
Abstract
Objective:
To assess the efficacy and safety of tocilizumab (TCZ) in Caucasian patients with refractory Takayasu’s arteritis (TAK) in clinical practice.
Methods:
A multicenter study of Caucasian patients with refractory TAK who received TCZ. The outcome variables were remission, glucocorticoid-sparing effect, improvement in imaging techniques, and adverse events. A comparative study between patients who received TCZ as monotherapy (TCZMONO) and combined with conventional disease modifying anti-rheumatic drugs (cDMARDs) (TCZCOMBO) was performed.
Results:
The study comprised 54 patients (46 women/8 men) with a median [interquartile range (IQR)] age of 42.0 (32.5–50.5) years. TCZ was started after a median (IQR) of 12.0 (3.0–31.5) months since TAK diagnosis. Remission was achieved in 12/54 (22.2%), 19/49 (38.8%), 23/44 (52.3%), and 27/36 (75%) patients at 1, 3, 6, and 12 months, respectively. The prednisone dose was reduced from 30.0 mg/day (12.5–50.0) to 5.0 (0.0–5.6) mg/day at 12 months. An improvement in imaging findings was reported in 28 (73.7%) patients after a median (IQR) of 9.0 (6.0–14.0) months. Twenty-three (42.6%) patients were on TCZMONO and 31 (57.4%) on TCZCOMBO: MTX (n = 28), cyclosporine A (n = 2), azathioprine (n = 1). Patients on TCZCOMBO were younger [38.0 (27.0–46.0) versus 45.0 (38.0–57.0)] years; difference (diff) [95% confidence interval (CI) = -7.0 (-17.9, -0.56] with a trend to longer TAK duration [21.0 (6.0–38.0) versus 6.0 (1.0–23.0)] months; diff 95% CI = 15 (-8.9, 35.5), and higher c-reactive protein [2.4 (0.7–5.6) versus 1.3 (0.3–3.3)] mg/dl; diff 95% CI = 1.1 (-0.26, 2.99). Despite these differences, similar outcomes were observed in both groups (log rank p = 0.862). Relevant adverse events were reported in six (11.1%) patients, but only three developed severe events that required TCZ withdrawal.
Conclusion:
TCZ in monotherapy, or combined with cDMARDs, is effective and safe in patients with refractory TAK of Caucasian origin.
Introduction
Takayasu’s arteritis (TAK) is a large-vessel vasculitis (LVV) characterized by the affection of the aorta and its main branches. This may lead to the development of severe vascular complications, such as stenosis, aneurysms, and aortic dissection. 1 TAK mainly affects young females of Asian descent; however, TAK is increasingly being recognized among individuals of Caucasian origin from both European countries and the United States.2–5
Epidemiology studies have revealed an estimated incidence of 2–3 cases per million people per year in the United States. 5 The reported incidences in Europe range from 0.4 to 1.5 per million people year while the prevalence varies from 4.7 to 33 per million people.4,6
Clinical manifestations and outcomes in Caucasian patients with TAK diagnosis appear to differ from those originally observed in patients of Asian origin. Caucasian patients are usually older at diagnosis, with nearly 25% of patients aging 40–50 years. Cardiovascular comorbidities are more frequent among these patients, which may potentially increase the risk for developing vascular complications.3,5 The pattern of vascular affection also seems to be different in Caucasian patients. Supra-aortic vessels are more likely affected in Caucasian individuals, whereas abdominal vascular involvement is more frequent in patients of South-Asian descent.3,7 Disturbingly, a recent study showed that Caucasian patients with TAK diagnosis have a significantly higher mortality than other ethnic groups. 8
The mainstay treatment of TAK remains a combination of glucocorticoids and conventional disease modifying anti-rheumatic drugs (cDMARDs). 9 Nonetheless, relapses are common in TAK despite treatment with cDMARDs. 10 A recent French study involving 318 patients with TAK showed that 50% of patients experience a relapse and vascular complications in the first 10 years from diagnosis.
