
Abstract
Although great improvements have been achieved in the fields of diagnosing and treating patients with giant-cell arteritis (GCA) in the last decades, several questions remain unanswered. The progressive increase in the number of older people, together with growing awareness of the disease and use of advanced diagnostic tools by healthcare professionals, foretells a possible increase in both prevalence and number of newly diagnosed patients with GCA in the coming years. A thorough clarification of pathogenetic mechanisms and a better definition of clinical subsets are the first steps toward a better understanding of the disease and, subsequently, toward a better use of existing and future therapeutic options. Examination of the role of different imaging techniques for GCA diagnosing and monitoring, optimization, and personalization of glucocorticoids and other immunosuppressive agents, further development and introduction of novel drugs, identification of prognostic factors for long-term outcomes and management of treatment discontinuation will be the central topics of the research agenda in years to come.
Introduction
Giant-cell arteritis (GCA) is a systemic vasculitis affecting people aged 50 and older that primarily involves large- and medium-sized vessels. GCA can cause acute, irreversible visual loss; therefore, prompt diagnosis and treatment initiation are essential. During the last decades, much interest has arisen in different aspects of this illness, and many new diagnostic and therapeutic options have emerged.
The purpose of this review is to shed some light on future perspectives of this polyhedral disease.
Novelties in pathogenesis epidemiology
Novelties in pathogenesis
GCA follows a polygenic inheritance pattern. The association with some HLA (HLA-DRB1 and HLA-DQA1) and, to a lesser extent, with some MHC class-I HLA-B and non-HLA polymorphisms, has been well established by large immune-focused genotyping arrays performed on patients with temporal artery biopsy (TAB)-confirmed disease.1–6
An increasing body of evidence suggests that GCA is characterized by both systemic and vascular inflammation and that these two processes can act independently with regard to pathogenesis and, subsequently, clinical phenotypes. 7 Figure 1 shows the main pathophysiological mechanisms underlying development of GCA.

Pathophysiological aspects of giant-cell arteritis: (a) activated DCs recruit and fuel proliferation and differentiation of T-cells, with subsequent activation of macrophages, formation of giant cells, vascular damage, and occlusion. (b) Proposed mechanisms implicated in the genesis of systemic inflammation. (c) Proposed mechanisms implicated in vascular inflammation.
Systemic inflammation
While mechanisms underlying vascular damage have been largely clarified during the last decades, much less is known about the genesis of systemic inflammation in GCA. It has been hypothesized that immune cell activation precedes vascular inflammation. In fact, there is a consistent overlap between activation patterns seen among circulating peripheral blood mononuclear cells in GCA and polymyalgia rheumatica (PMR) patients. Since PMR, which is considered a pre-vasculitic disease by some experts, shares with GCA many cellular and cytokine pathways (i.e. aberrant polarization of CD4+ T toward effector cells, expanded interferon (IFN)-γ Th1 and STAT3 activation patterns with increased interleukin (IL)-17 + Th17 cells), it may be postulated that systemic inflammation comes earlier than vascular damage in GCA. 7
One of the greatest challenges for the coming years will be to better understand the pathogenesis of inflammation in these conditions. In this regard, the concept of ‘inflamm-aging’ seems to play a central role in the initial immune activation in GCA. It has been proposed that the almost exclusive risk of individuals aged 50 or older to develop GCA may be related to the chronic low-grade inflammation that is characteristic of the elderly, including increased levels of IL-6.8,9
This pro-inflammatory state is strongly connected with the concept of immunosenescence. Immunosenescence is characterized by a shrinkage of the naïve T-cell pool, contraction of T-cell diversity, and impairment of innate immunity, particularly of dendritic cell (DC) function. Moreover, after the age of 50 years, there is a decrease in the activity of CD8 + CCR7 + T-regulatory cells (T-regs), which, under normal conditions, suppress activation, and expansion of pro-inflammatory CD4 + T-cells. 10 Specifically, in patients with GCA, T-regs lose their ability to package NADPH oxidase 2 (NOX2) into immunosuppressive exosomes. Under physiological conditions, T-regs NOX2 exosomes suppress CD4 + T-cell proliferation, halting the immune process. However, T-reg frequency declines progressively with age as they become deficient in NOX2, with consequent impairment of their suppressive and modulatory role. 11
In the near future, we also expect to see breakthroughs regarding the role of somatic variants (SVs) in GCA onset, phenotype and outcomes. SVs are postzygotic, mutations acquired during mitosis or after exposure to endogenous (i.e. products of cellular metabolism, reactive oxygen, and nitrogen species) or exogenous factors (i.e. ultraviolet light or radiation, tobacco, and alcohol), eventually leading to mosaicisms. Interestingly, the number of SVs increases with aging. SVs can render immune system cells resistant to apoptosis or change their functional profile (i.e. leading to aberrant cytokine secretion), causing high-inflammatory, non-proliferative (i.e. non-neoplastic) immune disorders such as primary immunodeficiency and autoinflammatory diseases 12 and the VEXAS syndrome. 13
Another pathogenetic mechanism potentially implicated in development of GCA might be clonal hematopoiesis of indeterminate potential (CHIP), a pre-malignant state characterized by somatic mutations in hematologic precursor cells. 14 Notably, the incidence of CHIP correlates with age, and it is associated with increased levels of C-reactive protein (CRP) and other classic systemic inflammatory markers. 15 Preliminary works exploring a potential correlation between CHIP and the development of GCA seem to corroborate this association. 16
Finally, GCA is characterized by an STAT3 activation pattern of CD4 + lymphocytes.17,18 In GCA, IL-6 and other pathophysiological relevant cytokines, chemokines, and hormones converge on activating the Janus kinase (JAK) – STAT signaling pathway, resulting in migration of immune cells into inflamed areas. 19 Although the presence of STAT3 SVs has not been ascertained in GCA so far, the presence of these SVs has already been detected in other autoimmune diseases such as multiple sclerosis, Felty’s syndrome and cryoglobulinemic vasculitis. 20 It needs to be clarified whether traditionally recognized risk factors for GCA, such as tobacco smoking and aging, are risk factors for the disease per se or risk factors for GCA-predisposing SVs.
