delivery of healthcare services (HIMA India, 2016). HIM professionals play a crucial role in providing, maintaining, protecting and managing health information.
An analysis of the literature from some developing countries such as Uganda, Nigeria, Ghana and Sierra Leone revealed shortcomings in the training of HIM professionals in health facilities (Ojo, 2018). There was an absence of formal training programmes in general for HIM practitioners, regardless of their level in the health system (Ojo, 2018). Local research has shown that Malawi’s health sector still lacks accurate, reliable, complete, consistent and timely health data to inform effective planning and resource management (Kasambara et al., 2017). A strong HIS makes it possible to track progress on improving the WHO’s other five health system building blocks and, ultimately, to monitor the achievement of the health-related sustainable development goals (SDGs) (MEASURE Evaluation and WHO, 2017).
HIM is the heart of a health organisation as it provides critically important information to data users such as doctors and other clinicians, health administrators and government health departments. The traditional role of a HIM professional is to organise, maintain and analyse accurate data, which are available for patient care and for management purposes (Nabimanya et al., 2020) and for health planning, population health monitoring, epidemiology and research. HIM specialists, therefore, need to integrate a variety of skills, such as a strong knowledge of medical terminology and disease processes, application of clinical classification systems, excellent managerial skills and computer and health information technology (IT) expertise, to manage the range of health information and human services for which they are responsible (Chikumba, 2017; Chikumba and Rasmussen, 2016). In the context of this study, both a health management information system (HMIS) and HIM system (HIS) are used interchangeably. In Malawi, these systems are used to collect, store, analyse and evaluate health-related data in health facilities. They also contribute to country-level monitoring and evaluation, research, policy and planning and generate indicators about outputs, outcomes and impact.
In Malawi, data are collected in health facilities through registers. Each health programme has registers for recording data for its specific indicators (Chikumba, 2017; Chikumba and Rasmussen, 2016). Key players at health facilities are facility managers (mainly clinical officers or nurses), and health surveillance assistants (HSAs). At the district level, each health programme has a coordinator who is responsible for managing the reported data from the health facilities. Critical activities of the health programme coordinators include data verification, compilation, analysis, reporting and provision of feedback to health facilities (Chikumba, 2017; Chikumba and Rasmussen, 2016). For some health programmes (including maternity, malaria and family planning services), data are captured into the District Health Information Software 2 (DHIS2) (national central data repository) from the paper forms with the assistance of HMIS officers, statistical clerks, data entry clerks and IT officers. DHIS2 was developed by the Health Information Systems Program (HISP) and it is supported by the University of Oslo’s Department of Informatics in Norway. The DHIS2 has the capability for data validation, analysis and reporting.
Health delivery systems lack HIM professionals who can perform effectively in HIM positions. Well-trained professionals in HIM can produce reports that are accurate, reliable, complete, consistent, relevant and up-to-date (MEASURE Evaluation and WHO, 2017). Normally, these reports are required by district health offices (DHOs), the MoH and other stakeholders for monitoring and evaluation of public health indicators, such as population health status; service provision, coverage and utility; drug stocks and consumption patterns; equipment status and availability of finances.
Currently, in Malawi there is a heavy shortfall of qualified personnel who can properly manage health information in both formats (print and electronic) in health facilities at all levels (Chikumba, 2017; Chikumba and Rasmussen, 2016; Kasambara et al., 2017; Malawi Ministry of Health, 2015). For example, staff who handle DHIS2 are not trained in HIM, rather, they have related qualifications such as in information and communication technology (ICT), computer science, informatics, statistics and others. There are some related academic programmes such as the master of informatics at the University of Malawi and master of public health (informatics) at Kamuzu University of Health Sciences. No institutions of higher learning in Malawi offer HIM at any level, be it certificate, diploma, bachelor degree, master degree or doctorate. This is evidenced by the absence of HIM on the National Council for Higher Education accredited programmes list across all higher education institutions in Malawi (National Council for Higher Education, 2022). In addition, in Malawi, there is no formally constituted HIM association to empower HIM professionals. It was against this background that the researchers observed a gap in qualified HIM professionals in Malawi, and were motivated to undertake this needs assessment study. It is noted that Kasambara et al. (2017) reported their related study in the Southern region, having collected their data in 2012. Therefore, the foci of the current study were the northern and central regions of Malawi.
