
Abstract
Introduction:
Psychological factors have been associated with knee osteoarthritis pain severity and treatment outcomes, yet their combined contribution to phenotypic heterogeneity is poorly understood. In particular, empirically derived psychological profiles must be replicated before they can be targeted or considered for treatment studies. The objectives of this study were to (1) confirm previously identified psychological profiles using unsupervised clustering methods in persons with knee osteoarthritis pain, (2) determine the replicability of profiles using supervised machine learning in a different sample, and (3) examine associations with clinical pain, brain structure, and experimental pain.
Methods:
Participants included two cohorts of individuals with knee osteoarthritis pain recruited as part of the multisite UPLOAD1 (n = 270, mean age = 56.8 ± 7.6, male = 37%) and UPLOAD2 (n = 164, mean age = 57.73 ± 7.8, male = 36%) studies. Similar psychological constructs (e.g. optimism, coping, somatization, affect, depression, and anxiety), sociodemographic and clinical characteristics, and somatosensory function were assessed across samples. UPLOAD2 participants also completed brain magnetic resonance imaging. Unsupervised hierarchical clustering analysis was first conducted in UPLOAD1 data to derive clusters, followed by supervised linear discriminative analysis to predict group membership in UPLOAD2 data. Associations among cluster membership and clinical variables were assessed, controlling for age, sex, education, ethnicity/race, study site, and number of pain sites.
Results:
Four distinct profiles emerged in UPLOAD1 and were replicated in UPLOAD2. Identified psychological profiles were associated with psychological variables (ps < 0.001), and clinical outcomes (ps = 0.001–0.03), indicating good internal and external validation of the cluster solution. Significant associations between psychological profiles and somatosensory function and brain structure were also found.
Conclusions:
This study highlights the importance of considering the biopsychosocial model in knee osteoarthritis pain assessment and treatment.
Introduction
Knee osteoarthritis (OA) is a leading cause of chronic musculoskeletal pain and pain-related disability among middle-aged and older adults.1,2 Pain and pain-related disability are poorly related to peripheral markers of joint degeneration, 3 and are widely variable, 4 complicating effective treatment.3,5,6 Recent efforts to better understand knee OA symptom heterogeneity have revealed multiple factors across the biopsychosocial model, 7 which may influence the pain experience.4,8–11 Particularly, psychosocial and neurobiological factors have been consistently associated with knee OA symptoms.12–15 Furthermore, there is a growing recognition that multiple psychosocial factors influence pain and treatment outcomes in knee OA.16,17
In an earlier study, 9 we identified four distinct psychological profiles in individuals with knee OA symptoms based on multiple measures of positive and negative psychological constructs. These profiles showed associations with clinical pain and function, and somatosensory processing. These findings have been further supported by more recent investigations examining the combined influence of multiple psychological factors on clinical outcomes in persons with chronic musculoskeletal pain.11,18,19 However, to our knowledge, no other researcher has investigated the presence of distinct psychological profiles in persons with knee OA based on multiple positive and negative psychological constructs. While promising, our original findings 9 require further confirmation and replication before these profiles can be considered in the development of targeted interventions for knee OA pain. If confirmed and replicated, these psychological profiles may elucidate important considerations in knee OA pain heterogeneity and aid in developing tailored interventions for optimized clinical outcomes.
There is also evidence for the role of neurobiological factors in the heterogeneity of OA knee pain. Numerous studies have shown increased pain sensitivity and altered endogenous pain modulation in adults with knee OA pain.10,14,20,21 Furthermore, researchers have identified subgroups in knee OA based on responses to quantitative sensory testing (QST), which display evidence of centrally mediated pain and are related to clinical outcomes.3,10,15 However, the relationships between psychological function and pain processing in knee OA are largely unknown.
The objectives of the present study were to (1) confirm previously identified psychological profiles using a data-driven, unsupervised machine learning approach to cluster psychological characteristics that best define subgroups among individuals in the UPLOAD1 data set, (2) examine the replicability of identified psychological profiles using a supervised machine learning approach to determine if previously identified clusters discriminate among subgroups within a different data set (i.e. UPLOAD2), and (3) explore the associations between these profiles and specific pain and sensory characteristics, including clinical pain, somatosensory function, and brain structure. We hypothesized that (1) previously identified psychological profiles would emerge within a larger sample of individuals, (2) the profiles would replicate in a separate cohort of adults with knee OA, and (3) the profiles would differ significantly across measures of clinical pain, somatosensory function, and brain structure.
Methods
Study samples
The current study leverages data obtained from two separate multisite observational studies, Understanding Pain and Limitations in Osteoarthritic Disease-1 (UPLOAD1), and Understanding Pain and Limitations in Osteoarthritic Disease-2 (UPLOAD2), both aimed at studying ethnic/racial differences in knee OA pain, and conducted at the University of Florida (UF) and University of Alabama, Birmingham (UAB). Studies were approved by the University of Florida (UF) and University of Alabama, Birmingham (UAB) Institutional Review Boards (IRB201400209, IRB201500906). While inclusion/exclusion criteria and recruitment methods were similar across studies, the UPLOAD1 and UPLOAD2 study samples are unique cohorts. This was ensured by limiting participation to one study only (i.e. participants from UPLOAD1 were not allowed to complete UPLOAD2). The UPLOAD2 sample is restricted to those with brain magnetic resonance imaging (MRI) data for the current analysis.
Participants were adults aged 45 to 85 years, who self-identified as African American/Non-Hispanic Black or non-Hispanic White, and presented with unilateral and/or bilateral symptomatic knee OA based upon the American College of Rheumatology criteria. 22 The samples were recruited from the communities surrounding UF and UAB between January 2010 and October 2013 (UPLOAD1, n = 270), and August 2015 and May 2017 (UPLOAD2; n = 164), using fliers, radio/print ads, word of mouth referrals, and clinic-based recruitment. All participants provided written informed consent and received compensation for participating.
