
Abstract
Background:
Knee osteoarthritis (KOA) is associated with decreased quadriceps strength and decreased activation of central motor cortex. It is necessary to investigate intervention strategies that combine central and peripheral treatments.
Objective:
To assess the effectiveness of high-frequency repetitive transcranial magnetic stimulation (rTMS) in conjunction with quadriceps strength training for 12 weeks in the treatment of KOA.
Design:
Prospective, randomized, single-blind, comparative effectiveness study.
Methods:
In this 12-week randomized controlled clinical trial, 48 eligible patients were randomly allocated to either an experimental group or a control group. The experimental group underwent high-frequency rTMS in conjunction with quadriceps strength training, whereas the control group received sham rTMS alongside quadriceps strength training. The primary outcome measure was the visual analog scale (VAS), while secondary outcome measures included the University of Western Ontario and McMaster University Osteoarthritis Index (WOMAC), the peak torque of the extensor muscles, the peak torque of the flexor muscles, and the flexion–extension ratio. A two-way repeated measures analysis of variance with group as a group factor and time factor was used to calculate the effects of the interventions on all outcome measures.
Results:
Forty-four of the 48 patients who were allocated at random finished the study. Twelve weeks later, the VAS index in the experimental group decreased from 3.14 ± 1.13 to 1.36 ± 0.85, and that in the control group decreased from 3.23 ± 1.15 to 2.18 ± 1.40 (p < 0.05). At the same time, the WOMAC score, the peak torque of the extensor muscles, the peak torque of the flexor muscles, and the flexion–extension ratio were improved in the two groups (p < 0.05), and the experimental group was significantly better than the control group (p < 0.05).
Conclusion:
High-frequency rTMS combined with quadriceps strength training for 12 weeks can effectively improve pain, muscle strength and joint function in patients with KOA.
Trial registration:
Chinese Clinical Trial Registry (https://www.chictr.org.cn/) ChiCTR2300067617.
Keywords
Introduction
Knee osteoarthritis (KOA) is a prevalent geriatric degenerative disease of orthopedics. 1 With an aging population, the incidence is rising annually, imposing a significant societal burden. Currently, no treatment exists that can reverse the progression of KOA. Present therapeutic approaches primarily encompass exercise, pharmacotherapy, intra-articular injections, and surgical interventions.2,3 While these strategies can alleviate symptoms to some degree, they often fall short of fully restoring joint function.
Pain and functional impairment are the primary manifestations of KOA. Consequently, the primary objective in the treatment of KOA is to alleviate pain and enhance functional capacity. Quadriceps strength training has been proven to be significantly effective in treating pain and functional impairment of KOA patients. 4 However, some studies have pointed out that the improvement of muscle strength and pain in KOA patients by quadriceps strength training alone does not continue to increase over time, but enters a plateau period and gradually declines.5,6 This affects the patient's motivation and compliance to persist in training, making it difficult to achieve the expected therapeutic effect. This persistent quadriceps weakness in KOA patients is related to the reflex inhibition of the primary motor cortex (M1). 7 Abnormal sensory input from the joints causes changes in the excitability of spinal and supraspinal neurons. This results in an inhibitory state in the motor cortex, which affects the efficiency of muscle activation through dysfunction of neural pathways (e.g., the γ loop and flexor reflex), thereby reducing the effect of strength training.7,8 Therefore, strength training for KOA patients should focus more on the activation of relevant brain areas to improve the efficacy. Another study found that the pain intensity of KOA patients does not always correspond to the severity of the disease. This may be due to the fact that long-term pain input can cause changes in neuroplasticity and central sensitization. This results in a decrease in M1 excitability, which is related to intracortical inhibition and endogenous pain regulation defects.9,10 Therefore, central intervention, such as repetitive transcranial magnetic stimulation (rTMS), to activate inhibited brain areas has become a potential intervention strategy. Central intervention promotes the activation of brain functional areas and improves neural plasticity. Meanwhile, peripheral intervention strengthens the positive feedback and input of sensory and motor control patterns to the central nervous system, thereby further promoting the remodeling of brain function and achieving a dual rehabilitation effect.