Tocilizumab (TCZ), a humanized monoclonal antibody directed against the interleukin 6 (IL-6) receptor, seems to be a promising therapeutic option for refractory TAK. Up to now, the main evidence for the efficacy of TCZ in TAK comes from retrospective studies,11–17 one small randomized clinical trial, 18 and one open trial; 19 however, none of these studies were focused on Caucasian population. As already mentioned, patients of Caucasian ethnicity usually have different demographic and clinical features which may influence treatment outcomes.
Taking all these considerations into account, our aim was to assess the efficacy and safety of TCZ for the management of refractory TAK in Caucasian patients from a real-world clinical setting.
Patients and methods
Study design
We conducted an observational, multicenter study in patients diagnosed with TAK who received at least one dose of TCZ in a real-world clinical setting from January 2014 to May 2020. Preliminary partial data on eight patients were previously reported. 13
Patients were diagnosed with TAK at the Rheumatology or Autoimmune Units of 26 national referral centers. TAK diagnosis was based on the American College of Rheumatology (ACR) 1990 criteria 20 or Ishikawa criteria modified by Sharma et al. 21 Vascular affection was confirmed in every patient by at least one imaging technique, including 18F-fluorodexyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) (Figure 1), magnetic resonance imaging angiography (MRI-A), and computed tomography angiography (CT-A).

PET/CT images of a 43 years-old woman with Takayasu’s arteritis showing an intense FDG uptake along the thoracic aorta (arrows) and the brachiocephalic trunk, subclavian and axillary arteries (head arrows).
The initial management of TAK was based on the classic pharmacological therapy strategy starting on a high dose of glucocorticoids, usually with an initial dose of prednisone between 40 and 60 mg/day, which was gradually tapered. cDMARDs and/or biologic therapy were added in patients with relapsing disease, or in those cases with adverse side effects related to glucocorticoid therapy.
As indicated by the Spanish National Guidelines for the administration of biologic therapy in patients with rheumatic diseases, the presence of infectious diseases had to be ruled out, including tuberculosis and hepatitis B or hepatitis C infections, before the onset of biologic therapy. To exclude latent tuberculosis, a tuberculin skin testing (PPD) and/or an interferon assay (quantiFERON), as well as a chest radiograph, were performed. In positive cases, prophylaxis with isoniazid was initiated at least 4 weeks before the onset of the biological agent and was maintained for 9 months. The presence of malignancies was also excluded in all the patients. 22
TCZ was prescribed as intravenous (IV) infusions at a standard dose (8 mg/kg/4 weeks) or as subcutaneous (SC) (162 mg/week) injections. It was started due to a lack of efficacy and/or unacceptable adverse side-effects related to previous therapy. Since TCZ is an off-label indication for TAK in Europe, written informed consent was requested and obtained from all the patients before starting therapy. Patients were treated with TCZ as monotherapy or combined with cDMARDs.
Clinical definitions and laboratory data
Remission was defined as the absence of new symptoms and the disappearance of all previous symptoms of TAK, along with the normalization of c-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Relapse was defined as the recurrence of signs or symptoms of TAK after a remission period of at least 6 months.
Limb claudication was defined as pain, tightness, heaviness, cramping and/or weakness in one or both of arms and/or legs. Chest pain was considered when pressure, pain, or heaviness in the chest was present. Constitutional symptoms included asthenia, anorexia, and weight loss greater than 5% of the normal body weight over the last 6 months before disease diagnosis. Fever was considered to be present if temperature was ⩾38°C. Headache if head pain was of recent development or had different characteristics than usual. Visual manifestations include blurred vision, diplopia, amaurosis fugax, unilateral or bilateral hemianopsia, and permanent unilateral or bilateral blindness. The definition of other clinical manifestations has been previously reported. 13
A full blood cell count, renal and liver function tests, as well as CRP and ESR were obtained at the time of TCZ onset and then at each follow-up visit. Normalization of CRP was considered when it was under 0.5 mg/dl and normalization of ESR when it was less than 25 mm/first hour.
