
Abstract
To present an overview of the current role of imaging in clinical trials of knee osteoarthritis (OA), focusing on radiography and magnetic resonance imaging (MRI) in the context of their role as both inclusion criteria and structural outcome measures. A non-systematic literature search (PubMed) was performed, starting with a list of terms including the title of the current manuscript, followed by multiple search terms. The identified methodologies, findings, concepts, and recommendations were organized into a systematic framework, providing an overview of the current and future role of imaging in OA clinical trials. Conventional radiography is the most commonly used modality for the evaluation of OA in clinical trials of disease-modifying OA drugs (DMOADs). Radiography is used to define the severity of structural disease and to measure joint space width as an inclusionary criterion, and has also been employed as an outcome measure. Limitations include a lack of reproducibility, a lack of sensitivity, specificity, and responsiveness regarding structural progression, and an insufficient ability to depict diagnoses of exclusion. MRI is more sensitive and specific in assessing tissue damage and its progression. Using abbreviated imaging protocols and rapid image assessment, MRI may be applied at screening. Quantitative and semiquantitative approaches have been commonly used as outcome measures, and both have advantages and disadvantages. Reasons for the failure of past DMOAD trials are multifold and include patient selection based on imaging and application of imaging outcome measures that are either not sufficiently sensitive to change or are difficult to reliably reproduce longitudinally.
Plain language summary
This article looks at how imaging is used in clinical trials for knee osteoarthritis (OA), with a focus on Xrays (radiography) and magnetic resonance imaging (MRI). Imaging is important for deciding who can take part in trials of new treatments, and for measuring whether these treatments work. X-rays are still the most commonly used method. They help show how severe the disease is, often by measuring the space between the bones in the knee joint. However, X-rays have clear drawbacks: results are not always consistent, they are not sensitive enough to detect early or small changes in the joint, and they do not show all the relevant tissues or rule out other conditions. MRI provides a more detailed picture. It can show damage of different tissues in the knee and track how these changes develop over time. Newer, shorter MRI scans and faster ways of reading the images may make MRI more practical for use in large trials. MRI results can be assessed in different ways (quantitative or semiquantitative), each with strengths and weaknesses. Many past trials of disease-modifying OA drugs (DMOADs) have failed, and one reason is the way imaging was used used – both for selecting patients and for measuring outcomes. Imaging tools sometimes lacked sensitivity to detect meaningful changes or were hard to reproduce reliably across time. While X-rays remain the standard in many trials, MRI is increasingly valuable and may play a bigger role in the future. Improving how imaging is applied could help design better trials and bring more effective treatments for knee OA.
Introduction
Osteoarthritis (OA) is a heterogeneous disease affecting more than 500 million people worldwide. 1 There are currently no disease-modifying treatments for OA, and there is an unmet need for new drugs that can target not only the symptoms but also the underlying mechanisms of the disease. 2 Current non-surgical management remains focused on symptom relief, including self-management, education, weight reduction, strength training, and analgesic and anti-inflammatory drug therapy. 3 The complex etiopathogenesis of OA has made the task of drug development complex, and there have been an abundance of failed clinical trials in the past decades. 4 Despite both phenotypic and etiological differences, OA patients are generally treated as a homogenous disease population, which is likely a contributing factor to trial failure. 5
In clinical trials, a “one size fits all” approach has led to reduced ability to show efficacy of novel treatments, resulting in discontinuation of drug development, which otherwise might have shown efficacy in specific subsets of patients. 6 One example is sprifermin, a treatment that showed a dose-dependent effect on cartilage thickness but no effects on symptoms in the intention-to-treat analysis. 7 However, a post hoc evaluation demonstrated both a clinical and structural benefit for a defined “subgroup at risk.” 8
One of the most significant advances in our understanding of OA pathophysiology over recent decades is the recognition that OA is no longer considered a degenerative condition caused only by mechanical wear and tear. It is now considered a serious disease by the United States Food and Drug Administration (FDA), which recognizes the significant impact of the condition on patients’ lives, encourages the development of more effective treatments, and can accelerate the development and approval of new treatments for this condition.9,10 OA is now understood as a multifactorial disease involving biomechanical dysfunction and persistent low-grade inflammation leading to progressive cartilage degradation.11,12 Enrichment and stratification strategies present an opportunity to improve clinical trial outcomes by identifying and grouping patients based on clinical, biochemical, or other markers, including imaging, considering a given mode of action of an investigational agent. 13
This perspective paper aims to give an overview of the current role of imaging in clinical trials of knee OA, focusing on radiography and magnetic resonance imaging (MRI) in an eligibility context and their role regarding structural outcomes. Furthermore, we will discuss analytic considerations, will elaborate on the differences between disease-modifying OA drug (DMOAD) and pain trials, and will conclude with an outlook on the current and future role of artificial intelligence (AI) in imaging of OA clinical trials.