Aim and objectives
The aim of the study was to investigate the need for HIM professionals in Malawi health facilities. The main objectives were to determine the kinds of data managed by data users in health facilities in Malawi; determine the competencies in HIM personnel in health facilities in Malawi and identify the challenges associated with the current HIM system.
Method
A cross-sectional research design, employing a qualitative approach, was adopted.
Sample
A sample of 13 data users and key informants was purposively selected from six health facilities dispersed across the northern and central regions. Purposive sampling was used to select participants who were the appropriate personnel to inform the study. The data users included HMIS officers, Statistical Clerks and Ward Clerks while key informants were those in management (i.e. DHOs, district medical officers, district nursing officers and hospital administrators). Within the national context, the study included representation of all three levels of public health delivery systems in the northern and central regions. Data were collected from six health facilities (three in each region) covering the primary, secondary and tertiary levels of the healthcare delivery systems. Thus, the sample was representative of all government health facilities in Malawi. It is noted that all government health facilities in southern region share the same healthcare delivery system.
Data collection
Written consent was obtained from all participants, and all health facilities in which sample members were employed. Two separate interview guides were developed to gather data from data users and key informants. Interview guides were piloted at the Saint John of God Mental Health Clinic using staff representing users and informants, and amended following their feedback. Data were collected through in-depth, face-to-face, semi-structured interviews, of approximately 45–55 minutes each, with all data users and key informants included in the sample. Two research assistants, trained on the interview guide prior to data collection, collected the data. A non-threatening environment allowed participants to open up and give rich information. Interviews continued until data saturation was achieved. Information obtained from participants was audio recorded and field notes also taken during data collection (see Supplemental Appendix 1 for copies of interview guides).
Data analysis
After listening to the audio recordings, researchers transcribed the interviews verbatim. They then verified transcriptions by re-reading the transcribed data to obtain an overall sense of the content. The data were analysed thematically (sorted into themes and sub-themes based on the study objectives). Thereafter, the researchers undertook a careful reading of the field notes, and further grouped related information and identifying themes. Finally, themes and sub-themes were grouped according to their content. Validation of findings was undertaken by returning transcripts to some participants.
Ethics approval
The research was approved initially by the Saint John of God College of Health Sciences Research Ethics Committee. Prior to the data collection, the study was reviewed and approved by the Mzuzu Central Hospital Publications and Ethics Committee.
Results
Demographic data
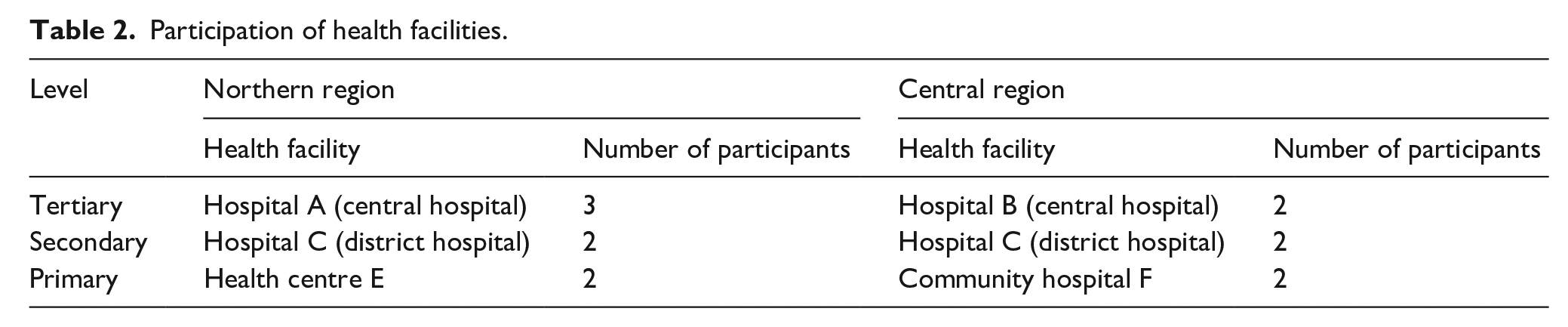
The 13 participants were from six government hospitals; seven participants were data users and six were key informants; six (86%) of data users were male, while key informants had equal gender representation; four data users were aged 30–34 years; three key informants were aged 35 years or over; four of the data users had worked for 6–10 years and three were holders of the Malawi School Certificate of Education (MSCE). Table 1 shows the participants’ demographic characteristics, while Table 2 summarises the participation of health facilities involved in the study in northern and central region of Malawi across all health care delivery systems.
