
Abstract
Axial spondyloarthritis (axSpA) is a group of debilitating, chronic, rheumatic conditions characterized by inflammation and new bone formation, mainly involving the spine and the sacroiliac joints. The lack of biomarkers in axSpA is well known. Despite significant treatment advances in recent years thanks to the introduction of drugs with a new mode of action, such as new biologic and targeted synthetic disease-modifying antirheumatic drugs, no relevant improvement in the identification of disease biomarkers has been achieved. Common parameters, such as erythrocyte sedimentation rate and C-reactive protein, which are routinely used to measure systemic inflammation, are the sole markers available to date and are not adequate to assess disease activity in all patients.
The aim of this study is to review the most promising serum biomarkers that may help treatment decision in axSpA via a proper assessment of disease activity and identification of negative prognostic factors.
Keywords
Introduction
Spondyloarthritis (SpA) is a group of chronic, inflammatory, rheumatic diseases characterized by overlapping clinical signs and symptoms and a common genetic background. 1 Depending on the predominant pattern of clinical symptoms, a primary peripheral or axial involvement can be distinguished.1,2 Axial spondyloarthritis (axSpA), which mainly affects the spine and the sacroiliac joints (SIJs) and with a symptom onset usually before the age of 45 years, can be further divided into nonradiographic axSpA (nr-axSpA) and radiographic axSpA, the latter also known as ankylosing spondylitis (AS). 2 If undiagnosed and untreated, long-term outcomes of axSpA are physical and functional permanent damage as well as lifelong disability.2,3 Importantly, patients with early disease also experience fatigue and functional impairment with subsequent depression. 4 Reduced social life and working ability result in a poor quality of life with consequent increase in the economic burden of the disease. 5
Significant steps forward have been taken in the management of axSpA in clinical practice, following the introduction of tumor necrosis factor (TNF)-α inhibitors (TNFi). Patients with axSpA respond quickly to TNFi, which provide an Assessment of Spondyloarthritis International Society response criteria (ASAS40) improvement in about 40% of patients in the first 3–6 months of treatment. Similar response rates have also been observed following treatment with biologic disease-modifying antirheumatic drugs (bDMARDs) targeting interleukin (IL)-17.6,7 The role of other bDMARDs targeting IL-12/IL-238,9 needs further evaluation in axSpA. Furthermore, the targeted synthetic DMARDs (tsDMARDs), which inhibit intracellular signaling molecules such as the Janus kinases (JAK) showed some preliminary promising results and may be approved in a short time in axSpA treatment.10,11 The introduction of these new targeted treatments allowed a better understanding of the pathogenesis of axSpA, but such improvements were not paralleled by the discovery of new biomarkers. Because of the absence of rheumatoid factor, axSpA has been long considered to have a seronegative property. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), routinely used inflammatory indices, in addition to human leucocyte antigen (HLA) B27, had been considered until now to be the main diagnostic and therapeutic biomarkers in axSpA. ESR and CRP levels are often within the normal range even in the case of very active disease, and are not adequate to monitor all axSpA patients.12–15 As a result of the growing awareness of the impact of chronic back pain in axSpA patients and of new breakthroughs on etiopathogenetic mechanisms and in the field of genetics thanks to genome-wide association studies, recent studies have investigated novel potential biomarkers of disease activity to identify patients at higher risk for a worse outcome.16–20 The National Institute of Health Biomarkers and Surrogate Endpoint Working Group have elaborated the definition of biomarker as a “characteristic that can be objectively measured and evaluated as an indicator of normal biological or pathogenic processes or pharmacological responses to a therapeutic intervention”. 21 However, clinical characteristics and comorbidities are also important biomarkers toward the definition and diagnosis of axSpA. The Italian board for the TAilored BIOlogic therapy (ITABIO) group attempted to develop an algorithm to guide first- and second-line biological treatments that mainly relies on clinical features of the disease.22,23 Likewise, the American College of Rheumatology recommendations for spondyloarthritides also take into account comorbidities to select the preferable treatment options. 24 In this regard, rheumatologists have to take into account concomitant cardiovascular disease and metabolic syndrome, the desire of a pregnancy, the risk of infections, and importantly the patients’ preference. Furthermore, concomitant skin psoriasis, uveitis and inflammatory bowel disease (IBD) may be used to characterize the disease in SpA. Along with these factors, other characteristics may help to profile the patient with axSpA and to personalize the treatment. Male sex, 25 smoking,26,27 presence of syndesmophytes 28 and active inflammatory or post-inflammatory modifications on MRI 29 are known predictors of a more severe disease with higher Ankylosing Spondylitis Disease Activity Score (ASDAS) or Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and with a radiographic progression.