Methods
A non-systematic literature search was performed using PubMed, starting with a list of terms including the title of the current manuscript, followed by multiple search terms including but not limited to “imaging,” ”radiography,” “quantitative,” “semiquantitative,” “joint,” “whole organ,” “joint tissue,” “joint structure,” “assessment,” “score,” “measure,” “endpoint,” “analysis,” “outcome,” “intervention,” “clinical trial,” “DMOAD,” “drug,” “mechanism of action,” “MRI,” “scoring,” “phenotype,” “morphotype,” “responsiveness,” “validity,” “reliability,” “artificial intelligence,” and possible variants for each. Results of the search were reviewed by the first and last authors to determine the relevance of the selected publications for the focus topic of this manuscript. All authors of this article made a joint decision on which articles to include and considered the most relevant. Finally, to receive broad and detailed input, informal (i.e., non-structured) consultations were held with domain experts in various research areas. The identified methodologies, findings, concepts, and recommendations were then organized into a systematic framework, providing an overview of the current and future role of imaging in OA clinical trials, considering the state of the art of current imaging science.
Results
Radiography
Radiography has been the core method for structural assessment of knee OA for decades. It supports establishing a structural diagnosis and monitoring disease progression. Radiographs visualize bony features of OA and offer an indirect estimate of cartilage thickness and meniscal integrity through joint space width (JSW) assessment. 14 The radiographic evaluation of OA typically focuses on osteophyte formation and joint space narrowing (JSN).
Technical considerations
Tibiofemoral joint radiography is commonly performed using the anteroposterior (a.p.) view. While supine (non-weight-bearing) a.p. images are easy to acquire, they are not suitable for assessing JSW or alignment in a clinical trial setting. To improve visualization of the medial joint space, Buckland-Wright and others introduced techniques that allow reproducible and standardized knee positioning, commonly using a posterior–anterior (p.a.) view and a positioning device.15,16 These methods aim to align the medial tibial plateau consistently while slightly flexing the knee. Alternatively, using a fluoroscopic approach, the anterior and posterior rims of the lateral tibial plateau are aligned under direct visualization. The modified Lyon-Schuss technique involves taking three radiographs with slight (2°) changes in beam angle and selecting the best image based on the inter-margin distance. 17
Long-limb films have traditionally been used to assess varus or valgus deformities, but more recent studies have suggested that standard weight-bearing knee radiographs are sufficient for alignment evaluation in the context of trial inclusion. 18 For eligibility purposes, most trials only acquire a single weight-bearing view that is used for Kellgren and Lawrence (KL) grading and scoring according to Osteoarthritis Research Society International (OARSI) atlas-based osteophyte and JSW assessment.
Challenges of radiography
Radiography projects 3D anatomy onto a 2D image, making it susceptible to distortion, magnification, and superimposition of anatomical structures. Even slight variability in positioning between visits can significantly affect JSW measurements. 19 Early cartilage loss often begins in the posterior femur, 20 which does not have contact with the tibia in full extension. Mild flexion brings the posterior femur in contact with the opposing tibia, therefore improving sensitivity to early disease. For longitudinal assessment of JSW, consistent imaging conditions are critical.
Radiographic image assessment
The KL grading system remains widely used for screening potential trial participants. A definite osteophyte indicates the presence of structural OA (KL grade 2) and is required to fulfill the American College of Rheumatology classification criteria for knee OA. 21 The presence of both definite JSN and osteophytes indicates moderate OA (KL grade 3). 22 Patients with both KL grades 2 and 3 are commonly included in clinical trials, while those with KL grades 0, 1, and 4 are often excluded. For more detailed assessments, the OARSI atlas provides a structured method to score individual radiographic features on a compartmental level. 23 Knee OA progression is often measured by changes in JSW, typically at the medial compartment, and is responsive. 24 Measurement methods include manual tools and semi- or fully automated software. 25
Magnetic resonance imaging
Although radiography remains the standard imaging modality for establishing structural inclusion and exclusion criteria, it has considerable limitations. These include, but are not limited to, a lack of reproducibility of JSW measurements, a lack of sensitivity and specificity, an insufficient definition of disease severity, a weak association of radiographic structural damage and symptoms, an inability to differentiate structural morphotypes, and an inability to depict diagnoses of exclusion. These shortcomings significantly constrain its usefulness in clinical trials. Historically considered a disease of “wear and tear,” the advent of MRI has shifted the paradigm in that OA is now recognized as a whole-organ disease involving multiple joint tissues. 12
Technical aspects
1.5T and 3T systems are commonly used for structural OA assessment in clinical trials. Low field systems have seen a renaissance in recent years, but their validation is still ongoing. 26 Super-high field systems (7T MRI) are not widely available and pose challenges regarding costs, patient comfort, and potential side effects. 27 Concerning specific MRI sequence protocols, the minimum requirement would consist of fluid-sensitive fat-suppressed sequences in three planes and one non-fat-suppressed T1-weighted sequence to rule out safety findings and allow for semiquantitative scoring. 25 If 3D volumetric or bone shape analysis is to be included for quantitative assessment, an additional high-resolution 3D gradient-echo (GRE) sequence is necessary. 28 Although developed for dedicated cartilage imaging, 3D GRE-based techniques are inferior in depicting focal cartilage defects and bone marrow lesions (BMLs) when compared to standard 2D turbo spin-echo techniques.29–31 Detailed suggestions for pulse sequence protocols to be used in a clinical trial setting have been published elsewhere.25,28,32
