
Abstract
Background:
Hip fractures are a major public health concern among elderly individuals. This study aimed to investigate potential perioperative factors that predict 1-year functional outcome, quality of life (QoL), care demands, and mortality in geriatric patients with a hip fracture.
Methods:
We prospectively enrolled geriatric patients who had undergone hip fracture surgery in one medical center from December 2017 to December 2019. Basic demographic data, handgrip strength, and responses to questionnaires for QoL and activities of daily living (ADL) before the injury were collected at baseline. QoL, ADL, additional care demands other than family support, and mortality events were monitored at 1 year after the operation.
Results:
Among 281 patients with a hip fracture, 39 (13.9%) died within 1 year of the index operation. The mean follow-up interval for the survivors was 403.3 (range: 358–480) days. Among the 242 survivors, ADL and QoL considerably decreased at approximately 1 year following hip surgery. Up to 33.9% of the participants became severely dependent and needed additional care at 1-year follow up. Prefracture ADL status was the crucial predictor for functional outcome, QoL, and additional care demand at 1-year follow up. Cox regression models indicated that male sex, low preoperative serum creatinine, handgrip strength, long surgical delay after a falling accident, and high Charlson Comorbidity Index were considerably associated with a high 1-year mortality risk in the geriatric hip fracture population.
Conclusion:
Hip fracture has long-lasting effects (e.g. functional loss, decline in QoL, increased care demands, and high postoperative mortality rate) on the geriatric population. A robust screening method must be developed for identifying potential prognostic factors, and a stratified care approach must be used that accounts for personalized risks to improve functional outcomes and reduce mortality after hip fracture in geriatric patients, especially in Taiwan.
Introduction
Hip fracture is a serious and debilitating injury among the geriatric population leading to functional dependence, social costs, and death.1,2 The number of hip fracture cases is increasing and is expected to reach 4.5 million worldwide by the year 2050. 3 In Asia, the number of hip fracture cases is estimated to increase from 1,124,060 in 2018 to 2,563,488 in 2050, contributing to an increase in the direct cost of treating hip fracture from US$9.5 billion to US$15 billion. 4 In addition, the number of hip fracture cases is estimated to increase from 18,338 in 2010 to 50,421 in 2035 in Taiwan, 5 inevitably causing a major socioeconomic impact in the near future.
For the geriatric population, hip fracture can be disastrous and fatal and was once regarded as the proverbial straw that breaks the camel’s back. Nationwide population-based cohort studies in Taiwan have reported that 1-year mortality following a geriatric hip fracture ranges from 14.0% to 18.1%.6–8 In addition, our previous report revealed that only one in five Taiwanese geriatric patients regains preinjury functional abilities by 6 months following hip fracture surgery, 9 and only 8.2% of such patients are able to walk unassisted at 1 year after surgery. 10 The functional loss among geriatric patients after hip fracture surgery is a critical concern for caregivers, causing a high care burden for one-fifth of the caregivers of patients with hip fracture. 11 In response to the increasing number of hip fracture events corresponding to an increase in the aging population, establishing a public health policy with a robust treatment protocol is crucial and necessary.
With knowledge of prognostic factors, clinicians can adopt a stratified care approach by prioritizing geriatric patients with hip fracture at a high risk of poor functional outcomes or high mortality for intensive care. 12 Several factors have been shown to predict outcome and mortality in patients with a hip fracture. Functional outcomes after hip fracture have been associated with advanced age, sex, fracture type, surgical delay, and preinjury functional status.13–15 In addition, quality of life (QoL) following repair of a hip fracture in elderly individuals has been associated with sex, preinjury functional and psychosocial status, and comorbidity.9,16 Major predictors of postoperative mortality in patients with hip fracture have been identified as age, sex, comorbidities, surgical delay, cognitive impairment, and poor renal function at presentation.17–20 However, findings regarding predictors of the long-term effect of hip fracture on activities of daily living (ADL), QoL, care demands, and mortality for elderly individuals have varied across studies. Moreover, associating these factors has been criticized: for example, older patients who are prone to have more comorbidities may present with a poorer preinjury functional status than do younger patients, which might interfere with the use of weight as a predictor of outcomes among these factors. In addition, few studies are available that have undertaken long-term follow up of the geriatric population, and further investigations are required to yield a quantitative basis for making future policy decisions in response to the increasing number of hip fracture cases and burden worldwide.