Exclusion criteria included (1) prosthetic knee replacement or other clinically significant surgery to the arthritic index knee; (2) uncontrolled hypertension (blood pressure > 150/95 mm Hg), heart failure, or history of acute myocardial infarction; (3) peripheral neuropathy; (4) systemic rheumatic disorders (i.e. rheumatoid arthritis, systemic lupus erythematosus, gout, and fibromyalgia); (5) daily opioid use; (6) cognitive impairment; (7) excessive anxiety regarding protocol procedures; (8) hospitalization within the preceding year for psychiatric illness; (9) neurological diseases (i.e. Parkinson’s, multiple sclerosis, stroke with loss of sensory or motor function, or uncontrolled seizures); (10) significantly greater pain in body sites other than the knee; and (11) pregnant or nursing.
General study procedures
Both studies consisted of multiple sessions and included similar measures. The current analysis is specific to measures obtained during the health assessment session (HAS), QST, and MRI sessions. MRI data are limited to UPLOAD2, as it was not collected in UPLOAD1.
UPLOAD1
Participants completed a HAS and QST on different days. The HAS consisted of general health and sociodemographic questionnaires, and a physical examination, which was used to identify the most painful (i.e. index) knee. The QST was scheduled to occur within 4 weeks of the HAS, and consisted of psychological measures followed by QST assessments including thermal and pain sensitivity, heat and punctate temporal summation (TS), and conditioned pain modulation (CPM). The order of thermal and mechanical tests was randomized and counterbalanced, followed by a period of rest, and then CPM. Recorded instructions were played prior to each testing procedure. Full study design and procedures have been previously reported.9,23
UPLOAD2
UPLOAD2 study procedures were similar to UPLOAD1 and have been previously reported in detail.18,24 Participants completed a HAS during which general health and sociodemographic data were collected, and a physical exam was performed, which was used to identify the most painful (i.e. index) knee. A QST session was scheduled to occur within 4 weeks of the HAS, followed by a brain magnetic resonance imaging (MRI) session approximately 1 week later. The QST session included the same assessments, and order of thermal and mechanical testing was randomized and counterbalanced, followed by a period of rest and then CPM testing. Measures of clinical pain and symptoms were assessed either online one day prior to the QST session, with psychological measures completed prior to the MRI session.
Measures
Psychological profiles
Coping
Active and passive coping was assessed using the Coping Strategies Questionnaire–Revised (CSQ-R), a 27-item questionnaire designed to assess coping responses to pain.25,26 The frequency with which a person engages in various coping techniques is self-rated on a 7-point scale, with higher scores indicating greater use of that coping strategy. 27
Pain hypervigilance/somatic sensations
Pain hypervigilance or somatic sensations are defined as ‘the excessive tendency to attend to pain/somatic sensations, or the excessive readiness to select pain-related information over other information from the environment’. 28 UPLOAD1 sample completed the Kohn Reactivity Scale (KRS), a 24-item measure assessing hypervigilance and general reactivity and arousability,29,30 and the Pain Vigilance and Awareness Questionnaire (PVAQ), a 16-item questionnaire assessing attention to pain or hypervigilance, with higher scores reflecting increased pain vigilance.31,32 UPLOAD2 sample completed the Patient Health Questionnaire Somatic Symptom Severity Scale (PHQ-15), which asks participants to self-rate how bothered they currently are in regard to 15 common somatic symptoms, with higher scores indicating greater somatic sensitivity. 33
Depression
The 20-item Center for Epidemiologic Studies Depression Scale (CES-D; UPLOAD1), and the eight-item PROMIS Depression Short Form (PROMIS-D-SF; UPLOAD2) were used to assess depressive symptomatology,34,35 with higher scores indicating more depressive symptomatology on both scales. The PROMIS-D-SF has been shown to have good convergent validity with the legacy measure CES-D in clinical populations.36,37
Affect
The Positive and Negative Affect Scale (PANAS) was used to assess trait affect (‘to what extent you generally feel this way’) and consists of 10 positively valenced (e.g. excited, proud) and 10 negatively valenced (e.g. distressed, scared) items rated on a 5-point scale.38,39 High scores on positive affect (PA) reflect enthusiasm, energy, and alertness; high scores on negative affect (NA) reflect distress and aversive mood states.
Negative emotion
Anger and anxiety are considered negative emotions often associated with poor health outcomes and emotional distress.40–43 UPLOAD1 participants completed the trait subscale of the State-Trait Anger Expression Inventory (STAXI), a 44-item self-assessment of trait anger level. 44 Higher scores indicate more feelings of anger and negative emotion. UPLOAD2 participants completed the PROMIS Anxiety Short Form, consisting of seven items rated on a 5-point scale. Higher scores indicate greater anxiety. 35 While not the same psychological constructs, anger and anxiety have shown to be positively correlated with each other45–47 and can be used as identifiers of emotional distress. 48
Optimism
The Life Orientation Test–Revised (LOT-R) is a measure of dispositional optimism consisting of 10 items rated on a 5-point scale, with higher scores indicating greater optimism. 49
Validation measures
Perceived Stress Scale (PSS)
The PSS 50 is a 10-item instrument which assesses participants’ perceived stress over the past month, using a 5-point scale, with higher scores indicating greater perceived stress. The PSS was used in the current analysis to investigate the internal validity of identified psychological profile clusters.
Multidimensional Scale of Perceived Social Support (MSPSS)
The MSPSS 51 is a brief measure of subjective social support which asks individuals to rate the perceived adequacy of support they receive from family, friends, and significant other, on a 7-point scale ranging from ‘strongly disagree’ (1) to ‘strongly agree’ (7). Higher scores indicate greater perceived social support. 52
Clinical pain and function
Number of pain sites
Participants were asked to self-report body site where they experienced pain on more days than not over the past 3 months, unilaterally and bilaterally, including the arms, neck, shoulders, head, chest, stomach, pelvis, upper back, lower back, legs, feet, and any other body region. The total number of pain sites was calculated as the sum of all areas reported.