Semiquantitative MRI assessment
MRI-based semiquantitative scoring is a valuable method for assessing knee OA in clinical trials. The first published scoring system employing a “whole-organ” approach to knee OA, the Whole-Organ Magnetic Resonance Imaging Score, was published in 2004. 33 It covers a range of tissues involved in the OA disease process. Several additional scoring systems have been presented since, with the MRI Osteoarthritis Knee Score being the one most commonly applied in a context of clinical trials and observational studies. 34 These scoring systems analyze MRI without intravenous contrast agents, whereas other methodologies focus on contrast-enhanced MRI, specifically tailored for the evaluation of synovitis, such as those developed by Guermazi et al. 35 (commonly referred to as the “11-point scoring system”), Rhodes et al., 36 and Baker et al. 37 Several clinical trials of knee OA have incorporated semiquantitative MRI assessments. Although quantitative MRI techniques are more sensitive to change and have demonstrated dose-dependent responses to potential DMOADs for cartilage assessment, 7 the primary utility of semiquantitative assessment lies in participant eligibility screening and on-study safety monitoring. 38
Quantitative MRI assessment
Quantitative assessment of cartilage morphology leverages the 3D capabilities of MRI to evaluate tissue structure as continuous variables through segmentation techniques. Image analysis software enables the calculation of various morphologic parameters, including cartilage volume, thickness, subchondral bone size, cartilage surface area, and the area of denuded subchondral bone, among others. Given that both cartilage thinning and thickening can occur concurrently in different subregions of the knee, location-independent analytical approaches that are focused on the overall magnitude of change have been proposed to enhance sensitivity in detecting structural alterations. 39 Quantitative assessments of changes in cartilage volume and thickness have been employed as outcome measures in interventional clinical trials investigating the effects of various agents. A phase II study showed that sprifermin (recombinant human fibroblast growth factor 18) had a dose-dependent beneficial effect on the preservation and potentially regeneration of articular cartilage compared to placebo. 7 Quantitative joint analyses of other joint tissues, such as the bone, meniscus, and infrapatellar fat pad, have been applied in observational studies, but not in clinical trials to date. 40
Bone shape analysis, particularly using 3D MRI-based statistical shape modeling, has emerged as a promising imaging biomarker in OA research and DMOAD trials. 41 It offers the ability to detect subtle and quantitative changes in joint surface morphology that may precede cartilage loss. 42 While shape alterations reflect surface remodeling and osteophyte growth, it remains unclear whether observed changes are a cause, consequence, or simply a correlate of other pathological processes. Limitations of bone shape analysis include potential variabilities secondary to differences in imaging protocols, scanner types, and software algorithms. Further validation, standardization, and integration with other imaging and clinical markers are desirable before using shape as a standalone endpoint in a regulatory context.
Contrast-enhanced MRI
In most DMOAD trials, MRI is performed without intravenous gadolinium contrast enhancement (CE) for operational and safety reasons. Standard clinical sequences without contrast may be used to evaluate synovitis, applying the surrogates of effusion- and Hoffa-synovitis.34,43 However, synovitis and effusion are ideally depicted by T1-weighted fat-suppressed CE-MRI, with several dedicated scoring and measurement systems being available, including synovitis assessment at multiple locations, allowing for a comprehensive whole joint evaluation of synovitis burden.35–37 Figure 1 depicts a comparison of non-enhanced and T1-weighted fat-suppressed CE MRI for the detection of inflammatory features in knee OA.

Non-enhanced and contrast-enhanced MRI visualization of inflammatory features of knee osteoarthritis. (a) Sagittal non-enhanced intermediate-weighted fat-suppressed MRI shows marked joint effusion-synovitis in the suprapatellar recess (asterisk) and hyperintensity signal changes at Hoffa’s fat pad consistent with Hoffa-synovitis (arrows). Note that a differentiation of synovial thickening from intra-articular fluid is not possible using non-enhanced MRI. (b) Corresponding T1-weighted fat-suppressed contrast-enhanced MRI shows synovial thickening and enhancement in the suprapatellar recess, at the infrapatellar location, and at the posterior border of Hoffa’s fat pad (arrows), three locations that are part of the so-called 11-point scoring instrument. (c) Axial T1-weighted fat-suppressed image of the same knee shows marked thickening of the synovial lining at the lateral (arrow) and medial (arrowhead) parapatellar recesses. Note that intra-articular joint fluid is depicted in a hypointense fashion (asterisk).
Dynamic CE (DCE) MRI may be applied for advanced assessment of synovitis and evaluation of therapeutic response. 44 The technique is based on rapid serial acquisitions of the same anatomical area. Various curve profiles are used to calculate the rate of CE, the maximum enhancement, the time to peak, the area under the enhancement curve, and the potential washout rate. 45 Ktrans is the most promising DCE-MRI parameter for synovitis assessment that measures contrast agent accumulation in the extravascular extracellular space. It shows the greatest sensitivity to temporal change, best discrimination between OA and healthy patients, and best test–retest reliability compared to other parameters. 44 DCE-MRI is less practical for screening purposes due to processing demands and limited joint coverage.