This prospective study aimed to investigate several crucial perioperative factors affecting the 1-year functional outcome, care demands, and mortality in patients with hip fracture aged 60 years or older. We hypothesized that preinjury functional status is a decisive factor for predicting 1-year functional outcome, QoL, and care demands in geriatric patients after hip fracture surgery. However, several risk factors, including sex, comorbidity, handgrip strength, surgical delay, and renal function at presentation, may be associated with postoperative mortality in geriatric patients following hip fracture surgery.
Methods
Study design
Patients who were diagnosed with hip fracture and underwent an operation in one medical center in Taiwan between December 2017 and December 2019 were prospectively enrolled. All patients deemed eligible for inclusion were contacted by the researchers and provided with detailed study information. Patient eligibility for enrollment was determined by the researchers by applying the study inclusion and exclusion criteria. Patients were included if they were at least 60 years old, had a hip fracture, namely femoral neck fracture (FNF) and peritrochanteric fracture (PTF), and were scheduled for surgery, namely hemiarthroplasty or internal fixation with intramedullary nailing by using in situ cannulated screws or dynamic hip screws. Patients were excluded if they were to undergo hip surgery for a reason other than a primary hip fracture, including osteoarthritis, trauma, tumor, infection, and avascular necrosis of the femoral heads.
Basic demographic data were collected for each patient according to medical records: age, sex, body mass index, fracture type, namely FNF or PTF, surgical method, namely hemiarthroplasty or internal fixation, surgical time, and blood loss. In addition, previously reported perioperative predictors for functional outcomes and mortality after hip fracture were recorded, namely Charlson Comorbidity Index (CCI), 17 bone mineral density [i.e. T-score obtained through dual-energy X-ray absorptiometry (DXA)], 21 preoperative serum hemoglobin and creatinine levels,20,22 American Society of Anesthesiologists (ASA) classification, 15 and handgrip strength. 23 Moreover, many studies20,24 have reported “surgical delay from falling accident” instead of “surgical delay from admission”, which was recorded for each patient in this study.
After giving consent for study enrollment, all participants completed questionnaires designed to elicit details on study metrics through interviews with patients and their families at baseline (during the admission for surgery). Specifically, the following assessment tools were used: the EuroQol-5D (EQ5D) for assessing QoL and the Barthel Index (BI) for measuring ADL. At 1-year follow up after hip surgery, the EQ5D and BI were again completed through telephone interviews with all participants. Moreover, additional care demands other than those imposed on family members, including the need to hire a caregiver or take up residency in a nursing home, at 1-year follow up and mortality within 1 year of hip surgery were recorded for all participants.
The entire protocol and instrumentation were approved by the Ethics Committee at Taipei Medical University, and ethical approval was registered as TMU-JIRB N201709053. More specifically, each participant provided a written informed consent for participation. All participants consented to being included in the study and data publication.