Recently, with advancements in non-invasive brain stimulation technologies, rTMS has garnered attention due to its high safety profile and minimal side effects. rTMS is capable of non-invasively penetrating the skull to produce a magnetic field, which subsequently induces a weak electrical current within the cerebral cortex, thereby facilitating (high frequency stimulation, ⩾5 Hz) or inhibiting (low frequency stimulation, ⩽1 Hz) cortical excitability and regulating the function of the brain network. In many studies on rTMS treatment of fibromyalgia, it was found that central sensitization affecting the pain regulation system plays an important role in causing pain in fibromyalgia patients, 11 and M1 is crucial in top-down pain control and opioid release. 12 Therefore, rTMS can improve the central sensitization state by regulating the excitability of M1. In addition, rTMS can also play a role in the chronic pain of fibromyalgia patients by regulating brain areas related to the emotional components of pain and mediating the activation of the endogenous opioid analgesic system by the motor cortex. 13 KOA is a common chronic musculoskeletal pain disease, and the above mechanism may also support the treatment of KOA by rTMS. A preliminary case report on KOA has also demonstrated favorable therapeutic outcomes of high-frequency rTMS in both pain alleviation and functional improvement. 14
Building on the aforementioned findings, while quadriceps strength training and high-frequency rTMS individually exhibit therapeutic benefits for patients with KOA, the effectiveness of their combined application remains uncertain. Therefore, this study aimed to evaluate whether a combined intervention of active high-frequency rTMS and quadriceps strength training is more effective in restoring function and relieving pain in patients with KOA more than sham rTMS combined with quadriceps strength training. The outcomes of this research are anticipated to contribute novel insights into the treatment strategies for KOA.
Methods
Study design
A randomized, controlled, single-blind trial was undertaken at the Shanghai Seventh People’s Hospital to evaluate the efficacy of the treatment. This investigation received approval from the Research and Ethics Committee of Shanghai Seventh People's Hospital (2022-7th-HIRB-065) and was registered with the Chinese Clinical Trial Registry (ChiCTR2300067617) on January 13, 2023. Informed written consent was obtained from all patients prior to their inclusion in the study.
Participants
Participants were recruited between October and December 2023 from the Department of Orthopedics and Rehabilitation at Shanghai Seventh People's Hospital, as well as from the surrounding community. Figure 1 provided a thorough description of the patient recruitment and retention procedure. The recruitment procedures were meticulously managed by a designated individual to ensure strict adherence to protocol. When writing this manuscript, we followed the Consolidated Standards of Reporting Trials Statement. 15

A brief flowchart of subject recruitment.
Inclusion criteria
(1) KOA patients aged between 50 and 75 years; (2) patients who met the American College of Rheumatology and Kellgren–Lawrence imaging diagnostic grading criteria II–III; (3) patients with a disease duration of more than 3 months and not in the acute attack phase; (4) patients with a VAS pain score of ⩽5/10; (5) patients who voluntarily participated and signed the informed consent form.
Exclusion criteria
(1) Patients with a history of knee trauma (meniscus, ligament injury); (2) patients after knee surgery; (3) patients who suffer from other joint diseases such as rheumatoid arthritis; (4) patients with severe organ failure, severe cardiovascular and cerebrovascular diseases and other contraindications to exercise; (5) patients with malignant tumors.
Sample size calculation
This study used a two-way repeated measures analysis of variance (ANOVA) for sample size calculation, based on a 2-group (between-group factor) × 2 repeated measures (within-group factor: baseline, 12 weeks) design, and mainly tested the group × time interaction of the VAS pain scores of the two groups after 12 weeks of treatment. Using G*Power software (α = 0.05, power = 90%), according to previous studies, 16 the effect size η2 = 0.06 (Cohen's f = 0.26) and repeated measures correlation ρ = 0.5, and, considering sphericity correction (ε = 1), the total sample size was calculated to be 48 (including a 10% dropout rate).
Randomization and blinding
An independent researcher utilized Microsoft Excel 2013 to perform computerized randomization of the numbers. 17 The 48 participants who satisfied the inclusion criteria were randomly allocated in a 1:1 ratio to either the experimental group (HT + Q group) or the control group (ST + Q group). To prevent selection bias, an independent researcher unpacked the envelopes one at a time only after every participant has finished the baseline tests. Given the observable nature of the quadriceps strength training intervention, it is not feasible to blind the physical therapists and patients to the intervention allocation. Consequently, the blinding procedure is restricted to the evaluators responsible for data acquisition and the data analysts responsible for final statistical results, thereby minimizing implementation and measurement biases. Notably, these individuals will not participate in the recruitment of participants.
Interventions
All patients attended health education sessions. Considering the diversity of intervention tasks for patients, this study selected six physical therapists with a master's degree and more than 3 years of clinical work experience to carry out the intervention tasks. They were divided into three groups, with two people in each group, to complete the three tasks of health education, rTMS stimulation, and quadriceps strength training respectively, and the two people in the group cooperated to ensure the timeliness and accuracy of the intervention. All patient assessments were performed by an independent, senior assessor specializing in rehabilitation. All personnel involved in the trial completed uniform methodological training before the start of the study. In addition, considering the possible impact of drugs and other therapies (such as knee joint injection) on the outcome of this trial, all patients did not take any drugs during the intervention period. The pain or discomfort caused during the intervention period will be determined by whether the patient can relieve it by himself after resting to determine whether the patient will continue with the subsequent trial. If necessary, relevant measures such as suspending the trial and conducting symptomatic treatment will be taken to protect the rights and interests of the patient. Any discomfort or pain caused by the intervention during the study will be reported as an adverse event. Both groups underwent interventions five days a week for a duration of 12 weeks.