Compositional MRI
Compositional MRI can detect changes in cartilage composition and ultra-structure during the earliest stages of cartilage degeneration prior to the onset of morphologic cartilage loss. 46 A wide variety of compositional MRI methods have been applied in observational studies. These techniques provide information regarding different constituents of cartilage and have different advantages and limitations. Due to challenges in the interpretation and missing standardization of these techniques, 47 application in a clinical trial context has been limited to date, although they may be particularly useful in the future in trials focused on “pre-OA.” 48
Accelerated MRI
MRI acquisition is more time-consuming and costly compared to radiography. However, recent advancements in MRI acquisition techniques have significantly reduced scan times, thereby enhancing the feasibility of MRI-based screening and lowering associated costs. 49 Parallel imaging, simultaneous multislice acquisition, and compressed sensing-based undersampling can be applied independently or in combination to expedite MRI scans substantially. Deep learning (DL)-based image reconstruction and superresolution augmentation methods support image reconstruction of such highly accelerated acquisitions. 50 In concert, moderate acceleration and image reconstruction techniques available today enable high diagnostic image quality, facilitating threefold to sixfold accelerated 2D turbo spin-echo MRI within 4–6 min. 51
Structural phenotyping
To increase the probability of demonstrating treatment success, trial inclusion criteria may target patients who are at increased risk for disease progression. In addition, the mode of action of the compound under study needs to be considered. Radiography does not allow adequate phenotypic characterization of joint structure, which is the domain of MRI. 52 A simplified MRI instrument, ROAMES, differentiates five structural pheno- or morphotypes of OA: inflammatory, meniscus/cartilage, subchondral bone, atrophic, and hypertrophic. 43 Figure 2 presents the three main structural phenotypes defined by MRI. The objective of this scoring tool is to facilitate subject stratification and identify exclusionary diagnoses. It is important to note that structural phenotypes may overlap, and investigators should be mindful of this limitation when applying phenotypic stratification. 52 Further refinement in the characterization of these structural phenotypes is necessary, and the development of novel analytical approaches may facilitate this process. 53

Examples of structural pheno- or morphotypes as visualized by MRI. (a) Sagittal intermediate-weighted fat-suppressed MRI shows large BMLs at the medial femur (arrowheads) and tibia (arrows), characterizing this knee as exhibiting the subchondral bone pheno- or morphotype. (b) Coronal intermediate-weighted fat-suppressed image shows diffuse full-thickness cartilage loss at the central medial femur and tibia (arrows). There is advanced substance loss of the medial meniscal body (arrowhead). Cartilage and meniscal damage characterize the meniscus/cartilage pheno- or morphotype. In addition, there is a large BML at the central medial femur (asterisk), which characterizes the subchondral bone pheno- or morphotype. Overlap between morphotypes is not unusual. (c) Axial intermediate-weighted fat-suppressed image shows full-thickness cartilage damage at the medial patellar facet (arrow). In addition, there is marked joint effusion-synovitis with extensive distension of the joint capsule (asterisk), characterizing this knee as exhibiting an inflammatory morphotype.
Detection of so-called exclusionary findings at screening
There are several reasons certain MRI findings may be deemed “exclusionary” at the eligibility stage. These include findings that increase risk for articular collapse, which is likely not amenable to any pharmacologic (i.e., DMOAD) intervention, and concerning findings that may be considered on-study safety findings, that is, potentially considered to be related to the treatment being tested. Finally, there may be findings or diagnoses that by consensus should not be present at baseline, such as tumors or malignant bone marrow infiltration. A recent study analyzing data from the Osteoarthritis Initiative (OAI) identified high-risk exclusionary MRI findings in up to 3% of knees with KL grade 2 and up to 12% of knees with KL grade 3, with complete medial meniscus root tears the most frequently present abnormality. 54 It has to be acknowledged that the real prevalence of these pathologies in the context of DMOAD trials is currently unavailable. Illustrative examples of baseline exclusionary MRI findings are presented in Figure 3.

Examples of baseline exclusionary imaging findings as visualized by MRI. Several structural so-called exclusionary findings are only visible on MRI and should be ruled out during the screening process of a given clinical trial, as they either increase the risk of articular collapse not amenable to any DMOAD treatment effects or may be considered on-study safety events in case these are detected during the course of a given trial. (a) Sagittal intermediate-weighted fat-suppressed image shows marked intra-articular effusion-synovitis (asterisk). In addition, there is an expansive soft tissue mass of intermediate signal intensity at the dorsal aspect of Hoffa’s fat pad, consistent with tenosynovial giant cell tumor (arrows). Joints with tumors are not considered eligible in clinical trials of osteoarthritis. (b) Coronal intermediate-weighted fat-suppressed image shows a SIF at the central medial femur characterized by a hypointense line in a subchondral location (arrow). Note also the slight depression of the articular surface but intact cartilage coverage (arrowhead). In addition, there is marked accompanying bone marrow edema, which is a characteristic finding in SIF (asterisk). (c) Another knee (coronal intermediate-weighted fat-suppressed image) shows a complete posterior root tear of the medial meniscus. Note that the tibial attachment of the meniscus is interrupted and not continuous (arrows). This often results in markedly altered biomechanics and a highly increased risk of fast cartilage loss, SIF, and articular collapse.