Instruments
The EQ5D is one of the internationally used instruments for measuring health-related QoL 24 and is based on five dimensions, namely mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each item has three levels of severity: no problems, some problems, or major problems. The Chinese version of the EQ5D was used in this study and it exhibited a high level of agreement (intraclass correlation coefficients >0.75) and convergent validity (Pearson’s correlation coefficients >0.95) with the value sets of the versions of the EQ5D from the UK, Japan, and Korea. 25
The BI is an ordinal scale used for measuring performance in ADL. 26 BI scores 0–100 with 10 variables describe ADL and mobility. A higher number is associated with a greater likelihood of being able to live at home independently following discharge from hospital. According to the proposed guideline, a BI score lower than 60 indicates ‘severe to total’ dependency. The BI can be used to accurately assess functional recovery in patients who undergo hemiarthroplasty after FNF. 27
Data analysis
Demographics and characteristics of the participants were analyzed using descriptive statistics, including mean [standard deviation (SD)] and frequency (percentage). Two multiple linear regression models were constructed to examine the potential predictors of QoL and ADL at 1-year follow up. Particularly, QoL and ADL at 1-year follow up were two dependent variables in multiple linear regression models. The multiple linear regression models included the same confounders (i.e. age, sex, body mass index, T-score, and preoperative serum hemoglobin and creatinine levels) and the same potential predictors (i.e. surgical delay after a falling accident, surgical methods and time, surgical blood, fracture types, ASA classification, handgrip strength, CCI, baseline QoL, and baseline ADL). Afterwards, one logistic regression model was constructed to explore the potential predictor of additional care demands at 1-year follow up. The logistic regression model had the same confounders and predictors as those in the two multiple linear regression models. Finally, a Cox regression model using multivariate analysis was used to investigate the potential risk of and protective factors for survival. All the statistics were analyzed using IBM SPSS 21.0 (IBM Corp., Armonk, NY, USA).
Results
In total, 346 patients who underwent surgery for hip fracture participated in this study. At 1-year follow up after hip surgery, 65 patients were lost to follow up. Thus, the study analyzed 281 participants with a mean age of 81.31 (SD = 9.75) years, 29.9% of whom were men (n = 84). In total, 238 participants (84.8%) completed the DXA assessment for bone mineral density, with an average T-score of −3.87 (SD = 1.13) during admission for hip surgery. The average surgical delay after a falling accident was 74.36 (SD = 196.70) h, and the average surgery time was 77.74 (SD = 40.75) min. At 1-year follow up, 39 participants had died within 1 year following the index operation, and the mean follow-up interval among the survivors was 403.30 (SD = 31.56, range: 358–480) days. Nearly one-third of survivors (33.8%, 82/242) needed additional care besides that from family members at 1-year follow up; 26 needed residency in a nursing home and 56 needed to hire a caregiver. Moreover, the participants had a decreased QoL (mean = 0.83, SD = 0.21 at baseline; mean = 0.76, SD = 0.24 at 1-year follow up) and ADL (mean = 82.53, SD = 25.51 at baseline; mean = 70.15, SD = 32.22 at 1-year follow up) after surgery (Table 1).
Participant characteristics (n = 281).

ADL, activities of daily living; ASA, American Society of Anesthesiologists; CCI, Charlson Comorbidity Index; FNF, femoral neck fracture; PTF, peritrochanteric fracture; QoL, quality of life; SD, standard deviation.
Among the 242 survivors 1 year after hip surgery, only 107 (44.2%) had returned to baseline ADL. Thus, 16.5% (40/242) of the geriatric patients with a hip fracture had severe to total dependency at baseline, but up to 33.9% (82/242) had become severely dependent at 1-year follow up. Multiple linear regression models showed that baseline ADL significantly predicted QoL [standardized coefficient (β) = 0.363; 95% confidence interval (CI) for unstandardized coefficient = 0.002, 0.005; p < 0.001] and ADL (β = 0.505; 95% CI for unstandardized coefficient = 0.454, 0.876; p < 0.001) at 1-year follow up after controlling potential confounders (Table 2). In addition, body mass index significantly predicted follow-up ADL (β = 1.182; 95% CI for unstandardized coefficient = 0.122, 2.242; p = 0.029). Moreover, the logistic regression model demonstrated that the baseline ADL [odds ratio (OR) = 0.946; 95% CI = 0.923, 0.970; p < 0.001] and female sex (OR = 1.093; 95% CI = 1.093, 8.140; p = 0.033) were significant predictors of additional care demands at 1-year follow up after controlling potential confounders (Table 3).
Multiple linear regression models on quality of life and activities of daily living.