Graded Chronic Pain Scale (GCPS)
The GCPS is a seven-item self-report questionnaire assessing characteristic pain intensity and pain-related disability over the previous 6 months. 53 Instructions were given specific to knee pain for the purpose of the UPLOAD1 and UPLOAD2 studies. Respondents are asked to rate their current, average, and worst knee pain on a 0–10 numeric rating scale (NRS). Ratings were averaged and multiplied by 10 to calculate a characteristic pain intensity score (range: 0–100), with higher scores indicating greater symptom severity. Pain-related disability was computed in a similar manner, with participants reporting the degree to which their knee pain interfered with daily activities during the past 6 months, and scores averaged and multiplied by 10 to generate a characteristic disability score, with higher scores indicating greater pain-related disability.
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC is a 24-item measure of lower extremity pain, function, and stiffness experienced in the past 48 hours. 54 Items are rated on a 5-point scale, with higher scores reflecting greater symptom burden. Subscales for pain and physical function were used for analysis.
Quantitative sensory testing (QST)
Multimodal QST was completed following standardized protocols.9,24 With the exception of CPM, procedures were the same across the two studies. All testing was completed by trained research staff.
Heat pain threshold and tolerance
Heat stimuli were delivered to the ipsilateral ventral forearm and the medial joint line of the index knee using a computer controlled Medoc Pathway (Ramat Yishai, Israel), equipped with a 16×16 thermode. The position of the thermode was moved between trials to avoid sensitization or habituation. Heat threshold (‘when sensation first becomes painful’) was assessed prior to heat tolerance (‘when you feel you are no longer able to tolerate the pain’). Each trial began at a baseline temperature of 32°C and increased at a rate of 0.5°C/second until the participant ended the trial by pressing a button. Temperature (°C) for heat pain threshold (HPTh) and heat pain tolerance (HPTol) was recorded for all procedures. Each test was repeated three times and the mean temperature was used for analysis.
Pressure pain threshold
Pressure pain threshold (PPT) was assessed on the medial and lateral joint lines of the index knee, and ipsilateral quadriceps and trapezius, using a digital handheld pressure algometer (AlgoMed, Medoc). The order of testing was randomized and counterbalanced. Pressure was applied at a constant rate of 30 kPa/second until the participant indicated, by pressing a button, that the pressure had ‘first become painful’. To maintain safety, the maximum pressure for the knee was 600 kPa, and 1000 kPa for the quadriceps and trapezius. If participants did not report pain upon reaching the maximum pressure level, the trial ended and the maximum score was assigned. The procedure was repeated three times for each testing site, and averaged for analysis. Due to the high correlation between PPT at the medial and lateral knee sites, an average score was computed across both sites for knee PPT.
Mechanical temporal summation
As a second measure of temporal summation, sensitivity to punctate stimuli was assessed on the patella of the index knee and back of the ipsilateral hand using a calibrated nylon monofilament delivering a target force of 300 gm. Order of testing sites was randomized. Participants were asked to provide pain ratings from 0 ( ‘no pain sensation’) to 100 (‘most intense pain sensation imaginable’) in response to a single contact, followed by a series of 10 contacts delivered at a rate of 1 contact/second. The procedure was repeated two times, and the ratings were averaged for analysis. Temporal summation was computed as the difference between pain after a single contact and pain rating following the series of 10 contacts.
Conditioned pain modulation
Conditioned pain modulation (CPM) was determined by the ability of a conditioning stimuli (i.e. cold water immersion), to diminish the pain experienced during a test stimulus (i.e. UPLOAD1-heat thermal pain; UPLOAD2-pressure pain).
In UPLOAD1, participants first underwent a series of 5 heat pain trials delivered to the left ventral forearm with a CHEPS thermode (Medoc). Then, participants immersed their right hand into a cold water bath for 1 minute. Following cold water immersion, participants underwent a second series of heat pain trials. Temperatures for heat and cold stimuli were tailored to evoke moderate pain (rating of 40–60/100 on a numeric rating scale), based on earlier testing. The means for the 5 pre-immersion and 5 post-immersion pain ratings were computed. CPM was calculated as the change in heat pain response from baseline to post-conditioning testing, with lower scores indicating greater pain inhibition.
In UPLOAD2, the test stimulus was PPT applied to the left trapezius, using an algometer. Participants indicated when they first felt pain from the pressure by pressing a button. The amount of force was recorded. Then, participants immersed their right hand into a cold water bath (12°C) for up to 1 minute. PPT was assessed again immediately after participants removed their hand from the cold water. If a participant was unable to leave their hand in the cold water bath for 1 minute, PPT was assessed immediately upon removal. CPM was calculated as the change in PPT from baseline to post-conditioning, such that a lower CPM reflected greater pain inhibition, as in the UPLOAD1 study.
Covariates
Baseline variables including age (in years), sex, ethnicity/race, education, study site (i.e. UF/UAB), number of self-reported pain sites, and body mass index (BMI) were used for descriptive purposes and assessed for their associations with identified profiles, as were used as covariates in adjusted models to control for potential confounding when relating psychological profiles to clinical outcomes. MRI analyses were adjusted for ethnicity/race, age, and study site.
Brain imaging
MRI data were acquired for eligible UPLOAD2 participants at the University of Florida using a 3.0 Tesla Philips Achieva whole body scanner with a 32-channel head coil and at the University of Alabama, Birmingham, using an eight-channel head coil. The head was secured via cushions positioned inside the head coil to minimize movement. T1-weighted (T1w) images were acquired using a high-resolution three-dimensional (3D) MP-RAGE sequence (repetition time = 7.0 ms, echo time = 3.2 ms/8°, 1 mm 3 isotropic voxels) and used for analysis. Every acquired T1w image was preprocessed using FreeSurfer 7.1.0 (http://surfer.nmr.mgh.harvard.edu/), using the ‘recon-all’ function with default parameters for the general cortical reconstruction process. All calculated areas and their respective parameters were then matched to Destrieux atlas 55 (Freesurfer’s aparc.2009s) for visualization and further analysis.
