
Abstract
Background:
Patients with inflammatory bowel disease (IBD) have an excess burden of axial spondyloarthritis (axSpA), which, if left untreated, may significantly impact on clinical outcomes. We aimed to estimate the prevalence of axSpA, including previously undiagnosed cases, in IBD patients from studies involving cross-sectional imaging and identify the IBD features potentially associated with axSpA.
Methods:
PubMed, Embase and Cochrane databases were searched systematically between 1990 and 2018. Article reference lists and key conference abstract lists from 2012 to 2018 were also reviewed. All abstracts were reviewed by two authors to determine eligibility for inclusion. The study inclusion criteria were (a) adults aged 18 years or above, (b) a clinical diagnosis of IBD and (c) reporting identification of sacroiliitis using cross-sectional imaging.
Results:
A total of 20 observational studies were identified: 12 used CT, 6 used MR and 2 utilised both computed tomography (CT) and magnetic resonance (MR) imaging. Sample sizes ranged from 25 to 1247 (a total of 4096 patients); 31 studies were considered to have low selection bias, 13 included two or more radiology readers, and 3 included rheumatological assessments. The prevalence of sacroiliitis, the most commonly reported axSpA feature, ranged from 2.2% to 68.0% with a pooled prevalence of 21.0% [95% confidence interval (CI) 17–26%]. Associated IBD features include increasing IBD duration, increasing age, male sex, IBD location, inflammatory back pain and peripheral arthritis. No significant difference in the prevalence of sacroiliitis between Crohn’s disease and ulcerative colitis was identified. Study limitations include variability in the individual study sample sizes and patient demographics.
Conclusion:
This review highlights the need for larger, well-designed studies using more sensitive imaging modalities and multivariable modelling to better estimate the prevalence of axSpA in IBD. An improved knowledge of the IBD phenotype(s) associated with axSpA and use of cross-sectional imaging intended for IBD assessment to screen for axSpA may help clinicians identify those patients most at risk.
Keywords
Introduction
Spondyloarthritis (SpA) is a term used to describe a group of chronic inflammatory musculoskeletal diseases that can present with axial and/or peripheral joint disease. SpA can be further subdivided into axial predominant (axial spondyloarthritis) and peripheral predominant (peripheral spondyloarthritis) forms. The axial predominant forms include ankylosing spondylitis (AS), or radiographic axial spondyloarthritis, and non-radiographic axial spondyloarthritis. These are characterised by a number of SpA features including the presence of inflammatory back pain (IBP). AS requires evidence of sacroiliitis on plain film radiographs using the modified New York criteria (mNYc). 1 Non-radiographic axial spondyloarthritis is diagnosed using a combination of clinical features, human leucocyte antigen B27 (HLA-B27) status and axial magnetic resonance imaging (MRI) using the assessment of spondyloarthritis international society (ASAS) criteria but does not require radiographic evidence of sacroiliitis. 2 The peripheral predominant forms of SpA include psoriatic arthritis (typically seen in the context of skin or nail psoriasis, or a first-degree family history of psoriasis), reactive arthritis (aseptic inflammatory arthritis associated with a recent infective episode, most commonly gastrointestinal or sexually transmitted infections) and enteropathic arthritis [associated with the presence of inflammatory bowel disease (IBD)].