A large number of biomarkers have been investigated and suggested in axSpA and variable evidence is available on their role in the diagnosis, clinical and prognostic assessment and evaluation of the response to treatment.
The purpose of our review was to summarize the available biomarkers in axSpA towards a more tailored therapeutic approach. Specifically, we focused on markers associated with disease activity and treatment response (clinical and radiological). We performed a PubMed search of articles published between 1984 and 2019. The search terms included: axial spondyloarthritis, ankylosing spondylitis, biomarkers, serological markers, antibodies, immunogenicity. Biomarkers are presented according to five main categories: (1) systemic markers of inflammation; (2) molecules implicated in the bone homeostasis; (3) miscellaneous; (4) anti-drug antibodies (ADAbs) and drug through levels; and (5) combination of biomarkers. A schematic summary of their potential use in axSpA is reported in Table 1.
A schematic summary of the potential use in the clinical practice of selected promising biomarkers in axial spondyloarthritis.
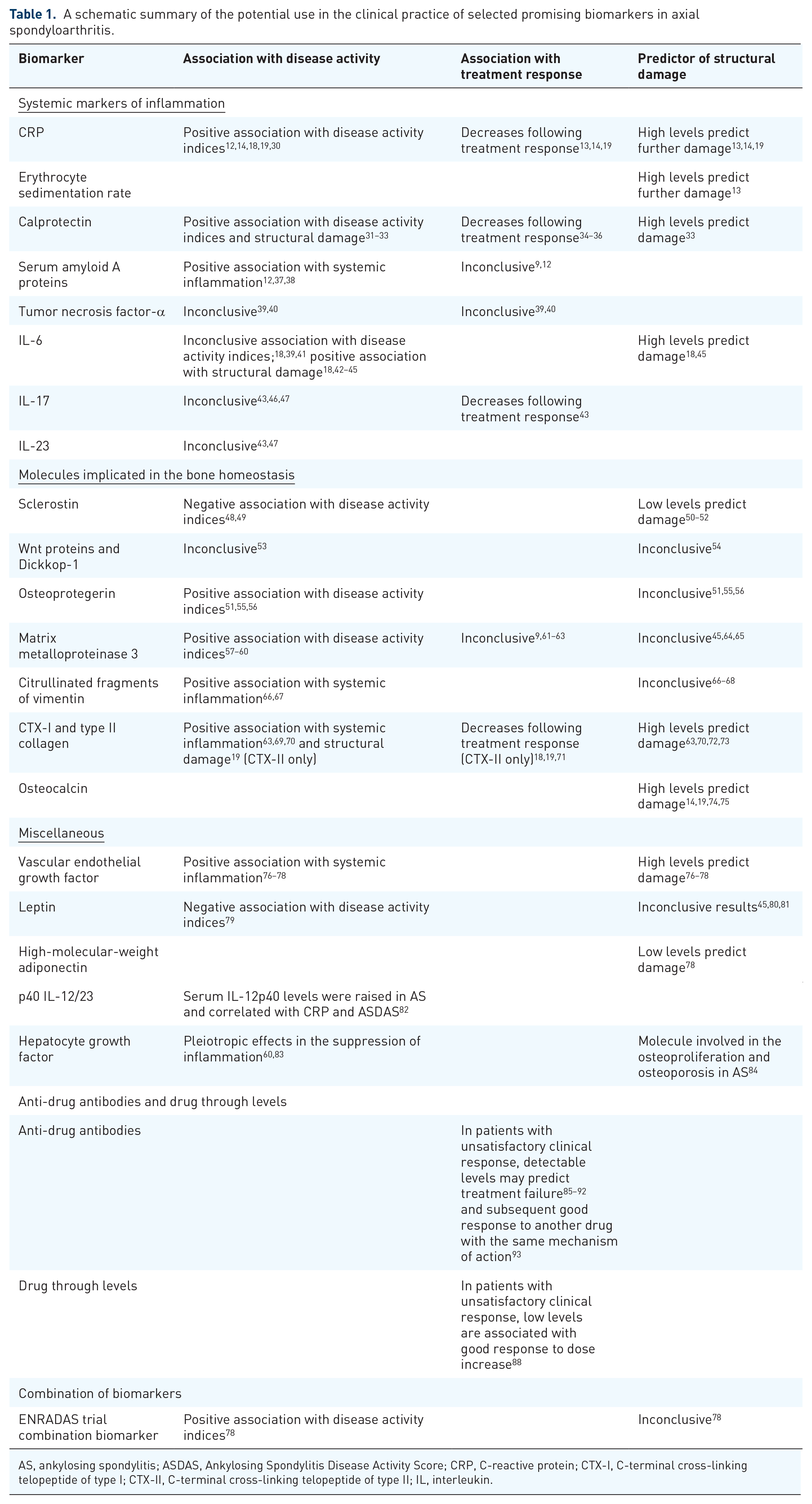
AS, ankylosing spondylitis; ASDAS, Ankylosing Spondylitis Disease Activity Score; CRP, C-reactive protein; CTX-I, C-terminal cross-linking telopeptide of type I; CTX-II, C-terminal cross-linking telopeptide of type II; IL, interleukin.
Systemic markers of inflammation
CRP and ESR, are acute-phase proteins used in clinical practice as markers of systemic inflammation. 94 Unfortunately, they may not fully represent the inflammatory process in axSpA due to their low sensitivity and specificity. 95 An elevated CRP is one of the items included in the classification criteria of the ASAS for axSpA. 2 CRP levels are also taken into consideration in the ASDAS and they were shown to correlate with the BASDAI. 96 However, elevated CRP or ESR levels are detected in only 40–50% of patients with AS. 97 In fact, the degree of inflammation fluctuates during the course of axSpA. In general, CRP levels are higher in patients with radiographic axSpA compared with nr-axSpA. 30 Although CRP is within the normal range in a large proportion of patients with active axSpA, it is still widely considered a reliable marker of disease activity. In fact, CRP levels are moderately correlated with magnetic resonance imaging (MRI) inflammation.14,18,19,30 In addition, CRP has been found to be a reliable biomarker for monitoring treatment response and predicting further radiographic progression.30,98 Several studies have shown that CRP