Follow-up imaging techniques were performed based on each physician criteria. Changes from baseline in imaging results were qualitatively evaluated by a radiologist or nuclear medicine expert at each referral center. Imaging vascular improvement was defined as the partial or complete enhancement of the vessel wall thickness, stenosis, or occlusions, along with the absence of new vascular lesions at the follow-up imaging technique as compared with the baseline.
Adverse events were recorded and severe infection was considered to be present when a life-threatening infection, fatal, or requiring hospitalization occurred, intravenous antibiotics were required, or the infectious process led to persistent or significant disability.
In a further step, a comparative study was performed between patients who received TCZ as monotherapy (TCZMONO) and combined with cDMARDs (TCZCOMBO).
Data collection and ethics
Information was retrieved from the patient’s clinical records, including data on clinical and laboratory parameters, angiographic classification, 23 previous administered treatment for the management of TAK, clinical response to TCZ, and the development of side effects while patients were undergoing TCZ therapy. All data were stored in a computerized database. The study was approved by the Cantabria Institutional Review Board (approval number 2018-110). It was carried out in accordance with the protocol and with the standard work procedures that ensure compliance with the Declaration of Helsinki and Good Clinical Practice standards, regulated by (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on data protection (RGPD) that entered into force on 25 May 2018. Retrospective data have been obtained during routine clinical practice with the informed consent of the patients to be treated in a service that performs assistance and research tasks.
Statistical analysis
Statistical analysis was performed using SPSS Statistics for Windows, version 18.0 (SPSS Inc, Chicago, IL, USA). All continuous variables were tested for normality and results were expressed as mean ± standard deviation (SD) or as a median and interquartile range (IQR) as appropriate. The comparison of continuous variables among time periods was performed using the Wilcoxon signed rank test. A p-value < 0.05 was considered as statistically significant in all the calculations.
Results
Patients’ characteristics
Sixty patients with TAK diagnosis who received TCZ were initially enrolled in the study. Six patients were non-Caucasians and were therefore excluded from the analysis (Figure 2). In consequence, we assessed 54 patients (46 women/8 men), with a median (IQR) age of 42.0 (32.5–50.5) years old at TCZ onset. The median time from TAK diagnosis to TCZ therapy was 12.0 (3.0–31.5) months. The main clinical manifestations at TCZ onset were constitutional symptoms (59.3%) and limb claudication (55.6%). The most common pattern of vascular affection was type IIa (31.5%), which involves the ascending aorta, aortic arch, and its branches. In contrast, type III (7.4%) and type IV (7.4%), which predominantly affects abdominal vessels, were the less frequent patterns of vascular inflammation. The main general features, laboratory data, previous therapies, and treatment at baseline are shown in Table 1. A total of forty-two (77.8%) patients were previously treated with at least one cDMARD, mainly methotrexate (MTX) (n = 37), followed by azathioprine (n = 10), cyclophosphamide (n = 8), mycophenolate mofetil (n = 6), and cyclosporine A (n = 2). Twelve patients (22.2%) also received at least one biologic agent before TCZ onset: infliximab (n = 10), adalimumab (n = 2), abatacept (n = 2), etanercept (n = 1), and rituximab (n = 1) (Figure 2).