The prevalence of SpA has been estimated to range between 10 per 100,000 (Japan) and 2500 per 100,000 (Alaska and Russia) of the general population. 3 There is an association with HLA-B27, which is estimated to be present in 50–95% of patients with SpA depending on ancestral origin and SpA subtype. 4 Patients with SpA have an excess burden of IBD, manifested as Crohn’s disease (CD) and ulcerative colitis (UC). Subclinical gastrointestinal inflammation may also be detected endoscopically and/or histologically. The prevalence of IBD in SpA has been estimated to range from 4% to 12%,5–9 with subclinical gut inflammation being reported in approximately 40–50% of SpA patients.10,11 However, there are limited data on the prevalence of SpA in patients with IBD. Peripheral arthropathy has been reported in 5–14% of UC patients and 10–20% of CD patients, with AS being reported in 1–16% of IBD patients.12–15 SpA can have a significant negative impact on various aspects of quality of life, including employment, social participation and intimacy,16–19 but with evidence of potential improvement following the initiation of conventional or biologic disease modifying anti-rheumatic drugs (DMARDs). 20
Novel biologic therapies for SpA have been developed to target the dysregulated innate and adaptive immune responses that underpin pathogenesis. Such targets include interleukin (IL)-17, IL-12/23 and tumour necrosis factor (TNF). These cytokines also have pathogenic roles in IBD.21–24 Several anti-TNF biological therapies are now co-licensed to treat both IBD and SpA, with IL-23 inhibitor trials showing promise for use in IBD. While treatment efficacy may vary by indication, if used appropriately and early in the course of disease, they can have a significant impact on disease burden.25,26 Timely diagnosis and treatment is therefore potentially crucial.
Sacroiliitis is the radiological hallmark of axial spondyloarthritis (axSpA), but in isolation is not diagnostic. Historically, sacroiliitis has been identified using plain radiographs of the sacroiliac joints (SIJs), forming part of the mNYc for AS, 1 and, in more recent years as a major component in the ASAS criteria. 2 However, over the last 30 years, cross-sectional imaging, with computed tomography (CT) and MRI, has become increasingly utilised. CT scans can better detect erosions, sclerosis and ankylosis, compared with plain radiographs.27–30 MRI offers the additional advantage of being able to identify acute inflammatory changes related to bone marrow oedema and chronic inflammatory changes related to fatty atrophy. MRI is therefore more sensitive at detecting the early signs of axSpA,27,31,32 and does not confer ionising radiation, thereby making it the imaging modality of choice in the 2009 ASAS guidelines. 27 Magnetic resonance enterography (MRE) of the small bowel is a type of oral contrast MRI scan used to aid the diagnosis and complications of IBD, principally small bowel CD.33,34 This form of imaging is available in some secondary care and most tertiary care centres. MRE imaging involves a variety of axial and coronal T1 and T2-weighted sequences to image the small bowel but also capture the axial skeleton, including the SIJs in coronal and axial views. These scans can therefore be used to assess the sacroiliac joints for features of sacroiliitis including joint erosions, ankylosis and juxta-articular signal changes. However, the radiological assessment of this aspect of the scan is often overlooked and deemed beyond the remit of the initial MRE request.
The aims of this systematic literature review (SLR) were to estimate the prevalence of sacroiliitis, including previously undiagnosed cases, in IBD patients as determined by cross-sectional imaging in the form of MRI and CT; and identify the clinical features of IBD associated with axSpA/sacroiliitis.
Methods
The SLR was performed in keeping with the meta-analyses of observational studies in epidemiology (MOOSE) guidelines. 35 Original articles in all languages between the years 1990 and 2018 were retrieved from PubMed, EMBASE and Cochrane databases using the search criteria detailed in Supplemental File S1. The articles’ reference lists were checked for further relevant literature. Abstracts from the following Annual Meetings (American College of Rheumatology, European League Against Rheumatism, Group for Research and Assessment of Psoriasis and Psoriatic Arthritis, British Society of Rheumatology, Gent Spondyloarthritis) between the years 2012 and 2018 were also reviewed. All unique abstracts were reviewed independently by two authors (JE, MS) to determine their eligibility, and any discrepancies were decided by consensus. Full papers were assessed where available. When results were only available in abstract form, the authors were contacted for additional unpublished results.
Eligibility criteria
Inclusion criteria for studies included (a) adults aged 18 years or above, (b) a clinical diagnosis of IBD and (c) reporting identification of sacroiliitis based upon cross-sectional imaging with either MRI or CT. Studies were excluded if they pre-screened patients for IBP and then selected only those with IBP.
