
Abstract
Background:
The flexion-rotation test (FRT) is widely used to detect movement dysfunction in the spinal segment C1/C2, especially in patients with cervicogenic headache. The current published literature indicates that range recorded during the FRT is not age dependent. This is questionable, considering the well documented relationship between aging and degeneration in the cervical spine and loss of cervical movement in older people. The present study therefore aims to examine the influence of age on FRT mobility, and to provide normative values for different age groups. An additional aim is to examine the influence of age on the ratio between lower and upper cervical rotation mobility.
Methods:
For this cross-sectional, observational study, healthy subjects aged from 18 to 90 years were recruited. The upper cervical range of rotation during the FRT was measured using a digital goniometer. Personal data including age, weight, height, and lifestyle factors were also assessed.
Results:
A total of 230 (124 male) healthy, asymptomatic subjects, aged between 18 and 87 years were included. Regression analysis showed that 27.91% (p < 0.0001) of the variance in FRT mobility can be explained by age alone, while 41.28% (p < 0.0001) of the variance in FRT mobility can be explained by age and total cervical range of motion (ROM). Normative values for different age decades were calculated using regression analysis. No significant influence of age on the ratio between ROM of lower and upper cervical rotation was found. There was no relevant impact of personal (gender, height, and weight) and lifestyle (smartphone and PC use) factors on ROM during the FRT.
Conclusion:
Upper cervical rotation mobility determined by the FRT correlates strongly with age; hence, the results of the FRT have to be interpreted taking into account the individual age of the tested subject. The ratio between lower and upper cervical rotation mobility is maintained in all age groups.
Introduction
Neck pain is one of the top five causes of years lived with disability (YLDs) in high- to middle-income countries worldwide, while tension-type headache is amongst the top three causes of YLDs. 1 For neck pain and headache, dysfunction of the cervical spine may be an important contributing factor. Examination of active and passive cervical movement is a routine component of the clinical examination of patients with neck pain or headache. 2 In many cases, rotation of the cervical spine is the most impaired movement. 3 This restriction can be caused by upper cervical spine (C0–C2) or lower cervical spine (C2–C7) dysfunction or both.
The largest contribution to cervical rotation occurs at C1/C2, 4 comprising slightly more than 50% of the total cervical range of motion (ROM).5,6 One way of measuring range of rotation between C1/C2 is the flexion-rotation test (FRT). By placing the cervical spine in maximum cervical flexion, all structures below C2 are theoretically constrained and have limited capability to contribute to rotation.7,8 In contrast to other passive segmental mobility tests, this test has been shown to be accurate and reliable even when used by inexperienced examiners.9–11 A change in mobility of more than 7°, measured by an analogue cervical ROM device (CROM), has been shown to be due to real change of upper cervical rotation and exceeds measurement error. 12 While numerous methods have been used to measure upper cervical ROM during the FRT, ranging from eyeball estimation to functional MRI, there are few reliable and valid instruments that can be used conveniently in clinical settings to collect kinematic data of cervical movements. One such instrument is a previously validated digital goniometer. 13
Robust evidence indicates a strong negative correlation between age and cervical ROM, with a significant decrease shown in all planes of movement.14–16 This loss of motion can be partly explained by age related degenerative change.17,18 However, the age-dependent reduction in cervical ROM is not continuous and differs between males and females. 15 Also it has been shown that during lateral flexion motion coupling in axial rotation increases with age, possibly reflecting compensatory mechanisms. 16 Conversely, it has been suggested that age does not significantly influence upper cervical rotation during the FRT. 19 Dvorak et al. even showed a slight non-significant increase in rotation during maximum flexion with increasing age. 20 In contrast, anatomical studies show an age-related linear increase in degenerative change of the atlantoaxial joints, particularly at the atlantodens interval, with less effect on the atlanto-axial facets.21–23 This relative sparing of degenerative change at the atlanto-axial facets with respect to more early and rapid change in the lower cervical segments suggests a slower and less pronounced age-dependent decrease in the rate of decline in upper cervical mobility. However, the recommended cut-off value of 34° rotation for a positive FRT indicating movement impairment between C1/2 has not been confirmed as being valid in different age groups. 24 Should the mobility of the upper cervical spine be age-dependent, many normal older people would erroneously show a positive test result, while younger symptomatic people may show a negative test result. Normal values for cervical mobility for a range of age groups have not yet been established. The primary aim of this study was therefore to evaluate whether age has an influence on the range of upper cervical rotation during the FRT.
