
Abstract
Background:
The aim of this study was to examine the impact of underweight, overweight and obesity on clinical outcomes and treatment responses to biologics in Chinese patients with ankylosing spondylitis (AS).
Methods:
Body mass index (BMI) was available in 1074 patients from the Smart-phone SpondyloArthritis Management System. Patients were categorized into four groups based on BMI: underweight, normal weight, overweight and obesity. Multivariable median regression analyses examined the effect of underweight and obesity on clinical outcomes and treatment response to biologics.
Results:
Among 1074 patients with AS, normal weight accounted for 49.1%, while underweight, overweight, and obesity for 8.1%, 30.1%, and 12.0%, respectively. Compared to patients with normal weight, patients with underweight, overweight and obesity had an increased disease activity, while patients with underweight and obesity had a significantly poor Bath Ankylosing Spondylitis Functional Index and Assessment of Spondyloarthritis International Society Health Index scores. For tumor necrosis factor (TNF)-α inhibitor users, BMI was found to be negatively correlated with changes in disease activity in the multivariate regression model (all p < 0.05). Besides, the patients using TNF-α inhibitor in the overweight or obesity categories were much less likely to achieve a significant reduction on disease activity during follow-up period in the multivariate regression model (all p < 0.05), taking these with normal-weight patients as a reference.
Conclusions:
Both underweight and obesity except for overweight were associated independently with worse disease activity, physical function and health status. Overweight and obesity might impact on treatment responses to biologics in patients with AS. This argues that weight management, to maintain it at a normal level, should be one of the disease management strategies in patients with AS.
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory condition with broad clinical spectrum and unknown etiology. Its primary characteristics are the apparent inflammation on the spinal and sacroiliac joints and neighboring structures, which will cause progressive bone erosion and bone fusion on the vertebrae and sacroiliac joint. 1 The pathogenesis of AS is not completely understood due to complex interaction between genetic risk factors and environmental triggers that leads to immune activation. 2 The studies have reported that AS had a multifactorial etiology with genetic risk factors [predominantly human leukocyte antigen (HLA)-B27], microbiota and biomechanical stress models shaping the disease-related features.3,4
Poor body mass index (BMI) level may also be one of factors considered in the pathogenesis of AS. Studies have shown that obesity, as a low-grade inflammatory status, could increase proinflammatory cytokines, such as tumor necrosis factor (TNF)-α, amyloid A, and interleukin (IL)-6, and overexpression of specific adipocyte-derived adipokines released by the visceral fat, 5 whose association with the development of rheumatic diseases was only partially elucidated.6–8 The association of obesity categorized by BMI and clinical outcomes of AS remains controversial, while the prevalence of AS in underweight individuals and the effect of underweight on patients with AS is always ignored. A small cross-sectional study shown that 68% of patients with AS patients were overweight or obese, and these patients had higher disease activity, more limited function, and less treatment benefit. 9 However, this study was conducted in Ireland with a White population. Thus, the results might not be suitable for the Chinese population, and the sample size of 46 patients was relatively small. Another cross-sectional study including 428 patients with axial spondyloarthritis suggested that BMI had no significant effect on patient-reported outcomes, and the study was conducted in European countries. 10
In addition, not only may obesity play a role in the pathophysiology of AS, but also may affect the response to biologics therapy. The studies demonstrated that obesity was associated with decreased response rates to treatments, 11 and weight reduction by gastric bypass might be an effective way to minimize risk and improve prognosis of psoriasis and psoriatic arthritis. 12 Besides, some studies in European and American countries suggested that overweight and obesity were associated with a lower success rate in achieving response status in patients with axial spondyloarthritis using anti-TNF agents.13–15 However, few studies have explored the relationship between obesity and its impact on clinical outcomes and therapeutic responses to biologics in Chinese patients with AS.
Therefore, based on Chinese AS cohort, our study aimed to investigate and assess the effects of underweight and obesity on disease activity and functional ability at baseline, and therapeutic responses to biologics in Chinese patients with AS.