Vascular inflammation
GCA is universally recognized as an antigen-driven disease, but the initial environmental trigger(s) for vascular injury is still unknown. After the triggering event, an aberrant maturation of adventitial DCs takes place, 21 and the inflammation process spreads into the arterial wall leading to a damage-and-repair response. 7 A recent meta-analysis failed to confirm the presence of a seasonal pattern for GCA and PMR onset, 22 while the hypothesis that infections may initiate the process is still debated. In elderly individuals, both clearance of circulating/tissue antigens and initiation of immune response are reduced as compared to young people. 23 In these circumstances, antigens persist much longer, potentially rendering them more likely to have a triggering effect. Recently, a large study on 1005 TAB-confirmed cases of GCA showed that infection exposure, especially those of the respiratory tract, was significantly more common among people subsequently diagnosed with GCA comparing to controls, supporting the hypothesis that exposure to different pathogens may trigger the disease. 24 What we do know is that the loss of arterial wall immune privilege plays a central role in the subsequent aberrant innate and adaptive immune system response and that activated DCs interact with CD4 + T-cells that are crucial effectors in fueling vessel inflammation. 24 Tissue aging has been recently implied in this process as well, since vascular DCs seem to progressively lose their tolerance as the host grows old. An attractive hypothesis is that the inflammatory milieu of a predisposed elderly person could induce a differentiation of these altered DCs toward a pro-inflammatory phenotype, rendering them unable to protect a structurally altered vascular vessel from inflammation and injury. In fact, tissue-aging largely affects vessel structure as well, with progressive thickening and stiffening of vascular walls.25–27 In this regard, several variants within plasminogen and P4HA2 genes, both involved in vascular remodeling and angiogenesis, have been firmly associated with risk to develop GCA at a genome-wide level of significance. 6 Moreover, several signaling pathways have been implicated in initiating and sustaining pathogenic CD4 + T-cell function and loss of tolerance in the artery wall, representing potential new therapeutic targets for the upcoming years. These include the NOTCH1-Jagged1 pathway,17,28 the CD28 co-stimulatory pathway, the PD-1/PD-L1 co-inhibitory pathway, a critical regulator of immunity, 29 and the JAK-STAT signaling pathway. In particular, the IL-6-driven JAK-STAT signaling pathway leads to proliferation, activation, and migration of inflammatory cells and in additional IL-6 production, fueling inflammation, and vascular damage.19,30
Epidemiology: will GCA prevalence increase over time?
According to the World Population Aging 2020 Highlights, drafted by the United Nations Department of Economic and Social Affairs, by 2050, the number of persons aged ⩾65 years will reach the impressive number of 1.5 billion worldwide. This means that 1 in 6 persons will be aged 65 years or older, with an overrepresentation of women in this age group. Although the relative incidence of GCA will probably stay stable over time, 31 the rising number of elderly individuals together with growing awareness of the disease and use of advanced diagnostic tools, foretells an increase in the absolute number of patients with newly diagnosed GCA. Besides, a meta-analysis has recently shown that mortality in GCA has generally decreased over time, 32 and a further reduction can be expected in the near future due to increasing longevity in the elderly, earlier diagnosis and treatment of the disease, increased surveillance as well as the increased use of glucocorticoid-sparing agents. It has been projected that by 2050, the disease burden of GCA will be greater than 3 million cases, with around 500,000 persons experiencing GCA-related visual complications. 33 Healthcare systems will therefore have to deal with these epidemiologic changes, and more resources should be allocated to ensure early diagnosis of GCA, and to facilitate the use of new, and at the same time more expensive drugs for management of the disease and to prevent glucocorticoid-related complications. Indeed, the already high overall healthcare costs 34 are very likely to further increase in the next years.
GCA during COVID-19 pandemic
Although the etiology of GCA has not been fully elucidated, environmental factors and infections, particularly respiratory-tract infections, have long been thought to contribute to its pathogenesis.24,35,36 A relevant question in this regard is how the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic may be affecting the incidence of the disease. Of interest, to date an increase in the incidence of GCA has not been reported, with the rate of newly diagnosed patients being stable over the last 2 years.37,38 At present, few (and not completely concordant) data are available in the literature, so that definitive conclusions cannot be drawn.37–39 Many potential biases are worthy of consideration in assessing the epidemiology of GCA during SARS-CoV-2 pandemic, such as the widespread use of surgical masks and social distancing measures, which could contribute to a reduced transmission of other respiratory pathogens who are concerned to trigger GCA. 40
A number of new-onset GCA cases following both mRNA and vector vaccines has recently been reported, even though is difficult to prove the causality.41–43 Notably, flares of autoimmune diseases with a short latency after SARS-CoV-2-vaccination have also been described, suggesting a possible role of vaccination as a trigger.44,45 However, notwithstanding that adequate numerator and denominator data are unavailable, SARS-CoV-2 vaccine benefits to combat the pandemic dramatically outweigh the potential risks, as the possible adverse events appear very rare in relation to the billions of doses administered so far.
Finally, whether patients with pre-existing rheumatic diseases including GCA and other large vessel vasculitis (LVV) are at increased risk of SARS-CoV-2 infection, or severe outcomes, remains unclear. 46 Literature suggests that the infection risk of patients with LVV is similar to (or even lower than) that of the general population.37,38
However, SARS-CoV-2 infection appears to be more severe in persons with LVV, with higher rates of hospitalization and lethality. 38 In this regard, it has to be considered that GCA affects mostly the elderly and that patients with GCA have higher rates of specific comorbidities such as diabetes mellitus. 47 Older age and specific comorbidities are now well-recognized predictors of SARS-CoV-2 related-death, both among the general populations 48 and among people with rheumatic diseases, 49 and thus they can at least partially explain the above-mentioned worse outcome of LVV-affected patients. Glucocorticoids use at moderate/high dose (⩾10 mg per day prednisone equivalent) has been shown to be associated with severe SARS-CoV-2 infection in patients with rheumatological diseases as well.46,50 However, these data should be taken cautiously since a causal interpretation of results based on a cross-sectional observational study is not possible and several biases, such as covariance with disease activity, should be considered. 51 In fact, a further sub-analysis on these data, specifically exploring the interaction between glucocorticoids and disease activity, has shown that is the latter to drive the association with SARS-Cov-2-related death, independently from glucocorticoids dose. 52 Intriguingly, the strength of the association seemed to intensify as the glucocorticoids dose increased. Whether this reflects a potential residual role of glucocorticoids in determining outcome or a proxy for level of disease activity, still needs to be clarified.