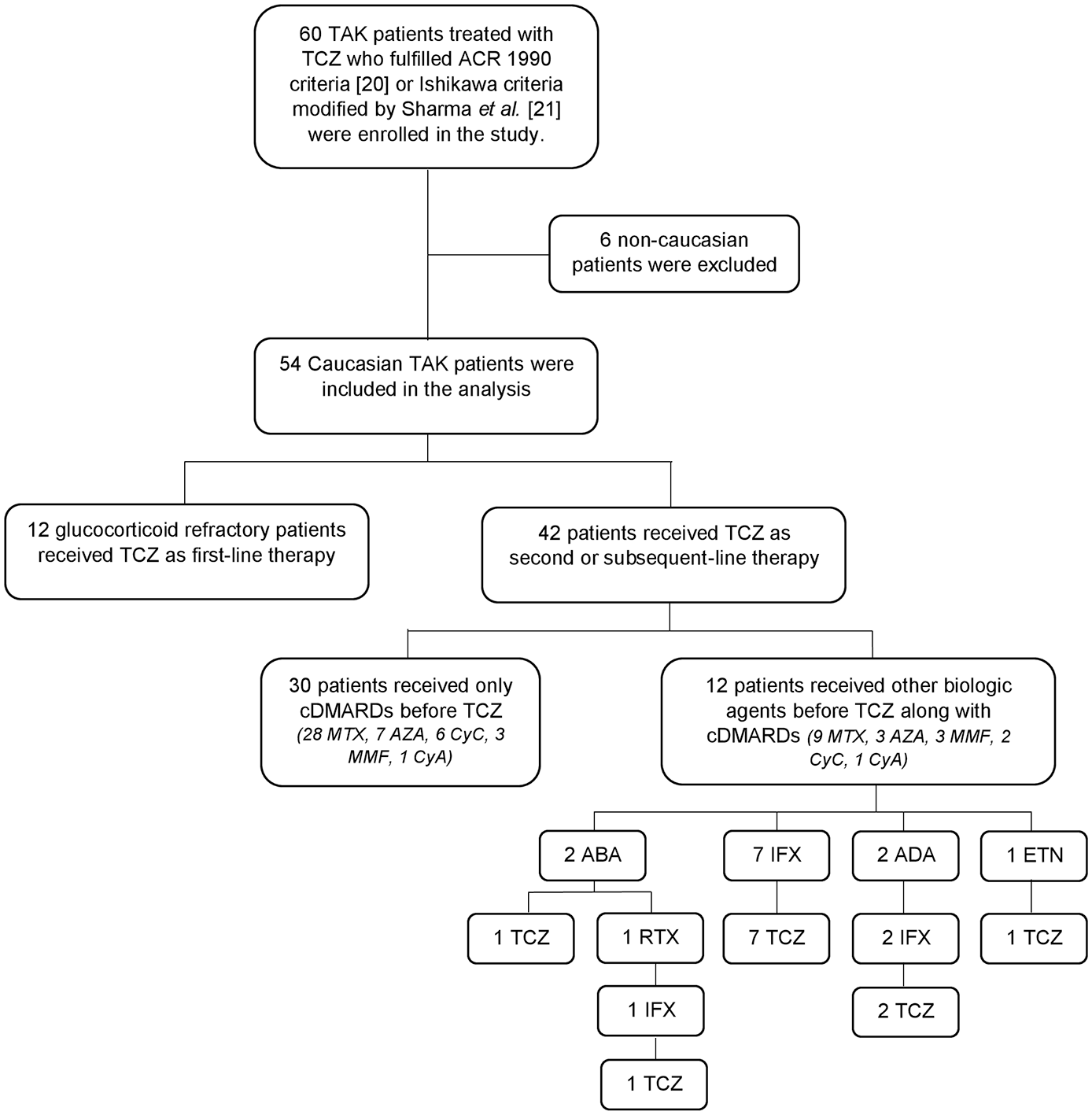
Flow chart of patients who met the inclusion/exclusion criteria for the study showing the immunosuppressive therapy prescribed prior to Tocilizumab therapy.
Baseline features of 54 Caucasian patients with refractory Takayasu’s arteritis who were treated with Tocilizumab.

Differences between patients who received TCZ monotherapy (TCZMONO) and TCZ combined with conventional disease modifying anti-rheumatic drugs (TCZCOMBO).
CI, confidence interval; CRP, C-reactive protein (mg/dl); ESR, erythrocyte sedimentation rate (mm/first hour); IQR, interquartile range; n, number; TAK, Takayasu’s arteritis; TCZ, tocilizumab.