Methods
Patients and inclusion criteria
The data were from the Chinese Ankylosing Spondylitis Imaging Cohort (CASPIC), which was a nationwide, prospective cohort study launched using a mobile health (mHealth) tool: Smart-phone SpondyloArthritis Management System (SpAMS). 16 SpAMS is linked to WeChat, the world’s largest multipurpose social media mobile application software (developed by Tencent, first released in 2011). WeChat was used by physicians to maintain communication with patients, record long-term follow-up information, and receive patients’ feedback. We enrolled patients without imposing limits on age and disease duration, so as to observe the whole picture and to comprehensively evaluate the characteristics and outcomes of patients with AS in China. The patients were from all over the country, and recruited consecutively from outpatient rheumatology clinics and diagnosed by rheumatologist according to the 1984 modified New York criteria in the Chinese People’s Liberation Army (PLA) General Hospital in Beijing. The inclusion criteria for patients in this study were as follows: (1) having a smart-phone with network access, (2) fulfilling the 1984 modified New York criteria, 17 (3) having complete clinical data, (4) having at least one follow-up visit after the first visit. Exclusion criteria for patient were as follows: (1) refusing to complete the survey, (2) having invalid/missing data on registration and questionnaires.
Drug exposure
TNF-α inhibitor users were defined as the patients who were treated with TNF-α inhibitors at any point during the first and follow-up visits; the baseline was defined as the time of enrollment for patients who were using TNF-α inhibitors at the time of enrollment or as the time at which patients started using TNF-α inhibitors after enrollment. TNF-α inhibitor users received subcutaneous administration of TNF-α inhibitors, including biosimilar etanercept (Yisaipu®; Sunshine Guojian Pharmaceutical Co., Ltd, Shanghai, China) or adalimumab (AbbVie, Ludwigshafen, Germany).18–20
Subsequent visits were scheduled by physician according to the patients’ conditions. TNF-α inhibitor users had at least one 3-month follow-up after the baseline for analyzing the effect of BMI on treatment response to TNF-α inhibitors.
Definitions of underweight, normal weight, overweight and obesity
World Health Organization (WHO) recommends the use of BMI cut-off points to define underweight, normal weight, overweight and obesity in adults. 21 There are two most commonly used BMI classifications for adults in China, which are the WHO standard (underweight: BMI < 18.5 kg/m2; normal weight: 18.5 ⩽ BMI < 25 kg/m2; overweight: 25 ⩽ BMI < 30 kg/m2; obesity: BMI ⩾ 30 kg/m2) and the developed Chinese standard (underweight: BMI < 18.5 kg/m2; normal weight: 18.5 ⩽ BMI < 24 kg/m2; overweight: 24 ⩽ BMI < 28 kg/m2; obesity: BMI ⩾ 28 kg/m2).22,23 Since there is growing evidence that people at lower BMI in Asian Pacific populations have an elevated risk for obesity-related diseases or conditions than White people,22,24,25 the lower BMI cut-off points are recommended in China.
Data collection and outcome assessments
Unified online protocol-directed methods were made. Characteristics of online registration included age, sex, height, weight, smoking status, comorbidities, past medical history, date at onset of back pain, date of diagnosis, presence of AS features, and family history. Follow-up assessments for AS were categorized as patient-reported assessment or physician-reported assessment.
Standardized questionnaires were used for patient-reported assessments, including Ankylosing Spondylitis Disease Activity Score (ASDAS), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), and Assessment of Spondyloarthritis International Society Health Index (ASAS HI). Standardized questionnaires were used for physician-reported assessments, including Bath Ankylosing Spondylitis Metrology Index (BASMI), inflammatory markers [erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)], HLA-B27 status, the location of peripheral arthritis (28 joints) and enthesitis according to the Maastricht Ankylosing Spondylitis Enthesitis Score, presence of uveitis, psoriasis, and a colonoscopy and pathology-confirmed diagnosis of inflammatory bowel disease, and ongoing treatment for AS. The primary clinical outcome was disease activity at baseline and changes in disease activity reflected by ASDAS during follow-up. The follow-up interval was set at 3 months, and the follow-up window was defined as within 1 month of each follow-up point.
