
Abstract
Background:
Acute anterior uveitis (AAU) is the most frequent extra-musculoskeletal manifestation in spondyloarhtritis (SpA). Previous data on AAU focused on axial disease; therefore, it is not well known whether the clinical characteristics of patients with AAU and recurrent AAU differ between patients with axial and peripheral SpA.
Objective:
Primary objective was to compare the clinical characteristics of patients with AAU from patients without AAU in axial and peripheral spondyloarthritis (SpA) patients. Secondary objectives were to describe the clinical features of patients with AAU in the subset of patients with peripheral SpA (pSpA) and the clinical characteristics of patients with recurrent AAU in SpA patients.
Design:
This is an ancillary analysis of the ASAS-PerSpA study which included 3152 patients, 2719 patients with axSpA and 433 with pSpA according to rheumatologist judgement.
Methods:
Recurrent AAU was defined as the presence of two or more episodes of AAU ever. Univariable and multivariable binary logistic regression analyses were conducted to identify factors associated with the presence of AAU ever and the presence of recurrent AAU.
Results:
Overall, 663 patients (21%) presented AAU. Of them, 444 (66.9%) presented recurrent episodes. In patients with SpA, HLA-B27 positivity is the most important factor linked to the presence of AAU, odds ratio (OR) = 2.70 (95% CI = 2.04–3.6). In patients with pSpA, HLA-B27 positivity was also the most relevant factor linked to the presence of AAU, OR = 6.08 (95% CI = 2.72–15.68). Moreover, disease duration, younger age and higher body mass index (BMI) were the only factors slightly linked to the presence of recurrent episodes, OR = 1.03 (95% CI = 1.01–1.04), OR = 1.01 (95% CI = 1.00–1.03) and OR = 1.04 (95% CI = 1.01–1.08), respectively.
Conclusion:
HLA-B27 positivity is the most relevant factor linked to AAU risk in SpA patients, and this association is even stronger in those patients with pSpA. Moreover, our study did not find an association between HLA-B27 positivity and recurrent AAU in SpA patients.
Introduction
Spondyloarthritis (SpA) are a family of related rheumatic diseases sharing clinical features and genetic expression, allowing us to recognize and group them. 1 The traditional classification includes a group of diseases that range from mainly axial symptoms such as ankylosing spondylitis (AS) to peripheral forms such as psoriatic arthritis (PsA), inflammatory bowel disease (IBD)-associated SpA, reactive arthritis (ReA) and juvenile SpA (Juv-SpA). 2 In 2009, the Assessment of Spondyloarthritis international Society (ASAS) developed new classification criteria for axial SpA (axSpA) forms 3 and in 2011 for peripheral spondyloarthritis (pSpA) forms. 4
AxSpA manifest with predominantly axial symptoms, inflammation of the sacroiliac joints (SIJs) and spine. However, patients with axSpA usually develop other symptoms such as peripheral arthritis, enthesitis and dactylitis, as well as extra-musculoskeletal manifestations such as psoriasis, uveitis and IBD. 5 On the other hand, pSpA refers to spondyloarthritis with predominant peripheral manifestations such as arthritis (typically mono- or oligoarthritis of the lower limbs), enthesitis or dactylitis. 6
The most common extra-musculoskeletal manifestation in SpA is uveitis. It is present in 21–33% of patients and is mainly associated with HLA-B27 [odds ratio (OR) = 4.2] and disease duration.7 –10 The prevalence of uveitis differs by region; studies from North America and Europe reported higher uveitis rates than Asia and Latin American populations. 11 Moreover, the prevalence of uveitis in SpA varies according to the type of SpA, being described as more frequent in axSpA than in PsA. 10
Uveitis is the intraocular inflammation of the iris, ciliary body and choroids. Usually, leucocytes appear in the anterior chamber of the vitreous humour and, it is one of the leading causes of acquired blindness in the developed world. 12 The most typical feature of uveitis associated with SpA is acute (89%), anterior (91%) and unilateral (87%). 10 Although published data on the prevalence and characteristics of axSpA and nr-axSpA patients with acute anterior uveitis (AAU) are large, data from pSpA are scarce. Therefore, it remains unknown whether factors associated with AAU in axSpA are equal in pSpA patients. Furthermore, up to 50% of patients with an acute episode of AAU develop recurrent uveitis. 7 Despite all the previous studies reported, the factors associated with recurrent AAU remain unknown.