All linear regression models were significant (for follow-up QoL: F = 6.79, df = 16, p < 0.001, R2 = 0.365, and adjusted R2 = 0.311; and for follow-up ADL: F = 10.27, df = 16, p < 0.001, R2 = 0.465, and adjusted R2 = 0.420).
ADL, activities of daily living; ASA, American Society of Anesthesiologists; B, unstandardized coefficient; Beta, standardized coefficient; CCI, Charlson Comorbidity Index; df, degrees of freedom; FNF, femoral neck fracture; LLCI, lower limit confidence interval at 95%; QoL, quality of life; Ref, reference; SE, standard error; ULCI, upper limit confidence interval at 95%.
Logistic regression model on additional care.

The entire logistic regression model was significant (χ2 in the log-likelihood ratio test = 77.10; df = 16; p < 0.001; Cox & Snell R2 = 0.312; Nagelkerke R2 = 0.434).
ADL, activities of daily living; ASA, American Society of Anesthesiologists; B, unstandardized coefficient; CCI, Charlson Comorbidity Index; df, degrees of freedom; FNF, femoral neck fracture; LLCI, lower limit confidence interval at 95%; OR, odds ratio; QoL, quality of life; Ref, reference; SE, standard error; ULCI, upper limit confidence interval at 95%.
Among our participants, the 1-year and 3-month mortality rates after hip surgery were 13.9% (39/281) and 51.3% (20/39), respectively. Cardiogenic shock and failure (15/39, 38.4%) was the main cause of mortality, followed by pneumonia (11/39, 28.2%) and upper gastrointestinal bleeding (4/39, 10.3%). A Cox regression model indicated that potential risk factors for mortality included preoperative serum creatinine [risk ratio (RR) = 1.282; 95% CI = 1.024, 1.605; p = 0.030], surgical delay after a falling accident (RR = 1.002; 95% CI = 1.001, 1.004; p = 0.006), and CCI (RR = 1.249; 95% CI = 1.039, 1.502; p = 0.018), and potential protectors of mortality included female sex (RR = 0.321; 95% CI = 0.130, 0.792; p = 0.014) and handgrip strength (RR = 0.841; 95% CI = 0.749, 0.944; p = 0.003) (Table 4).
Cox regression model on survival.
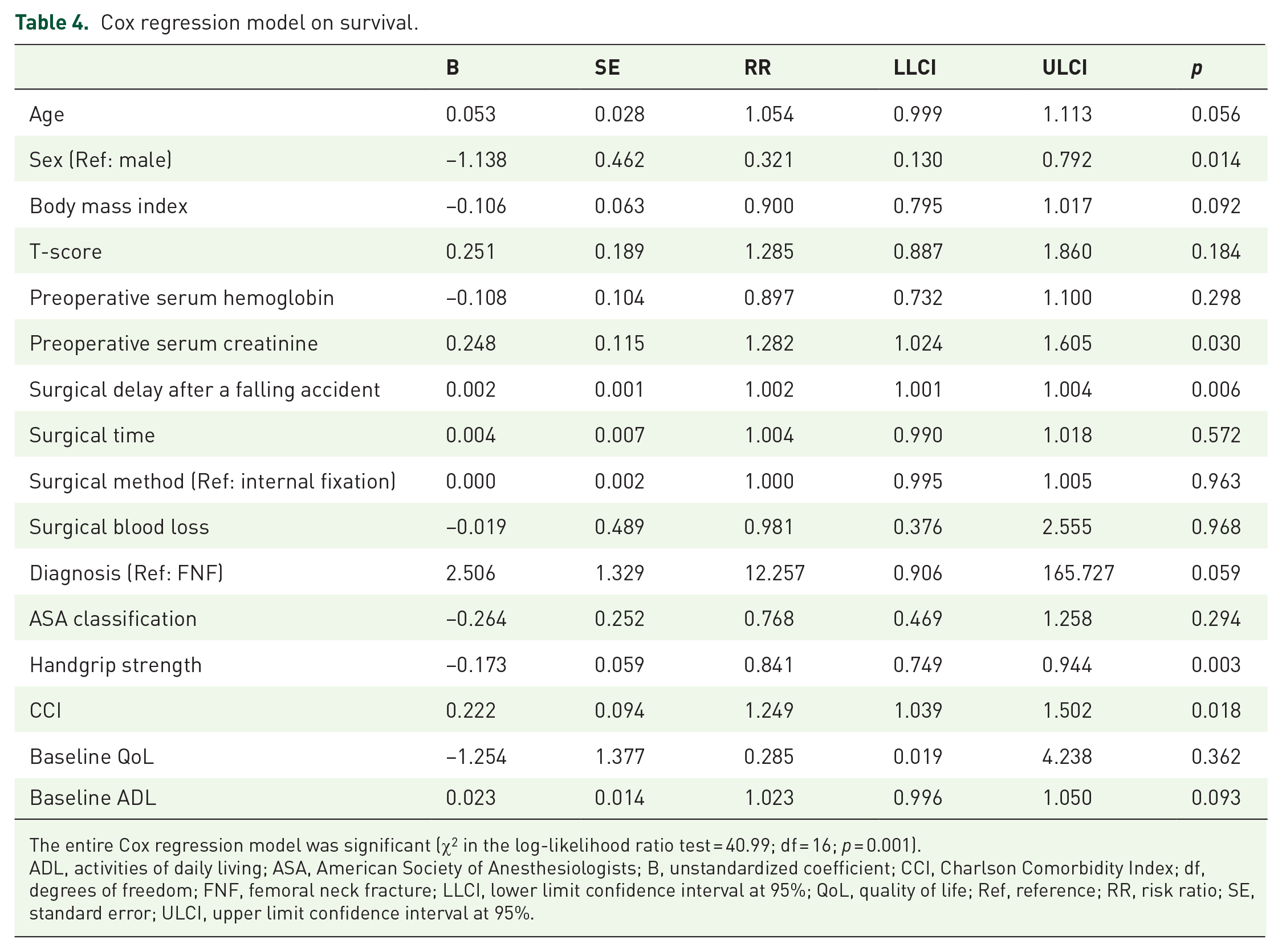
The entire Cox regression model was significant (χ2 in the log-likelihood ratio test = 40.99; df = 16; p = 0.001).
ADL, activities of daily living; ASA, American Society of Anesthesiologists; B, unstandardized coefficient; CCI, Charlson Comorbidity Index; df, degrees of freedom; FNF, femoral neck fracture; LLCI, lower limit confidence interval at 95%; QoL, quality of life; Ref, reference; RR, risk ratio; SE, standard error; ULCI, upper limit confidence interval at 95%.