Handling of missing values
Missing values, such as not evaluable segments due to missing clinical information, were not imputed. Results were always presented based on the available data for each parameter.
Statistical analysis
Continuous variables with positive distribution were expressed as mean ± SD, and categorical variables were expressed as number of patients (%). One-way analysis of variance or Kruskal–Wallis test was used to analyze differences among BMI groups for continuous variables, and Pearson’s Ci-squared or Fisher’s exact test were used to analyze differences among BMI groups for categorical variables.
BMI categories were introduced separately as independent variables in the median regression models for each of these dependent variables, such as clinical outcomes and treatment response to biologics, and normal weight category was used as reference. In order to correct the possible confounding effects, then a multivariable median regression model was developed, and these variables considered significant in univariable regression model were adjusted. Variables with p < 0.05 in the final multivariate regression models were considered statistically significant. In order to avoid multicollinearity, the variables with variance inflation factor <5 are included.
All the statistical analyses were conducted using Stata MP 15.1 for Mac (StataCorp, College Station, TX, USA). Two-tailed p < 0.05 was interpreted as significant.
Ethical considerations
The study protocol was reviewed and approved by the Ethics Committee of the Chinese PLA General Hospital (S2016-049-02). Informed consent for participation in the study was obtained from all patients before study entry.
Results
Patients’ characteristics at baseline
A total of 1614 patients with AS were recruited through the SpAMS from April 2016 to February 2019. Among these, 1074 patients had available BMI at baseline (Figure 1). Descriptive statistics for the stratified BMI categories of available patients were presented in Table 1.

STROBE flowchart.
Patient characteristics based on BMI category.

p < 0.05 compared with patients with normal weight.
AS, ankylosing spondylitis; ASAS HI, the Assessment of Spondyloarthritis International Society Health Index; ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI, Bath Ankylosing Spondylitis Metrology Index; BMI, body mass index; CRP, C-reactive protein; csDMARD, conventional synthetic disease modifying antirheumatic drug; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; IBD, inflammatory bowel disease; NSAID, nonsteroidal anti-inflammatory drug.
Among 1074 patients with AS, according to the BMI definition, normal weight accounted for 49.1%, while underweight, overweight, and obesity for 8.1%, 30.1%, and 12.0%, respectively. Compared to the normal-weight patients, the patients with overweight and obesity were older (p < 0.01), while the underweight patients indicated a younger age (p < 0.01). At inclusion, 32.3% patients were daily current smokers, and there were no significant differences among the four BMI categories. There was also no statistical difference in family history (inflammatory bowel disease, uveitis, psoriasis, and AS) among the four BMI categories. Similarly, enthesitis and peripheral joint presentation did not differ statistically among the four BMI categories.
In addition, the patients with underweight, overweight and obesity had significantly elevated disease activity as measured by higher ASDAS scores (p = 0.014, p = 0.019 and p < 0.001, respectively), and reduced functional capacity by higher BASFI scores (p = 0.017, p = 0.005, and p < 0.001, respectively), while comparing with normal-weight patients. Besides, the patients with underweight and obesity showed a worse health index (ASAS HI, p < 0.001 and p < 0.001), while about spinal mobility (BASMI), only patients with obesity showed a significantly worse score (p < 0.001). Patients with underweight, overweight and obesity had a higher ESR and CRP level than normal-weight patients (all p < 0.001). Above all, the trend appeared to be U-shaped, as both very low and high BMI was associated with unfavorable functional capacity and disease activity (Supplemental Figures 1–5).
The baseline treatment with various drugs are presented in Table 1. There were 98.1%, 49.3%, and 31.1% of patients receiving nonsteroidal anti-inflammatory drugs (NSAIDs), conventional synthetic disease modifying antirheumatic drugs (csDMARDs), and biologics, respectively. There was no significant difference on the use of these drugs among the BMI categories.