levels drop significantly during TNFi treatment.13–15 Modifications in CRP levels correlate with changes in BASDAI and MRI scores. Elevated baseline CRP levels are associated with a good treatment response12,14 and represent a strong positive predictor of radiographic sacroiliitis progression, especially for nr-axSpA into AS. 14 Several prospective studies have also demonstrated that elevated CRP levels are independently associated with radiographic spinal progression in axSpA patients. 98 The ESR seems to be a nonspecific measure of inflammation that may be influenced by a variety of other nonrheumatic conditions and comorbidities. However, some studies reported that high ESR levels and increased CRP levels are independently associated with structural disease progression in patients with nr-axSpA. 13
Besides the two most common inflammation markers, calprotectin (CPT) is a promising marker of inflammation that has recently gained interest in several inflammatory rheumatic diseases. CPT is a heterodimeric calcium- and zinc-binding protein complex, composed of S100A8 and S100A9 subunits, expressed in the cytosol of keratinocytes, neutrophils and monocytes. This protein exerts diverse intra- and extracellular functions, acting on different target tissues/organs, such as muscle, cartilage, bone, synovial tissue, vessels and epithelium, among others. Modulation of the inflammatory response by binding to different cell-surface proteins such as Toll-like receptor, as well as oxidant-scavenging, antimicrobial and apoptosis-inducing activities are among the extracellular functions attributed to CPT. 99 Interestingly, both pro- and anti-inflammatory roles have been reported for CPT.50,100 Additionally, previous studies showed that CPT is a sensitive and specific biomarker of local inflammation, mirroring intestinal or synovial inflammation. Fecal CPT levels have been associated with disease activity in AS and are associated with inflammatory activity in the bowel.101–103 Serum CPT levels can be used as a marker of inflammation in nr-axSpA, AS and reactive arthritis without significant difference in the levels between these diseases. Some authors reported that elevated CPT levels positively correlated with ESR, CRP, BASDAI, and ASDAS as well as Spondyloarthritis Research Consortium of Canada (SPARCC) scoring.31,32 CPT might also be used to monitor treatment response. Serum levels of CPT were reported to decrease following treatment with TNFi.34,35 S100A8 and S100A9 subunits were reduced after 6 weeks of IL-17 inhibition with secukinumab and correlated with ASAS response. 