TCZ was administered IV to 40 (74.1%) patients and SC to 14 (25.9%). The maintenance dose of TCZ ranged from 8 mg/IV/kg/4 weeks to 4 mg/IV/kg/8 weeks, and from 162 mg/SC/week to 162 mg/SC/every other week.
TCZMONO was administered to 23 (42.6%) patients and TCZCOMBO to 31 (57.4%) patients. In the TCZCOMBO group, the combined drugs used were: MTX (n = 28), cyclosporine A (n = 2), and azathioprine (n = 1). Baseline features of these subgroups of patients are summarized in Table 1. Patients on TCZCOMBO were significantly younger than those on TCZMONO. No other statistically significant differences were found between both groups, but a trend to longer disease duration and higher levels of acute phase reactants was observed in patients on TCZCOMBO.
Efficacy outcomes
Remission was achieved in 12/54 (22.2%), 19/49 (38.8%), 23/44 (52.3%), and 27/36 (75%) patients at 1, 3, 6, and 12 months, respectively. The improvement of laboratory parameters and reduction of prednisone dose throughout follow-up is shown in Table 2 and Figure 3. The percentage of patients who achieved remission was similar in patients receiving TCZMONO and TCZCOMBO (log rank p = 0.862) (Figure 4). The age-adjusted hazard ratio (HR) at 12 months = 1.33; 95% confidence interval (CI) = 0.30–5.90; p = 0.71.
Main outcome variables of 54 Caucasian patients with refractory Takayasu’s arteritis treated with tocilizumab.

p < 0.01 versus baseline (Wilcoxon test).
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IQR, interquartile range; n, number; SD, standard deviation.

Spaghetti plot of changes in C-reactive protein and hemoglobin for individual patients from baseline to 12 months.

Kaplan–Meier plot showing remission results in patients who received Tocilizumab as monotherapy (TCZMONO) and combined with cDMARDs (TCZCOMBO).
A follow-up imaging technique was performed in 38 (70.4%) patients after a median (IQR) of 9.0 (6.0–14.0) months. Improvement in imaging findings was reported in 28 (73.7%) patients, whereas no improvement was observed in 10 (26.3%) patients. Among these 10 patients with persistent inflammatory activity: four patients were in clinical remission, five patients experienced only partial clinical improvement and one patient did not respond to TCZ.
Follow-up and adverse events
The median (IQR) follow-up after TCZ onset was 13.5 (6.0–41.0) months (range 1–108 months). At 12 months, 29/36 (80.6%) were still receiving TCZ. At the end of follow-up, TCZ was discontinued in 18 patients. TCZ was stopped in six patients due to prolonged remission after a median (IQR) of 57.0 (52.0–76.5) months. None of these patients experienced a relapse after a median (IQR) of 37.5 (24.0–63.5) months from TCZ withdrawal. Other reasons for TCZ discontinuation were inefficacy (n = 4), pregnancy (n = 4), adverse reactions (n = 3), and loss to follow-up (n = 1).
A total of six (11.1%) patients developed relevant adverse events during TCZ therapy, most of them infections: severe pneumonia (n = 2), mild upper respiratory tract infection (n = 1), and herpes zoster (n = 1). Hematological side effects were observed in two patients: pancytopenia (n = 1) and thrombocytopenia (n = 1). TCZ was discontinued in the two patients with severe pneumonia and in the patient with pancytopenia. No deaths occurred during the study period.
Discussion
TAK is often a refractory disease despite conventional treatment with glucocorticoids and cDMARDs. 10 It should be noted that different clinical features and higher mortality rates have been observed in Caucasian patients with TAK diagnosis in comparison to other ethnic groups. 8 TCZ has shown to be effective for the management of TAK, but most studies predominantly involve patients of Asian origin. We report here the largest study focused on Caucasian patients with refractory TAK treated with TCZ. Most patients achieved remission and experienced radiological improvement in imaging techniques. In addition, TCZ led to a sparing glucocorticoid-dose effect and a good safety profile was observed.