Demographic distribution of study participants.
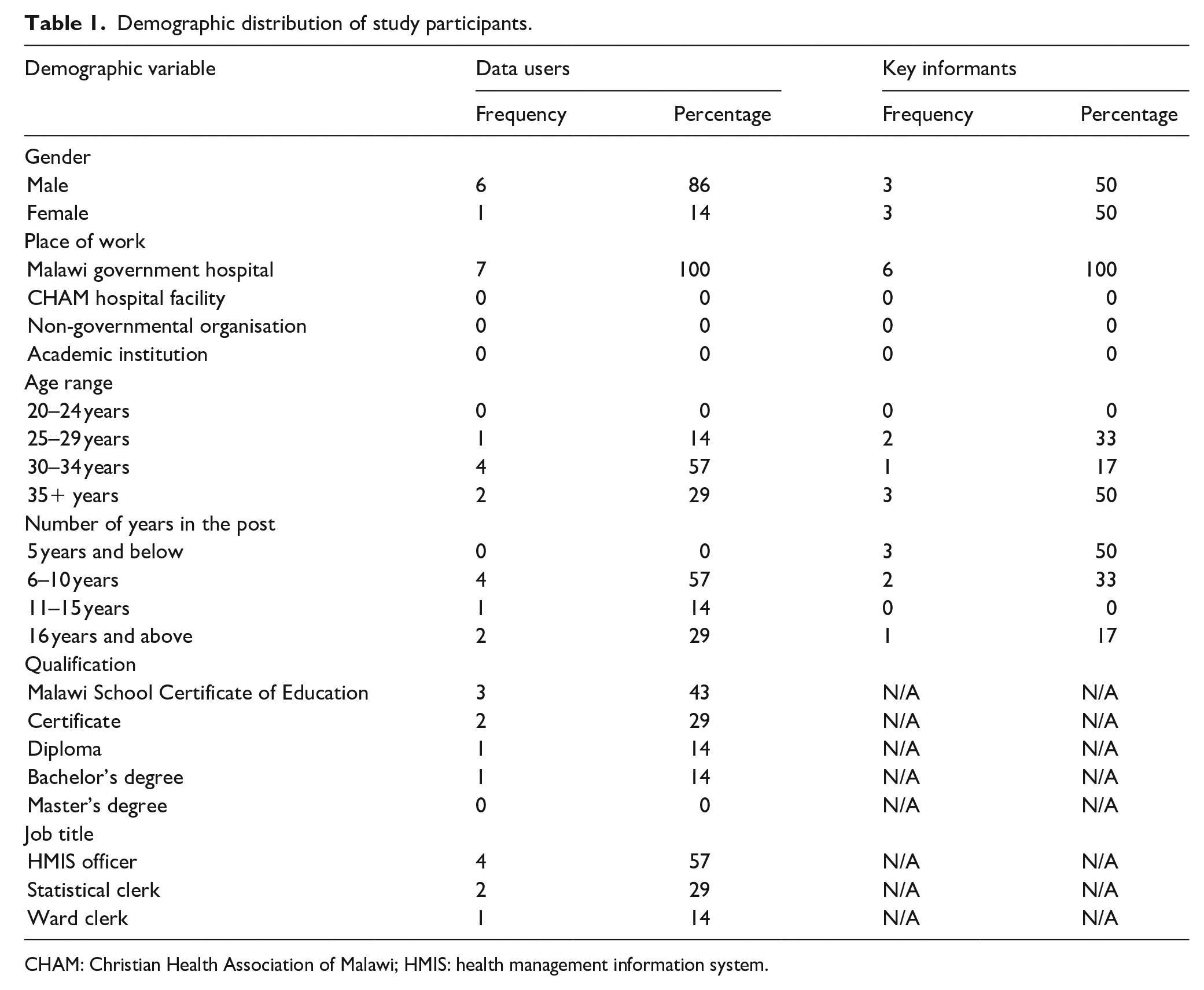
CHAM: Christian Health Association of Malawi; HMIS: health management information system.