Statistical analysis
Data were analyzed using SPSS v.27 (IBM) and R (R v3.6). Data were checked for normality, outliers, missingness, and multicollinearity. Summary statistics are reported as means and standard deviations (SDs) for continuous data, and frequency statistics for categorical data. Baseline differences between study samples were analyzed using one-way analysis of variance (ANOVA) for discrete continuous variables and chi-square for categorical variables. All testing was two-sided at a 0.05 significance level.
Hierarchical cluster analysis (i.e. unsupervised machine learning), employing Ward’s clustering method with squared Euclidean distances as the similarity measure, was first applied to the UPLOAD1 data set (i.e. training sample), to identify psychological profiles. 9 Visual inspection of the dendrogram and agglomeration coefficients were used to identify the optimal number of clusters. 56 Linear discriminative analysis (i.e. supervised machine learning) was applied to UPLOAD1 cluster centers (training data) to predict group classification in UPLOAD2 data. To be specific, the squared Euclidian distance between each subject in UPLOAD2 and each of the UPLOAD1 cluster centers was calculated, with group membership based on the shortest distance with the UPLOAD1 cluster center. Analyses of variance (ANOVAs) were used to examine associations between profiles and continuous phenotypes to establish validity of the identified profiles. The empirically derived psychological profile subgroups were compared across measures of clinical pain, pain-related disability, and experimental pain using multivariate analysis of covariance (MANCOVA), controlling for age, sex, ethnicity/race, education, study site, number of pain sites, and BMI. Multiple testing correction was performed by the Bonferroni method. Missing data (all < 5%) were listwise deleted from the analyses.
Brain imaging analysis
Contrasts were computed between psychological profile clusters classified in UPLOAD2 and the vertex-wise measures for cortical volumes and cortical thickness. The analysis was carried by employing Freesurfer’s ‘mri_glmfit’ function assessing cluster level significance threshold of p < 0.01 and controlling for age, ethnicity/race, and study site. We accounted for false positive rates by applying Freesurfer’s implementation of Cluster-wise Correction for Multiple Comparisons 57 and Bonferroni correction across brain hemispheres at p < 0.05, two-tailed. For the correct anatomic labeling, the significant clusters were then matched to Destrieux’s anatomical atlas of sulcus and gyri (Freesurfer’s aparc2009s). 55
