
Abstract
Background:
Autoimmune thyroid disease (AITD) is the commonest autoimmune disease. Although viewed as a classic form of single-organ autoimmunity, AITD is increasingly associated with non-thyroid sequelae including musculoskeletal manifestations and chronic pain syndromes. However, large population-based studies are needed.
Objectives:
To examine the relationships between chronic hand pain and the AITD autoantibodies, anti-thyroid peroxidase antibody (TPOAb), and anti-thyroglobulin antibody (TgAb), in the Third National Health and Nutrition Examination Survey (NHANES III).
Design:
This is a cross-sectional study.
Methods:
We examined data from NHANES III on 4820 persons aged 60 years or older with respect to hand pain and its association with TPOAb and TgAb. Log-binomial regressions were fit to examine the associations between the anti-thyroid autoantibodies and hand pain.
Results:
Positive TPOAb was associated with a higher prevalence of hand pain than negative TPOAb [prevalence ratio (PR) = 1.158, p = 0.048] in the unadjusted model. This association was no longer significant after controlling for age, body mass index, gender, and diabetes (p = 0.313). When positive TPOAb was considered as a categorical variable with four levels, the highest quartile was associated with hand pain in the unadjusted (PR = 1.489, p = 0.005) and adjusted models (PR = 1.325, p = 0.042). There was no significant association between TgAb and hand pain when covariates were controlled for.
Conclusion:
TPOAb may be associated with the presence of chronic hand pain in persons aged over 60 years, especially at higher serum levels.
Keywords
Introduction
The anti-thyroid peroxidase antibody (TPOAb) is associated with clinically significant autoimmune thyroid disease (AITD) and is present in over 90% of hypothyroid Hashimoto’s thyroiditis patients and about 70% of those with hyperthyroid Grave’s disease.1–3 Hypothyroidism and hyperthyroidism have been estimated to affect 4.6% and 1.3% of the US population, respectively. 4 Although classically viewed as a form of single-organ autoimmunity, AITD is increasingly found to be associated with musculoskeletal manifestations and chronic pain disorders including peripheral osteoarthritis, spinal degenerative disc disease, and chronic widespread pain, often fulfilling criteria for fibromyalgia syndrome.5,6 In a significant percentage of the population with anti-thyroid antibodies, the presence of these rheumatic syndromes occurs in the absence of overt thyroid dysfunction.7–9 The anti-thyroglobulin antibody (TgAb) was prevalent in 11.5% of the United States (US) population in the Third National Health and Nutrition Examination Survey (NHANES III), while the TPOAb, also referred to as the anti-microsomal antibody, occurred in about 13% of a sample of 17,353 persons aged ⩾12 years. 4
Hand pain is a prominent manifestation of multiple autoimmune diseases and is frequently the initial presentation of both arthritic and chronic widespread pain syndromes.10–12 We therefore examined the question of chronic pain in AITD by focusing on chronic hand pain in particular in association with the TPOAb and TgAb using NHANES III because data were collected for symptoms of hand osteoarthritis including hand pain and the anti-thyroid antibodies in participants over the age of 60 years. We hypothesized that there might be a relationship between hand pain and the TPOAb or TgAb as markers of the presence of AITD. Furthermore, if the relationships were immunologic, there might be an association of hand pain with markers of systemic inflammation like C-reactive protein (CRP), but not necessarily with thyroid hormonal function.
Materials and methods
Data source
Data were obtained from both phases I (1988–1991) and II (1991–1994) of NHANES III, which involved complex, multi-stage, stratified, clustered national probability samples of civilian, non-institutionalized persons in the US population, aged 2 months and older, oversampling children aged 2 months to 5 years, persons aged 60 years and over, and Black non-Hispanic and Mexican American persons. The Household Adult Questionnaire (HAQ) was administered at home to adults aged 17 years and over, and included questions related to joint pain and arthritis for participants aged 60 years and older. 13 The home interview was followed by the Mobile Examination Centers (MEC) portion of the study which included a physician’s examination of joints and obtaining of hand radiographs. The operation and procedures for NHANES III including the consent process have been described in detail. 13 Participant consent for publication was not required and the data source exists in the public domain at https://wwwn.cdc.gov/nchs/nhanes/nhanes3/default.aspx. The conduct of this study followed the recommendations of the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement checklist 14 (STROBE Checklist; Supplemental material).