Diagnosis
Imaging
In GCA, almost all large-caliber arteries affected by the inflammatory process can be quite easily evaluated exploiting one of the different imaging techniques available. 53 In the next 10 years, the role of these imaging techniques will become better defined and their use will become more standardized.
Vascular ultrasound
In the last 10 years, the role of vascular ultrasound in diagnosing GCA has grown markedly. From an ancillary tool used only by a limited group of experts, it has become a fundamental instrument for rheumatologists managing patients with GCA, as long as they have a good expertise. 54 Indeed, the most recent EULAR recommendations for GCA management specify this technique as the first-choice measure to confirm diagnosis when new onset, predominantly cranial GCA is suspected. 55 Low invasiveness, rapidity of execution, and immediate feedback are its main strengths, in addition to the fact that it can be performed by clinicians caring for the patient. 56 While there is a considerable body of data on the utility of ultrasound in the evaluation of GCA, a number of questions remain about its role.
First, it would be interesting to understand how widespread the use of vascular ultrasound is in clinical practice. It would be desirable that every rheumatologist approaching a new patient with suspected GCA was able to confidently perform a vascular ultrasound examination to rule out or confirm the diagnosis. In order for this to happen, appropriate training is of fundamental importance. 57 It is likely that the role of TABs will be reevaluated, and in future limited to indeterminate, uncertain cases and research purposes.
Second, vascular territories routinely investigated by means of ultrasound will probably be redefined. Currently, a standard GCA ultrasound evaluation comprises the assessment of common temporal arteries, with their parietal and frontal branches, and of axillary arteries. This combination provides a good balance between rapidity, ease of execution and sensitivity in diagnosing both cranial and extracranial subsets of GCA. 56 With improvement of vascular ultrasound techniques, it can be expected that other vessels will soon be included in the clinical practice assessment. Cranial disease may be further evaluated by ultrasonographic interrogation of vertebral, facial, and occipital arteries,58,59 while carotid and subclavian arteries are probably the best additional candidates for assessment of extracranial arteries. 60
Third, it is likely that vascular ultrasound will acquire a role in defining disease severity. Currently, vascular ultrasound is performed primarily to rule out/rule in GCA diagnosis. 56 This certainly is a critical role, especially in GCA where prompt initiation of adequate treatment is required. However, it is also realistic to predict a role for ultrasound in stratifying patients in order to tailor treatment according to the extension and distribution of the vascular involvement. Quantitative scores, such as the ‘Halo score’, are already being used and probably will become soon part of routine clinical practice. 61 Such scores could allow to categorize patients into groups with more and less severe vascular inflammation, to monitor response to treatment and to predict relapses and other clinical outcomes. Hence, it is possible to hypothesize a future in which patients with a greater burden of vascular involvement of cranial vessels will receive a different treatment (e.g. higher initial glucocorticoid dose) as compared to patients with predominant ultrasound-verified extracranial pattern. Other clinical and laboratory risk factors will certainly also be considered.
Finally, along with enhancement of rheumatologists’ ultrasound skills, we will probably witness additional technical developments and the introduction of new features. High-resolution (up to 55 MHz) probes have already been developed, but they are still mostly relegated to research purposes. 62 Owing to their extremely high sensitivity, their use will become more common, and potentially be of particular usefulness in evaluating patients already on glucocorticoid therapy or when the classic halo sign cannot be visualized, but the clinical picture is highly suggestive of GCA. Another innovation we expect will spread in the next years in the field of GCA is real-time ultrasound directly performed at bedside by means of a single probe with multiple frequencies wirelessly connected to a small display (e.g. iPhone/iPad). This approach, commonly known as point-of-care ultrasound (POCUS), enables clinicians to promptly perform the examination of patients with suspected disease in almost any setting, whether the clinic, hospital, or emergency room. Recently, its reliability was evaluated in a small cohort of 10 patients, with positive results. 63 Certainly, larger studies are needed before widespread implementation is pursued.
Positron emission tomography
18-fluorodeoxyglucose positron emission tomography (FDG-PET) was originally introduced in clinical practice to diagnose and stage cancers. 64 However, once it became clear that activated inflammatory cells also accumulate the radiotracer, the use of this imaging technique began to be applied to the evaluation of rheumatologic diseases characterized by a significant inflammatory burden. 65 GCA, particularly its extracranial subset, is a paradigmatic model: it is a highly inflammatory disease and, in addition, affected vessels have a size greater than the limit for spatial resolution of FDG-PET (i.e. around 4–5 mm). 66 FDG-PET is therefore a useful tool for assessment of patients with GCA, even though its use for both diagnosis and follow-up has not yet been completely standardized. The reason is that this imaging technique has some limitations that constrain more widespread application. These include high costs and limited availability. The sensitivity of FDG-PET dwindles down rapidly once glucocorticoid treatment has been started. Ideally, an FDG-PET should be conducted within 3 days of initiation of treatment, but this is not feasible in many centers.67,68
It is difficult to predict how the role of FDG-PET in GCA will evolve over the next 10 years. It is likely that its use in unclear situations will be consolidated. Paradigmatic cases will be those where systemic, non-specific symptoms prevail and other diagnoses such as malignancies need to be ruled out, in particular when ultrasound of axillary arteries is negative or not available. How extensive the use of FDG-PET will be in patients already diagnosed with GCA by cranial or axillary ultrasound depends on the understanding of how much the additional information from FDG-PET will influence management decisions. We already know that the involvement of the aorta and its main branches can adversely affect disease prognosis,69–71 but most of these vessels, with the notable exception of the descending thoracic aorta, can be adequately evaluated by means of a more economic tool such as vascular ultrasound. 54 An important step toward a greater use of FDG-PET in GCA would result from data demonstrating that specific patterns of radiotracer uptake correlated with worse disease outcome or even predicted better response to a specific treatment. At the present time, we only know that FDG uptake by the ascending aorta is associated with a higher risk of aneurysm formation, but this information does not always impact treatment decisions.70,72–74 In addition, the true risk of developing clinically relevant aortic aneurysms (i.e. requiring surgery) in GCA is still not clear.