Impact of underweight and obesity on clinical outcomes at baseline
Univariate analysis
The results of univariate median regression model suggested that obesity as defined by the BMI had a significant association with higher disease activity as reflected by ASDAS (β = 0.45, p < 0.001) and BASDAI (β = 0.60, p = 0.003), decreased functional capacity (BASFI: β = 0.70, p < 0.001), spinal mobility (BASMI: β = 1.00, p < 0.001) and worse health index (ASAS HI: β = 2.00, p < 0.001), and normal weight category was used as reference. Besides, higher ASDAS (β = 0.39, p = 0.003), BASFI (β = 0.50, p = 0.012) and ASAS HI (β = 2.00, p < 0.001) were also associated with underweight defined by the BMI without adjusting for potential confounders, and normal weight category was used as reference (Table 2).
Univariable and multivariable regression analysis of association between BMI categories and clinical outcomes.

Normal weight patients as a reference.
Adjusting for age, sex, smoking, HLA-B27, and treatments with biologics, csDMARDs and NSAIDs.
ASAS HI, Assessment of Spondyloarthritis International Society Health Index; ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI, Bath Ankylosing Spondylitis Metrology Index; csDMARD, conventional synthetic disease modifying antirheumatic drug; CI, confidence interval; HLA, human leukocyte antigen; NSAID, nonsteroidal anti-inflammatory drug.
Multivariate analysis
In the multivariate median regression model, while adjusting for potential confounders including age, sex, smoking, HLA-B27, and treatment with biologics, csDMARDs and NSAIDs, obesity remained associated with higher disease activity (ASDAS: β = 0.36, p = 0.001; BASDAI: β = 0.63, p = 0.001), poorer functional capacity (BASFI: β = 0.59, p = 0.002), worse health index (ASAS HI: β = 1.37, p = 0.009) and spinal mobility (BASMI: β = 0.64, p = 0.039), and normal weight category was used as reference. Additionally, underweight was also proved an independent association with higher ASDAS (β = 0.34, p = 0.008), BASFI (β = 0.56, p = 0.010) and ASAS HI (β = 1.73, p = 0.004) scores, while adjusting for potential confounders including age, sex, smoking, HLA-B27, and treatment with biologics, csDMARDs and NSAIDs, and normal weight category was used as reference (Table 2).
Impact of obesity on treatment response to TNF-α inhibitors
In addition, of the 1074 patients, 334 were treated with biologics (including recombinant human TNF-α receptor II: IgG Fc fusion protein and adalimumab), 225 of whom were treated for at least three months. The changes on disease activity (ΔASDAS and ΔBASDAI) were used as indicators of treatment response to TNF-α inhibitors. While adjusting for potential confounders, such as sex, smoking, age, HLA-B27, treatments with csDMARDs and NSAIDs, and baseline disease activity, BMI was negatively associated with the changes on disease activity in the multivariate median regression model (all p < 0.05). Figure 2 showed the regression analysis results of ΔASDAS and ΔBASDAI for TNF-α inhibitor users during 3-month, 6-month, 9-month, and 12-month follow-up periods (Supplemental Table 1).

Forest of regression analysis of association between BMI and changes of disease activity [(a) ΔASDAS; (b) ΔBASDAI] for TNF-α inhibitor users during 3-, 6-, 9- and 12-month follow-up. Note: adjusting for age, sex, smoking, HLA-B27, treatments with csDMARDs and NSAIDs, and baseline disease activity scores [(a) baseline ASDAS; (b) baseline BASDAI].
In addition, TNF-α inhibitor users were divided into four categories based on BMI, including underweight, normal weight, overweight and obesity. For TNF-α inhibitor users, the number of patients completed follow-up visits were shown in Supplemental Table 2. The results based on Kruskal–Wallis test demonstrated that the patients in the overweight or obesity categories had less reduction on disease activity during 3-, 6-, 9- and 12-month follow-up period, compared with these with normal-weight patients (Figure 3 and Supplemental Table 3). While adjusting for potential confounders, such as sex, smoking, age, and HLA-B27, treatments with csDMARDs and NSAIDs, and baseline disease activity, the patients in the overweight or obesity categories were much less likely to achieve a significant reduction on disease activity during 3-, 6-, 9- and 12-month follow-up period, taking these with normal-weight patients as a reference (Table 3).