Study population
There were 33,994 participants of an original sample of 39,695 interviewed in NHANES III. One focus of the study was to obtain data on arthritis in persons over the age of 60, all of whom completed the HAQ and some of whom were invited for the MEC portions of the study. Phases I and II had 6596 participants in that age group. There were 4820 persons for whom hand pain was recorded and the data were available for the anti-thyroid antibodies (Figure 1).

Flow diagram of study participant selection process.
Outcome measures
The presence of chronic hand pain was the primary outcome measure and was defined as the response yes, to the question, ‘Have you ever had pain in your hands on most days for at least 6 weeks? This also includes aching and stiffness’, obtained in the musculoskeletal conditions section G of the HAQ.
Covariates
Covariates were selected based on the results of our primary analysis and possible confounders reported in the literature. They included age, gender, race/ethnicity, education, occupation, current cigarette smoking, body mass index (BMI), CRP, diabetes, and thyroid disease.15–17 Data were obtained by participant interview and examination at the home interview or MEC portions of the study.
Demographic information
Race/ethnicity was defined as non-Hispanic White, non-Hispanic Black, Mexican American, and others (defined as other Hispanics, Asians, and Native Americans in NHANES III). Education was dichotomized into ⩽12 years and > 12 years. Occupation was defined as what kind of work the respondents were doing the longest out of all the paid jobs or businesses they had ever had. Over 40 types of occupations were catalogued (variable HAS17R) and were classified as manual workers (types 8 and 19–40) and non-manual workers (the other types). 18 Participants who had never worked or were in the military were considered non-manual workers.
Clinical covariates
A detailed report on the NHANES III laboratory methods for clinical variables has been published and is available online. 19 The main independent variables were TPOAb, which was assayed by a highly sensitive, direct radioimmunoassay system based on the use of a highly purified, stable preparation of 125I-labeled thyroid peroxidase enzyme with positive levels ⩾0.5 U/mL, and TgAb, which was assayed by a highly sensitive, direct radioimmunoassay system based on the use of a highly purified, stable preparation of 125I-labeled thyroglobulin and was positive with levels ⩾1.0 U/mL. 19 The assays were not changed during the study and reference levels of the thyroid autoantibodies were comparable throughout. Other variables were assayed and reported as previously briefly described. 18 CRP was measured by latex-enhanced nephelometry with a reported detection range of 0.21–25.2 mg/dL. 19 The presence of thyroid disease was identified as the answer ‘yes’ to the questions ‘Has a doctor ever told you that you had goiter?’ or ‘Has a doctor ever told you that you had other thyroid disease?’ Diabetes in this analysis was defined by self-report from the question, ‘Have you ever been told by a doctor that you have diabetes or sugar diabetes?’ in the home interview. BMI was derived from weight and height measured from the MEC portion of the study. Smoking was defined as the response yes to the question ‘Do you smoke cigarettes now?’
Statistical methods
There were 1.16% missing values in the dataset on demographic and clinical variables for 4820 participants. Multiple imputation using fully conditional specification in the chained equation approach was used to replace the missing data on several demographic and clinical variables, such as education, smoking, BMI, diabetes, thyroid disease, T4, and CRP. Frequencies, estimated percentages (weighted %), and standard error of the percentages were reported on the categorical variables. Relative standard error >30% criterion was used to mark potential unreliable or suppressed percentage estimates. 20 Median and ranges were reported on the continuous variables. The analyses were generated on the five pseudo-complete datasets, and the results were combined using Rubin’s rules. 21 Several log-binomial regression models were conducted to examine the associations between TPOAb, TgAb, and hand pain. According to preliminary analysis, age and BMI were significantly and positively correlated with TPOAb and TgAb. Females were more likely to report hand pain and had higher levels of TPOAb than males, and diabetics participants were more likely to report hand pain. Those covariates, which have also been suggested to associate with hand osteoarthritis in the literature, were therefore included as covariates in the model. 18 The adjusted prevalence ratio (PR) and 95% confidence interval (CI) were reported to estimate the effects of predictors. Age was normalized and interpreted as every standard deviation change in age on hand pain incidence. All data were analyzed using SAS, version 9.4 (SAS Institute Inc., Cary, North Carolina, U.S.) survey procedures, taking into account the cluster, strata, and MEC-examined final sampling weights adjusted for interview non-response, MEC examinations non-response, non-coverage, and differential selection probabilities on the population by age, race, household size, self-reported health status, etc. A two-sided p < 0.05 was considered statistically significant.