Discussion
This prospective study demonstrated that hip fracture has long-term effects, including functional loss, decline in QoL, increased care burden, and high 1-year mortality rate, on the geriatric population. The ADL of geriatric patients before hip fracture was a crucial predictor of functional outcome, QoL, and additional care demands at 1-year follow up after hip surgery. In addition, high preoperative serum creatinine, long surgical delay after a falling accident, and high CCI were significant risk factors for mortality within 1 year of hip surgery in the geriatric population. Moreover, geriatric patients with hip fracture who were female and had high baseline handgrip strength were expected to survive longer after hip surgery.
Permanent functional loss and associated decline in QoL were major concerns for geriatric patients with hip fracture. Our previous study prospectively followed 117 geriatric patients undergoing hip fracture surgery and found that only 20% regained baseline ADL after 6 months of follow up. 9 Poor ADL can predict and reflect poor QoL after the 6-month follow up. 9 In this extended study with a long follow up and large case number, although 44.2% of patients with geriatric hip fracture regained their prefracture ADL at 1-year follow up, the number of severely dependent patients at 1 year after hip surgery was twice that at baseline. Our findings are consistent with those of Civinini et al. 28 who reported that only 32.1% of 677 geriatric patients achieved full recovery or low-impairment mobility status, whereas 22.9% were highly mobility impaired or fully dependent at 1 year after hip surgery. 24 In addition, QoL declined with the loss of ADL in this study. This reflects the finding of a study that used the Norwegian hip fracture register and determined that hip fracture drastically affects patients’ health-related QoL with sustained deterioration even 1 year after the fracture. 29 However, unlike previously reported predictors of poor functional outcomes after hip surgery, including advanced age, female sex, long surgical delay, and poor preinjury functional status,13–15 this study demonstrated that only baseline ADL can predict the 1-year function and QoL following hip surgery in the geriatric population. This emphasizes the necessity for a stratified care approach with robust rehabilitation programs for geriatric patients with hip fracture with poor prefracture ADL to prevent poor long-term outcomes following hip surgery.