36 A significant decrease in serum CPT was noted also after intensive physiotherapy in patients with nr-axSpA and AS. 104 Serum CPT has a potential role as a prognostic factor, being associated with radiographic spinal progression. 33 Baseline CPT serum levels have been found significantly increased in patients with a higher modified Stoke Ankylosing Spondylitis Spinal Scores (mSASSS) versus those without. 33 A few studies reported an association of CPT with adverse lipid profiles, in addition to the known association with classical inflammatory biomarkers, which strengthens the association between inflammation and development of atherosclerosis and may help to identify patients with axSpA at high risk of cardiovascular events.55,105–107
Serum amyloid A (SAA) protein was also suggested to help in disease monitoring although it is less reliable compared with CPT. SAA is a family of apolipoproteins associated with high-density lipoproteins that are produced in response to an inflammatory trigger. Patients with AS have higher serum SAA levels with respect to healthy controls; SAA levels also correlated with inflammatory markers and disease activity variables.12,37,38 Similarly to CRP, baseline high SAA levels were shown to be associated with higher odds of treatment response to TNFi, especially in patients with elevated CRP. 12 SAA levels were decreased following treatment with ustekinumab, and anti-IL-12/23, in patients with AS; however, no correlation with clinical response was observed. 9
Cytokines are key mediators in the pathogenesis of rheumatic diseases. However, their role as biomarkers are widely debated. TNF-α has long been the only cytokine known to be involved in the pathogenesis of axSpA, leading to the development of therapeutic antibodies targeting this cytokine. Notably, TNF-α provides a potential link between inflammatory response and disturbed bone homeostasis, 39 exerting several effector and biological functions via proinflammatory cytokines and chemokine release, the activation of endothelial cells with upregulation of adhesive molecules, leucocyte accumulation, angiogenesis, lymphocyte activation, fibroblast proliferation and chondrocyte and osteoclast activation. TNF-α expression is strongly upregulated in SIJ biopsies of patients with AS 40 and serum levels are significantly higher in patients with AS compared with subjects with noninflammatory back pain or healthy controls.39,108 In addition to the interesting findings that support TNF-α involvement in the disease, the serum levels did not prove to be reliable biomarkers of disease activity.