Recently, in the ASAS-PerSpA study (PERipheral involvement in SpondyloArthritis), the reported prevalence of AAU ever was similar in axial and peripheral SpA (21.6% and 17.3%, respectively). 13 However, the study did not report the clinical characteristics associated with the presence of AAU and recurrent episodes in axial and peripheral SpA.
The primary objective of our study was to compare the clinical characteristics of patients with AAU from patients without AAU in SpA patients, based on the rheumatologist’s judgement. Secondary objectives were to describe the clinical features of patients with AAU in pSpA patients and to compare the clinical characteristics of patients with a single episode of AAU versus patients with more than one episode of AAU in SpA patients.
Methods
Study design and patients
This is an ancillary analysis of the ASAS-PerSpA study. A detailed description of the entire study has been reported previously. 13 Briefly, ASAS-PerSpA is an observational, cross-sectional, multicentre, international study that involved 68 centres in 24 different countries all around the world and aimed to evaluate the peripheral involvement of SpA including PsA. Patients were included consecutively and grouped according to the diagnosis that in the rheumatologist judgement best described the disease of the patient irrespective of the fulfilment of any classification criteria (axSpA, PsA, pSpA, IBD-associated SpA, ReA and Juv-SpA or alternatives). All participants provided written informed consent, and local ethics committees approved the ASAS-PerSpA study protocol. However, no specific signed consent to publish was obtained, but all patient details have been de-identified. The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cross-sectional studies. In this ancillary analysis, we selected a total of 3152 patients: 2719 patients with axSpA and 433 with pSpA according to rheumatologist judgement.
Clinical data
AAU was considered if the patient has ever suffered from one episode of AAU confirmed by an ophthalmologist. Recurrent AAU was defined as the presence of two or more episodes of AAU ever, being 5.3 (7.1) the average number of episodes in this population. The variables recorded in the registry and selected for analysis in our study comprised demographic data: age, gender, body mass index (BMI) and smoking status. Disease characteristics analysed were HLA-B27 status, family history of SpA, the presence of sacroiliitis on X-ray, sacroiliitis on magnetic resonance imaging (MRI; ASAS definition), disease duration, psoriasis confirmed by a dermatologist, IBD confirmed by endoscopy, the presence of fibromyalgia (physician diagnosis) and current treatment with conventional synthetic and biological disease-modifying antirheumatic drugs [conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and biologic disease-modifying antirheumatic drugs (bDMARDs), respectively]. Peripheral musculoskeletal manifestations analysed were root joint (including hip and shoulder) involvement in the past according to the rheumatologist, peripheral joint disease (excluding root joints) in the past, enthesitis in the past confirmed and non-confirmed by specific test, and dactylitis in the past. Disease activity measurements included the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score (ASDAS). To assess the health status of patients, we reported the ASAS Health Index (ASAS HI), and to assess functionality, we reported the Bath Ankylosing Spondylitis Functional Index (BASFI).
Statistical analysis
Descriptive data were presented as proportions for qualitative variables and as means with standard deviation for continuous ones. Between-group differences were analysed using the Pearson chi-square or Fisher test for proportions and the Student’s t test or the Mann–Whitney U test for continuous variables.
To assess the variables independently associated with the presence of AAU in SpA patients, a comparative analysis between patients with AAU and without AAU was performed using a multiple logistic regression model. In this model, we performed a backward stepwise model to select the relevant factors to be included in the analysis, variables known to be related to the presence of AAU and others taken from the univariate analysis (p < 0.2). The same procedure was done for the second group of patients, presence of one episode of AAU compared with recurrent AAU, to assess the variables independently associated with the presence of recurrent uveitis in SpA patients.
Adjusted ORs after controlling for all the variables in the model were presented with their 95% confidence intervals. Two-tailed p values (p < 0.05) were established to be statistically significant. All analyses were carried out using R Studio. 14
Results
A total of 3152 patients with SpA (2719 with axSpA and 433 with pSpA) were included in our study. Adalimumab was the most current bDMARD used in axial and peripheral SpA patients. A detailed description of the current bDMARD therapy used is available in Supplementary Table 1b. At study entry, 1407 (44.6%) patients with SpA [1253 (46.1%) with axSpA and 154 (35.6%) with pSpA] were on current bDMARD treatment. Furthermore, at study entry, a high proportion of patients had active disease. Current abnormal C-reactive protein (CRP) or current ASDAS >2.1 among patients with current bDMARD treatment was present in 59.8% of patients with SpA (59.5% with axSpA and 62.3% with pSpA) at study entry.