Assessment of methodological quality
The studies were assessed in terms of their data collection methods by a quality assessment tool comprising eight yes/no answers. This was based on the National Institutes of Health (NIH) quality assessment tool for observational cohort and cross-sectional studies and was adjusted for our purposes. 36 We included questions about a clearly stated objective, clearly defined study population, representative sample, appropriate recruitment methods, sample size calculations, exposure of interest (IBD) being measured prior to the outcome being measured, use of standard criteria for the assessment of the condition (sacroiliitis) and the condition being measured reliably (were two or more radiology readers used). The quality assessment tool with instructions on how we applied it can be found in Supplemental File S2. For the purposes of this SLR, each individual criteria question was considered to be met only if the study fulfilled all of the requirements for that particular criteria question.
Pooling of data
Forest plots were generated to illustrate the variation across the studies in the prevalence of sacroiliitis in IBD and to compare the reported prevalence of sacroiliitis according to the imaging modality used. The forest plots were generated using the ‘metaprop’ command in Stata 16 with a random effects model. 37 I 2 was used to measure the between-study heterogeneity.
Results
A total of 551 abstracts were retrieved from the PubMed, EMBASE and Cochrane databases and the rheumatology conference search. All of the retrieved abstracts were available in the English language. A total of 30 abstracts met the SLR eligibility criteria and were reviewed by two independent reviewers (JE, MS). After excluding 11 studies and identifying a further 1 study from checking reference lists, a total of 20 observational studies were finally selected (see Figure 1).
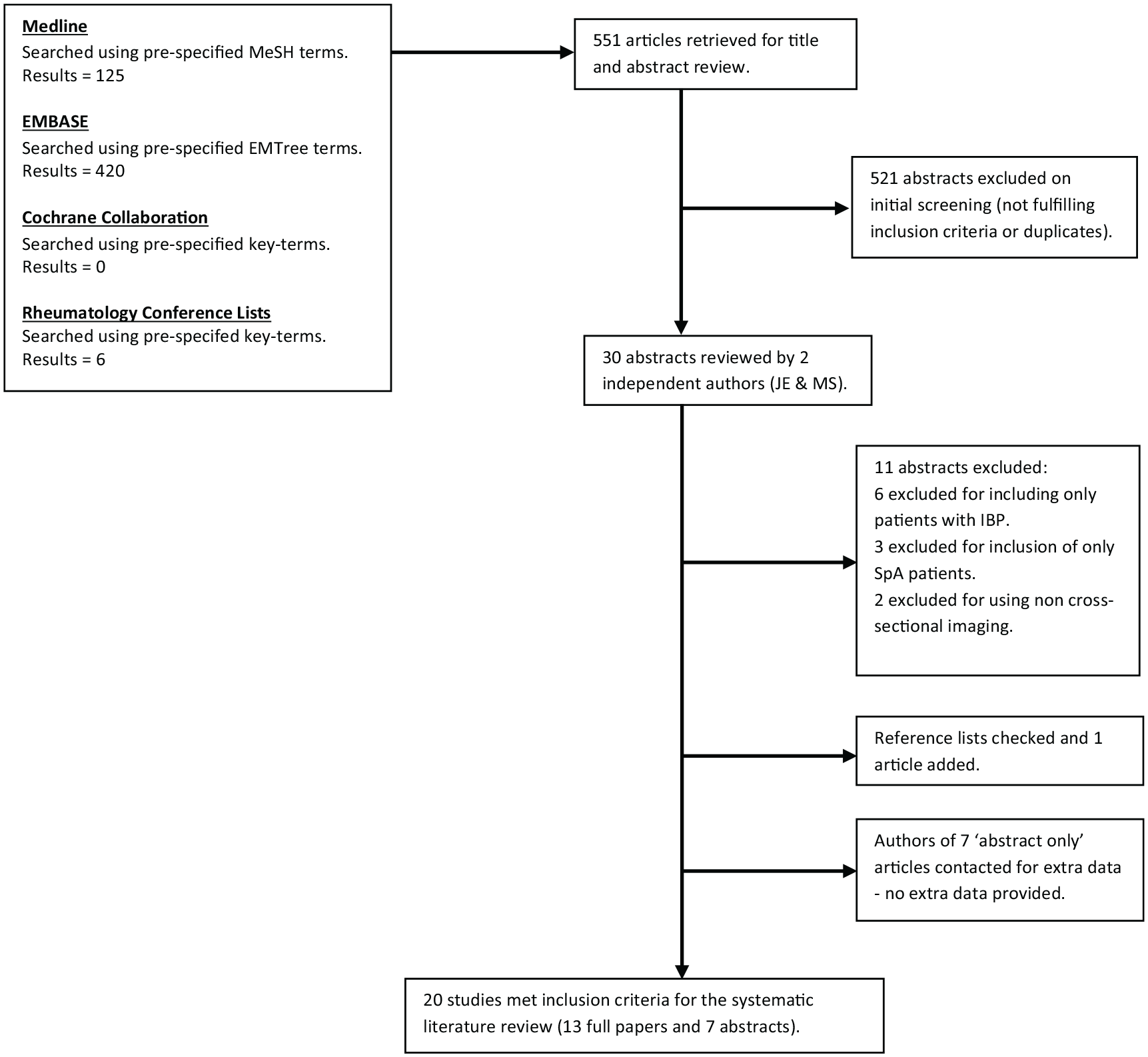
Systematic literature review eligibility algorithm.