Results
Sample characteristics
Approximately 18.8% of participants reported hand pain. Their TPOAb levels ranged from 0.30 U/mL (negative TPOAb) to 3000 U/mL (mean = 11.98 U/mL), and TgAb ranged from 0.70 U/mL (negative TgAb) to 3000.00 U/mL (mean = 12.59 U/mL). Most participants had negative TPOAb (81.2%) or negative TgAb (84.8%). More detailed descriptive variable information is summarized in Table 1. All descriptive statistics were run on the original dataset without missing data imputation to reflect the actual weighted characteristics of the US population aged 60 years and older.
Descriptive statistics for sample characteristics.
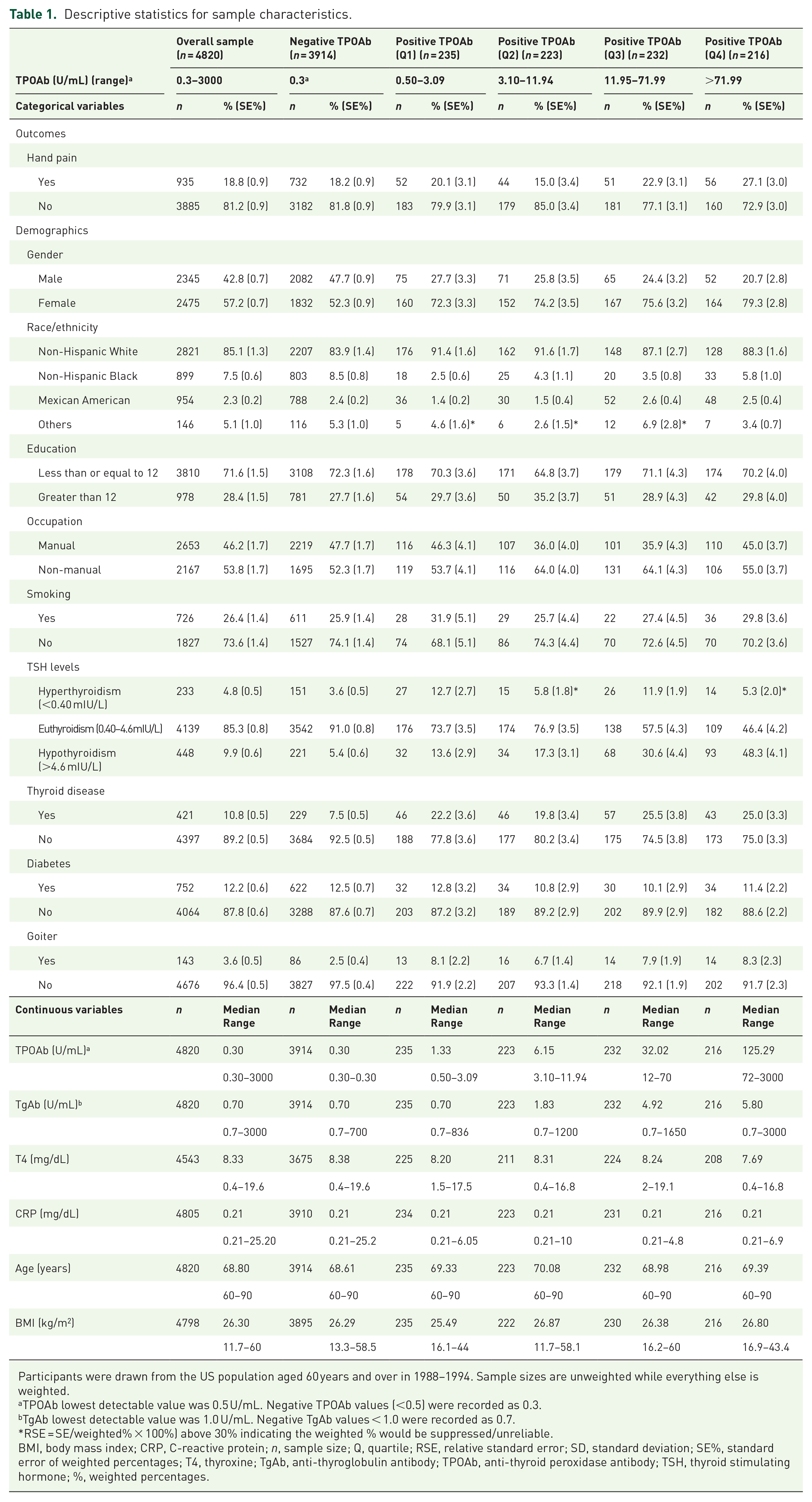
Participants were drawn from the US population aged 60 years and over in 1988–1994. Sample sizes are unweighted while everything else is weighted.