Of all uveitis reported, 92.8% were acute, anterior and unilateral and diagnosed by an ophthalmologist. The mean episode of AAU in patients with more than one episode was 5.3 (6.9). Among patients with AAU, 116 (17.5%) patients with SpA needed specific treatment for AAU with bDMARDs and 120 (18.1%) with csDMARDs. Treatment for AAU was more often prescribed, but not significantly, in axSpA patients than in pSpA patients for both bDMARDs and csDMARDs, 107 (18.2%) in axSpA versus 9 (12.0%) in pSpA and 109 (18.5%) in axSpA versus 11 (14.7%) in pSpA, respectively. At study entry, eight patients had the first episode of uveitis within the previous 2 months.
Uveitis in SpA patients (axSpA and pSpA)
A total of 663 patients (21%) presented at least one episode of AAU: 588 patients (21.6%) with axSpA and 75 patients (17.3%) with pSpA. Table 1 shows the sociodemographic and disease characteristics of the overall SpA patients with and without AAU.
Demographic, clinical and therapeutic features in the total of SpA patients (axSpA and pSpA) with and without uveitis.

ASAS, Assessment of Spondyloarthritis international Society; ASAS-HI, ASAS Health Index; ASDAS, Ankylosing Spondylitis Disease Activity Score; axSpA, axial SpA; BASDAI, Bath Ankylosing Spondylitis; Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; bDMARDs, biological disease-modifying antirheumatic drugs; BMI, body mass index; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; CRP, C-reactive protein; HLA-B27, human leucocyte antigen B27; IBD, inflammatory bowel disease; MRI, magnetic resonance imaging; pSpA, peripheral SpA; SD, standard deviation; SpA, spondyloarhtritis.
Continuous variables are described by their mean and the standard deviation (between brackets), while absolute and percentages are shown for categorical variables.
The proportion of patients fulfilling axial ASAS classification criteria was higher in patients with AAU than those without AAU (85.1% versus 80.5%). In this sense, patients with AAU showed higher prevalence of sacroiliitis on X-ray (79.1% versus 70%) compared with those patients without AAU. In contrast, patients with AAU presented more peripheral articular disease and root joint involvement than patients without AAU (47.7% versus 43.1% and 39.8% versus 34.1%, respectively).
The age at study entry in patients with AAU was higher than patients without AAU (44.3 versus 41.7 years). Nevertheless, age at first symptom and age at diagnose was lower in patients suffering from AAU (26.2 versus 29.3 years, and 33.1 versus 34.5 years, respectively). Patients with AAU also had a higher HLA-B27 positivity (88.5% versus 73.2%), BMI and long disease duration compared with patients without AAU (Table 1).
There were no significant differences according to the presence or no of AAU in the rest of the variables analysed, including smoking status, sex, psoriasis, IBD, disease activity status (measured by ASDAS or BASDAI), CRP, disease functionality (measured by BASFI) and quality of life (measured by ASAS-Hi). When we further categorized disease activity variables into inactive or low disease activity, no significant differences were found as well (Table 1).
Regarding geographical areas, the presence of AAU was more frequent in the region of Europe and North America than in patients from Middle East and North Africa.
In the multivariable analysis, patients with HLA-B27 positive were more likely to present uveitis, OR = 2.70 (95% CI = 2.04–3.6). Current bDMARDs and csDMARDs were also significantly associated with the presence of AAU, OR = 1.59 (95% CI = 1.28–1.99) and 1.46 (95% CI = 1.19–1.78; Figure 1).

Multivariable analysis of 3152 spondyloarthritis patients (axial and peripheral) to identify factors associated with the presence of acute anterior uveitis.
Supplementary Table 1d shows the multivariable analysis of 2042 r-axSpA patients and 603 nr-axSpA patients to identify factors associated with the presence of AAU.
Uveitis in patients with peripheral SpA
A total of 75 (17.3%) out of 433 patients with pSpA presented AAU. In the univariate analysis, as was seen in SpA patients, the presence of AAU was associated with axial involvement as measured by sacroiliitis on RX and MRI (54.5% versus 33.1% and 68.9% versus 41.1%, respectively). Age at first symptom and age at diagnoses were also lower in patients suffering from AAU (29.3 versus 35.2 years and 34.4 versus 39.2 years, respectively).