Changes of disease activity [(a) ASDAS; (b) BASDAI] for TNF-α inhibitor users during 3-, 6-, 9- and 12-month follow-up according to BMI categories.
Multivariable regression analysis of association between BMI categories and the changes of disease activity for TNF-α inhibitor users during 3-, 6-, 9- and 12-month follow-up.
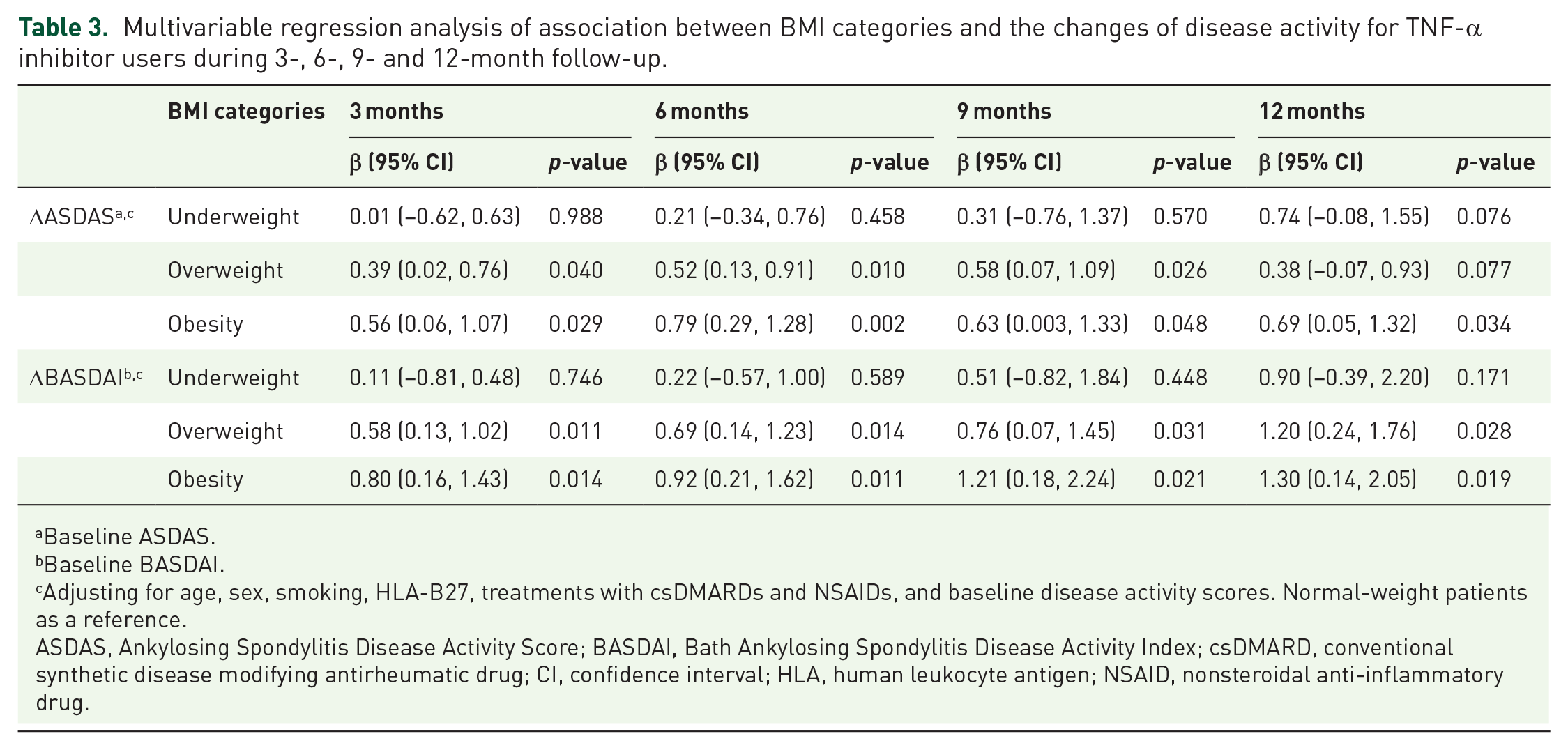
Baseline ASDAS.