Motor impairment following hip fracture among geriatric patients may cause a potential burden for their caregivers resulting in the need for additional help with patient care. Functional loss after a hip fracture was reported to be correlated with the service time provided to assist with ADL in a study on the long-term care insurance system. 30 Furthermore, monthly care costs were correlated with walking ability in elderly patients after surgical treatments for hip fractures. 31 In Taiwan, Lin and Lu 32 reported that the families of geriatric patients with hip fracture experienced a high care burden within 1 month of hip surgery, and up to 77.6% of the families needed help with care tasks. 32 However, clinical reports on changes in care demands in the long term are lacking, and long-term functional loss may be inevitable among geriatric patients with hip fracture. Our study demonstrated that one-third of patients needed additional care other than that from their family at 1 year after hip surgery, indicating the long-lasting socioeconomic burden following hip fracture. Similarly, prefracture ADL was the most crucial predictor for determining long-term needs for additional care following hip fracture surgery in the geriatric population.
Wu et al. 33 followed 192 Taiwanese geriatric patients with hip fracture for 1 year and reported that their 1-year mortality rate was up to 20.1%. However, the overall 1-year mortality rate following hip surgery in our study was only 13.9%, which was close to the estimation of 14% from a national population-based study in Taiwan. The 1-year mortality rate in our study was lower than that reported by Wu et al. 33 probably because of the different characteristics of the enrolled participants. Although the average age of participants was similar in both studies, the number of male participants was higher in the study by Wu et al. 33 than in our study (64.7% versus 29.9%), which may have resulted in a higher 1-year mortality in the study by Wu et al. 33 because evidence suggests that men have a worse prognosis after hip fracture, with a 4.6-fold increased mortality compared with 2.8-fold increased mortality in women. 34 In addition, cardiogenic problems and infection were reported to be the main causes of mortality in this study, which may be attributable to the population of fragile and susceptible elderly individuals with long-term immobility following hip surgery. 35
In concurrence with studies that have reported predictors of mortality risk following hip surgery,17,34,36,37 our study also demonstrated that male sex, high preoperative serum creatinine, low baseline handgrip strength, and high CCI were poor indictors of a high risk of mortality within 1 year of hip surgery in the geriatric population. In addition, long surgical delay after a falling accident was an important predictor for mortality risk in this study. Numerous studies have disclosed that a delay in surgery from admission was associated with high in-hospital and 6-month mortality rates following hip surgery.15,38 However, under the National Health Insurance program in Taiwan, reducing the waiting time for hip fracture surgery to reduce the total days of hospital stay is acceptable. In our study, almost all geriatric patients with a hip fracture (95%) received hip fracture surgery within 48 h of admission, making it difficult to discuss the association of surgical delay from admission with mortality risk. Instead, we used surgical delay after a falling accident, which was interpreted as the real immobilizing time before surgery but has seldom been discussed in the literature. Therefore, surgical delay after a falling accident was analyzed in this study and indeed proved to be a crucial predictor for 1-year mortality risk after hip surgery. These findings highlight the importance of rapid medial consultation once fragile elderly individuals fall to minimize mortality risk.