IL-6, similarly to TNF-α, is one of the most extensively studied cytokine in rheumatic diseases, especially in rheumatoid arthritis (RA), but it has also been evaluated in axSpA. IL-6 is produced by a variety of immune cells that further induce the production of several acute-phase proteins. 39 IL-6 is involved in the very early stage of the inflammation process by inducing the gathering of neutrophils at the inflammation site and modulating T-cell activation and differentiation. Elevated IL-6 levels were also found to be expressed in cartilage, synovial fluid and connective tissue in SIJ biopsies of patients with AS, particularly in early stages. 109 Higher IL-6 serum levels are usually found in patients with AS compared with healthy controls.39,110,111 An association between IL-6 serum levels and activity indices or inflammatory markers was demonstrated by some authors,39,41–43 but was not confirmed by others.18,44 Particularly, IL-6 does not seem to be associated with other emerging cytokines in the pathogenesis of axSpA, that is, IL-17 and IL-23. 112 Notably, IL-6 is associated with MRI changes. Lower baseline levels were found to be associated with lower MRI inflammation scores following TNFi treatment.18,45 Interestingly, the change of IL-6 levels from baseline to week 4 and week 14 was associated with spinal inflammation in MRI. IL-6 appears to have a potential prognostic role, as high baseline levels were predictive of a high probability of structural response to TNFi as assessed with mSASSS. 45
Following the introduction of biologics with new modes of action, the interest moved to other cytokines, namely IL-17 and IL-23, which are the targets of these drugs. Both of them are involved in the helper T cell type 17 (TH17) pathway and are often tested together due to their tight connection. In fact, IL-17 is mainly produced by TH17 following IL-23 production. The IL-23–IL-17 immune axis is implicated in the pathogenesis of axSpA,9,80,113–115 particularly at the entheseal level.116–118 Most studies reported elevated IL-17 and IL-23 levels in the plasma and serum of patients with AS.9,46,47,69,110,116,119 The association with clinical variables is not consistently reported in all studies. IL-17 and peripheral TH17 cells are reported to be reduced following successful TNFi treatment 43 and IL-17 correlates with CRP and disease activity indices, such as BASDAI.43,46 Other authors failed to find correlation between IL-17 levels and inflammatory indices, disease activity or MRI changes.46,47 Very similar findings have been found for IL-23 in the same studies.43,46 Chen et al., showed that IL-17 and IL-23 performed even better compared to ESR and CRP in discriminating patients with disease activity, assessed by BASDAI. 46
In addition to the above discussed cytokines, IL-21 and IL-22, both linked to IL-17 and TH17 cells, are elevated in patients with AS.46,120–122 IL-22 was strongly associated with IL-23 in one study, but no associations with clinical, serological and imaging variables were found. 119 IL-31 emerged as the only cytokine to be higher in patients with SpA compared with controls in a French cohort, and it was associated with less structural damage. 112 IL-33, a member of the IL-1 family, was found to be elevated in the serum of patients with AS in China and to correlate with disease activity or other inflammatory markers.123–125
Molecules involved in bone homeostasis
Molecules mirroring bone metabolism that can be detected in the serum represent an opportunity to better understand and monitor axSpA. Molecules driving bone resorption and formation and enzymes degrading extracellular matrix are among the best studied. Components of the extracellular matrix and its degradation products have been extensively studied in the field of osteoporosis and associations between their serum levels with axSpA disease activity have also been investigated.