Table 1 illustrates the methodological assessment used and the percentage of studies that scored positive on each item. Of the included studies, 13 were papers and 7 were abstracts29,30,38–55 (see Table 2); 14 studies used CT-sacroiliitis, 4 MRE and 4 axial MRI to determine the prevalence of axSpA in IBD cases, with 2 studies including both CT and MR imaging modalities.39,53 A summary of the cohorts’ demographics and IBD phenotypes are detailed in Table 2 and the IBD features associated with sacroiliitis are summarised in Table 3. Sample sizes ranged from 25 to 1247 patients (a total of 4096 patients), age range of subjects from 28.8 to 50.2 years and IBD duration ranged 1.5–12.6 years. Of the 20 studies, 2 included three independent radiologist readers, 11 included two readers, 1 used one reader and 6 did not state the reader number. The presence of IBP was assessed in 10 studies, 5 included a control group (defined as either healthy subjects or subjects with other diseases) and only 3 included a clinical rheumatology assessment.
Study Assessment Tool Summary (adapted from the NIH study quality assessment tool for observational cohort and cross-sectional studies). 36

IBD, inflammatory bowel disease; NIH, National Institutes of Health.
Summary of studies.

p < 0.05 for IBD versus controls.
B, biologic therapy; BMO, bone marrow oedema; CD, Crohn’s disease; CI, confidence intervals; CS, corticosteroids; CT, computed tomography; F, female; gastro, gastroenterology; GI, gastrointestinal; HLA-B27, human leucocyte antigen B27; IBD, inflammatory bowel disease; IBP, inflammatory back pain; IS, immunosuppressant (methotrexate, azathioprine, tacrolimus, cyclosporin, aminosalicylate); M, male; MRE, magnetic resonance enterography; MRI, magnetic resonance imaging; rheum, rheumatology; SC, secondary care; SIJs, sacroiliac joints; TC, tertiary centre; TNF, tumour necrosis factor; UC, ulcerative colitis.
Features of IBD associated with the presence of sacroiliitis on cross-sectional imaging.

AS, ankylosing spondylitis; CD, Crohn’s disease; CI, confidence intervals; CT, computed tomography; GI, gastrointestinal; IBD, inflammatory bowel disease; MRE, magnetic resonance enterography; MRI, magnetic resonance imaging; NA, not applicable; NS, not stated or not included in study; SI, sacroiliitis; UC, ulcerative colitis.