The aims of the study were (1) to test if age influences upper cervical mobility during the flexion rotation test, and (2) to investigate if age influences the ratio between lower and upper cervical rotation mobility. We hypothesized firstly, that, with increasing age, upper cervical mobility decreases and, secondly, that the ratio between lower and upper cervical rotation is not affected by age.
Methods
Design
Cross-sectional observational study.
Participants, therapists, centres
Participants were recruited from rehabilitation centres, physiotherapy and medical practices, fitness studios, hospitals, sports facilities, as well as by word of mouth. Inclusion criteria were that subjects were asymptomatic (self-report) and aged 18–90 years. Exclusion criteria (self-report) were a history of neck trauma, neck pain, headaches, dizziness, jaw pain and facial pain in the last 3 months, neurological diseases, osteoporosis, pregnancy, anatomical abnormalities of the cervical spine or Down’s syndrome, dizziness, headache and/or facial pain during test movements, unable to read and understand German or English, and positive screening tests.
Four trained physiotherapists (three male, one female) performed the measurements. The mean age was 34 years (range 29–42). All physiotherapists worked in clinics and practices in Germany and had at least 7 years clinical experience in treating patients with musculoskeletal disorders. The physiotherapists were trained by qualified IMTA (International Maitland Teachers Association) teachers to perform the FRT in a standardised manner.
Subjects included in the study were 220 asymptomatic volunteers (124 male) aged 18–90 years (mean 46 ± 17 years). Mean height was 173 ± 9 cm and mean weight was 79 ± 15 kg. Right-hand dominance was reported by 200 subjects, while 18 were left-hand dominant (two subjects had missing values). Table 1 presents the distribution of the independent variables used in the multiple linear regression model and their correlation to the total rotation ROM during the FRT.
Procedure
After providing signed informed consent, participant characteristics were recorded including gender, hand-dominance, age, height, body weight, as well as smartphone and PC use, as all of these may potentially influence cervical ROM. Standardised pre-test screening was conducted to exclude subjects with vertebro-basilar insufficiency, spinal cord compromise or upper cervical instability. We used a short self report questionnaire to rule out neck pain, headache and jaw pain. In addition, the examiner asked supplementary questions and performed active movements of the cervical spine. If symptoms occurred, patients were excluded.
Outcome measures
Cervical spine ROM was evaluated by a digital goniometer (EasyAngle, Meloq AB, Stockholm, Sweden) placed on the head of the participant via an elastic band as shown in Figure 1. In a different study with symptomatic participants and a different set of raters it has been shown to be a valid and reliable measure of cervical ROM with an intra-class correlation coefficient (ICC)(3,1) for intra-rater reliability between 0.94 and 0.96 and ICC(2,1) for interrater-reliability of 0.66 [95% confidence interval (CI) 0.47–0.79, p < 0.001, SEM 6.6°]. 13 The construct validity of the digital goniometer is excellent with an ICC of 0.97 compared with an ultrasound based measurement system. 13
Active physiological cervical movements were evaluated in sitting, with ROM determined for flexion, extension, rotation to the left and right, and lateral flexion to the left and right. A single measurement was made of each movement.
The FRT was tested in supine (Figure 1). The therapist moved the subjects’ head and neck into maximum flexion and rotated the head to either side to the onset of pain or maximum range with firm resistance. ROM, pain and resistance were documented. The FRT was measured three times on each side and the mean value was calculated. The reported normal range of rotation during the FRT is 44° to each side and is positive if mobility is restricted by more than 10° or if symptoms occur during the procedure. 24

FRT with digital goniometer.
Data analysis
All data were analysed using STATA 15.1 (2015, StataCorp, College Station, TX). In all analyses, alpha levels were set at 0.05. Cervical ROM data was transformed into total ROM in the three cardinal planes to reduce the number of variables. Total movement in the sagittal plane was calculated by addition of active flexion and extension. Total rotation (movement in the transversal plane) and total lateral flexion (movement in the frontal plane) was by addition of active range to the left and right. For the FRT score, the total range was calculated by adding the range for left and right rotation. In addition, the ratio between total rotation ROM during the FRT and global cervical rotation ROM was calculated.