FDG-PET is usually performed in association with computed tomography (PET-CT) in order to localize radiotracer anatomical distribution. In more recent years, the use of combination of FDG-PET with magnetic resonance imaging (MRI) has become more common, even in the field of LVV.75,76 This imaging technique has the strength of coupling the quantitative analysis of vascular inflammation by FDG-PET scan with the morphological evaluation of vascular remodeling by MRI (Figure 2). Hence, its use in GCA will likely increase in the next years, but its high costs will limit its use to selected patients. Patients with extracranial GCA, clinical refractoriness to treatment and those at high-risk for arterial stenoses or aneurysms will probably be the ideal candidates for these combined imaging techniques.

FDG PET-MRI images of a 78-year-old patient affected by giant-cell arteritis. STIR image (a) shows diffuse hyperintensity, due to edema, of the walls of aortic arch (arrowheads) and common brachiocephalic trunk (arrow). Late gadolinium enhancement image (b) shows mild thickening and hyperintensity of the same vessel walls, that are also characterized by diffuse uptake of FDG as demonstrated by the PET image (c) and by the corresponding fused PET-MRI image (d).
Another technical innovation which might be introduced in the next years is the use of novel radiotracers as alternative to FDG. Most studies concerning the assessment of vascular inflammation have been performed in patients with atherosclerosis, 77 while in GCA, preliminary data are available only for the following radiotracers: 11 C-PK11195, 68Ga-DOTATATE, and 18F-FET-βAG-TOCA. The first one binds to the translocator protein (TSPO) receptor, which is highly expressed by activated macrophages, 78 whereas the latter two bind to the somatostatin receptor subtype-2 (SST2), predominantly upregulated by M1 macrophages. 79 At present, we only know that these novel radiotracers allow localization of vascular inflammation,78–80 but many questions, such as how they are influenced by glucocorticoids, whether they can predict vessel injury and disease outcome, and whether they can define response to therapy, are still unanswered. These questions need to be addressed by future research.
Biomarkers/signatures
Elevation of classic inflammatory markers has been and continues to be one of the cornerstones of both, new-onset GCA diagnosis and relapse identification. 81 Indeed, it is extremely rare, if not anecdotal, that both, CRP or erythrocyte-sedimentation rate (ESR) are normal in new onset GCA. This finding has a fundamental importance since GCA symptoms are often non-specific and potentially misleading, such as headache or visual disturbances. 82 Hence, we expect CRP and ESR to still have a dominant role in the evaluation of GCA in the next 10 years. Limitations to their value are well known and pushed the search for new, complementary biomarkers. The most important limitation in the current management paradigm is the strong influence of the IL-6 receptor antagonist tocilizumab on ESR and CRP levels, regardless of the actual clinical response. Patients on tocilizumab almost always have normal CRP and ESR, even when GCA is clinically or radiologically deemed to be active. 83 In addition, classic inflammatory markers have a poor yield in predicting disease course. Patients with a stronger inflammatory response seem to have a higher relapse rate, 84 but studies are still heterogeneous and of poor quality. Novel potential serum biomarkers have been identified in the last years that may be introduced into clinical practice soon, given they demonstrate utility for GCA assessment. For example, elevation of YKL-40 or osteopontin at baseline seems to predict a more aggressive disease course and higher glucocorticoid requirements.85,86 On the other hand, high levels of MMP-2, VEGF, and angiopoietin-1 have been linked to a more favorable disease course.86,87 In addition, tocilizumab apparently does not affect osteopontin serum levels, and this makes it a potential activity biomarker in patients treated with IL-6 receptor antagonists. 85 The possible influence of IL-6 blocking therapy on the other biomarkers mentioned still needs to be investigated.
Even if future need for TABs gradually decreases, histologic analysis might still have an ancillary role in disclosing disease biomarkers. Given that Th1-dependent inflammation in GCA is poorly sensitive to systemic glucocorticoids and that it is associated with relapsing disease, it could be speculated that patients with Th17-enriched infiltrates might benefit from an early addition of glucocorticoid-sparing agents. On the other hand, glucocorticoid monotherapy might be appropriate when Th17 cells dominate and when the IL-6-IL-17 inflammatory cluster prevails.88,89
Finally, as the role of acquired somatic mutations in causing non-malignant diseases emerges, in some cases with an inflammatory phenotype, such as VEXAS syndrome or CHIP,14,20 it becomes of particular interest to explore how these mutations affect the inflammatory disease response and disease course in GCA.
Disease stratification
For years, GCA has been regarded as a monomorphic disorder, characterized by homogeneous clinical features and outcomes, and therefore easily treatable with a standard therapeutic strategy. However, this paradigm has now been overturned. The extensive use of imaging tools for GCA diagnosis and the greater knowledge of disease pathogenesis have made clear that the clinical spectrum of GCA is far more complex. Consequently, we believe that in future GCA will be managed with a stratified approach. 90 This means that demographic, clinical, laboratory, and imaging features will be used to predict the disease course of each patient with GCA and to determine the risk of developing disease- and therapy-related complications, in order to tailor the treatment accordingly. To date, relapse rates seem to be higher when constitutional symptoms prevail and when inflammation involves extracranial large vessels.69–71,84,91 However, available data are still conflicting and do not allow clinicians to define precise disease phenotypes requiring specific tailored treatments. We expect that artificial intelligence (AI) will be developed to individualize management of GCA. This will help to improve algorithms for stratifying patients according to their tendency to experience disease flares upon glucocorticoid reduction, to identify patients in whom early introduction of glucocorticoid-sparing agents is appropriate (important especially for patients at high risk of glucocorticoid-related adverse effects) and to identify patients at risk for refractory disease as well as catastrophic disease outcomes. 71 In order to develop effective and reliable AI approaches, it will be imperative to collect large volumes of information from various centers worldwide, the so-called ‘Big Data’.