Participation of health facilities.
Types of data managed by data users in health facilities
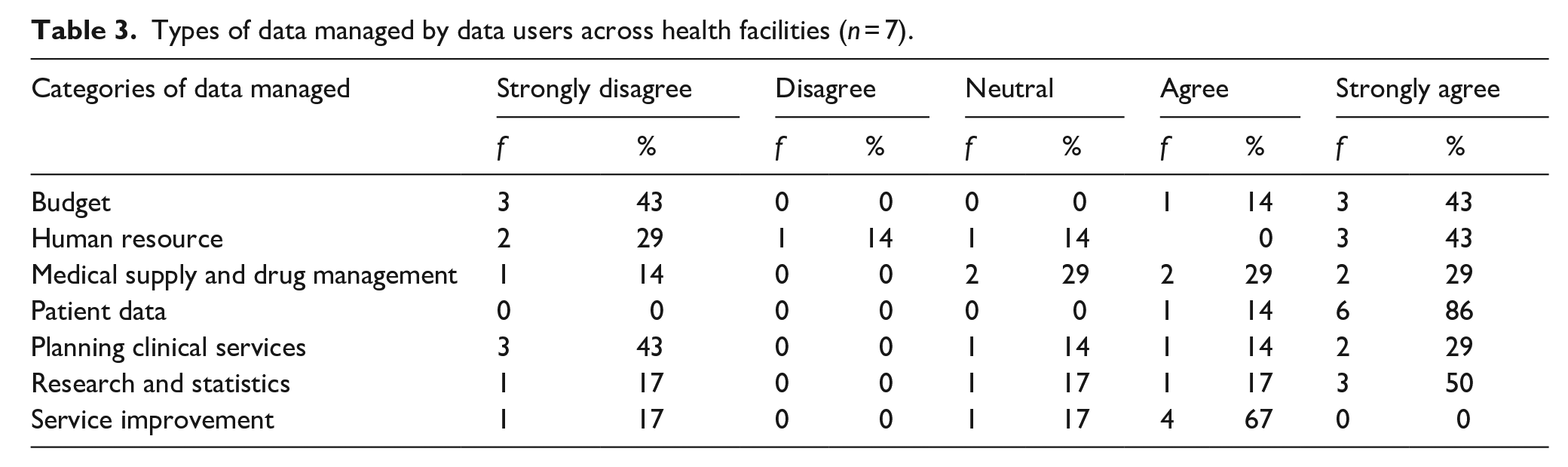
The data users managed all of the health facilities’ data. All seven of them (100%) indicated they managed patient data, while four of these also managed research, statistics and service improvement data. Table 3 presents additional details on categories of data managed by data users across the health facilities.
Types of data managed by data users across health facilities (n = 7).
Competencies in HIM
Four data users self-rated as having average skills in HIM, one self-rated as having low skills and two self-reported having high skills. No data user rated themselves as having very high skills in HIM.
Challenges associated with the available HIM system
Shortage of registers and stationery where case notes are captured
There was shortage of registers for capturing patient information in the health facilities. As highlighted in the data-flow section, registers in the health facilities were the primary data sources. The absence of registers resulted in missing data for patients who had sought health services at the facilities. Overall, this led to under-reporting of data collected from the health facilities. Consequently, this affected planning by management: ‘I would say that it is now almost a year without registers and this is a great challenge to us’ (Participant 1).