The human receptor activator of nuclear factor-κB ligand (RANKL) and monocyte colony-stimulating factor (M-CSF) are the two key molecules involved in osteoclast formation from peripheral blood monocytes and in osteoclast activation 126 and are the best studied. These cytokines play a critical role in physiological bone turnover and their dysregulation leads to impairment of osteoclast generation and excessive bone formation, as observed in several rheumatic diseases, including SpA. However, there is substantial discrepancy regarding serum RANKL levels in patients with SpA (especially axSpA). Some studies reported either higher or lower serum RANKL levels in patients with axSpA in comparison to healthy subjects.48,51,127,128
Sclerostin (SOST) is a bone morphogenic protein antagonist. SOST, being an antagonist of the Wnt/β-catenin pathway, exerts anti-anabolic effects on bone formation and a reduced biological effect of SOST seems responsible for the bone neo-ossification that is typical of AS. 129 Nonetheless, studies focusing on SOST levels in patients with AS gave diverging results. Most of the studies found lower levels in individuals with AS compared with controls,50,56,64 and an association with disease activity was found.49,51 Some studies also suggested a prognostic value, as low baseline SOST levels in AS and axSpA were associated with new syndesmophyte formation.50–52 Interestingly, anti-SOST antibodies were found together with low SOST levels, thereby implying a possible pathogenic role of the antibodies neutralizing SOST.130,131
The Dickkopf (Dkk) proteins are one of the two main families of soluble inhibitors of the Wnt proteins, and include the most important protein, Dkk-1. The activation of Wnt signaling induces osteoblastogenesis and is implicated in new bone formation. As Dkk-1 is an inhibitor of the Wnt pathway, one might expect Dkk-1 concentrations to be low in the diseases characterized by an increase of new bone formation. Nevertheless, only a few studies found lower Dkk-1 levels in patients with AS.74,132 Furthermore, consistently with most other studies, Dkk-1 concentrations were higher in patients with AS compared with healthy subjects,54,55,133,134 similarly in patients with peripheral SpA compared with healthy controls; and higher in patients with AS compared with psoriatic arthritis (PsA). 133 Thus, it has been suggested that Dkk-1 serum levels may be higher in axial disease because of a pathologically dysfunctional Dkk-1 molecule, which does not inhibit Wnt-mediated osteoproliferation in axSpA. In fact, possible explanations are provided by the observation that Dkk-1at high levels binds to its receptor LRP6 with low avidity in AS,54,133 and that Dkk-1 even has a stimulatory effect on the Wnt pathway in the presence of anti-Dkk-1 monoclonal antibodies. 133 Dkk-1 is not correlated with CRP level, 53 and TNFi treatment does not affect Dkk-1 levels. 54 The latter observation may be unexpected because recent data showed a retardation of radiographic progression under TNFi in different patient groups (e.g. with treatment initiation within the first 10 years after symptoms, 135 after long-term treatment 136 or in the case of a good treatment response 137 ).
Osteoprotegerin (OPG), a member of the TNF receptor superfamily, inhibits the RANK–RANKL interaction, impeding osteoclastogenesis with anti-resorptive effects. Several studies found OPG levels higher in patients with AS compared with controls,8,55,127,138 whereas others found the opposite.51,56 OPG seems to correlate with BASDAI score, being higher in patients with more active disease, but not with TNFi treatment response.51,55,56
Matrix metalloproteinases (MMPs) are relevant enzymes involved in the degradation of extracellular matrix proteins. These zinc-dependent endopeptidases also play a role in cell proliferation, migration, differentiation, angiogenesis, apoptosis and host defence.139–141 MMP-3 is the most studied among these molecules in axSpA. MMP-3 serum levels are increased in patients with AS with respect to healthy controls.139–141 Furthermore, some investigators have reported that MMP-3 correlated with ESR and CRP levels, disease activity and functional status, as assessed by the BASDAI. 142 Similar findings have been also found in PsA, further confirming the potential role of this molecule as a biomarker.57–59 TNFi induce a significant and rapid decrease in serum MMP-3 levels together with a reduction in conventional variables (ESR and BASDAI).61–63 A similar effect was observed after treatment with ustekinumab, although MMP-3 decrease was not associated with clinical variables. 9 MMP-3 association with structural damage has been reported.64,143 Maksymowych et al. showed that MMP-3 was a significant independent predictor of radiographic progression over a 2-year observation period in axSpA, 143 suggesting that MMP-3 could be considered a parameter of bone metabolism. Other studies did not confirm the association of MMP-3 with inflammation in the SIJs detected by MRI, 144 with radiographic progression.45,65 Although fewer studies have been carried out on other MMPs, MMP-8 and MMP-9 (but not MMP-3) were found to be associated with disease activity, as assessed by the BASDAI score. 60