Pair-wise correlation coefficients between the range recorded for the FRT and the total range of cervical movement, age, height, body weight, smartphone use and PC use were calculated. We used the following descriptive terms for strength of correlation coefficients. 25
0.00–0.25 little, if any correlation
0.26–0.49 low correlation
0.50–0.69 moderate correlation
0.70–0.89 high correlation
0.90–1.00 very high correlation
A multiple linear regression model was used to predict total rotation mobility during the FRT. Variables were selected using the leaps-and-bounds algorithm. 26 The information criteria for the selection were Akaike’s (AIC), Bayesian information criterion (BIC) and adjusted R 2 . 27 Independent variables were total cervical rotation, lateral flexion, flexion and extension, smart phone use, PC use, gender, age and side-dominance.
In addition, to estimate the effect of age on the FRT and active cervical movements in all three planes simple linear regression models were fitted with cervical movements as dependent variables and age as the only predictor. Then we used multiple regression to test the influence from independent variables total cervical rotation, lateral flexion, flexion and extension, smart phone use, PC use, gender, age and side-dominance on the ratio between total rotation ROM during the FRT and global cervical rotation ROM.
All p-values and CI are Bonferroni adjusted for multiple testing. All assumptions for the use of multiple linear regression models were tested. 28
Ethical considerations
The study followed the principles of the Declaration of Helsinki. 29 Ethical approval was granted by the ethics committee of the University of Applied Science and Art (Hildesheim, Germany) dated 6 December 2017 (approval number= 6/12/2017).
Results
Research question 1: does age influence upper cervical mobility during the flexion rotation test?
Age (r = –0.53) showed a moderate negative correlation, total cervical ROM in flexion/extension (r = 0.512), total cervical rotation ROM (r = 0.60) and total cervical lateral flexion ROM (r = 0.48) showed a moderate positive correlation with range of rotation during the FRT (p < 0.0001). Smartphone use (r = 0.3264) showed a low correlation with the amount of rotation during the FRT (p < 0.0001) (Table 1). Table 2 presents the pairwise correlations between the metric independent variables. The correlation between age and total cervical ROM as well as correlations between the total cervical movements were moderate to high. Correlations between smart phone use and age were also moderate. The correlation between smart phone use and different directions of cervical ROM were low. All other correlations were low or very low or not significant.
Characteristics of the variables and their correlation with the total range of motion during the FRT (n = 220).

Point biserial correlation.
FRT, flexion-rotation test; SDE, standard deviation.
Correlation matrix independent variables.

p ⩽ 0.05, **p < 0.01, ***p < 0.001.
Not significant, all Pearson’s correlations.
Point biserial correlations.
Tretrachoric correlations.
Based on the values of AIC, BIC and adjusted R 2 , the multiple linear regression model best explaining the variance of the total rotation during the FRT included total cervical rotation and age as predictors. Both independent variables explained 41% (R 2 = 0.406) of the variance in the FRT, which is highly significant [F(3,216) = 49.3, p < 0.0000]. The amount of rotation during the FRT showed a negative correlation with age.
The simple linear regression model with FRT as dependent variable showed that the age of the participants explained 27.91% of the variance in upper cervical rotation. The 95% CI for this estimate ranged from 18% to 37%. Figure 2 visualizes the effect of age on cervical ROM. With increasing age, upper cervical rotation decreased by 0.55° (95% CI 0.44°−0.68°) per year.

Estimated influence of age on the FRT, and active total cervical movement in all planes based on four simple linear regression models (steps of 2 years).
Table 3 shows the predicted values for different ages in steps of 10 years. For FRT to the left the differences for a decade was −2.6° (95% CI: −3.5 to −1.6, p < 0.0001), and −2.9° (95% CI: −3.9 to −1.9, p < 0.0001) for FRT to the right and −5.6° (95% CI: −7.4 to −3.7, p < 0.0001) for FRT total respectively.
Predicted ROM values of upper cervical rotation and 95% confidence intervals during FRT (n = 220).