Specific aspects regarding the use of imaging in OA clinical trials
Assessment of intra-articular drug delivery
In the context of imaging, it is important to confirm the correct intra-articular administration of a given drug. 55 Confirmation can be obtained using ultrasound by direct visualization of the needle within the articular cavity at the time of injection or by radiography showing intra-articular air after injecting 5–10 ml of air. While ultrasound-guided injection showed somewhat higher success rates compared to palpation-guided injection, X-ray documentation of intra-articular injection using air seems paramount to avoid subsequent extra-articular injection and thus, maximize efficacy. 56 Figure 4 shows examples of intra- versus extra-articular injection.

Relevance of confirmation of correct intra-articular injection of active drug or placebo. (a) Lateral X-ray acquired 5 min after intra-articular injection of drug or placebo, and subsequent injection of 10 mL air shows complete intra-articular distribution of air. Air is clearly visible in the suprapatellar recess (asterisk), posterior to the femoral condyles (arrow), and along the posterior border of Hoffa’s fat pad and clearly not within the fat pad (arrowheads). (b) Another example shows insufficient intra-articular distribution. Most of the air was injected into Hoffa’s fat pad, but not the intra-articular cavity (arrows). In addition, there is clearly an extra-articular distribution of air adjacent to the quadriceps tendon and anterior to the patella (arrowheads). (c) Lateral X-ray of another case shows no intra-articular air at all, but extra-articular distribution of air along the quadriceps fascia (arrows). Note that extra-articular deposition of the drug may potentially lead to on-study safety events.
Centralized assessment, reliability, and training
The FDA clearly recommends centralized reading in their guidance document from 2018 entitled “Clinical Trial Imaging Endpoint Process Standards—Guidance for Industry” that states “a centralized image interpretation process, fully blinded, may greatly enhance the credibility of image assessments and better ensure consistency of image assessments. Hence, a centralized image interpretation process may be used to help control image quality as well as to provide the actual imaging-based endpoint measurements. Some image interpretation methods, such as trial-specific measures of bone or joint disease in arthritic diseases, rely upon centralized imaging because of the extent of reader training recommended for the specialized image interpretation.”
In a systematic review on the responsiveness to change and reliability of radiographic JSW assessment, Reichmann et al. 24 reported a pooled standardized response mean (SRM) of 0.33 and reliability around 0.9, concluding that measurement of JSW is moderately responsive and highly reliable. Regarding semiquantitative MRI assessment, Crema et al. 57 reported that high levels of cross-sectional reliability and moderate to high longitudinal reliability were achieved using four experienced readers of most knee OA features with longitudinal reliability. Regarding a direct comparison between radiography and quantitative MRI, the latter displayed greater responsiveness than radiographic JSW, with the greatest SRM for MRI observed in the central medial femorotibial compartment (−0.43 vs −0.31, p = 0.017). 58 Concerning reader training, it has been shown that site investigators commonly over-grade osteophytes compared to a highly experienced central reader and an adjudicator, emphasizing the relevance of centralized reading in clinical trials of knee OA. 59
Analytic considerations
Several key aspects must be considered in the statistical analysis of imaging data. The data are often hierarchically clustered, for example, subregions nested in compartments, or longitudinal, which require appropriate statistical models. Analyzing multiple joint regions or evaluating multiple imaging biomarkers requires adjustment for multiple comparisons. The common approach of summing subregional scores across the knee joint and comparing these sums between treatment and placebo groups can mitigate the multiple testing problem by creating one summary score; however, much information is lost, which may mask meaningful variation in individual subregions or features. 60
Within-grade changes in semiquantitative scoring are changes that do not meet the criteria for a full-grade change but reflect definite visual alterations. These changes have been demonstrated to be clinically significant and enhance sensitivity to detecting change. 61 Validity has been established for longitudinal cartilage assessment, demonstrating strong correlations with quantitative cartilage loss. 62
There has been growing interest in defining a composite outcome that captures disease progression across the entire joint. Driban et al. 63 sought to establish a multi-domain outcome incorporating quantitative assessments of cartilage damage, BMLs, and effusion-synovitis to represent pathology across multiple joint tissues.
No studies have directly compared the sensitivity to change between quantitative and semiquantitative MRI assessments. Although SRMs are commonly employed to evaluate responsiveness, interpreting this metric, defined as the mean change divided by the standard deviation of change, is less straightforward for non-Gaussian data, thereby complicating direct comparisons between semiquantitative and quantitative measures. 60
There has been an ongoing debate regarding whether image interpretation blinded to the timing of acquisition is preferable to unblinded reading. While unblinded reading may introduce a slight bias toward detecting greater change, evidence indicates that scoring without knowledge of the chronological sequence significantly reduces sensitivity to change.64,65 Another important aspect is that assessing image data in chronological order allows for potential structural adverse events to be detected early, which would not be the case when assessing images in blinded chronological order after the study has been completed.