Understanding long-term vascular complications, especially aneurysm development, is another critical unmet need in GCA. Coexisting arterial hypertension and/or PMR, smoking habit, and increased radiotracer uptake in the aorta in PET have all been associated with a higher risk of aneurysms, but, again, no different treatment approaches have been proposed so far for patients with and without these risk factors. 92 In addition, no data on the ability of glucocorticoid-sparing agents to prevent vascular complications are available yet. As a future plan, it is therefore mandatory to (1) define a scoring system to stratify patients according to the risk of developing aneurysms and other vascular complications; (2) study if methotrexate, tocilizumab, and other disease-modifying anti-rheumatic drugs (DMARDs) may actually play a role in preventing vascular complications; and (3) define the best follow-up strategy and appropriate imaging techniques to monitor patients at risk of such complications.
Management/follow-up
Treat-to-target strategy in GCA
Treat-to-target (T2T) is a disease management approach aimed at reaching a pre-specified treatment goal, the so-called target. This concept has been successfully used in both rheumatological93,94 and non-rheumatological conditions.95–98 The ultimate goal of T2T in rheumatology is to improve patients’ quality of life through better disease control, optimization of immunosuppressive therapy, and minimization of disease-related damage and treatment side effects. Although this concept may theoretically apply to GCA, 99 a well-defined T2T strategy has not yet been identified or endorsed, since an unanimously accepted definition of the targets is still lacking. In fact, target is a multifaceted concept in GCA, having different domains and declinations depending on the disease phase. While in early stages, the target should be avoidance of visual loss through early diagnosis, rapid initiation of treatment and achievement of remission, in established disease, the aim should be minimization of glucocorticoid use and relapse prevention, along with avoidance of damage accrual.
A further problem is the difficulty in finding agreement on the definition of remission and relapse that is a key-concept in a T2T strategy. These concepts have been variously defined in the literature, incorporating a number of different combinations of clinical and laboratory items. Another critical issue is the distinction between disease activity and damage accrual and their scoring: while this distinction is well established in antineutrophil cytoplasmic antibody-associated vasculitis, 100 dedicated instruments for monitoring and measuring chronic damage are still an unmet need in GCA.
Another important aspect of disease management that will require more attention is the fact that symptoms such as fatigue, non-specific malaise, and glucocorticoid side effects are outside the traditional set of outcome measures for GCA. Although patients’ perspective has received increasing attention in recent years, more needs to be done. Patient-reported outcomes (PROs) are an important way of ensuring that patient perspective is always included both in trials and in clinical practice. 101 Recently, an international study underpinning the development of candidate items for a GCA-specific PRO measure has been published 102 and the draft questionnaire is now undergoing psychometric testing.
Will it be possible to treat GCA without glucocorticoid?
For nearly 70 years, glucocorticoids have been the only available therapeutic option and hence have been the cornerstone of GCA treatment. The long-term burden of glucocorticoid treatment-related side effects are now often a greater management problem than the disease itself.103,104 However, minimizing side effects at all costs is often not the best strategy: the clinical tradeoff is that the burden from ischemic complications, foremost visual loss, far outweighs that of glucocorticoid-related complications. Minimizing the use of glucocorticoids therefore is still one of the biggest challenges for the near future. As already emphasized, the first step in this direction will be the stratification of patients into clinical-serological phenotypes and their associated outcomes (such as risks of ischemic complications, relapse and treatment adverse events), facilitating selection of the minimal, individualized effective glucocorticoid dose for each patient. A glucocorticoid toxicity index has been recently developed which should allow better standardization of treatment-induced damage. 105 It is hoped that newer drugs will contribute to minimizing glucocorticoid-related adverse effects. While it is an open question whether GCA can ever be treated without glucocorticoids, we speculate this is a possibility within the next 10 years.
Induction phase
Despite the great efforts to minimize their use, to date, glucocorticoids are still essential in both the induction and maintenance phase according to current clinical practice and international recommendations, with an initial suggested dose of 40–60 mg/day, unless ischemic complications are present.106,107 In that case, glucocorticoids pulse therapy (250–1000 mg per day for 3 days) should be considered.
When glucocorticoids are administered in combination with tocilizumab, the tapering scheme can often be shortened to 6 months. 108 Even more rapid tapering schemes have been tried, but experiences with this strategy have not been convincing.109–111 A recent trial of 18 GCA patients (GUSTO trial) demonstrated that tocilizumab, administrated after a 3-day-ultra-short glucocorticoid regimen, is probably not adequate for inducing rapid remission. 112 Moreover, one of these persons experienced acute inflammatory optic neuropathy, suggesting that patients may not be protected from ischemic complications if glucocorticoids are not used long enough during the remission induction phase. This seems to be corroborated by ultrasound data: the 3-day glucocorticoid pulses led to a profound but transient reduction of the temporal artery intima-media thickness (IMT), with subsequent increase of IMT after glucocorticoid discontinuation and then to a slow but steady IMT reduction over 52 weeks following introduction of tocilizumab. 113 It can be anticipated that at least for the near future, glucocorticoids will remain our quickest weapon for achieving rapid remission and for avoiding visual loss. The most intriguing question is which is the minimum dose and duration of glucocorticoid therapy, since immunosuppressive therapies are increasingly administered concomitantly in patients with new-onset disease.
Maintenance phase
Glucocorticoids are currently regarded as crucial for maintenance therapy. Slower tapering of glucocorticoid dose seems to prevent relapses.114–118 The overall glucocorticoid-sparing effect of tocilizumab and methotrexate has been demonstrated in randomized clinical trials114,115 and in a meta-analysis. 119 Much uncertainty concerns glucocorticoid monotherapy. Current EULAR recommendations suggest tapering the glucocorticoid to a target dose ⩽ 5 mg prednisone equivalent daily after 12 months of treatment but admit that this goal is hard to reach, and most patients require longer treatment. 106 Disease stratification (see Paragraph 2.3) will probably be necessary to identify patients with a higher probability of requiring a standard 1–2 years course and those needing slower dose tapering. Future approaches must also address if a strategy of trying to stop glucocorticoids at all costs, with the risk of disease flare and subsequent need for increased dosing is a better strategy than maintaining a low dose (e.g. prednisone equivalent ⩽ 5 mg daily) indefinitely.