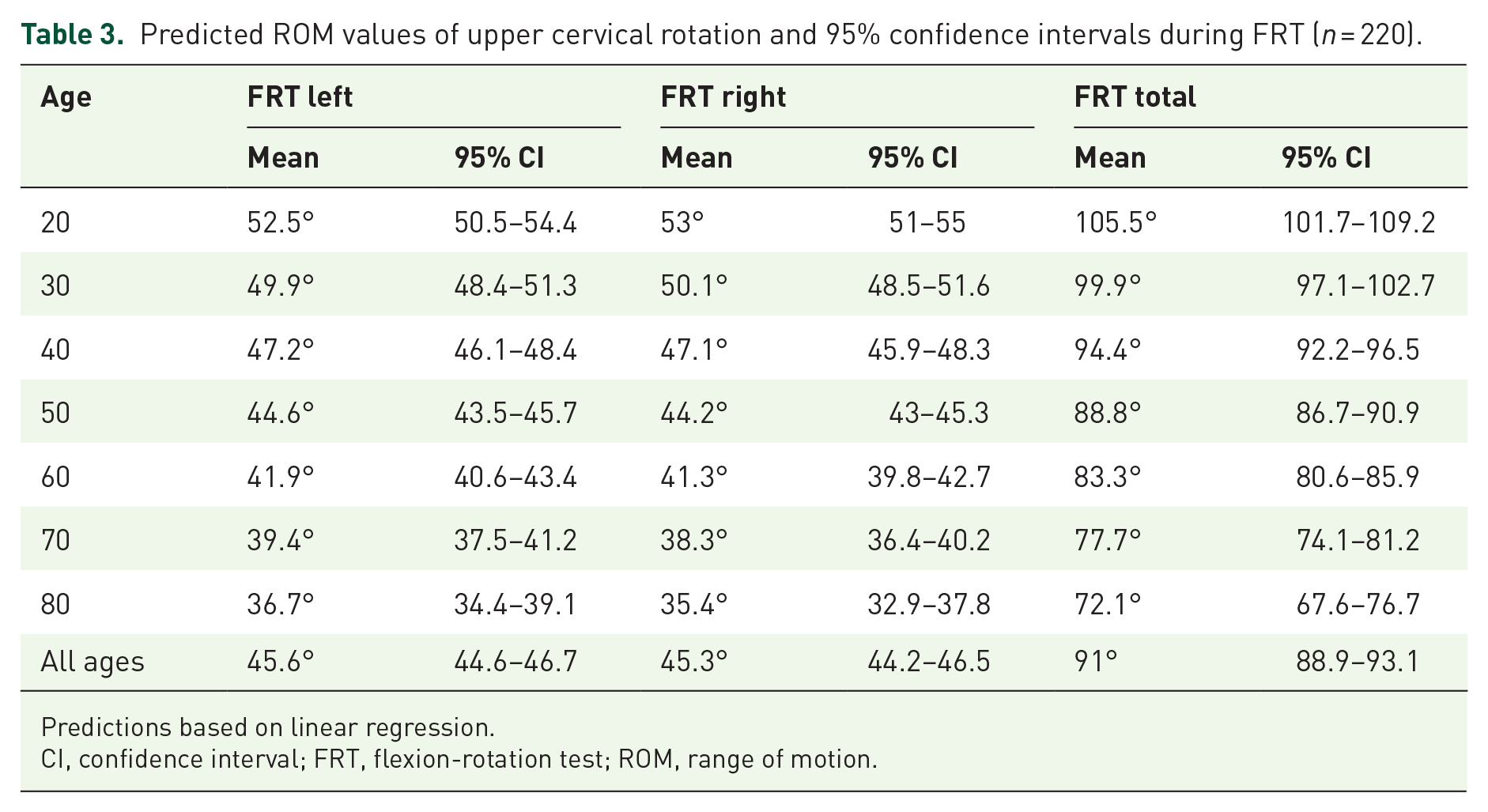
Predictions based on linear regression.
CI, confidence interval; FRT, flexion-rotation test; ROM, range of motion.
Research question 2: does age influence the ratio between lower and upper cervical rotation mobility?
The mean ratio between total rotation ROM in the FRT and total cervical rotation ROM was 0.59. Although movement during the FRT is not completely isolated to the upper cervical spine, this result indicates that a substantial proportion of total cervical rotation ROM take place in the upper cervical segments. This ratio is not affected by age (F1,218 = 0.26, p = 0.609, R 2 = 0.0012), or any other measured variable.
Discussion
The results of this study show for the first time that the amount of upper cervical rotation during the FRT decreases with age. One important finding is that approximately 60% of the total cervical rotation takes place at C1/2 regardless of age. This helps to estimate the expected amount of upper cervical rotation in subjects at any age.
In contrast to the present study’s findings, Smith et al. reported that mobility determined by the FRT was not influenced by age. 19 The disparity in findings can be explained by the characteristics of the sample recruited by Smith et al. Only 38 out of 66 assessed participants were asymptomatic and subclinical pain was the strongest predictor for ROM recorded during FRT in that study. The age structure of the asymptomatic participants was not reported, although the mean age was 33 years and thereby much younger than in the current study’s sample and likely prior to any significant morphological changes. The age of these subjects and the symptomatic nature of their presentation of subclinical pain limits the comparison between the sample in Smiths et al.’s study and the present sample.