Baseline BASDAI.
Adjusting for age, sex, smoking, HLA-B27, treatments with csDMARDs and NSAIDs, and baseline disease activity scores. Normal-weight patients as a reference.
ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; csDMARD, conventional synthetic disease modifying antirheumatic drug; CI, confidence interval; HLA, human leukocyte antigen; NSAID, nonsteroidal anti-inflammatory drug.
Discussion
In this study, we analyzed the impact of underweight, overweight and obesity on disease manifestations in Chinese patients with AS. Approximately half of patients with AS were either underweight or obese/overweight according to the developed Chinese standard on BMI classification for adults. These patients had higher disease activity based on two assessment methods of disease activity (ASDAS and BASDAI), and were more likely to experience a poorer physical function (BASFI), worse health index (ASAS HI) and spinal mobility (BASMI).
Studies have suggested that obesity could promote the pathogenesis and inflammatory processes of several inflammatory diseases, such as rheumatic arthritis and psoriatic arthritis, while our study also demonstrated that obesity might have a significant correlation with poor clinical outcomes of patients with AS, but not with overweight and poor clinical outcomes in patients with AS. Some of the mechanisms were relatively easy to explain the association. The abnormal accumulation of adipose tissue in patients with high BMI was significantly infiltrated by macrophages secreting adipocytokines or cytokines. One study inferred that adipocyte-derived factors might stimulate macrophage activation, and identified pigment epithelium-derived factors as an inflammation mediator secreted by adipocytes and mediated macrophage activation. 26 Recombinant pigment epithelium-derived factor activated macrophages to release TNF-α, IL-6 and IL-1 into the systemic circulation. Another study suggested that TNF was critical to the cognitive experience of pain and the emotional changes associated with chronic pain. 27 In addition, obesity has been considered as a significant influence factor of poor outcomes in the general people and in some rheumatic diseases. A study showed that IL-6 concentration was increased in patients with obesity with systemic lupus erythematosus. 28 Another study suggested that the extent of endogenous cytokine control was very crucial for the development of bone tissue destruction in patients with rheumatoid arthritis. 29 Obesity was associated with higher disease activity, worse physical function and health-related quality of life, and had a significant negative effect on obtaining a low DAS28 in patients with rheumatoid arthritis. 30
Besides, overweight and obesity could seriously affect the treatment response to TNF-α inhibitors in patients with AS. Current some studies have explored the impact of obesity on clinical responses to treatment of TNF-α inhibitors in patients with arthritides.14,31,32 These studies suggested that compared to patients with normal weight, the number of good responders among patients with obesity was reduced. Ottaviani et al. 31 reported in a retrospective study including 155 AS patients that compared with normal-weight patients, the responses to treatment in patients with obesity were significantly lower, defined as 50% improvement in BASDAI and VAS after 6-month infliximab treatment. Another study showed that of 153 patients with AS receiving TNF-α inhibitor treatment, having an elevated BMI was related to the decreased probability of clinical efficacy (odds ratio, 40; 95% confidence interval, 4.2–333.3). 32 In a study conducted in a clinical practice setting, patients with obesity showed a significantly lower serum adalimumab level as compared to patients with normal weight, which was not related to the increased presence of immunogenicity in patients with obesity. 14 As in our study, the increase in BMI and overweight/obesity were also independently related to the worse clinical responses in patients with AS treated with biologics after adjusting potential confounders. These studies have not yet elucidated the underlying mechanisms behind the association between obesity and some less favorable disease outcomes in patients with AS. Some retrospective studies have suggested that obesity could affect the volume of distribution and pharmacokinetics of drugs, which meant that it could alter the response to biologics, and decrease their efficacy.31,33,34
The association of underweight with AS disease features found in our study was unexpected, in that underweight patients also had an unfavorable disease activity and poor functional capacity. Thus, the BMI was not the lower the better, and the association appeared to be U-shaped, as both very low and high BMI related to poor disease outcomes in AS patients. Among these patients, a significant reduction in BMI might be the result of high disease activity over many years rather than vice versa. Huang et al. 35 investigated the prevalence of malnutrition reflected by BMI in patients with AS in China. The results suggested that 23.8% of the patients had malnutrition, and the prevalence of malnutrition risk in patients with pain score ⩾5 was higher than that in patients with pain score <5. Furthermore, a study even suggested that underweight has been associated with increased mortality in patients with rheumatoid arthritis, and highlighted the importance to maintain a certain muscle mass. 36 Currently, the mechanism on explaining the higher disease activity, physical dysfunction, worse health index and poor prognosis in underweight AS patients with very low BMI has not been elucidated. We should pay attention to this and continue to explore the pathophysiological mechanisms involved.