Results
Participant characteristics
The UPLOAD1 (n = 270) and UPLOAD2 (n = 164) study samples were predominantly female (62.6% and 64%, respectively), with approximately equal representation across ethnicity/race groups (Table 1). The study samples did not differ significantly on age, sex, education, study site, number of self-reported anatomical pain sites, or BMI (Table 1).
Overall sociodemographic and clinical characteristics of study participants.

AA/NHB, African American/non-Hispanic Black; BMI, body mass index; C/NHW, Caucasian/non-Hispanic White; GCPS, Graded Chronic Pain Scale; MSPSS, Multidimensional Scale of Perceived Social Support; PSS, Perceived Stress Scale; SD, standard deviation; UAB, University of Alabama, Birmingham; UF, University of Florida; UPLOAD1, Understanding Pain and Limitations in Osteoarthritic Disease-1; UPLOAD2, Understanding Pain and Limitations in Osteoarthritic Disease-2; WOMAC, Ontario and McMaster Universities Osteoarthritis Index.
Bolded values represent statistically significant differences between study samples.
Determination of psychological profiles
Four distinct psychological profiles emerged in the UPLOAD1 training data set and replicated in the UPLOAD2 data. Profile 1 had the lowest passive coping, somatic reactivity, and pain hypervigilance scores (‘low somatic sensitivity/pain hypervigilance’). Profile 2 was characterized by the highest scores on both active and passive coping (‘high coping’). Profile 3 demonstrated the highest scores for depression, negative affect, and anxiety, and the lowest scores for positive affect and optimism (‘high negative emotions/low positive emotions’). Profile 4 had the lowest scores for depression and negative affect, and the highest scores for positive affect and optimism (‘low negative emotions/high positive emotions’) (Figures 1 and 2).
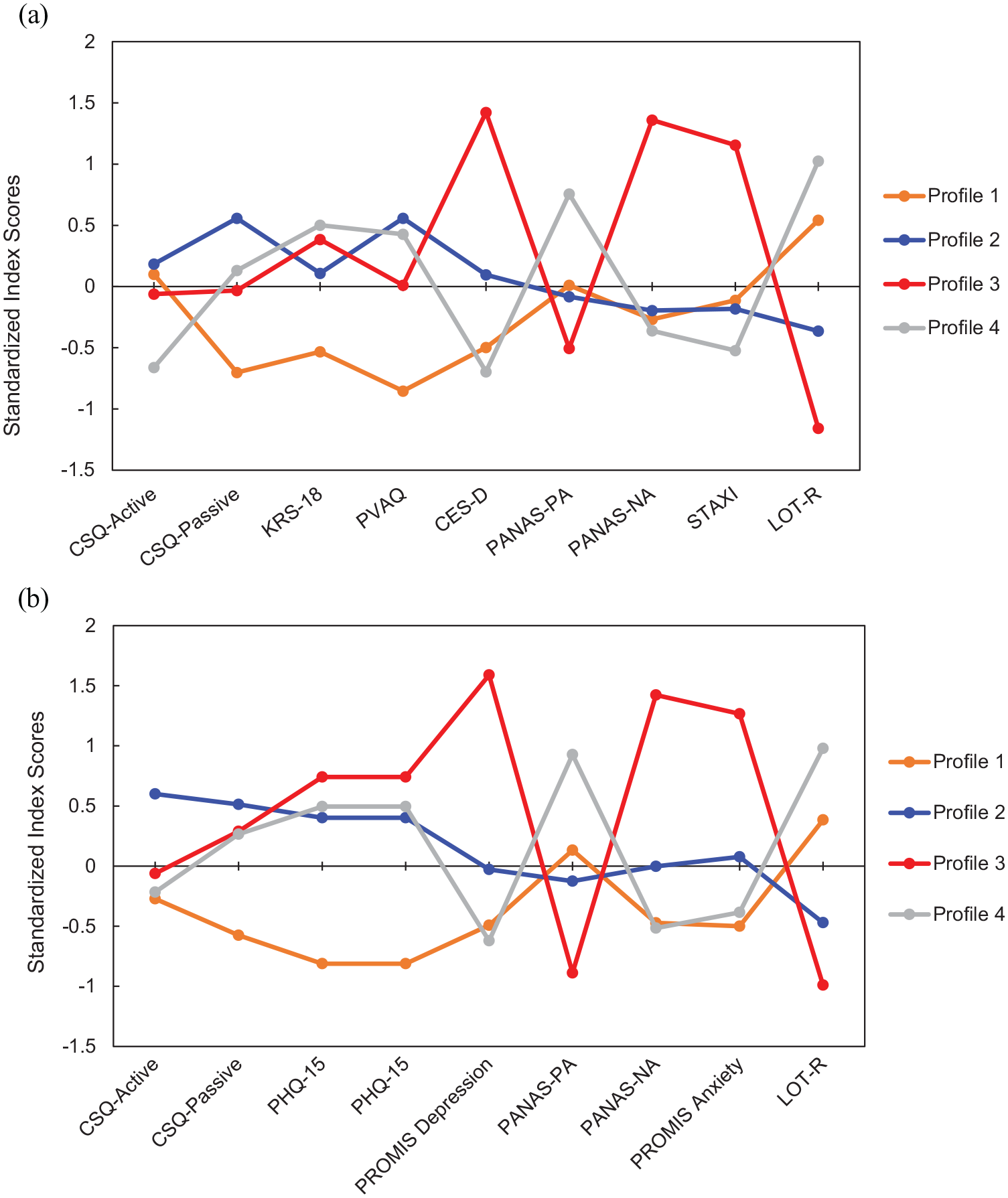
Profiles identified using unsupervised and supervised machine learning. (a) UPLOAD1; (b) UPLOAD2.
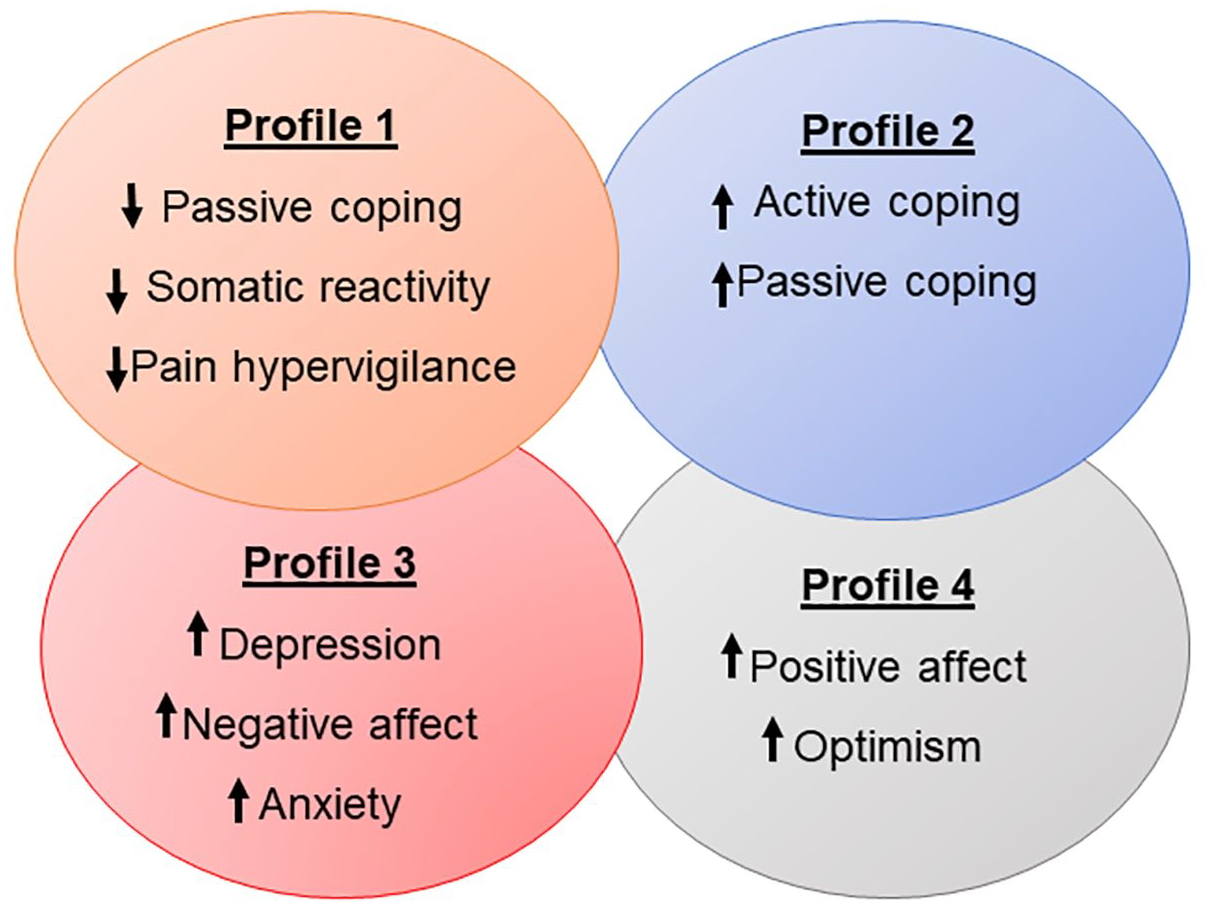
Summary of psychological profile characteristics.
One-way ANOVA demonstrated significant group differences among profiles continuous psychological variables (ps < 0.001) (Table 2), demographics, and other sample characteristics (ps = 0.032–0.001) (Table 3), indicating cluster validity.