Dvorak et al. included 150 asymptomatic subjects with a mean age of 40.5 years (Range 21–71 years) that showed a slight increase in ROM recorded during the FRT with increasing age, although all other cervical spine movements decreased with age. 20 The authors explained this finding by a compensatory mechanism of the upper cervical spine as a result of rotatory dysfunction of the lower cervical segments. However, the study by Dvorak et al. used a different test procedure and showed a skewed age and sex distribution. 20 According to Debernardi et al. and Dvorak and Panjabi, mobility of the C1/2 motion segment is mainly limited by ligaments.30,31 From a biomechanical point of view, decreased upper cervical rotation during the FRT with increasing age may be explained by degenerative changes occurring in upper cervical ligaments. However, the influence of age on the composition of these ligaments has not yet been investigated. The body of evidence on articular degeneration of C1/2 joint is more extensive. Several studies showed an increased prevalence of osteoarthritis at the atlantoaxial joint associated with age.21,22 An increased incidence was especially shown in the medial atlantoaxial joint. 32 Prescher, and Skaane and Klott describe the typical picture of a ‘peridental aureole’ as a local and frequently occurring feature of anterior atlantodental arthritis.33,34 Furthermore, studies show a decrease in the linear atlantodental interval with increasing age.23,35 From a biomechanical point of view, the results of the above cited studies support the findings of the present study. Further research is required to determine whether changes to other structures or other theories may explain the decrease in FRT mobility with age.
Our results indicate that active mobility of the cervical spine decreases by about 0.4–0.7 degrees per year. This is consistent with other studies showing a reduction of cervical mobility of 4–7 degrees per decade, as well as 0.5 degrees per year.36,37
Studies by Anderst et al. and Penning have shown that approximately 50% of total cervical spine rotation occurs at C1/2.5,6 In the present study, range recorded during the FRT corresponds to an average of 59.5% of the total rotation of the cervical spine, resulting in a ratio of 60:40 reflecting upper to lower cervical spine mobility. This is of clinical importance, as it allows the age-independent differentiation of upper versus lower cervical spine movement restriction. It should also be recognised that the FRT is performed passively, while general cervical ROM testing was assessed actively.
The present study showed no effect of sex on the range recorded during the FRT. Dvorak et al., in contrast, found significantly higher cervical spine mobility in rotation during maximum flexion for women in the age groups 30–39 years (+8.6°) and 40–49 years (+13.7°). 20 It is unclear why such differences occurred.
Some limitations of the present study need to be taken into account. To limit the duration of the testing procedure and reduce strain for the patients, we took only one measurement to estimate active global cervical ROM. This may have potentially affected the results for global cervical ROM; however, values for ROM in our sample correspond to those previously reported in the literature.20,38,39
Another limitation of our study is that the ICC for inter-rater reliability of the digital goniometer in measuring upper cervical ROM was 0.66, 13 which is below the ICC value of 0.70 typically considered as acceptable. 40 This could have affected the validity of our measurements, as four different raters took the measurements. However, the ICC is sample dependent. Inter-rater reliability of measurements was examined with a different set of raters in a more homogeneous group of patients in regards to upper cervical ROM. The SD of ROM for upper cervical rotation was 11.61 for rater 1 and 11.10 for rater 2 in the reliability study, compared with 18.52 in our study. In a more homogeneous sample, it is harder to distinguish between patients and this negatively affects the reliability parameter. 40 The greater homogeneity in the reliability sample may therefore have deflated ICC values. This might affect the direct transferability of the reported inter-rater reliability data to our sample.
In conclusion, analysis of data obtained from the FRT must always be interpreted with respect to the age of the tested person and should also always be considered in relation to the total mobility of the cervical spine in rotation. The greater the age, the smaller the expected ROM during the FRT. Thus, decreased ROM becomes more pronounced with every decade. The range recorded during the FRT corresponds to 60% of the total mobility of the cervical spine in rotation. This ratio remains stable in all age groups. It can therefore be assumed that the proportion of upper cervical spine rotation for the total amount of cervical rotation does not change. This allows reliable diagnostic statements about the origin of cervical hypomobility in rotation.