Discussion
Do we still need X-rays in clinical DMOAD trials? And for which use?
The limitations of conventional radiography as an imaging technique to meaningfully assess pathological features of OA are described above. 66 Radiography, however, is still relevant to define established structural disease, that is, exclude those without radiographic OA (KL grade 0, 1) as well as those with end-stage structural disease (KL grade 4). Furthermore, a minimal JSW at inclusion is required for DMOAD trials and needs to be quantified by a standardized assessment. For example, the so-called “subjects-at-risk” subgroup of the above-mentioned sprifermin trial was based on low minimal JSW (1.5–3.5 mm) and moderate-to-high pain at baseline. 8 A suggestion for a screening and inclusion algorithm using imaging in a knee DMOAD trial is presented in Figure 5.
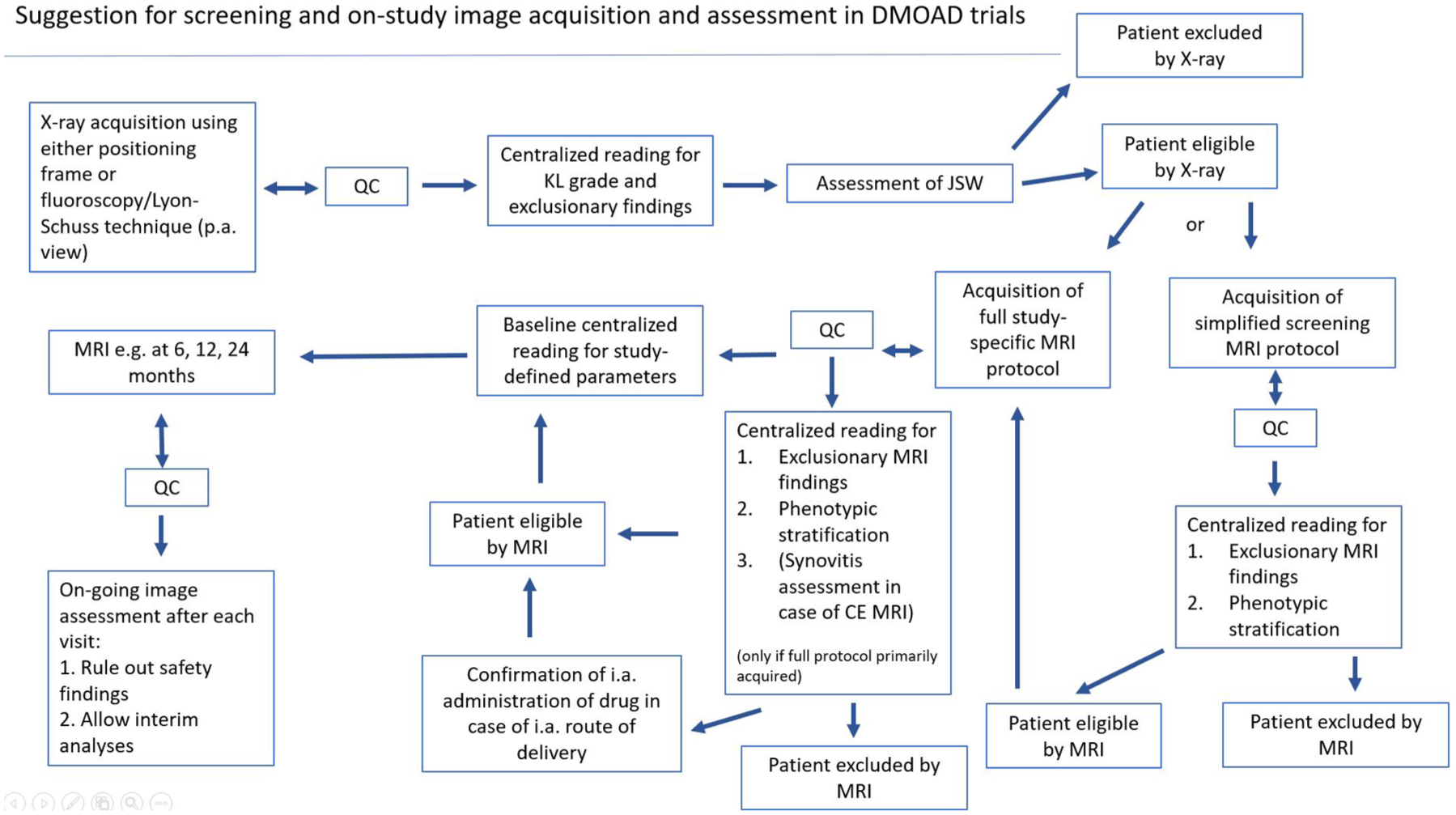
Flowchart of study inclusion using imaging in a DMOAD trial. At the beginning of the screening phase, X-rays are acquired and assessed for KLG and minimum JSW. If the patient is eligible, an abbreviated MRI is acquired to rule out exclusionary findings only visible on MRI and define a structural morphotype. If the patient is eligible, a full study protocol is acquired. Alternatively, a full protocol is acquired initially, with the risk that patients will be excluded despite having undergone an extensive MRI examination. In case of intra-articular drug delivery, confirmation of correct needle placement to rule out extra-articular administration of the active agent is needed. In case of an anti-inflammatory mode of action of a given compound, additional assessment of whole joint synovitis is needed to define the amount of synovial inflammation. MRIs are evaluated in an ongoing fashion to maximize sensitivity to change and allow for timely diagnosis of potential adverse safety events.