Mean ± SD for psychological profile variables.

CES-D, Center for Epidemiologic Studies Depression Scale; CSQ-R, Coping Strategies Questionnaire–Revised; KRS, Kohn Reactivity Scale; LOT-R, Life Orientation Test–Revised; PANAS, Positive and Negative Affect Scale; PHQ-15, Patient Health Questionnaire Somatic Symptom Severity; PROMIS-A, PROMIS Anxiety Short Form; PROMIS-D, PROMIS Depression c; PVAQ, Pain Vigilance and Awareness Questionnaire; SD, standard deviation; STAXI, State-Trait Anger Expression Inventory; UPLOAD1, Understanding Pain and Limitations in Osteoarthritic Disease-1; UPLOAD2, Understanding Pain and Limitations in Osteoarthritic Disease-2.
Sample characteristics by psychological profile.

AA/NHB, African American/non-Hispanic Black; BMI, body mass index; C/NHW, Caucasian/non-Hispanic White; MSPSS, Multidimensional Scale of Perceived Social Support; PSS, Perceived Stress Scale; SD, standard deviation; UAB, University of Alabama, Birmingham; UF, University of Florida; UPLOAD1, Understanding Pain and Limitations in Osteoarthritic Disease-1; UPLOAD2, Understanding Pain and Limitations in Osteoarthritic Disease-2.
Bolded values were significant at α = 0.05.
Associations between psychological profiles and clinical pain
Multivariate analyses of covariance (MANCOVAs), controlling for age, sex, ethnicity/race, education, study site, number of pain sites, and BMI demonstrated statically significant differences on clinical pain measures between psychological profile groups in both samples, Table 4. Bonferroni corrected post hoc comparisons showed individuals with low somatic sensitivity/pain hypervigilance (Profile 1) had lower WOMAC pain (ps = 0.019–0.001) and WOMAC physical function (ps = 0.025–0.002), scores compared to those with high negative emotions/low positive emotions (Profile 3). GCPS characteristic pain intensity and GCPS pain-related disability differed significantly across psychological profile groups in UPLOAD1, with Profile 1 reporting less pain intensity and pain interference compared with Profiles 2 and 3 (ps = 0.019–0.001). These differences were not observed in UPLOAD2 data.
Raw mean ± SD values for clinical pain by psychological profile.
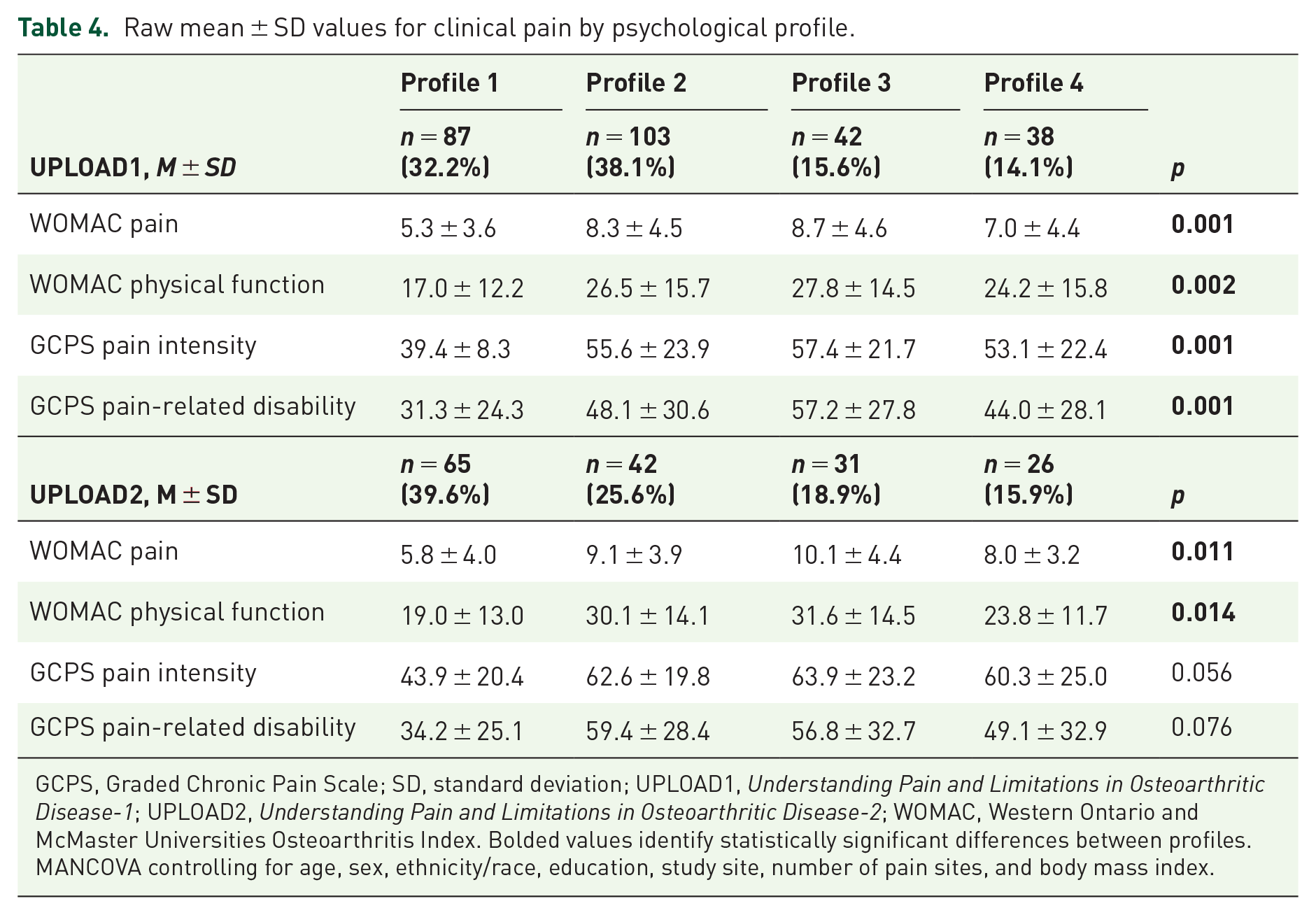
GCPS, Graded Chronic Pain Scale; SD, standard deviation; UPLOAD1, Understanding Pain and Limitations in Osteoarthritic Disease-1; UPLOAD2, Understanding Pain and Limitations in Osteoarthritic Disease-2; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. Bolded values identify statistically significant differences between profiles.