Health education
Health education is based on the core interventions recommended by the Osteoarthritis Research Society International (OARSI). 18 It covers (1) offering an educational booklet to patients, complete with illustrations and annotations for independent study at home, and (2) facilitating weekly in-person group sessions. The content of the health education encompasses recommendations for KOA common considerations, exercise methodologies, and advice on daily care practices.
rTMS therapy
The HT + Q group patients received active high-frequency rTMS with randomization of treatment order. This magnetic neuromodulation technique is recognized for its non-invasive nature and therapeutic potential in chronic pain management. 19 According to the International Federation of Clinical Neurophysiology recommendations, cortical stimulation employed a Super-Rapid Magstim apparatus (Yiruide Medical Equipment Co., LTD, Wuhan, China) equipped with a biphasic eight-shaped coil, positioned to map the cortical representation area (motor hotspot) corresponding to the ipsilateral knee's first dorsal interosseous muscle. 14 The rTMS was targeted at the motor cortex contralateral to the affected knee, such that left motor cortex stimulation was employed for cases of right knee arthritis. After the subject wears the positioning cap correctly, the researcher will install the eight-shaped coil 1 cm lateral and 1 cm posterior to Cz. Then, the optimal position and angle of the coil were determined by finding the minimum stimulator intensity necessary to evoke a motor response in the targeted lower limb. The resting motor threshold (rMT) is operationally defined as the minimum intensity required to elicit a response in at least 5 out of 10 consecutive stimuli, with each response measuring a minimum of 50 µV, when delivered to the designated “hot spot.” The rMT was evaluated at the commencement of each treatment session. The parameters for stimulation during each treatment session were as follows: a stimulation frequency of 10 Hz was employed, with each session consisting of 20 stimulation trains, culminating in a total of 1400 pulses. Each pulse train had a duration of 7 s, with an inter-train interval of 55 s. This treatment protocol was administered once daily, from Monday to Friday, at an intensity of 80% of the rMT, over a period of 12 weeks. 14 The ST + Q group patients received sham rTMS using identical parameters; however, the coil was positioned such that its edge was perpendicular to the head, with the remainder of the coil rotating 90° away from the scalp in the sagittal plane, to ensure that the noise of the stimulus during stimulation was similar.
Quadriceps strength training
Both groups engaged in quadriceps strength training utilizing a Biodex Multi-Joint System Model 3 isokinetic dynamometer (System 3, Biodex Corporation, Shirley, NY, USA). During the training sessions, participants underwent standardized positioning procedures: seated with thoracic, pelvic, and femoral stabilization via adjustable straps to minimize extraneous motion. The dynamometer's mechanical axis was precisely aligned with the knee joint's rotational center, maintaining a one-fist distance. The lever arm length was customized to individual lower limb dimensions, and resistance was applied anteriorly to the ankle joint. Meta-analytical evidence indicates that isokinetic training at 60°/s angular velocity can significantly enhance peak knee extension torque in KOA patients. 20 Consequently, the training protocol was conducted at an angular velocity of 60°/s, comprising 10 repetitions of knee flexion and extension exercises per set, with three consecutive sets constituting one session, and a 60-s rest interval between sets. This regimen was administered once daily, five times per week, over a 12-week period.
Outcome
Primary outcome
The visual analog scale (VAS) serves as a straightforward evaluative instrument for quantifying pain intensity in patients. 21 Typically, the VAS consists of a 10-cm line, with one extremity denoting “no pain” (0 points) and the opposite extremity indicating the “worst pain” (10 points). Patients are instructed by the assessor to place a mark on the line corresponding to their perceived pain level, thereby providing a quantifiable measure of pain intensity. The resultant pain score is directly proportional to the intensity of the pain experienced. The minimal clinically important difference (MCID) of VAS was 1.4 points. 22
Secondary outcome
Western Ontario and McMaster Universities Osteoarthritis Index
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scale is a reliable and valid questionnaire with 24 items across three subscales: pain (5 items), stiffness (2 items), and joint function (17 items), totaling 96 points. A higher score indicates a more severe condition. 23
Isokinetic muscle strength test
The Isokinetic muscle strength test (IMST) is a technique utilized to evaluate muscle strength and performance, characterized by its ability to maintain a constant speed of muscle contraction. This method allows for evaluation and training at varying speeds—low, medium, and high—while providing reliable data. Specifically, the IMST assesses maximum strength, or peak torque, and the flexion–extension ratio of muscles at a designated speed. 24 The procedure employs the Biodex System 3 isokinetic muscle strength testing system (Biodex Corporation, NY, USA) following routine calibration. Patients were seated with their knee joint secured in the testing position. The isokinetic contraction test was conducted using a concentric continuous contraction mode to evaluate the muscle strength of the affected side (all patients are right-legged), beginning with the extensor muscles followed by the flexors. Testing was performed at movement speeds of 60°/s (slow), 120°/s (medium), and 180°/s (fast), with a joint motion range set between 0° and 90° of knee flexion. 25 The peak torques of both the knee extensors and flexors in patients with KOA were measured during concentric contraction. Each contraction was repeated three times per group. The patients were asked to maintain maximum contraction throughout the test. To minimize potential interference with subsequent tests, patients were allowed to rest 3 min each time the test speed was adjusted. The highest value obtained in each test was recorded.