Given the described shortcomings of radiography, it seems highly unlikely that DMOAD effects will be shown by JSW assessment alone. However, it has to be acknowledged that responsiveness to change is comparable to quantitative MRI when X-rays are acquired in a highly standardized fashion, as in the OAI. 67 While Table 1 presents a comparative overview of the role of X-ray and MRI in the context of clinical DMOAD trials, Table 2 presents a broader comparison of the different imaging modalities with their respective advantages and limitations, and potential application in a clinical trial context.
Comparison of radiography versus MRI in clinical osteoarthritis trials.
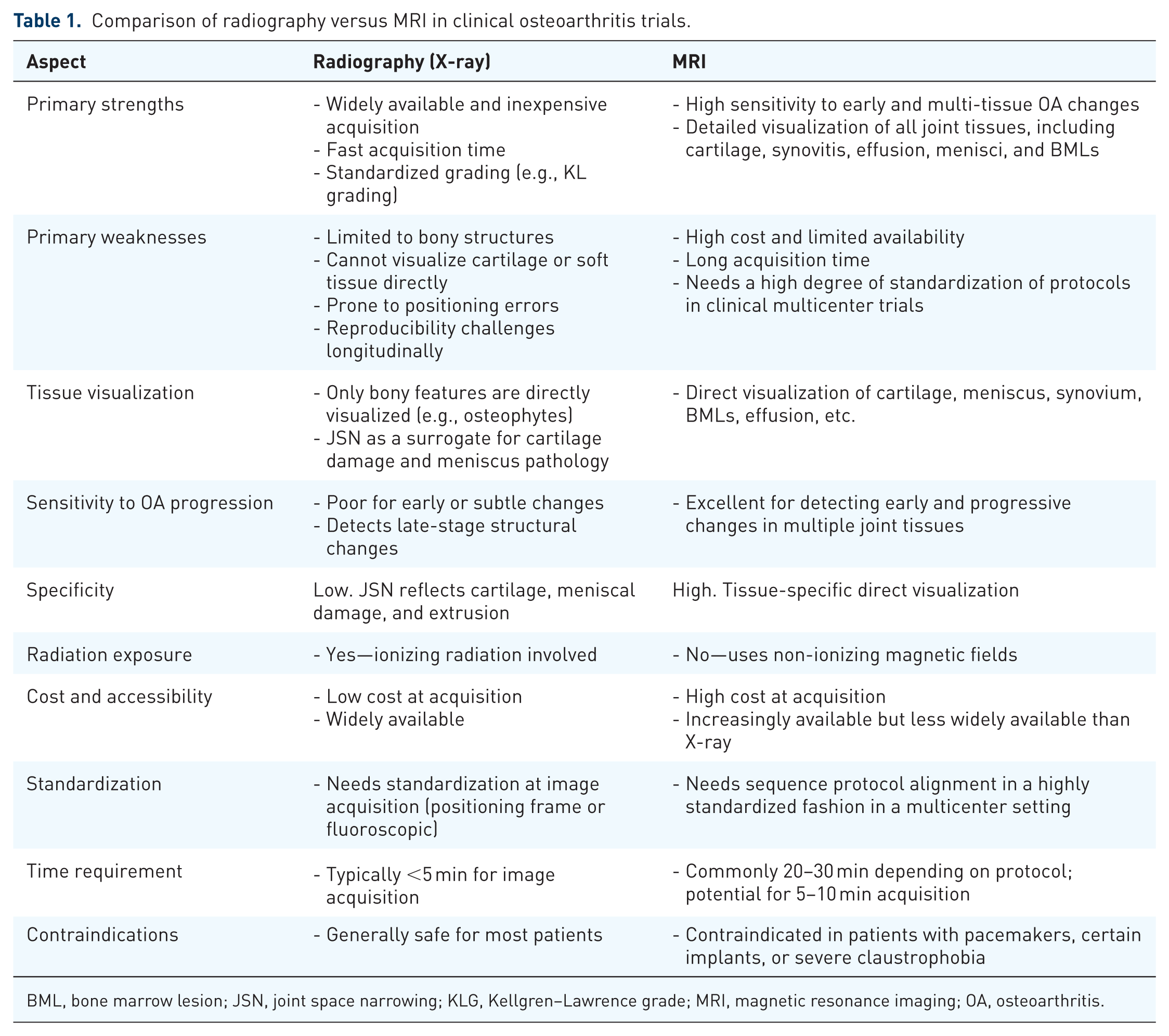
BML, bone marrow lesion; JSN, joint space narrowing; KLG, Kellgren–Lawrence grade; MRI, magnetic resonance imaging; OA, osteoarthritis.