MANCOVA controlling for age, sex, ethnicity/race, education, study site, number of pain sites, and body mass index.
Associations between psychological profiles and experimental pain
A MANCOVA controlling for age, sex, ethnicity/race, education, study site, number of pain sites, and BMI demonstrated statistically significant differences in heat pain tolerance (HPTol) at the knee in UPLOAD1 profile groups (p = 0.034) (Table 5). Individuals in the ‘low somatic sensitivity/pain hypervigilance’ profile (Profile 1) demonstrated higher HPTol compared with the ‘high coping’ profile (Profile 2). There were no statistically significant differences among psychological profiles groups on heat pain sensitivity measures in UPLOAD2 sample.
Raw mean ± SD values for experimental pain by psychological profile.

HPTh, heat pain threshold; HPTol, heat pain tolerance; PPT, pressure pain threshold; SD, standard deviation; TS, temporal summation; UPLOAD1, Understanding Pain and Limitations in Osteoarthritic Disease-1; UPLOAD2, Understanding Pain and Limitations in Osteoarthritic Disease-2.
Bolded values identify statistically significant differences between profiles.
MANCOVA controlling for age, sex, ethnicity/race, education, study site, number of pain sites, and body mass index.
In UPLOAD1, pressure pain threshold (PPT) at the knee, trapezius, and quadriceps differed significantly between psychological profiles (ps = 0.014–0.001; MANCOVA) (Table 5). Individuals in Profile 1 had significantly greater PPTs than those in Profile 2 (Bonferroni corrected ps = 0.014–0.001). The differences were not observed in UPLOAD2 profiles.
Mechanical temporal summation at the hand and knee were significantly associated with psychological profiles in UPLOAD1 participants (ps = 0.005–0.001, MANCOVA) (Table 5). Post hoc Bonferroni corrected multiple comparisons indicated ‘low somatic sensitivity/pain hypervigilance’ profile (Profile 1) reported less temporal summation at the knee and hand compared with the ‘high negative emotions/low positive emotions’ profile (Profile 3) (p = 0.004). Mechanical temporal summation did not differ significantly in UPLOAD2 profiles.
The results from a one-way analysis of covariance (ANCOVA), adjusting for age, sex, ethnicity/race, education, study site, number of pain sites, and BMI showed that psychological profiles did not differ significantly in either sample on CPM (Table 6).
Conditioned pain modulation by psychological profile.

NRS, numerical rating scale; PPT, pressure pain threshold; SD, standard deviation; UPLOAD1, Understanding Pain and Limitations in Osteoarthritic Disease-1; UPLOAD2, Understanding Pain and Limitations in Osteoarthritic Disease-2.
MANCOVA controlling for age, sex, ethnicity/race, education, study site, number of pain sites, and body mass index. Lower values indicate greater pain inhibition.
Differences in brain volume among psychological profiles
Findings from UPLOAD2 brain magnetic resonance imaging (MRI) showed significant differences in brain volume between psychological profiles. Individuals classified as low somatic sensitivity (i.e. Profile 1) had greater precuneus gray matter volume compared with individuals classified as high negative emotions/low positive emotions (i.e. Profile 3), p = 0.005, Figure 3(a). In addition, those with high negative emotions/low positive emotions (i.e. Profile 3) had significantly less volume in the middle occipital gyrus compared with those classified as low negative emotions/high positive emotions (i.e. Profile 4), p = 0.040, Figure 3(b).

Associations between psychological profiles and brain volume in UPLOAD2 participants. (a) Cluster 1 versus Cluster 3 volumetric differences in precuneus and (b) Cluster 3 versus Cluster 4 volumetric differences in middle occipital gyrus.
Discussion
We sought to confirm the presence of previously identified psychological profiles, 9 in a larger sample of adults with knee OA pain, and determine the replicability of identified psychological profiles in a separate cohort, and their associations with psychological variables, clinical pain, somatosensory function, and brain structure. Several noteworthy findings emerged. First, we confirmed the presence of four distinct profiles based on the psychological data from UPLOAD1, which were replicated in UPLOAD2. Second, these psychological profiles were significantly associated with clinical pain and pain-related disability outcomes in a similar pattern across both study cohorts. Taken together, these findings support the hypothesis that distinct psychological profiles exist among individuals with knee OA-related pain, which need to be considered in pain assessment and treatment in knee OA.
Psychological profiles differed across sociodemographic variables in both the UPLOAD1 and UPLOAD2 cohorts. Individuals demonstrating high negative emotions/low positive emotions (i.e. Profile 3) were, on average, younger, compared with other psychological profiles. In addition, individuals who were classified in Profile 2 (i.e. high coping), and Profile 3 (i.e. high negative emotions/low positive emotions), reported significantly lower educational attainment. These findings are similar to our previous work, 9 indicating those with the least favorable psychological profiles and knee OA pain are on average younger with less educational achievement. Ethnicity/race differed significantly in UPLOAD1 sample, with a greater proportion of African Americans represented in the high coping (i.e. Profile 2) subgroup. This relationship was similar in UPLOAD2 but failed to reach statistical significance. Given these differences and prior research demonstrating the effects of age, education, and ethnicity/race on pain, these variables were controlled for in analyses of pain outcomes. Therefore, the differences between psychological profiles on pain and pain-related disability outcomes are attributable to factors beyond sociodemographic characteristics.