A total of 14 studies used imaging initially intended for the evaluation of IBD to assess for sacroiliitis, whilst 6 studies used dedicated MRI or CT imaging of the SIJs. The prevalence of sacroiliitis in IBD ranged from 2.2% to 68.0%, with a pooled prevalence of 21.0% [95% confidence interval (CI) 17–26%] and an I 2 of 93.6% (see Figure 2). In the five studies with a control group, the prevalence of sacroiliitis was higher in the IBD group: 5.6 versus 15.5%; 7.5 versus 20.0%; 8.3 versus 15.4%; 0.0 versus 68.0%; and 3.2 versus 29.0% in controls and IBD cases, respectively.

Prevalence of sacroiliitis and axSpA using the different imaging modalities
In the 14 studies using CT, the prevalence of sacroiliitis varied from 2.2% to 68.0%29,30,38–40,43,44,46–48,52–55 (Tables 2 and 3). In the four studies using MRI, the prevalence of sacroiliitis ranged from 20.0% to 38.6%.41,45,50,51 The prevalence of sacroiliitis in the four studies using MRE ranged from 15.4% to 28.9%.39,42,49,53
For the studies using IBD imaging to assess for sacroiliitis, which included CT and MR imaging modalities, the prevalence ranged from 2.2% to 29.1% compared with 20.0% to 68.0% in the studies using dedicated SIJ (CT and MR) imaging (Tables 2 and 3). Comparing MRI with CT imaging of the SIJs, the prevalence in the MRI studies ranged from 20.0% to 38.6% compared with 32.3% to 68.0% in the CT studies. A higher prevalence of sacroiliitis was seen in the studies using dedicated imaging of the SIJs, with four of the six SIJ imaging studies observing this (see Figures 2 and 3).30,45,47,51 All of the studies utilising SIJ CT imaging observed a higher prevalence compared with only half of the studies using SIJ MR imaging. In contrast, only one study using IBD imaging was found to observe a higher prevalence. 49

Four of the studies assessed patients for a diagnosis of AS or axSpA,41,44,45,51 with two studies using the mNYc and one study using the ASAS criteria.44,45,51 One study did not comment on the criteria used. 41 The prevalence of axSpA/AS in these studies ranged from 1.2% to 33.3%.
IBD and sacroiliitis
A total of 11 studies included both CD and UC patients38–42,44,47,51–54 (Table 2). From these studies, the prevalence of sacroiliitis in CD cases ranged from 8.7% to 30.3% compared with 8.0% to 34.4% in UC. Seven of these studies found no significant difference in the prevalence of sacroiliitis between CD and UC,38,40–42,47,52,53 but the remaining four studies did not comment on this (Table 3). One study demonstrated a higher probability of sacroiliitis with longer IBD duration, 53 two with IBD location (upper gastro-intestinal, ileocolonic and peri-anal involvement),44,45 and one with non-penetrating CD. 40 However, no association was identified between sacroiliitis and IBD activity.40,42,44,53
Age, sex and sacroiliitis
Seven studies commented on the association of sex with sacroiliitis,30,40,42,44,47,52,53 and seven with age and sacroiliitis (Table 3).30,40,42,44,47,50,53 Two studies found a higher prevalence of sacroiliitis with increasing age, but this was not adjusted for IBD duration.42,50 Two studies found that sacroiliitis was more common in male IBD patients,40,52 whilst another found it to be more common in female CD patients, although there was no significant difference in the total IBD group. 42
Musculoskeletal symptoms, HLA B27 and sacroiliitis
Four studies included IBP assessment prior to recruitment,29,44,47,49 and six included an IBP assessment following recruitment,39,41,45,48,50,51 but the forms of assessment varied and were not always stated (Table 2). Two of the studies found an association between the presence of IBP and sacroiliitis.29,45 Three studies, two of which used CT imaging and one MRI, included only patients without IBP.29,47,49 The range of sacroiliitis in this set of studies with asymptomatic IBD patients was 20.0–32.3% compared with a range of 2.2–68.0% in the studies that did not pre-screen for IBP. An association of sacroiliitis with peripheral arthritis was reported in two studies (Table 3).40,41 Five studies commented on the presence of HLA-B27 in their patient cohort but only two studies reported its association with sacroiliitis (Table 2).45,52 The proportion of IBD cases with sacroiliitis who were HLA B27-positive in these studies was 16.0 and 41.2%.