Qualifications of those involved in data capturing
Under-qualification of ward and statistical clerks and HMIS officers affected data management in the health facilities. The study revealed that the majority of ward and statistical clerks held the MSCE.
Absence of some indicators in DHIS2
Data users also reported that DHIS2 lacked some core indicators that existed in the health facilities’ registers. The missing indicators also led to data entry problems.
Frequent changes in some indicators and forms in DHIS2
It was reported that DHIS2 management periodically changed the reporting tools and indicators. Inadequate comprehension of the new data collection tools affected data quality.
Challenges associated with absence of well-trained HIM professionals
While the majority of individuals handling data in health facilities held the MSCE, very few had a diploma in ICT-related programmes and a few had a bachelor’s degree in statistics. No personnel who handled data had a HIM-specific qualification.
Inadequate medical and medical terminology knowledge
Data management was affected by inadequate medical knowledge by ward and statistical clerks. Data entry errors occurred when these categories of staff transferred data from patient files to registers because they did not understand medical abbreviations, medication and other medical terms. For example, ‘Honestly, I fail to understand the terms, abbreviations used by the clinicians. As a result, I end up missing some data when entering in registers’ (Participant 3).
Incomplete data
There was a problem of incomplete data across the sampled health facilities. It was reported that in some instances, data entry and statistical clerks were not recording some information in the registers, report forms and DHIS2. Some missing information included demographics of clients, such as age. For example, ‘It is frustrating to note that in most of the reports there are some gaps in terms of patients’ data like their age, diagnosis and some [other] information’ (Participant 4).
Errors at data entry due to clinicians’ handwriting
The handwriting of doctors and other clinicians contributed to data entry errors made by ward and statistical clerks. Due to inadequate medical knowledge, the latter categories of staff could not read and understand clinical information documented in patient files.
Manipulating data
Some data were also manipulated by data entry clerks. It was also noted that ward clerks at times entered incorrect data, which gave a false representation of the facts.
Limited analytical and data interpretation skills by ward clerks
Inadequate training of ward and statistical clerks affected data management in the health facilities. It was noted that these staff held the MSCE only and had received on-the-job training in data management when commencing their positions. These participants indicated that their training was not adequate for them to competently manage the data or to use tools such as Pivot tables and graphs; similarly, analysis of data was a challenge for them. For example, ‘I cannot come up with high level data analytics in the form of graphs, Pivot tables and others’ (Participant 8).
Late submission of reports
There was late submission of important reports to management from the HMIS office.
Lost data, especially during night shift
Unavailability of ward and statistical clerks at night resulted in missing data in the wards. This lack of coverage meant that data were not entered in the registers at night in health facilities.
Discussion
To have high-quality and reliable health information for administrative and medical operations, Malawian government hospitals must incorporate formally trained HIM practitioners (i.e. health information managers). This study found that various categories of data were managed by data users across health facilities in Malawi. These users had a mediocre level of knowledge and competencies in managing health information. The HIM system in Malawi’s public hospitals had a variety of problems.
Data users were managing all health facility data, including those related to budget; human resources; medical supplies and drug management; clinical services planning; service improvement, patient data and research and statistics. These findings are similar to those of Kasambara et al. (2017), Chikumba and Rasmussen (2016) and Chikumba (2017), who reported that data users were handling finance, administrative and human resource, research and client data. This implies that data users handled diverse forms of data depending on the setup of the hospital. Advancement in health IT has significantly assisted in the capturing and use of health data for supporting patient care, disease monitoring, health system planning and management, financial planning, education and research. Access to these systems and the skilled, qualified staff to operate them, would significantly improve the quality of data in all of the above areas.
Findings from this study demonstrated that few data users had high skills in HIM, and the majority had low skills in this specialised area. Some scholars in Africa have also reported gaps in skills and knowledge among workers who manage health information in hospitals (Adeleke et al., 2014; Kasambara et al., 2017; Ojo, 2018). They have recommended that much more needs to be done with regard to training to enhance skills and improve healthcare data management. HIM specialists need to integrate a number of skills to be competent at their job and manage the range of health information and human services for which they are responsible; these include strong knowledge of medical terminologies and disease processes, application of clinical classification systems, excellent managerial skills and computer and health IT expertise.