Furthermore, the presence of AAU was associated with HLA-B27 positivity (87.9% versus 56.6%) and long disease duration (10.6 versus 8.8) compared with patients without AAU (Table 2).
Demographic, clinical and therapeutic features in pSpA patients with and without uveitis.

ASAS, Assessment of Spondyloarthritis international Society; ASAS-HI, ASAS Health Index; ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Spondylitis; Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; bDMARDs, biological disease-modifying antirheumatic drugs; BMI, body mass index; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; CRP, C-reactive protein; HLA-B27, human leucocyte antigen B27; IBD, Inflammatory bowel disease; MRI, magnetic resonance imaging; pSpA, peripheral SpA; SD, standard deviation.
Continuous variables are described by their mean and the standard deviation (between brackets), while absolute and percentages are showed for categorical variables.
We did not find other relevant differences in the rest of the variables analysed, including no differences regarding geographical areas.
In the multivariable analysis, HLA-B27 positivity was the most relevant factor linked to AAU development in pSpA patients, with an OR = 6.08 (95% CI = 2.72–15.68). Moreover, long disease duration was slightly linked to the risk of uveitis, OR = 1.09 (95% CI = 1.05–1.12) (Figure 2).
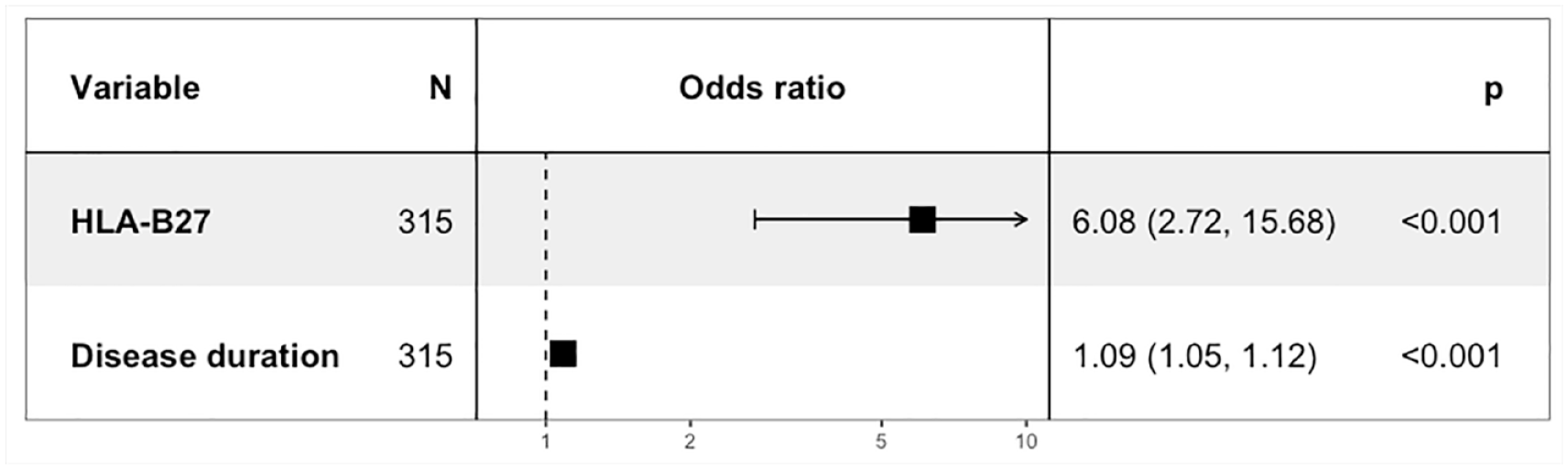
Multivariable analysis of 433 patients with peripheral spondyloarthritis to identify factors associated with the presence of acute anterior uveitis.