Therapeutic prospects
To date, the list of approved drugs for the treatment of GCA is quite short. According to current EULAR recommendations, only methotrexate and tocilizumab should be administered to patients requiring a glucocorticoid-sparing agent. 106 Apart from glucocorticoids, there are currently no drugs that are recommended as stand-alone treatments for GCA. However, our impression is that the therapeutic landscape is certainly going to change in the not-all-too-distant future, as many other DMARDs are currently under evaluation or will be evaluated shortly 120 (Table 1).
Summary of ongoing or recently completed clinical trials evaluating efficacy and safety of biological or targeted synthetic disease-modifying anti-rheumatic drugs in giant-cell arteritis.
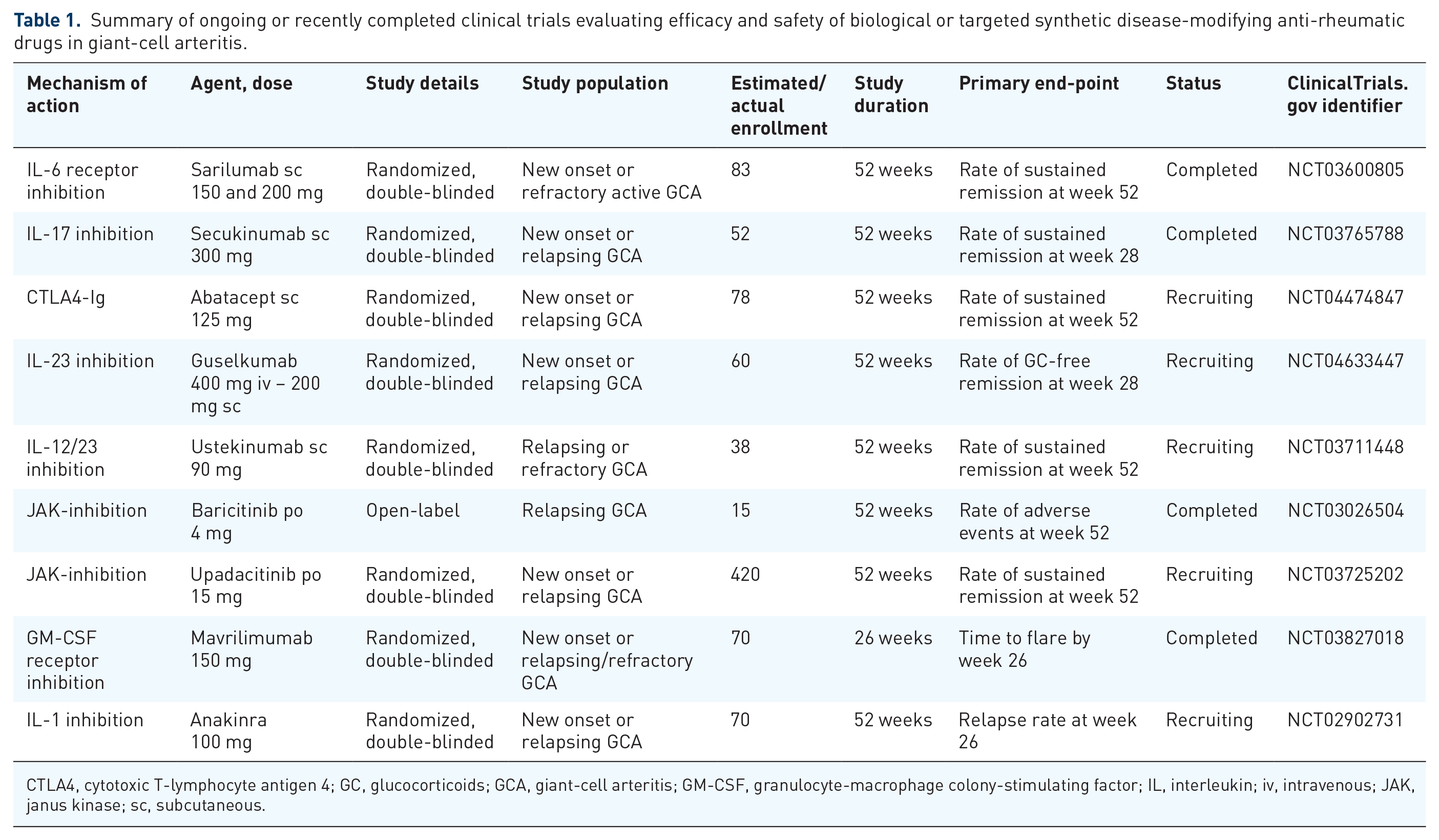
CTLA4, cytotoxic T-lymphocyte antigen 4; GC, glucocorticoids; GCA, giant-cell arteritis; GM-CSF, granulocyte-macrophage colony-stimulating factor; IL, interleukin; iv, intravenous; JAK, janus kinase; sc, subcutaneous.
Among these drugs, one of the most promising is the granulocyte-macrophage colony-stimulating factor (GM-CSF) inhibitor mavrilimumab which was recently evaluated in a phase-II randomized-controlled trial. In this study, mavrilimumab reduced the risk of flare and increased sustained remission until week 26, with an acceptable safety profile. 121 Through its innovative mechanism of action, mavrilimumab targets both the TH17 and TH1 axes involved in GCA pathogenesis, and therefore might be able not only to curb acute inflammation but also to extinguish chronic and smoldering disease and to prevent long-term vascular damage. If these preliminary results are confirmed in other larger studies with a longer follow-up, it is highly likely that mavrilimumab will be included in the GCA therapeutic arsenal.
Considerable hope is also placed in drugs belonging to the large family of JAK inhibitors. The well-known pleiotropic effects of these agents suggest a role in controlling GCA-related inflammation at multiple levels. 122 Recently, a prospective, open-label study with baricitinib in a small cohort of patients with relapsing GCA showed promising results and a randomized trials with upadacitinib is currently ongoing 123
Among other agents, data on ustekinumab are still conflicting, whereas a single randomized trial on abatacept showed some benefits on reducing the risk of relapses. Therefore, it is difficult to predict whether these two agents will become standard therapeutic options for GCA in the future.124–126 More optimism is now placed in the IL-17A inhibitor secukinumab after the successful conclusion of a double-blind, placebo-controlled, phase-II trial. In this study, sustained remission until week 52 was achieved in 59.3% of patients treated with secukinumab compared to 8.0% of patients who received placebo. 127 Finally, the IL-23 blocker guselkumab is currently under evaluation but no data are available yet, and therefore, its future for GCA treatment is still uncertain.