It was very important to identify underweight or obesity as a cause of decreased quality of life and an inducement to inflammation in patients with AS, as underweight or obesity was a risk factor that could be adjusted, and such adjustments would alter the risk. 37 Among the general people, reducing obesity could improve function capacity and reduce pain and concentrations of inflammatory markers. 28 Previous studies shown that lost weight had a beneficial effect on disease status of individuals with rheumatoid arthritis, and the underlying mechanisms behind the associations might be directly associated with exercise rather than the indirect effect of weight loss. 30 Regular exercise, whether for patients with obesity or underweight patients, was the best way to maintain a good BMI level and increase muscle mass. Furthermore, the skeletal muscle could contribute to an anti-inflammatory milieu, and secrete muscle-derived IL-6, which was the prototype myokine and had anti-inflammatory effects by responsible for increasing the circulating levels of the anti-inflammatory cytokine IL-10 and IL-1 receptor antagonists.38–40 However, obesity itself was often considered a barrier to exercise. 41 Compared to patients with a normal weight, the patients with obesity had fewer positive perceptions on the benefits of exercise and increased awareness of barriers to exercise. 9 Besides, if patients did not get enough nutrients from their diet to maintain a healthy body weight, it could exacerbate their fatigue, which would also lead to a reluctance to exercise. Therefore, it was very important to intelligently supervise patient to exercise and cultivate patient’s habits to exercise in the management of patients with AS.
Conclusion
Both underweight and obesity except for overweight were associated independently with worse disease activity, physical function and health status. Overweight and obesity might impact on treatment responses to biologics in patients with AS. This argues that weight management, to maintain it at a normal level, should be one of the disease management strategies in patients with AS.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X211030792 – Supplemental material for Underweight and obesity are strong predictors of clinical outcomes in patients with ankylosing spondylitis: data from the Smart-phone SpondyloArthritis Management System
Supplemental material, sj-docx-1-tab-10.1177_1759720X211030792 for Underweight and obesity are strong predictors of clinical outcomes in patients with ankylosing spondylitis: data from the Smart-phone SpondyloArthritis Management System by Lidong Hu, Xiaojian Ji, Yiwen Wang, Siliang Man, Xingkang Liu, Lei Wang, Jian Zhu, Jidong Cheng and Feng Huang in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Author contributions
Lidong Hu and Xiaojian Ji contributed equally to this work. Huang Feng, Jidong Cheng and Jian Zhu designed and supervised the study. All the authors contributed to collection of clinical data. Lidong Hu, Xiaojian Ji, Yiwen Wang and Siliang Man analyzed and interpreted the data. Xingkang Liu and Lei Wang collected and analyzed the clinical data and prepared the tables. Lidong Hu and Xiaojian Ji drafted and revised the manuscript. Feng Huang interpreted the results and revised the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.