Recurrent uveitis in SpA patients
Among the 663 SpA patients with AAU, 444 (66.9%) presented recurrent episodes, without differences comparing axSpA and pSpA patients, 66.8% (393/588) and 68% (51/75), respectively. In the univariate analysis, the age at study entry in patients with recurrent AAU was higher than in patients without recurrent AAU (45.8 versus 41.3 years). BMI and disease duration was additionally higher in patients with recurrent AAU (26.9 versus 25.5 kg/m2 and 19.6 versus 15.8 years, respectively). Surprisingly, HLA-B27 positivity was only slightly higher and, therefore, not clinically significant in patients with recurrent AAU compared with patients with one episode of AAU (89.7% versus 86.2%). Furthermore, when analysing axSpA and pSpA separately, no significant differences were found regarding HLA-B27 positivity, between patients with recurrent AAU and one episode of AAU (89.5% versus 86.6% in axSpA and 91.4% versus 82.6% in pSpA). There were no other relevant differences between the two groups for the rest of variables analysed (Table 3).
Demographic, clinical and therapeutic features in SpA patients (axSpA and pSpA) with one episode of uveitis compared with patients with more than one uveitis.

ASAS, Assessment of Spondyloarthritis international Society; ASAS-HI, ASAS Health Index; ASDAS, Ankylosing Spondylitis Disease Activity Score; axSpA, axial SpA; BASDAI, Bath Ankylosing Spondylitis; Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; bDMARDs, biological disease-modifying antirheumatic drugs; BMI, body mass index; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; CRP, C-reactive protein; HLA-B27, human leucocyte antigen B27; IBD, Inflammatory bowel disease; MRI, magnetic resonance imaging; pSpA, peripheral SpA; SD, standard deviation; SpA, Spondyloarhtritis.
Continuous variables are described by their mean and the standard deviation (between brackets), while absolute and percentages are showed for categorical variables.
In the multivariable analysis, long disease duration and higher BMI were slightly associated with more risk of recurrent episodes, OR = 1.03 (95% CI = 1.01–1.04) and OR = 1.05 (95% CI = 1.01–1.09), respectively. As expected, current csDMARDs was also associated with more risk of recurrent episodes OR = 1.68 (95% CI = 1.17–2.44) (Figure 3).

Multivariable analysis of patients with spondyloarthritis to identify factors associated with the presence of recurrent acute anterior uveitis.
Discussion
The present study evidenced that the positivity of HLA-B27 seems to be the primary risk factor for AAU development, not only in axSpA but also in patients with pSpA. In fact, this association between HLA-B27 and uveitis seems to be stronger in pSpA than in axSpA patients. To highlight, more than half of the patients who have ever suffered from AAU (66.9%) presented recurrent episodes during the disease evolution, independently of the type of SpA (axial or peripheral). It is also important to underline that we did not find a significant association between the positivity of HLA-B27 and the presence of recurrent AAU defined as more than one episode of AAU during the disease evolution.
Our findings are consistent with previous data showing that HLA-B27 and disease duration are the main factors associated with the presence of AAU in SpA patients.7,10,15 We also found that the prevalence of AAU was higher in patients with axSpA than patients with pSpA, suggesting that factors associated with axial involvement probably must be implicated. In this sense, the fact that the positivity of HLA-B27 was the principal risk factor associated with AAU, especially in pSpA patients, seems to support this assumption. On the other hand, it is known that the prevalence of AAU in SpA varies according to the type of SpA,7,10 with a higher prevalence reported in radiographic-SpA forms.7,16 The result we observed in our study is in agreement with previous data, showing a higher prevalence of radiographic sacroiliitis in SpA patients with AAU compared with patients without AAU. Furthermore, some previous studies suggest a higher prevalence of uveitis in r-axSpA patients with peripheral arthritis.10,17,18 Nevertheless, in our study, peripheral arthritis was not independently associated with the presence of AAU in SpA patients.
In our study, regarding the burden of disease, we observed a numerical lower disease burden in axial than in peripheral SpA, both in those with and without AAU. Hence, patients with axSpA had lower ASDAS, lower BASDAI, lower CRP levels and better ASAS-HI indices. As described in other studies,15,16 the presence of arthritis in the peripheral forms may influence the burden of disease to a greater extent than axial pain.
A Chinese cross-sectional study described an association between uveitis with disease activity (as measured by BASDAI), functional ability and physical mobility in patients with AS. 17 However, a study based on a French cohort reported no association between high disease activities as measured by BASDAI with the presence of uveitis. 15 In line with this study, in our data, disease activity was not related to the presence of AAU, measured neither by BASDAI nor by ASDAS. Moreover, when we categorized disease activity by ASDAS as inactive or low disease activity, no association with AAU was found. We also found no associations with functional disease status as measured by BASFI, supporting the broad clinical experience that AAU is not significantly linked to SpA activity.