In keeping with the scarce available literature addressing the distinctive features of Caucasian patients with TAK diagnosis,3,5,7 our patients were older at diagnosis and showed more frequently supra-aortic and thoracic aorta vessel involvement than patients of Asian origin.
Our results support the efficacy of TCZ for the management of TAK. Table 3 summarizes the most relevant studies conducted on patients with TAK treated with TCZ. As previously mentioned, two small trials, the TAKT 18 and the TOCITAKA 19 studies, showed that TCZ was useful for the management of TAK. The TAKT study is a placebo-controlled randomized trial which involved 36 Japanese patients. Longer time to relapse was observed in TCZ-treated patients, although no significant differences were achieved. 18 A steroid-sparing effect and an improvement in patient reported outcomes were observed in the open-label extension of the TAKT study over 96 weeks of TCZ treatment. 24 The TOCITAKA trial is an open-label prospective study that assessed the effect of TCZ to discontinue glucocorticoids after 6 months of IV TCZ therapy. Thirteen patients were included in the study, of which seven were Caucasians. Clinical remission and withdrawal of steroid therapy was achieved in 54% patients after 6 months of TCZ onset. 19 In our study, 52.3% of patients achieved remission at 6 months, but most of them were still receiving prednisone at a median (IQR) dose of 5.0 (5.0–10.0) mg/day. It is worth mentioning that we assessed patients with refractory TAK, whereas the TOCITAKA study only included treatment-naïve patients. The early use of TCZ may be more effective to induce TAK remission and rapid withdrawal of glucocorticoids, but well-randomized studies are needed to confirm this hypothesis.
The main studies on patients with Takayasu’s arteritis treated with TCZ.

Treatment response was defined as NIH scale <2 and prednisone <7.5 mg/dL #remission was defined as the absence of new symptoms and disappearance of all previous symptoms of TAK along with the normalization of CRP and ESR.
CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HR, hazard ratio; IV, intravenous; NIH, National Institute of Health; NR, non-reported; PD, prednisone; SC, subcutaneous; TCZ, tocilizumab.
Mekinian et al. 12 conducted a retrospective study of 46 patients with TAK diagnosis, including 29 individuals of Caucasian origin. Both treatment-naïve and refractory patients were included in the study. As in our series of patients, TCZ was mainly prescribed as IV injections. The percentage of patients who achieved clinical remission, defined as National Institute of Health (NIH) scale < 2 receiving less than 7.5 mg/day of prednisolone was 28%, 67%, and 79% at 3, 6, and 12 months, respectively. Similar clinical outcomes were observed in our study.
Mekinian et al. 12 observed that 20% and 17% of patients showed persistence of inflammatory activity in the follow-up imaging tests at 6 and 12 months, respectively. Nakaoka et al. 24 reported that 4 out of 28 (14.3%) of patients showed worsening from baseline in the follow-up imaging evaluations. Interestingly, only one of the four patients with worsened imaging data met the protocol-defined clinical criteria for TAK relapse. In our study, 10 (26.3%) of the 38 patients in whom an imaging follow-up test was performed showed no radiographic improvement. In an attempt to correlate imaging findings with clinical outcomes, we found that 4 of these 10 patients were in clinical remission despite the persistence of inflammatory imaging activity. These findings suggest that a discordance between clinical and imaging activity assessment may exist, as it has been observed in patients with large-vessel giant cell arteritis treated with TCZ. 25 The assessment of disease activity in TAK remains a challenge, particularly in patients undergoing TCZ therapy in whom acute phase reactants levels are not reliable indicators of relapse. Vascular progression has been reported on imaging techniques despite clinical remission and normal acute phase reactants.25–28
More research is needed to address the role of imaging techniques in monitoring disease activity in patients with LVV. In this sense, the identification of new biomarkers and the validation of disease activity scores, including clinical, laboratory, and imaging outcomes, will be crucial to improve the treatment of patients with TAK. 29
It remains unknown if the combination of TCZ with cDMARDs may have an additional favorable effect in the management of TAK. Mekinian et al. 12 observed similar event-free survival in 38 patients who received TCZ in monotherapy and 18 patients treated with combined therapy with cDMARDs. In our cohort of patients, those who received TCZ along with cDMARDs were younger, had longer TAK disease duration, and higher acute phase reactants levels at baseline. Despite these differences, we observed similar outcomes in patients receiving TCZ with and without cDMARDs. Further studies are needed to determine if combined therapy may be particularly useful in patients with more severe TAK disease.