Safety and adverse events
The safety of treatment is evaluated by monitoring adverse events, specifically the number and severity of affected patients among all participants. When adverse reactions occur in the trial, they will be classified as mild, moderate, or severe according to the type of adverse reaction and the duration of symptoms after the stimulation is removed. Symptoms such as headache, scalp tingling, nausea, insomnia, and facial spasm that disappear on their own after the stimulation is removed are mild adverse reactions; mild adverse reactions are considered moderate adverse reactions when they persist for more than 24 h without relief; unbearable pain, epileptic seizures, and permanent functional impairment are considered severe adverse reactions. Recorded adverse events, 26 such as headaches, treatment site discomfort, and muscle cramps, were documented in the case report form and analyzed for potential links to the intervention.
Statistics
Statistical analyses were performed utilizing SPSS Statistics (v25.0, IBM Corp., Chicago, IL, USA). Normally distributed continuous measures are reported as mean ± SD, while nonparametric data are presented as median and interquartile range. Categorical data were summarized using frequency distributions. To assess changes over time and between groups, a two-way repeated measures ANOVA was conducted, with group (ST + Q vs HT + Q) as the between-subjects factor and time (baseline, 12 weeks) as the within-subjects factor. Chi-square tests evaluated categorical variable associations, with statistical significance defined as p < 0.05.
Results
Baseline characteristics of the patients
Out of 62 cases, 48 participants meeting the inclusion criteria were randomly assigned to either the experimental or control group. In the experimental group, one patient withdrew after symptom improvement, and another due to adverse reactions. In the control group, two patients withdrew due to physical discomfort. Ultimately, 22 patients from each group completed the trials. The average patient age was 64, with 77% female, 48% having right-side issues, 81% at K-L grade II, an average height of 163.77 cm, weight of 72.10 kg, BMI of 27.00, and 7.79 months since onset. All patients are right-legged. The groups did not exhibit any substantial differences in their baseline characteristics (p > 0.05), as shown in Table 1.
Baseline demographic characteristics of patients.

A difference was considered statistically significant if p < 0.05.
BMI, Body mass index; HT, high-frequency repetitive transcranial magnetic stimulation; K-L, Kellgren–Lawrence; Q, quadriceps strength training; ST, sham repetitive transcranial magnetic stimulation.
Primary outcome
Table 2 shows the score of the VAS between two groups at baseline and 12 weeks. A significant group × time interaction emerged for VAS scores (p = 0.034, η2 = 0.103). The simple effect results showed that there was no statistically significant difference between the two groups before treatment (p > 0.05, η2 = 0.002). However, the significant group differences were observed after treatment (p = 0.024, η2 = 0.116). In addition, the significant time effect was found in the score of VAS between the two groups (p < 0.001, η2 = 0.632).
Comparison of the score of the VAS between two groups at baseline and 12 weeks.

HT, high-frequency repetitive transcranial magnetic stimulation; Q, quadriceps strength training; ST, sham repetitive transcranial magnetic stimulation; VAS, Visual Analog Scale; Δ, difference compared to baseline.
Secondary outcome
Table 3 shows the score of the WOMAC between two groups at baseline and 12 weeks. Significant group × time interactions emerged for WOMAC scores (p < 0.001). The simple effect results showed that there was no statistically significant difference between the two groups before treatment (p > 0.05). However, the significant group differences were observed in the WOMAC-pain (p < 0.001, η2 = 0.327), stiffness (p = 0.020, η2 = 0.123), function (p < 0.001, η2 = 0.390), and total score (p < 0.001, η2 = 0.488) after treatment. Additionally, the significant time effect was found in the score of WOMAC between the two groups (p < 0.001).
Comparison of the score of the WOMAC between two groups at baseline and 12 weeks.

HT, high-frequency repetitive transcranial magnetic stimulation; Q, quadriceps strength training; ST, sham repetitive transcranial magnetic stimulation; WOMAC, Western Ontario and McMaster Index; Δ, difference compared to baseline.