In addition, some negative past experiences with rituximab and the uncertainty regarding the role of B-cells in disease pathogenesis have significantly reduced the appeal of this drug for treatment of GCA. Not surprisingly, no trials evaluating the efficacy of rituximab in GCA are currently ongoing and, as far as we know, none are planned. However, the recent publication of a proof-of-concept trial reporting promising results of rituximab in PMR might encourage the future design of new studies in GCA as well. 128
Finally, new immunosuppressive molecules with innovative mechanisms of action are appearing in rheumatology and it is plausible that, after they will be investigated in more common diseases such as rheumatoid arthritis, they will be also evaluated in GCA. Among these, it is worth mentioning ABBV-154, a novel antibody drug conjugate composed of adalimumab linked to a glucocorticoid receptor modulator. A phase-II, randomized, placebo-controlled trial in PMR patients has just started recruiting patients, 129 and results of this study will probably determine its possible application in GCA.
Treatment discontinuation
At the present time, only a relatively small fraction of patients with GCA achieve definitive, long-lasting (i.e., ⩾3 years) treatment-free disease remission.106,130 In fact, in order to avoid disease relapse or progression, most require chronic DMARDs, low-dose glucocorticoids, or even combination therapy. When to attempt and how to manage suspension of therapy is still a matter of debate, but we are confident this topic will be successfully addressed in the not-so-distant future.
Suspension of glucocorticoids will certainly remain one of the main goals of GCA management even in 10 years. However, what is likely to change is how they are employed (see paragraph 4.2).
A similar question surrounds strategies for suspension of glucocorticoid-sparing agents, particularly of tocilizumab. Data from GiACTA part-II revealed that in ~60% of patients disease flared up upon tocilizumab suspension. 131 One strategy might be to keep these patients on tocilizumab chronically, 132 but this approach might expose them to a higher risk of infections and, in addition, has a significant economic impact. Potential alternatives could be increasing the administration interval (i.e. to every 2 weeks or longer), after the first year of weekly tocilizumab, or to follow-up the first year of tocilizumab therapy with a course of a conventional DMARD (e.g. methotrexate). Such strategies must be evaluated through rigorous clinical trials before they can be widely embraced.
Prognosis
Even if GCA does not lead to an overall increased risk of mortality, the frequency of vascular events (such as, stroke, coronary and peripheral arterial disease, venous thromboembolism) is higher in patients than in age- and sex-matched controls.92,133–135 Besides the disease itself, a major contributing factor to GCA-related morbidity is the use of glucocorticoids and will continue to be a driving force behind efforts to develop glucocorticoid-sparing therapeutics in future. Additional treatment strategies will probably be evaluated, including possibly prophylactic introduction of low-dose aspirin. The latest EULAR recommendations discouraged its extensive use (unless indicated for concomitant diseases). This recommendation was based on two cohort studies and a meta-analysis which showed no significant beneficial effects.106,136–138 Nevertheless, no rigorous interventional trial has yet been conducted; these may be undertaken in the next years. Obviously, such studies must also evaluate if the potential beneficial effects of this strategy are counterbalanced by adequate safety. Another class of drugs commonly used to prevent cardiovascular complications, statins, could be further evaluated. Currently available studies are all retrospective and failed to demonstrate a reliable role of this class of drugs in modifying disease course and rate of ischemic complications.139–141 However, until prospective trials are conducted, early statin use in patients with GCA should not be definitively ruled out.
How prevent therapeutically structural vascular damage associated with GCA (aneurysms and stenoses) is another key unmet need in GCA research. First of all, we must understand if tocilizumab and other biologic DMARDs potentially approved in the future, can actually play a role in preventing these late-onset complications. In addition, it would also be interesting to investigate whether the introduction of these agents may have the ability of stopping, or at least slowing the progression of vascular complications once aortic aneurysm or arterial stenosis have already started to develop. The answer to these questions can be only obtained through a long-term (e.g. at least 5-year) careful evaluation of treated patients compared to a control group.
Risk of infection: is there a rationale for antimicrobial prophylaxis?
Existing literature suggests that risk of all-cause infections is increased among patients suffering from GCA. Disease-related factors such as immunosenescence, as well as use of immunosuppressive drugs, are primary contributors to this increased risk. 116 The risk of infections related to glucocorticoids is directly related to both (mean) daily and cumulative dose (especially in the first year of treatment) and progressively declines thereafter but does not appear to differ among distinct disease phenotypes. 142 Infections are an independent predictor of mortality and, together with cardiovascular events, one of the main causes of death among patients with GCA.143–145 Sepsis and pneumonia are the leading causes of hospitalization and death among patients with GCA. Other serious infections include soft tissue, opportunistic and urinary tract infections.145,146 A key question for the coming years is how to reduce the burden of such complications. Optimization of immunosuppressive drugs use and dosing is an important but not sufficient first step, considering the older age, immunosenescence, and frailty of the GCA population. Unanswered is whether antimicrobial prophylaxis should be pursued, and at what time points. The association between high-dose glucocorticoid therapy and opportunistic infections, particularly pneumocystis jirovecii pneumonia (PJP), is now well established in both non-rheumatological and rheumatological diseases.147–149 Trimethoprim/sulfamethoxazole (TMP-SMX) has been proved to be effective as a primary prophylaxis for PJP in patients suffering from rheumatological diseases treated with high dose (⩾30 mg/day prednisone) glucocorticoid therapy, with an overall favorable safety profile. 148 Although this study included only few patients with LVV, TMP-SMX prophylaxis should be considered on an individual basis, particularly in those requiring high glucocorticoid doses for a prolonged time, those treated with cyclophosphamide (considering that his agent is rarely used in GCA) or having a low count of CD4 + lymphocytes. The utility of universal PJP prophylaxis in patients with GCA has not been addressed so far in proper clinical trials. Furthermore, it would be intriguing to assess whether chronic TMP-SMX use could also reduce the incidence of other severe infections, as it has been noted in patients with ANCA-associated vasculitis. 150
GCA: treatable versus curable disease?