TPOAb lowest detectable value was 0.5 U/mL. Negative TPOAb values (<0.5) were recorded as 0.3.
TgAb lowest detectable value was 1.0 U/mL. Negative TgAb values < 1.0 were recorded as 0.7.
RSE = SE/weighted% × 100%) above 30% indicating the weighted % would be suppressed/unreliable.
BMI, body mass index; CRP, C-reactive protein; n, sample size; Q, quartile; RSE, relative standard error; SD, standard deviation; SE%, standard error of weighted percentages; T4, thyroxine; TgAb, anti-thyroglobulin antibody; TPOAb, anti-thyroid peroxidase antibody; TSH, thyroid stimulating hormone; %, weighted percentages.
Anti-thyroid peroxidase antibody
In the unadjusted model examining TPOAb, older adults with positive TPOAb had a higher prevalence of hand pain than those with negative TPOAb (PR = 1.158, 95% CI: 1.00–1.34, p = 0.048). However, when age, BMI, gender, and diabetes were controlled for in the regression model, this association was no longer significant (p = 0.313) (models 1 and 2 in Table 2).
Associations between anti-thyroid antibodies and hand pain.

Compared with negative cases.
Compared with male.
Compared with non-diabetes.
BMI, body mass index; CI, confidence interval; LL, lower limit; PR, prevalence ratio; Q, quartile; SE, standard error; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; UL, upper limit.
Significant values are in bold text.
To further investigate a potential dose-dependent relationship between TPOAb and hand pain, persons with positive TPOAb levels were stratified into quartiles. The results, in models 3 and 4 of Table 2, suggest that older adults with the highest TPOAb (4th quartile) had a higher prevalence of hand pain than those with negative TPOAb levels in the unadjusted model (PR = 1.489, p = 0.005) and when age, BMI, gender, and diabetes were controlled for (PR = 1.325, p = 0.042). When treating TPOAb as a continuous variable, CRP was significantly positively related to TPOAb (R2 = 0.008, p < 0.001). There was no significant relationship between CRP and thyroid stimulating hormone (TSH). A significantly greater proportion of older adults with a history of thyroid disease reported hand pain (26.6%) than the those without thyroid disease (17.9%) (p = 0.009). Hand pain was not significantly related with TSH and serum thyroxine (T4) levels (data not shown).
Anti-thyroglobulin antibody
The results for the TgAb are displayed in models 5–8 of Table 2. Significantly higher hand pain was only found when comparing positive TgAb with negative TgAb without including any covariates (model 5; PR = 1.231, p = 0.010). CRP was also positively related to TgAb (R2 = 0.002 p < 0.001). Although the results were significant, the R coefficients indicated their relationships were weak. There were no significant differences between hand pain and any level of TgAb examined as a multi-categorical variable (all ps > 0.05) (models 7 and 8; Table 2). The percentage with hand pain in each category of TPOAb levels and TgAb levels showing the dose relationship is displayed in Figure 2(a) and (b).

Prevalence of hand pain by (a) TPOAb levels and (b) TgAb levels.
Discussion
We explored the association between the anti-thyroid antibodies TPOAb and TgAb, and chronic hand pain in the US population aged 60 years and older in 1988–1994 using NHANES III. Our findings suggest that higher TPOAb levels may be associated with the presence of hand pain in persons over the age of 60 years. The association was strongest in the highest quartile of TPOAb-positive individuals whose antibody concentrations were ⩾72 U/mL, and most pronounced in those with concentrations ⩾324 U/mL in whom 42.24% (weighted %) experienced hand pain (data not shown). TgAb was not associated with hand pain and has not been shown to be pathologically linked to thyroid or extra-thyroid disease. 22 The group at highest risk in the 75–100 percentile constituted 4.24% (weighted %) of the study population over the age of 60 years and represented a combined population of 1.7 million (M) out of 40.1 M over the age of 60 years in the general civilian, non-institutionalized population of 251.1 M at the time of NHANES III (accessed at https://wwwn.cdc.gov/nchs/nhanes/ResponseRates.aspx). We estimate that this translates to about 3.2 million persons using the current general population estimate in 2020 of 331,449,281, of whom about 23% are aged older than 60 years, who may be at risk of experiencing chronic hand pain associated with the presence of high-titer TPOAb, assuming there has been no change in the age frequencies of the TPOAb over time. 23