Table 4 shows the peak torque of extensor muscles between two groups at baseline and 12 weeks. Significant group × time interaction emerged for peak torque of extensor muscles at angular velocities of 60°/s (p = 0.002, η2 = 0.211), 120°/s (p = 0.046, η2 = 0.091), and 180°/s (p = 0.005, η2 = 0.174). The simple effect results showed that there was no statistically significant difference between the two groups before treatment (p > 0.05). However, the significant group differences were observed at angular velocities of 60°/s (p = 0.019, η2 = 0.125), 120°/s (p = 0.045, η2 = 0.092), and 180°/s (p = 0.024, η2 = 0.116) after treatment. Additionally, the significant time effect was found in the peak torque of extensor muscles between two groups at angular velocities of 60°/s (p < 0.001, η2 = 0.826), 120°/s (p < 0.001, η2 = 0.727), and 180°/s (p < 0.001, η2 = 0.717).
Comparison of the peak torque of extensor muscles between two groups at baseline and 12 weeks.
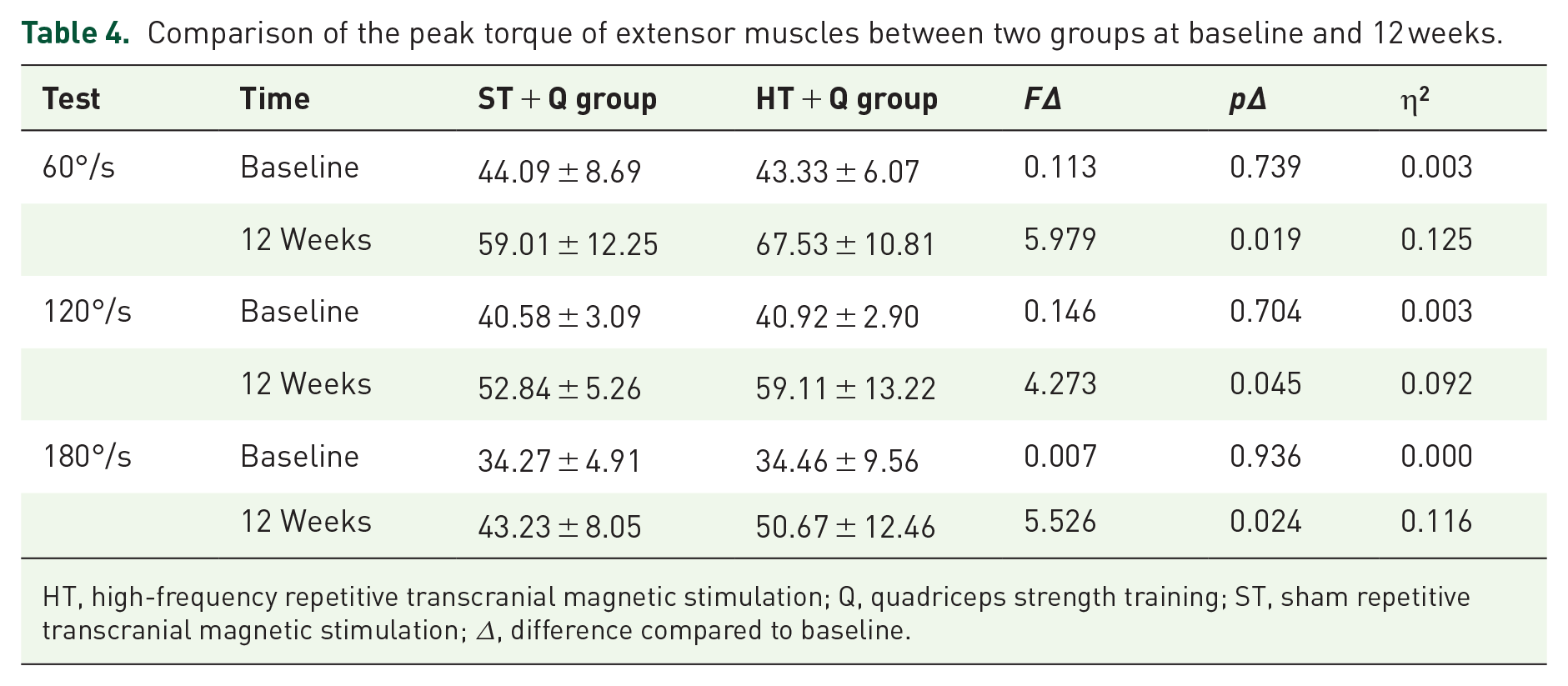
HT, high-frequency repetitive transcranial magnetic stimulation; Q, quadriceps strength training; ST, sham repetitive transcranial magnetic stimulation; Δ, difference compared to baseline.