Discussion
This SLR summarises what is known on the prevalence of sacroiliitis, and therefore inferred axSpA in IBD patients and highlights gaps in the current canon of knowledge. AxSpA appears to affect a substantial number of IBD patients and is significantly underdiagnosed. This is an important finding given that a delayed diagnosis of axSpA and/or untreated axSpA, could lead to irreversible structural damage. This in turn can result in significant disability and pain, which can have a negative impact on participation in employment, social activities and function.16–18,56,57 Such complications could be potentially minimised if appropriate therapy is commenced early in the course of disease.25,26
We have shown that the prevalence of sacroiliitis on cross-sectional imaging in IBD patients ranges from 2.2% to 68.0%, with a pooled prevalence of 21.0% (95% CI 17–26%). However, given that there was a high level of heterogeneity between the studies, this estimate should be interpreted with caution. Previous studies using plain radiographs have estimated this to be 9.2–24.0%, and the disparity is likely explained by the poorer sensitivity of plain radiographs.58–61 This SLR also shows that dedicated cross-sectional (MR and CT) SIJ imaging is more sensitive in detecting sacroiliitis than cross-sectional imaging intended for IBD assessment. Dedicated CT SIJ imaging was shown to be more sensitive than dedicated SIJ MRI and is reflective of the fact that CT imaging is more sensitive than MRI at detecting chronic bony changes.
There were limited data on the IBD clinical characteristics and demographics associated with sacroiliitis, with 13 studies reporting on this.29,30,39–42,44,45,47,49,50,52,53 Only 11 studies included both CD and UC patients, with 8 including only CD patients (IBD type was not stated in 1 study). It is unclear if there was any associated selection bias for CD patients in these studies. This SLR revealed no significant difference in the prevalence of sacroiliitis in patients with CD or UC.38,40–42,44,47,53 Similar rates of axial involvement in CD and UC have been reported previously, 12 but an increased risk of axial involvement and peripheral joint involvement in patients with CD compared with UC has been suggested elsewhere.13,62–64 There was no reported association of sacroiliitis with current or recent (within last 6 months) endoscopic IBD activity,40,42,44 or recent (within last 3 months) clinical activity, 40 supporting the conclusions of previous studies.65–67 Two studies identified an association of sacroiliitis with IBD location, with an increased prevalence of upper gastro-intestinal, ileocolonic and peri-anal involvement in patients with sacroiliitis.44,45 Hwangbo et al. did adjust for IBD duration, 44 but this was not stated in the study by Orchard et al. 45 This does to some degree reflect the results of previous studies that reported an increased risk of joint complications in patients with colonic CD, more extensive involvement in UC and with peri-anal disease.64,68
There was only a weak association of sacroiliitis with IBD inflammatory phenotype (non-penetrating CD) and increased IBD duration, with one study reporting on each of these.40,53 Two studies reported an association of sacroiliitis with male sex,40,52 whilst another reported an association with female CD patients. 42 The cause of these differing results is unclear, but we would expect to see a higher frequency of sacroiliitis in male IBD patients, as per Kelly et al. and Nangit et al., given that AS is more common in men.56,69 One of the studies used MRE whilst two used CT imaging, yet the study methods were otherwise similar. The mean ages were similar in the studies by Leclerc-Jacob et al. and Kelly et al. (34.0 years versus 37.0 years), although specific mean ages for male and female groups were not specified in either study. Furthermore, these three studies did not state an adjustment for age or IBD duration. Two studies reported an increased risk of sacroiliitis with increasing age.42,50 Whilst neither study stated if they had adjusted for IBD duration, neither found a significant increased risk of sacroiliitis with IBD duration.