The possibility that Hashimoto’s disease may exert profound autoimmune features has been explored in a recent systematic review in which multiple non-endocrine associations of the disease were described. 22 Recently, Guldvog et al. reported a cohort of 150 patients aged 18–79 years with persistent symptoms related to the presence of AITD with euthyroid status while receiving hormone replacement therapy, who were offered total thyroidectomy or medical management with hormone substitution to secure euthyroid status in both groups. 24 All participants had TPOAb levels >1000 IU/mL at study entry. The symptom complex reported included profound fatigue, poor sleep quality, muscle and joint tenderness, and dry mouth and eyes. Multiple outcome measures of physical, emotional, pain, fatigue scores, and general health showed improvement in the thyroidectomy group. The median baseline TPOAb level in the surgical group fell from 2232 IU/mL to 152 IU/L 18 months after surgery versus 1300 IU/mL in the medical treatment group, with attendant significant improvements in multiple outcome measures including the bodily pain score. 24 We suspect that hand pain could have been part of the symptom complex in these subjects with very high serum concentrations of TPOAb, and the improvement in symptoms with the fall in TPOAb levels in the thyroidectomy group lent support to there being a possible immunological mechanism to pain generation. We have reported previously an association of the TPOAb with knee chondrocalcinosis which may lend further support to its possible role in non-thyroid disorders including arthritis and pain syndromes. 18 A report by Dahaghin et al. which found hand pain in 16.9% of an elderly population aged 55 years and over in the Netherlands noted the contribution of thyroid disease to hand pain supporting our findings. 25 The enrichment of hand pain in the female population was also noted. However, the authors did not document specific associations with thyroid function and did not assess anti-thyroid antibody status in their patients.
Our analysis establishes a relationship with the TPOAb but does not identify a cause for hand pain. The possible sources of pain could include joint pain through degenerative joint disease, frank inflammatory arthritis, or neuropathic pain and would need to be investigated further in future studies.8,26,27 Ancillary studies like musculoskeletal ultrasound, nerve conduction studies, and skin biopsies for small fiber neuropathy would be needed to better understand the pathogenesis of the hand pain. 28 We briefly explored a possible role of inflammation by examining the association of TPOAb with CRP. Although there was a significant relationship the correlation was weak with an R2 value of 0.008 and this was only seen if TPOAb was analyzed as a continuous variable and not seen when analyzed as a binary variable, thus providing no conclusive evidence for a role of inflammation. However, the association of hand pain with reported thyroid disease but not with TSH or T4 levels specifically supports the hypothesis that the mechanism of injury may be immunologic and not hormonally mediated. The role of AITD-associated hand pain in the symptom complex of rheumatic syndromes including fibromyalgia, hand osteoarthritis, and inflammatory arthritis would need to be explored in future studies. 5
Our study has some limitations. The cross-sectional design of NHANES III only allows tests of association and not of causation and was not amenable to rigorous testing of the role of inflammation and specific causes of hand pain such as neuropathy, arthritis, or fibromyalgia. The data for arthritis in NHANES III were restricted to the persons aged over 60 years and prevent generalization of the findings to other age groups. Future prospective studies would be needed to corroborate the results and investigate a possible causative association. The generalizability of the data may be handicapped by the methodology used. NHANES III used a highly sensitive radioimmunological assay for measuring the anti-thyroid antibodies. The use of modern chemiluminescent assays may give significantly different population views of the prevalence and incidence of the anti-thyroid antibodies. Continuing international standardization of these assays would help to improve the interpretation of future epidemiologic studies. 29
Conclusions
In conclusion, TPOAb may be associated with pain syndromes and the presence of chronic hand pain and should be measured as part of the assessment of rheumatic disorders. 30 Furthermore, the presence of hand pain can obscure the disease assessment of well-defined clinical syndromes such as rheumatoid arthritis and psoriatic arthritis.31,32 Thus, the potential for AITD to modulate the clinical presentation of autoimmune inflammatory diseases should be considered. Future work would need to determine clinically relevant TPOAb levels which are likely to vary depending on the diseases studied and end-organs involved.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X231154984 – Supplemental material for Association of the anti-thyroid peroxidase antibody with chronic hand pain in older adults in the Third National Health and Nutrition Examination Survey: a cross-sectional study
Supplemental material, sj-docx-1-tab-10.1177_1759720X231154984 for Association of the anti-thyroid peroxidase antibody with chronic hand pain in older adults in the Third National Health and Nutrition Examination Survey: a cross-sectional study by Clement E. Tagoe, Wanyi Wang and Kamil E. Barbour in Therapeutic Advances in Musculoskeletal Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.