While current therapies for GCA are able to control disease symptoms and reduce the occurrence of severe complications such as blindness, they are not curative of the disease. Insights into the disease pathogenesis may at some point contribute to mitigation of developing the disease, but currently, no therapy can be regarded as truly curative once the disease is established. Even in patients who clinically appear to be in longer term, treatment-free remission, the reappearance of disease after sometimes quite prolonged periods, and the occurrence of long-term disease-related complications is evidence of a more chronic disease course over many years. Is a ‘cure’ for GCA on the horizon? Not yet. Like most autoimmune inflammatory rheumatological diseases, GCA is an immunologically and genetically complex disease. Better understanding of the underlying disease process and perhaps recent evidence from other forms of primary vasculitides such as ANCA-associated vasculitis suggest that very long-term remission, if not cure, is certainly possible.
Conclusion
Although in the last decades great improvements have been achieved in pathogenesis, diagnosis, and treatment of GCA, some questions still remain unanswered. The next 10 years will be crucial for a better understanding and management of this polyhedral disease. The purpose of this review was to shed some light on future perspectives in the field of GCA. A thorough clarification of initial mechanisms of inflammation, and a thoughtful stratification into different clinical subsets of patients with GCA are the first steps toward a better understanding of the disease and, subsequently, toward a more tailored use of existing and future therapeutic options. Definition of the role of existing and new imaging techniques, both in diagnosis and monitoring, definition of minimal required dose of glucocorticoids and other immunosuppressive agents, further development of novel drugs, identification of prognostic factors for long-term outcomes and management of treatment discontinuation are just some of the central topics of the research agenda in years to come (Table 2).
Research agenda.
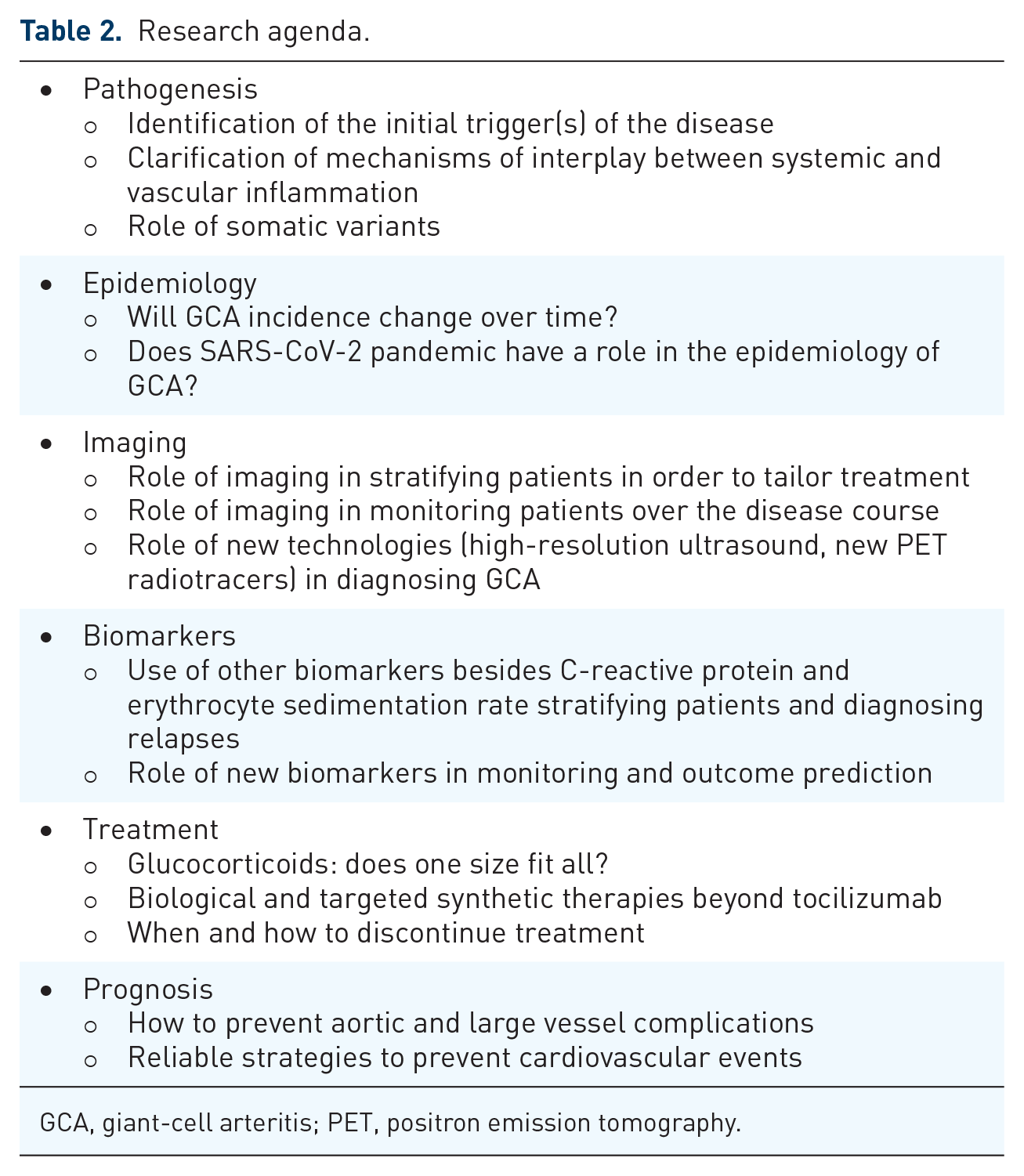
GCA, giant-cell arteritis; PET, positron emission tomography.
Footnotes
Author contribution(s)
Ethics approval
Not applicable, no subjects involved. All authors approved publication of this article
Availability of data and materials
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FB reported receiving consultancy fees, honoraria, and travel expenses from Horizon Pharma, Roche, Sanofi and Galapagos. He served as principal investigator and site investigator in GCA and PMR trials (Sanofi). CD has received consulting/speaker’s fees from Abbvie, Eli Lilly, Janssen, Novartis, Pfizer, Roche, Galapagos, and Sanofi. ELM has received consulting/speaker’s fees from Boehringer Ingelheim and Gilead, editorial royalties from UpToDate, Data Safety Monitoring Board for Horizon Pharmaceuticals