Two studies reported an increased risk of sacroiliitis with the presence of peripheral arthritis,40,41 which is expected given the co-existence of peripheral and axial joint disease in SpA. However, only one of these studies stated an adjustment for IBD duration. 41 In terms of IBP, a narrower range of sacroiliitis, with a smaller upper prevalence value, was found in the sub-group of studies that selected IBD patients without IBP.29,47,49 A lower prevalence of sacroiliitis would be expected in this subset of studies, given that the absence of IBP suggests lower levels of SIJ inflammation.
The reported association between the presence of HLA-B27 variants and sacroiliitis ranged from 16.0% to 41.2% in this SLR. These values are lower than the reported prevalence of HLA-B27 in UK patients with IBD and SpA (50–60%). 4
There are some limitations of this SLR and of the studies included. These may in part account for the wide range in the prevalence of sacroiliitis reported in this SLR (2.2–68.0%). In terms of the individual studies, there is significant variation in the study methods used, which may in part contribute to the disparity of results. The studies included a wide range of sample sizes, with four studies having a relatively small sample size (<50 participants). There was also variability in the participant demographics with a wide range of age and IBD duration. IBD associated SpA can precede or occur after IBD onset and therefore increased IBD duration would be expected to be correlated positively with sacroiliitis prevalence.66,68 Most studies did not adjust for this using multivariable models. There were varying proportions of male and female participants included in the studies and, given that AS is more common in men, this may have had an impact on the results obtained. The variation in the geographical region of the studies may have also influenced the different prevalence values reported in view of the known ethnic variation of axSpA. Different proportions of IBD types were included in the studies. As previously discussed, 7 of the 11 studies including both CD and UC reported no significant difference in the prevalence of sacroiliitis between the IBD types. However, the remaining four studies did not report on this and many previous studies have reported axSpA to be more common in CD than UC. Therefore, this may have influenced the results in this subset of studies and therefore potentially contributed to the variation in prevalence results. The inclusion of asymptomatic patients in some of the studies may have also influenced the findings, given that the likelihood of sacroiliitis is lower in patients without back pain. The radiology reader number varied between the studies, with one using one reader and six studies not stating reader number. The use of double radiology reading (two radiologists reviewing the images independently) has been shown to increase the number of changed reports and thus, without such consensus reading, the reliability of studies using one reader comes into question. 70 There is also likely to be variation between the radiology assessors in the different studies, resulting in differences in the assessment for sacroiliitis. Focusing on the two studies with the lowest (2.2%; Bruining et al.) and highest (68.0%; Mester et al.) prevalence values,30,46 both were CT imaging studies. Bruining et al. used the original reports from the CT imaging and it is not clear if the scans were reassessed for sacroiliitis for the purposes of the study. 46 This may explain to some degree the lower prevalence value reported. Mester et al. included a small sample size (n = 25) and did not state patient age, the proportion of male and female patients included, IBD duration, radiology reader number or how the patients were selected in their study. 30 Therefore, it is possible that some or all of these factors contributed to the high prevalence of sacroiliitis reported in their study. A potential limitation of this SLR is the inclusion of both MRI and CT studies because these imaging modalities have different sensitivities for detecting different features of sacroiliitis. Therefore, one would expect different results in terms of the prevalence of sacroiliitis reported in the MR and CT imaging studies. This may account for some of the variation in the reported frequency of sacroiliitis and highlights limitations in their comparability. In view of this, we separated the sacroiliitis prevalence results in terms of imaging modality to demonstrate this variation (see Figure 3), which showed dedicated CT imaging of the SIJs to be the most sensitive form of imaging for sacroiliitis. Most IBD patients will have some form of cross-sectional imaging to assess their IBD, but MRI (or MRE) availability is limited, resulting in some heterogeneity in the imaging type used for IBD patients (CT or MRI). Therefore, it is useful to include the results of both MR and CT imaging studies to highlight the potential benefit and variation in their sensitivity to screen for sacroiliitis in IBD patients, which can be applied to the real world. There is also some overlap in the features of sacroiliitis that can be detected in both imaging modalities, including erosions, sclerosis and ankylosis. The majority of the studies included these features in their assessment for sacroiliitis and therefore, for the purposes of this study, the sacroiliitis prevalence values were comparable to some degree for the two forms of imaging.