Table 5 shows the peak torque of flexor muscles between two groups at baseline and 12 weeks. Significant group × time interaction emerged for peak torque of flexor muscles at angular velocities of 60°/s (p = 0.003, η2 = 0.194), 120°/s (p = 0.015, η2 = 0.133), and 180°/s (p = 0.001, η2 = 0.232). The simple effect results showed that there was no statistically significant difference between the two groups before treatment (p > 0.05). However, the significant group differences were observed at angular velocities of 60°/s (p = 0.018, η2 = 0.127), 120°/s (p = 0.020, η2 = 0.122), and 180°/s (p = 0.004, η2 = 0.184) after treatment. Additionally, the significant time effect was found in the peak torque of flexor muscles between two groups at angular velocities of 60°/s (p < 0.001, η2 = 0.839), 120°/s (p < 0.001, η2 = 0.757), and 180°/s (p < 0.001, η2 = 0.722).
Comparison of the peak torque of flexor muscles between two groups at baseline and 12 weeks.

HT, high-frequency repetitive transcranial magnetic stimulation; Q, quadriceps strength training; ST, sham repetitive transcranial magnetic stimulation; Δ, difference compared to baseline.
Table 6 shows the flexion–extension ratio between two groups at baseline and 12 weeks. A significant Group×Time interaction emerged for flexion–extension ratio at angular velocities of 120°/s (p = 0.001, η2 = 0.227), but no significant interaction at angular velocities of 60°/s and 180°/s . Before treatment, there was no statistically significant difference in the flexion–extension ratio between the groups of patients at 60°/s, 120°/s, and 180°/s angular velocities (p > 0.05). The significant group differences were observed at angular velocities of 60°/s (p = 0.016, η2 = 0.131), 120°/s (p = 0.003, η2 = 0.190), and 180°/s (p = 0.022, η2 = 0.119) after treatment. Additionally, the significant time effect was found in the peak torque of extensor muscles between two groups at angular velocities of 60°/s (p < 0.001, η2 = 0.875), 120°/s (p < 0.001, η2 = 0.904), and 180°/s (p < 0.001, η2 = 0.344).
Comparison of the flexion–extension ratio between two groups at baseline and 12 weeks.
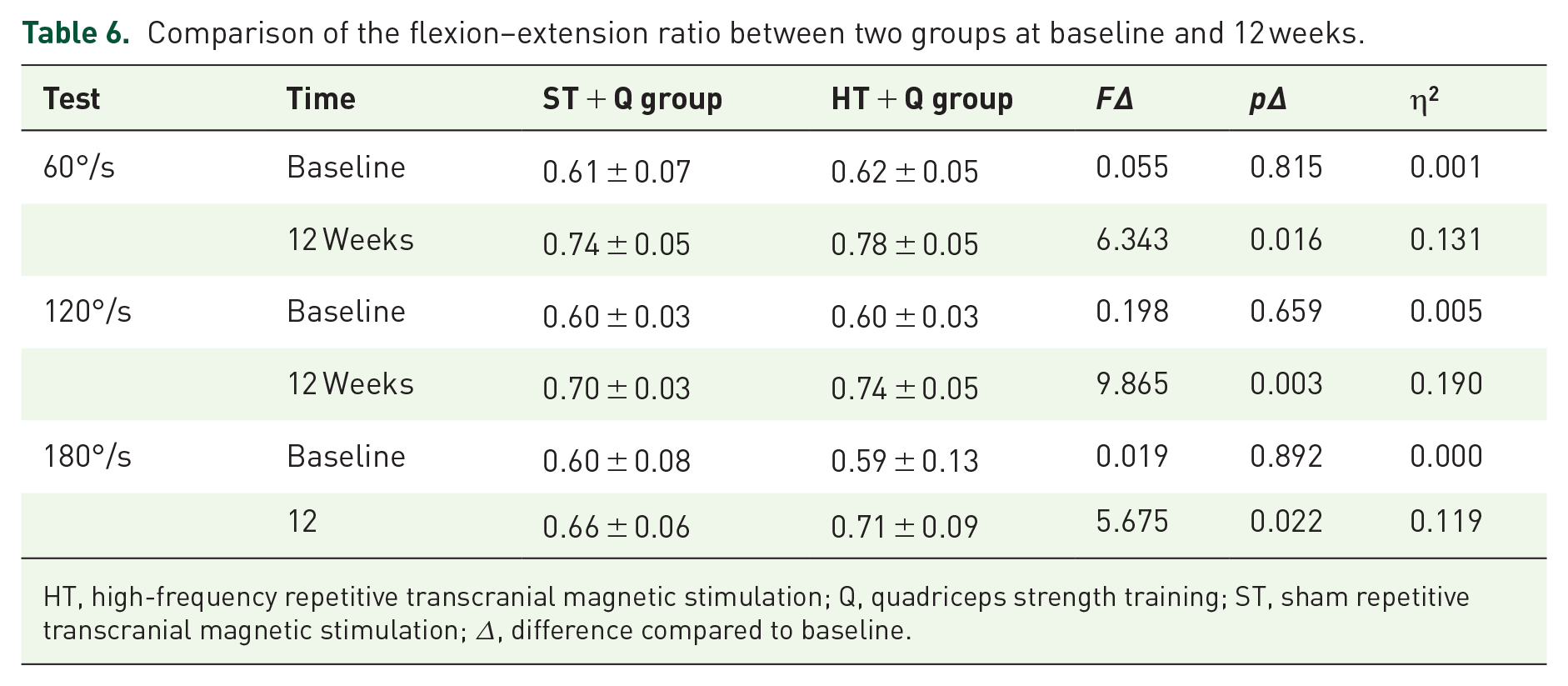
HT, high-frequency repetitive transcranial magnetic stimulation; Q, quadriceps strength training; ST, sham repetitive transcranial magnetic stimulation; Δ, difference compared to baseline.