Strengths and limitations of radiography, CT, MRI, ultrasound, and nuclear medicine techniques for use in clinical DMOAD trials.

DMOAD, disease-modifying OA drugs; MRI, magnetic resonance imaging; OA, osteoarthritis.
What is different in pain clinical trials compared to DMOAD trials?
In OA efficacy and pain studies, imaging serves distinct purposes. In DMOAD efficacy trials, image acquisition and evaluation are optimized to maximize sensitivity for detecting structural differences between treated and untreated participants over time. By contrast, pain trials focus on identifying structural tissue changes that either increase the risk of adverse outcomes (at eligibility screening) or warrant discontinuation of treatment during the study (safety monitoring). 68 Radiography typically reveals most joint abnormalities only in the late and irreversible stages of such structural pathologies, whereas MRI is a considerably more sensitive modality for detecting early signs of potential adverse events. Consequently, expert readers often have the option to request an MRI to confirm or exclude suspicious radiographic findings, or when there is a significant discrepancy between minimal or absent radiographic changes and the clinical presentation. 69
MRI simpler and more applicable: What’s next?
While we have seen marked advances in MRI technology in recent years, it remains speculative which of these developments will play a future role in clinical trials. MRI clinical trial protocols are commonly extensive and time-consuming. Image acceleration techniques will allow cost savings and increase patient comfort. 70 Cross-calibration and standardization of compositional MRI techniques as part of the Quantitative Imaging Biomarker Alliance (QIBA) initiative of the Radiologic Society of North America may help bring compositional MRI techniques eventually to the clinical trial arena. 47 Efforts are underway to establish direct synovitis visualization using non-enhanced MRI techniques.71–74 Finally, composite sequences such as the qDESS or others may allow for 3D quantification as well as compositional assessment using a single acquisition. 75 It is expected that we will see more development of such hybrid sequences in the future. 76
Current and future role of AI
Deep learning (DL) represents an advanced AI technique that utilizes hierarchical transformation of data through interconnected nonlinear layers. Currently, research is needed to evaluate the applicability of existing OA risk assessment models to the more heterogeneous MRI datasets commonly obtained in clinical trials. To date, nearly all DL risk assessment models have been developed and validated using the highly standardized OAI and Multicenter Osteoarthritis Study cohorts, which predominantly consist of middle-aged and older adults with high body mass index, thereby introducing potential bias.
AI algorithms can be trained to automatically quantify important structural features such as cartilage thickness, JSW, subchondral bone changes, osteophyte formation, and meniscal damage. 77 However, validation of these techniques and subsequent acceptance by regulatory authorities is needed. Another potential emerging role for AI is in imaging-based phenotyping and patient stratification at trial inclusion. Finally—albeit not supported by evidence to date—AI can be used to standardize image acquisition and analysis across different scanners and sites, ensuring consistency and reliability of imaging data.
Limitations
This perspective is not intended to serve as a systematic meta-analysis on the topic of imaging in clinical DMOAD trials. It should be acknowledged that enrichment of trial populations with the help of imaging—while feasible—may or may not result in cost-savings or decreased trial durations. MRI is particularly suited to help define potentially eligible patients and has also been used as an outcome measure in several studies. Other imaging modalities and methods—whether within the realm of MRI or beyond—like metabolic imaging including PET-MRI—may play an additional role in the future in selected scenarios. Studies referenced are relevant, but other work that is potentially of interest may not have been included, which is a result of the perspective format chosen. Table 3 presents an overview of prominent clinical trials of knee OA in the last 10 years and the role of imaging at inclusion or eligibility and as an outcome measure in those trials.
Selected DMOAD trials of the last 10 years.

Imaging included at eligibility/screening and as an outcome measure.
ACR, American College of Rheumatology; cMFTC, change in medial femorotibial cartilage thickness; DMOAD, disease-modifying OA drugs; ICRS, International Cartilage Repair Society; mJSW, minimum medial joint-space width; MRI, magnetic resonance imaging; OA, osteoarthritis; qMRI, quantitative MRI.
Summary
To date, not a single DMOAD has been approved by regulatory authorities in the United States and Europe. The reasons for this are multifold and include challenges related to patient selection based on imaging and application of imaging outcome measures that are either not sufficiently sensitive to change or are difficult to reliably reproduce longitudinally. Interventions and primary outcomes of trials with patients who have different underlying pathophysiology or exhibit different phases of disease progression must be differentiated, and modern imaging techniques will be able to achieve these goals. Biomarker qualification, including imaging, has been an international effort for several years and is currently still ongoing. 84
Conclusion
Once a more complete understanding of the development and progression of OA has been established and a set of clinically valid and responsive imaging biomarkers has been defined, hopefully future success rates of clinical trials of pharmacological interventions in OA will finally increase, particularly with the support of widespread application of MRI in clinical trials of knee OA.