This study identified several important prognostic factors for 1-year functional outcome and mortality after surgery in geriatric patients with a hip fracture. Although the baseline condition of some prognostic factors including prefracture ADL, gender, and CCI may not be correctable, the clinical value of recognizing these potential risks factors may offer clinicians a way to adopt a stratified care approach by prioritizing geriatric patients with hip fracture at a high risk of poor function or mortality to optimize the postoperative outcomes. 12 Evidence has revealed that ‘a comprehensive multidisciplinary hip fracture care pathway’, which consists of standard bundles of care and integrated care managers engaging in patient education, care coordination, and discharge planning, can effectively reduce time to surgery, rate of in-hospital postoperative complications, mortality rate, and readmission rate.39,40 In addition, evidence also disclosed that the implementation of an orthogeriatric co-management (OGCM) for patients with hip fracture can effectively facilitate functional gains and reduce length of hospital stay and postoperative mortality,41,42 although the cost-effectiveness of OGCM was still criticized. 43 With knowledge of prognostic factors for patients with hip fracture prone to poor outcomes following hip surgery, medical resources including multidisciplinary hip fracture care pathway or OGCM can be appropriately implemented on these patients in need of intensive care. However, owing to the lack of long-term results on the stratified care approach for patients with hip fracture based on a standardized screening protocol for these prognostic factors, further prospective and interventional studies are warranted to conduct clinical and economic evaluation of the efficacy of a stratified care approach for the patients with hip fracture with estimated poor prognosis.
Limitations
Our study has some limitations. First, the representativeness of our sample was limited by its small case number. All participants were recruited from the same institution and might not represent the geriatric population undergoing hip fracture surgery throughout Taiwan. Second, not all of the initially enrolled participants could be followed up for 1 year after hip surgery. However, the rate of loss to follow up in this study was 18.8%, which is lower than the recommended 20% to minimize the threat to validity. 44 Third, functional outcome measurement was based on patient-reported or caregiver-reported ADL but lacked objective functional assessments, which may have resulted in potential observer bias. Fourth, geriatric patients with hip fracture were prone to secondary fracture, which may also affect the risk of postoperative mortality. 45 However, this study did not assess the information of secondary fracture events. Therefore, future studies on similar topics are warranted to include this important confounder.
Fifth, ample evidence reveals that intensity of post-hospital rehabilitation (e.g. physiotherapy) is associated with functional recovery following hip surgery in geriatric patients with a hip fracture. 46 Specifically, physiotherapy is found to be a positive factor for QoL improvement and resumption of ADL. 47 Unfortunately, post-hospital rehabilitation treatment for the participants was not studied and collected in this study. Therefore, future studies should consider the role of physiotherapy should they want to conduct a similar investigation. Sixth, this study only reported the postoperative 1-year outcomes, therefore, results from a longer follow up among these geriatric patients who underwent hip fracture surgery are still needed to portray the full picture of the trajectory for these patients. Last, this investigation was conducted as an observational study without intentional changes to the routine of postoperative care among the participants. Although it seems reasonable to take a stratified care approach for patients with a hip fracture based on the reported prognostic factors in order to reverse the estimated poor prognosis, evidence for the association of care pathway and postoperative outcomes is still lacking. Therefore, future studies are needed to elucidate the clinical effectiveness of a stratified care approach. However, even with these limitations, this study provided quantitative data on the 1-year outcomes and mortality following hip surgery among Taiwanese geriatric patients and can be a valuable reference for establishing public health policy to serve the needs of these vulnerable elderly individuals.
Conclusion
Hip fracture has long-lasting effects on the geriatric population, including functional loss, a decline in QoL, increased care demands, and high postoperative mortality rate. Baseline ADL was the most crucial predictor of 1-year functional outcome and QoL. However, male patients with high preoperative serum creatinine, low handgrip strength, and high CCI had a particularly high mortality risk within 1 year of hip surgery. Clinicians must construct a robust screening method for identifying potential prognostic factors and provide stratified care depending on personalized risks to improve functional outcomes and reduce mortality after hip fracture in geriatric patients in Taiwan.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to Wan Fang Hospital (Grant numbers 109-wf-eva-11, 109-wf-eva-30, and 110-swf-01) for financially supporting this research.