AAU is the most common extra-musculoskeletal manifestation in SpA, and it is well known to have a consequential impact on the burden of the disease, especially in recurrent forms. 18 However, our study did not observe any association between AAU and recurrent AAU with the health quality of life, as measured by the recently developed ASAS Health Index.
The prevalence of uveitis is known to be lower in patients with PsA 19 and IBD 20 compared with patients with AS. In this sense, we did not find any association between psoriasis and IBD with AAU. Some clinical manifestations, such as peripheral arthritis, seem to be more frequent in SpA patients related to geographical areas. 13 In this sense, previous data 7 suggest a lower prevalence of uveitis in Latin American patients with SpA. In our study, we observed that the presence of AAU was more frequent in the region of Europe and North America than in patients from Middle East and North Africa.
We found a prevalence of AAU of 17.3% in patients with pSpA. Several previous studies have assessed clinical characteristics of uveitis in axSpA patients; however, these data in pSpA patients are scarce. Our study showed that HLA-B27 positivity was the only relevant factor independently associated with uveitis in pSpA patients. The association between HLA-B27 and uveitis is even stronger in pSpA than in axSpA patients (OR = 7.98 versus 2.59, respectively). Furthermore, we found a weak association between disease duration and the presence of AAU. This association, although it is numerically significant, is not clinically significant.
Recurrent AAU (presence of at least one episode of uveitis during the disease course) was observed in more than half of SpA patients (66%). Moreover, this percentage was similar despite the type of SpA (axSpA and pSpA). According to our data, in contrast to the strong association observed between HLA-B27 positivity and AAU, we found no association between HLA-B27 positivity and recurrent AAU. Some previous studies reported that HLA-B27 positivity is implicated with the pathogenesis of uveitis 10 and related to the recurrence of uveitis.7,10 Conversely, other studies pointed out a high prevalence of uveitis in SpA patients HLA-B27 negative,21 –23 suggesting that other unknown factors could be implicated in the pathogenesis of uveitis in SpA patients and therefore explaining the lack of association we observed between HLA-B27 positivity and recurrent uveitis. In fact, HLA-B27-transgenic rats develop spondylitis, peripheral arthritis, colitis and dermatitis but not uveitis. 24 Currently, risk factors and biomarkers predisposing to uveitis and, more importantly, to the risk of recurrence are still lacking. Over the last years, increasing research in metagenomics studies has led to the hypothesis that the microbiome plays a role in the evolution of both SpA and uveitis; 12 however, the scientific support in this theory is lacking.
Finally, the presence of AAU was associated with an increase in the prescription of csDMARDs and bDMARDs, especially adalimumab, in SpA patients. These findings could be explained because the efficacy of these treatments in this situation and emphasizes the higher burden and costs of SpA associated with the presence of AAU.
Our study has several limitations. First, this is an observational cross-sectional study including the collection of some past manifestations retrospectively. The sample size for SpA patients with AAU is large for axSpA and modest for pSpA which may difficult the possibility to analyse some associations. Nonetheless, this is the large worldwide cohort of pSpA patients recorded. Furthermore, data on ocular complications and characteristics of AAU were scarce.
In summary, HLA-B27 positivity is the most relevant factor linked to AAU risk in SpA patients, and this association is even stronger in those patients with pSpA. However, our study did not find any association between HLA-B27 positivity and recurrent AAU in SpA patients. Hence, additional biomarkers are needed to identify patients at risk of recurrent AAU.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X221119246 – Supplemental material for Uveitis in peripheral spondyloarthritis patients: an ancillary analysis of the ASAS-PerSpA study
Supplemental material, sj-docx-1-tab-10.1177_1759720X221119246 for Uveitis in peripheral spondyloarthritis patients: an ancillary analysis of the ASAS-PerSpA study by Maria Llop, Jordi Gratacós, Mireia Moreno, Marta Arévalo, Joan Calvet, Maxime Dougados and Clementina López-Medina in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
We would like to thank the Assessment of SpondyloArthritis international Society (ASAS), the patients who participated in the study and the investigators who included the participants and completed the case report form. We also thank the steering committee members of the ASAS-PerSpA (PERipheral involvement in SpondyloArthritis) study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.