Key challenges associated with the existing HIM system in health facilities in Malawi were identified. These included a shortage of registers; incompetence in staff members’ handling of data; omission of some indicators in DHIS2 and frequent changes in some indicators and forms in DHIS2. The literature has suggested that these challenges are not new in Africa (Ojo, 2018; Sasaki et al., 2018; Smith et al., 2007) and may be linked to the fact that development of HIS in Africa has encountered serious problems due to substantial disparities in access to resources, including human resources. These resource insufficiencies in the health sector, coupled with the burden of disease, poor indicators and frail and unsuitable health systems are exacerbated by extreme poverty (Ssekitooleko, 2017). It has also been established that key challenges associated with the absence of well-trained HIM professionals in Malawi health facilities included inadequate knowledge of medical terms; incomplete data; mistakes at data entry; manipulation of data; lack of skills in data analysis and interpretation; delays in report submission and loss of data. All of these problems could be attributed to the absence of a training programme in HIM in Malawi. Compounding this is the fact that there are no established HIM career paths within the Malawi Ministry of Health.
Limitations
The most significant limitations of this study were the small number of study participants and the inclusion of only northern and central region government health facilities. Therefore, findings might not be generalisable to the Southern region. Absence of representation from CHAM, private companies, NGOs and academic institutions might have influenced results. In addition, participants may not necessarily have represented the gender distribution of data users in Malawi (although in Malawi many managerial positions are held by males). Chima (2022) found that more male students were enrolled for the past 3 years at Saint John of God College of Health Sciences in Malawi. Chima et al. (2023), Chawinga and Zozie (2016), Zozie and Chawinga (2018) also observed the dominance of male students in institutions of higher learning in Malawi. Thus, equal representation of male and female informants in the current study might not reflect the actual gender distribution of this category of health worker.
Recommendations
The following recommendations are made based on study findings:
A formal academic education programme in HIM should be introduced in Malawi, with consideration given to developing this at three levels: certificate, diploma and degree.
The MoH should be lobbied to recognise graduates in HIM for employment opportunities in the system, reflective of their academic level. This should include approaches by universities and colleges to the Malawi Ministry of Health to create various grades or cadres for HIM professionals for career pathways and their growth in the educational and healthcare systems.
Conclusion
In conclusion, this study found that health information has been affected because of untrained and under-trained data management personnel, attributable to the lack of qualified individuals to handle health data across health facilities. Furthermore, results have shown that the majority of data users had only average skills and knowledge in HIM. Consequently, inadequately skilled data-handling personnel have affected health facilities’ data quality and utilisation, paving the way for poor decision-making, contributed to incomplete and unreliable data, led to poor presentation of data, underpinned difficulties in retrieving important information in a timely manner, and associated difficulties in storage of data. Finally, the researchers acknowledge that qualified HIM professionals (health information managers) play a significant role in the healthcare delivery system by guaranteeing that the information necessary for improving services and outcomes is both timely and adequate. To this end, they recommended new academic programmes in HIM, which would be the first of their kind in the country. The curriculum should be contextualised to the local setting, and benchmarking undertaken with accredited institutions of higher learning outside Malawi.
Supplemental Material
sj-docx-1-him-10.1177_18333583231180772 – Supplemental material for The need for health information management professionals in Malawi health facilities
Supplemental material, sj-docx-1-him-10.1177_18333583231180772 for The need for health information management professionals in Malawi health facilities by Teddie Chima, Esmie Mkwinda and Stephen Kumwenda in Health Information Management Journal
Footnotes
Acknowledgements
The authors would like to thank the management of the health facilities for granting permission to gather data in their premises.
Postscript
Since undertaking this study, the researchers have developed a bachelor of science in HIM curriculum at their institution. The establishment of a national HIM association is the next necessary milestone for Malawi.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.