Safety
During the study, one adverse reaction occurred in the HT + Q group, which was mainly manifested as scalp pain at the irritation site during treatment, and the pain gradually eased after the coil was removed; no adverse reactions were found in the ST + Q group. Importantly, neither group experienced any serious adverse events. Overall, both groups demonstrated a favorable safety profile, with no statistically significant difference in the incidence of adverse events (p > 0.05).
Discussion
The purpose of this study was to explore the effectiveness of high-frequency rTMS combined with quadriceps strength training on KOA at 12 weeks of treatment. The results showed that 12 weeks of high-frequency rTMS combined with quadriceps isometric strength training can effectively improve patients' pain, muscle strength, and joint function levels.
KOA is frequently regarded as a peripheral condition, characterized by joint pain, stiffness, swelling, and functional limitations resulting from the degradation of articular cartilage. 27 Pain is a predominant concern for individuals with KOA, and persistent chronic pain can substantially diminish their quality of life. Although earlier research has posited that pain in KOA patients arises from peripheral afferent nerve damage, the perception of pain does not consistently relate to the structural alterations observed in imaging studies. 28 This discrepancy has led to a re-evaluation of the underlying causes of pain in KOA patients. Recent investigations suggest that this inconsistency may be attributed to maladaptive changes within the pain processing centers, associated with central sensitization and inadequate endogenous pain inhibition.29,30 The persistent nociceptive input from the damaged joint, coupled with insufficient endogenous pain inhibition, is believed to enhance the excitability of neurons within the central pain pathways, resulting in hyperalgesia among KOA patients.31,32 Furthermore, severe pain and impaired motor performance in KOA patients have been linked to reduced excitability of the primary motor cortex (M1).31,33,34 In patients with KOA, pain can lead to reflexive inhibition of the primary motor cortex, diminish the excitability of the M1 nerve, and induce detrimental neuroplastic alterations. These changes hinder the autonomous activation of the quadriceps muscle, consequently impairing its contraction capability. Thus, enhancing the excitability of the M1 is critically important for the effective treatment of KOA.
The results of this study suggest that a combined intervention of high-frequency rTMS and quadriceps strength training was superior to sham rTMS with quadriceps strength training. The findings demonstrate synergistic therapeutic benefits when combining neuromodulatory interventions with peripheral muscle rehabilitation. The experimental protocol yielded superior outcomes in both pain mitigation and functional recovery compared to sham-controlled conditioning, consistent with prior investigations employing cortical stimulation techniques. Cheng et al. respectively divided the 160 KOA patients into hip abduction strength training combined with rTMS and celecoxib groups for clinical intervention. 35 Upon completion of 4 weeks of treatment, the outcomes revealed that the strength training combined with M1 transcranial magnetic stimulation intervention group was superior to the celecoxib group in terms of pain relief, muscle strength, and improvement in joint function. 35 A case study investigated monthly 10 Hz motor cortex rTMS in a chronic KOA patient with central sensitization, demonstrating marked alleviation of neuropathic pain components, psychological comorbidities, and functional disability, suggesting its potential as a non-invasive neuromodulatory strategy for central pain mechanisms refractory to conventional therapies. 14 In another study using non-invasive brain stimulation techniques to intervene in KOA, Rahimi et al. randomized 80 patients into four groups, each of which was subjected to tDCS stimulation of the M1, primary sensory cortex, dorsolateral prefrontal cortex, and sham stimulation, respectively, in conjunction with conventional physical therapy. 36 The results showed that tDCS combined with exercise therapy was equally effective in improving pain and functional levels in patients with KOA. Notably, studies have shown that compared to tDCS, rTMS directly activates the cortex through electromagnetic induction, precise M1 targeting, and sustained neuroplasticity effects, synergistically addressing central sensitization and peripheral muscle dysfunction, demonstrating superior clinical efficacy, and has been widely applied in pain management of various diseases related to central sensitization.37,38