It should be noted, that, in our study, none of the six patients in whom TCZ was discontinued due to sustained remission experienced a relapse after TCZ withdrawal. These six patients received TCZ for a median (IQR) of 57.0 (52.0–76.5) months before TCZ discontinuation and maintained remission until the end of the study period for at least 37.5 (24.0–63.5) months. In contrast, in the TOCITAKA study, 19 a relapse occurred in 45% of patients within 12 months of TCZ withdrawal when TCZ was discontinued after 6 months of treatment. A longer duration of TCZ therapy in our patients may explain these differences. Longer maintenance therapy with TCZ may be needed to prevent relapses. Further investigation is needed to define the most adequate duration of treatment with TCZ for TAK management.
TCZ has shown a good-safety profile in several studies.22,30 Our results are consistent with previous studies on TAK.11,12,18,19,24 In our study, only three (5.5%) patients had to discontinue TCZ due to severe effects including pneumonia and pancytopenia.
Despite the limitations derived from the retrospective nature of this study, our results support the efficacy of TCZ in the management of refractory TAK in a real-world setting. In addition, this is the first study to focus on Caucasian patients.
In conclusion, TCZ is effective and safe in Caucasian patients with refractory TAK despite demographical and clinical differences with other ethnic groups.
Footnotes
Acknowledgements
The authors thank Dr. Isabel Martínez-Rodríguez from the Nuclear Medicine Department of Hospital Universitario Marqués de Valdecilla, Santander (Spain) for the generous contribution of the image to Figure 1. The authors also thank all the members and patients of the participating hospitals.
Abbreviations
cDMARDS, conventional disease modifying anti-rheumatic drugs; CI, confidence intervals;
CT-A, computed tomography angiography; 18F-FDG PET/CT, 18F-fluorodexyglucose positron emission tomography/computed tomography; IL, interleukin; IQR, interquartile range; LVV, large-vessel-vasculitis; MRI-A, magnetic resonance imaging angiography; MTX, methotrexate; OR, odds ratio; PPD, tuberculin skin test; quantiFERON, interferon assay (for excluding latent tuberculosis); SD, standard deviation; TAK, Takayasu’s arteritis; TCZ, tocilizumab.
Conflict of interest statement
Disclosures that might be interpreted as constituting of possible conflict(s) of interest for the study: DP-P is supported by a research contract from the Carlos III Health Institute of Spain (Rio Hortega program, ref. CM20/00006) and has received research support from UCB Pharma, Roche, Sanofi, Pfizer, AbbVie, and Lilly. MAG-G received grants/research supports from Abbvie, MSD, Jansen, and Roche and had consultation fees/participation in company sponsored speaker’s bureau from Abbvie, Pfizer, Roche, Sanofi, Lilly, Celgene, and MSD. RB received grants/research supports from Abbvie, MSD, and Roche, and had consultation fees/participation in company sponsored speaker’s bureau from Abbvie, Lilly, Pfizer, Roche, Bristol-Myers, Janssen, UCB Pharma, and MSD. The remaining authors declare they do not have conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by RETICS Programs, RD08/0075 (RIER), RD12/0009/0013 and RD16/0012 from “Instituto de Salud Carlos III” (ISCIII) (Spain).
However, this research did not receive any specific grant from funding agencies in the commercial or not-for-profit sectors.