Comparison groups are an important method of contextualising results, but only 5 of 20 studies included these. The assessment for IBP also varied with ten studies assessing for this but using differing methods. Only three studies included a rheumatological assessment, an important consideration if an attempt is to be made to assess for a diagnosis of axSpA. A total of 13 studies adopted methods to minimise selection bias, either using consecutive IBD patients or complete cohorts of IBD patients, but the method of patient selection was either not stated or only patients without IBP were included in the remaining studies. There was also variation in the assessment of the association of sacroiliitis with IBD type (7 of 20 studies), IBD location (5 of 20 studies), IBD activity (4 of 20 studies), increasing age (7 of 20 studies), sex (7 of 20 studies), IBD duration (7 of 20 studies) and peripheral arthritis (3 of 20 studies). HLA-B27 testing was reported in only five studies and only four included data on axSpA prevalence. Seven of the articles included were abstracts, thereby limiting the amount of information available.
The imaging used for axSpA assessment in these studies was limited to the SIJs, and was, in many cases, intended for IBD assessment, whilst the gold standard imaging assessment for axSpA involves dedicated MRI of the spine and SIJs. 27 However, this provides some preliminary insight into the potential utility of IBD imaging, such as MRE, as a screening tool for sacroiliitis in IBD patients. This in turn could improve the referral process from gastroenterology to rheumatology for axSpA assessment and, ultimately, reduce the time to diagnosis and treatment.
Conclusion
To our knowledge this is the first SLR to assess the prevalence of axSpA in IBD cases using cross-sectional imaging. We have highlighted the need for larger, well-designed studies using more sensitive imaging modalities such as MRI and using multivariable modelling to better estimate the prevalence of total and undiagnosed axSpA in IBD patients. There is a lack of knowledge on the IBD phenotype most associated with axSpA, which might help clinicians better screen patients most at risk. Cross-sectional imaging intended for the assessment of IBD, such as MRE, might be used to screen for axSpA, perhaps even before the onset of musculoskeletal symptoms and without significant additional cost or inconvenience to the patient. Such patients could then be referred for rheumatological assessment, thus potentially reducing the delay in diagnosis and treatment. Such cross-speciality working between rheumatology, gastroenterology and radiology is in keeping with all international recommendations for the management of IBD and SpA.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X21996973 – Supplemental material for Prevalence of axial spondyloarthritis in patients with inflammatory bowel disease using cross-sectional imaging: a systematic literature review
Supplemental material, sj-docx-1-tab-10.1177_1759720X21996973 for Prevalence of axial spondyloarthritis in patients with inflammatory bowel disease using cross-sectional imaging: a systematic literature review by Jobie Evans, Mark Sapsford, Scott McDonald, Kenneth Poole, Tim Raine and Deepak R. Jadon in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X21996973 – Supplemental material for Prevalence of axial spondyloarthritis in patients with inflammatory bowel disease using cross-sectional imaging: a systematic literature review
Supplemental material, sj-docx-2-tab-10.1177_1759720X21996973 for Prevalence of axial spondyloarthritis in patients with inflammatory bowel disease using cross-sectional imaging: a systematic literature review by Jobie Evans, Mark Sapsford, Scott McDonald, Kenneth Poole, Tim Raine and Deepak R. Jadon in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.