Overall, individuals classified with less favorable psychological profiles reported greater clinical pain and pain-related disability. These findings are consistent with previous studies showing psychological resilience and optimism may be protective in chronic pain against poor clinical outcomes.11,58 However, few studies have investigated the role of multiple positive and negative psychological characteristics on pain outcomes in knee OA. 17 A greater consideration of the combined influence of both positive and negative psychological factors is needed to improve treatment outcomes. Interestingly, in the UPLOAD2 sample, individuals with a more favorable psychological profile (i.e. Profile 4: low negative emotions/high positive emotions) reported significantly more anatomical pain sites compared with the other profiles, which is notable given that their clinical pain and pain-related disability scores were among the lowest. This is in contrast to previous research that has shown a significant relationship between number of pain sites and increased pain and physical dysfunction. 59 The current finding may represent the protective nature of multiple high positive psychological characteristics combined with multiple low negative psychological characteristics in this subgroup.
We examined associations between psychological profiles and responses to a standardized multimodal QST battery. Individuals with low somatic sensitivity/pain hypervigilance (i.e. Profile 1) demonstrated the least pain sensitivity to heat and pressure in both samples. This is consistent with our previous findings, 9 and other studies demonstrating associations between somatic sensitivity and pain hypervigilance, and decreased pain tolerance.60,61 While not all of these associations achieved statistical significance, they are worth noting given their consistency across the samples.
Mechanical temporal summation at the hand and knee was significantly greater in those with high negative emotions/low positive emotions (i.e. Profile 3), but did not replicate in the UPLOAD2 sample. Surprisingly, individuals with high negative emotions/low positive emotions (i.e. Profile 3) demonstrated the greatest CPM responses in both samples; however, this finding did not reach statistical significance in either cohort. It is worth noting that most participants in UPLOAD1 did not demonstrate descending pain inhibition, and the majority of individuals in UPLOAD2 showed very modest pain inhibition. This is consistent with previous studies reporting decreased CPM among adults with OA.15,62 Our findings further suggest that those with more favorable psychological profiles may have less pain sensitivity based on pre-conditioning pain ratings and pressure pain thresholds in the CPM paradigms.
This study is among the first to investigate associations between multifactorial psychological profiles and brain structure in persons with knee OA pain. Findings indicate significant differences across psychological profiles in brain structure, including significant volumetric differences between individuals with low somatic sensitivity (i.e. Profile 1), and those with high negative emotions/low positive emotions (i.e. Profile 3) in precuneus gray matter, further supporting its involvement in the affective responses to pain in persons with knee OA. 63 Also, significant differences between individuals with high positive emotions/low negative emotions (i.e. Profile 4), and those with high negative emotions/low positive emotions (i.e. Profile 3) in the middle occipital gyrus may reflect differences in multisensory perception and emotional processing of pain. 64
We have now confirmed the presence of distinct profiles in persons with knee OA pain based on multiple positive and negative psychological characteristics and have demonstrated their replicability and associations with clinical symptoms and somatosensory function. Future studies that include assessment of these profiles in relation to treatment response to both pharmacological and non-pharmacological interventions are warranted, as well as consideration for the types and frequency of intensive treatments (e.g. injections and surgical procedures) previously used. Furthermore, investigations on the associations between these psychological profiles and cases of intractable knee OA pain, considering other potential socio-economic factors (e.g. health insurance status, type) will provide valuable information regarding potential treatment responsiveness. It is possible that those demonstrating low psychological distress and experimental pain sensitivity would benefit from more peripherally targeted interventions (e.g. physical therapy), while those demonstrating greater centrally mediated pain characteristics would benefit more from a comprehensive treatment approach that targets both central and peripheral pain mechanisms (e.g. cognitive behavioral therapy). The next steps are to determine if these psychological and somatosensory profiles can reliably predict treatment response, and their utility for tailored interventions for improved clinical outcomes.
Limitations
Several limitations must be considered. First, it is not possible to determine causal relationships from the current study given the cross-sectional nature of the data. It is possible that the relationships between pain, somatosensory function, and psychological characteristics are bidirectional, with psychological factors influencing pain and pain influencing psychological function. Future studies assessing these characteristics longitudinally will help to address these questions. It is also possible that we have excluded other potentially relevant variables that would improve our understanding of the biopsychosocial nature of knee OA pain, such as other biological (e.g. myofascial, immune/inflammatory markers), or psychosocial (e.g. social support, efficacy, kinesiophobia) factors. The use of artificial intelligence (e.g. machine learning) to investigate these potential relationships in large prospective data sets holds tremendous promise for developing tailored interventions for optimal clinical outcomes. Also, given the exclusion criteria, we did not capture data on more psychologically distressed or cognitively impaired individuals, which limits the generalizability of our findings. Exploring these relationships in more clinical settings is needed to address this question.
Conclusions
In conclusion, our study provides further support for the existence of multifactorial psychological profiles among adults with knee OA pain that may influence pain and physical function. Treatment outcomes in knee OA may be improved by targeting these profiles. Future research is warranted comparing treatment outcomes across these profiles.
Footnotes
Acknowledgements
We are grateful to our participants and the UPLOAD1 and UPLOAD2 study teams at the University of Florida and the University of Alabama, Birmingham.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Alisa J. Johnson, Chavier Laffitte Nodarse, Julio A. Peraza, Pedro A. Valdes-Hernandez, Soamy Montesino-Goicolea, Zhiguang Huo, Roger B. Fillingim and Yenisel Cruz-Almeida. All authors contributed to revisions and read and approved the final manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH/NIA Grants R01AG059809, R01AG067757 (YCA); R37AG033906 (RBF), and T32AG049673 (SMG). A portion of this work was performed in the McKnight Brain Institute at the National High Magnetic Field Laboratory’s Advanced Magnetic Resonance Imaging and Spectroscopy (AMRIS) Facility, which is supported by National Science Foundation Cooperative Agreement No. DMR-1157490 and DMR-1644779 and the State of Florida. This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other funding agencies.