The knee flexion/extension strength ratio (hamstring/quadriceps ratio, H/Q) represents the ratio of hamstring to quadriceps strength. The ratio of hamstring to quadriceps peak torque is often used to reflect the ability of the two muscle groups to maintain knee stability, but there is no consensus on the research on the knee flexion/extension ratio. Affected by factors such as angular velocity, group differences, and the use of gravity compensation, the range of H/Q is usually reported to be 0.43–0.90. Among them, the H/Q of the elderly group is higher than that of the young group. This is because the strength of the hamstrings and quadriceps decreases with age, and the degree of decline in quadriceps strength is greater than that of the hamstrings. 39 Currently, 0.6 is generally accepted as the standard value for measuring muscle balance around the knee joint, 40 However, the flexion–extension ratio of the two group patients before treatment was closer to 0.6 than after intervention, which was lower than the H/Q of the healthy elderly population. This may be related to the pain and joint-induced muscle inhibition in KOA patients. 41 Arthrogenic muscle inhibition is a central reflex inhibition caused by intra-articular injury and abnormal proprioceptive afferent nerves, 42 involved in the flexion reflex pathway, affecting both quadriceps and hamstring strength. 43 Therefore, the flexion–extension ratio of KOA patients is lower. Biomechanical analysis showed that the flexion–extension ratio of both groups at each angular velocity increased after the intervention, and the flexion–extension ratio in the experimental group were increased compared with the control group, indicating that the dynamic joint stability mechanism was enhanced, which may be mediated by cortical recombination and peripheral neuromuscular adaptation. These values are closer to the high H/Q for healthy aging populations, indicating that the physiological muscle coordination pattern previously disrupted by the arthrogenic inhibition pathways was partially restored, and the combination therapy was significant in improving knee stability in KOA. A previous study showed that rTMS applied to M1 improved upper limb spasticity in stroke patients by modulating the flexion reflex. 44 Another study on spasticity in patients with pre-traumatic spinal cord injury with rTMS concluded that M1 stimulation could improve patients’ spasticity by improving contraction and relaxation of both agonist and antagonist muscles mediated by reciprocal inhibition, consistent with the neural mechanisms involved in Arthrogenic Muscle Inhibition (AMI) in patients with KOA. 45 The improvement in H/Q may be related to the elimination of AMI. rTMS acting on M1 may be mediated by the flexion reflex, or Iareciprocal inhibition modulates the contraction of the patients’ quadriceps and relaxation of the hamstrings, thereby improving their flexion–extension ratio.
In addition, during the course of this study, only one mild adverse reaction occurred in the experimental group during the treatment, and the scalp pain was eliminated after the coil was removed. No serious adverse reactions were observed during the 12-week intervention period, demonstrating that rTMS in conjunction with quadriceps strength training is a safe and effective therapeutic strategy for KOA. However, the mechanism of its efficacy is still unclear, which may be the result of the combined action of central regulation and peripheral intervention. Central regulation reduces pain and increases the activation of motor units by enhancing the excitability of the stimulated area of the brain, while peripheral intervention reduces joint damage and inflammation by enhancing muscle strength and improving biomechanical state. This dual mechanism of action enables this combined treatment to significantly improve the joint function and pain of KOA patients.
However, there are some limitations to this study. Although this study was originally designed to blind both the subjects and the assessors, the placement method of rTMS used in the placebo control group was significantly different from that in the experimental group, resulting in the risk of the trial being unblinded. Therefore, this study was only reported as the assessor-blind method, which has a certain risk of bias. At the same time, since an isokinetic muscle tester was used for patient assessment and intervention, the baseline pain level of the included patients was VAS ⩽ 5 points, which to some extent reduced the universality of the patient population. Furthermore, the primary outcome measure of this study was pain, but the pain level of KOA patients may show different results at different times of the day, such as lighter in the morning and heavier in the evening. This study did not set a unified intervention time, which may have a certain impact on the results.
In conclusion, this study supports the effectiveness of quadriceps strength training combined with active high-frequency rTMS in treating KOA patients, offering a novel perspective on KOA management. Nonetheless, several aspects warrant further investigation. Specifically, the optimal parameters for rTMS, including frequency, intensity, and duration, remain to be determined, and the ideal exercise regimen for quadriceps strength training requires additional research. Furthermore, examining the differential efficacy of this combined approach in KOA patients with varying severity levels constitutes a crucial avenue for future inquiry. Moving forward, we intend to investigate the application of this combined method in KOA patients at different stages and evaluate its long-term effectiveness.
Conclusion
This study demonstrated that adding high-frequency rTMS to quadriceps strength training for 12 weeks can effectively improve pain, muscle strength, and joint function in patients with KOA. Although the mechanism is still unclear, the peripheral combined with central intervention strategy seems to work both peripherally and centrally, exerting a positive effect on pain and function in KOA.