Cathepsin K is a potent collagenase predominantly expressed in osteoclasts and is involved in bone remodeling and resorption. Cathepsin K expression follows the signal of inflammatory cytokines released after tissue injury. Reports of cathepsin K levels in AS are controversial; this molecule seems to be expressed at a higher level by mononuclear cells, fibroblast-like cells, and other cells attached to bone but cathepsin K serum levels were not different compared with healthy controls and no significant modification following TNFi was observed.145,146
The cartilage oligomeric matrix (COMP) protein catalyzes the assembly of collagen in the extracellular matrix. Elevated COMP levels were observed in a variety of inflammatory joint diseases; 18 however, its association with other clinical and disease activity markers in AS have been inconsistently reported. Nevertheless, one study reported an inverse relationship between COMP levels and MRI inflammation in patients with axSpA. 19 Bone-specific alkaline phosphatase (BAP) is a marker of active bone formation. High levels of BAP have been found in patients with axSpA and are associated with disease activity.53,64
Recently, extracellular matrix turnover products have gained interest as possible biomarkers in SpA. Citrullinated fragments of vimentin (VICM) are MMP-degraded fragments modified by citrullination, a process occurring unspecifically during the inflammatory phase. VICM was found to be higher in patients with AS compared with controls and to be associated with high CRP serum levels.66,67 VICM levels, together with high baseline mSASSS values, were found to be predictors of radiographic progression. 66 However, other researchers did not confirm this finding.67,68 Furthermore, indirect biomarkers of VICM, anti-citrullinated vimentin antibodies, are higher in SpA, including individuals with AS versus controls and appeared to show promising molecules associated with radiographic damage and correlated with CRP. 65
Other products of collagen degradation are fragments of type I (C1M), II (C2M), IV (C4M), V (C5M), and VI (C6M) collagens generated by MMP. Their high levels in AS, compared with controls, supports their association with tissue remodeling during active disease.66,147,148 C1M and C6M are also correlated with CRP.65,66 C1M was associated with mSASSS progression in one study; however, the association was not confirmed after adjustment for confounders. 67 A combination of C2M, C3M and C6M was found to be a marker of structural progression as it correlated with mSASSS. 66 More recently C1M, C5M and C6M showed no relationship with mSASSS progression. 68
An MMP-mediated metabolite of CRP (CRPM) was found to have higher levels in AS compared with nr-axSpA and was associated with some disease activity indices, such as CRP and ASDAS-CRP. 65
Type I and type II collagen are proteins of cartilage and components of connective tissue. Studies have evaluated both serum and urinary type I and II C-terminal telopeptides (CTX-I and CTX-II). CTX-I is a marker of osteoclast activity reflecting bone degradation. 149 Both urinary and serum CTX-I levels are higher in patients with AS compared with healthy controls.72,150 CTX-II levels were shown to correlate with MRI inflammation scores in SIJs and/or lumbar spine in patients with axSpA . 19 CTX-II serum levels were also correlated with serological markers of disease activity,63,70,72 and they decreased after treatment with TNFi.18,19,71 CTX-II seems to be a biomarker of radiographic progression in axSpA. In multivariate analyses with a 2-year change in mSASSS, 70 CTX-II seems to significantly and independently contribute to explaining variation in radiological damage and progression and the association remained after the adjustment for markers of inflammation (which also correlated with CTX-II). This observation suggests that cartilage degradation might be related to the process of syndesmophyte formation. Notably, CTX-II and CTX-I may serve as prognostic markers to identify patients prone to radiographic spinal progression with a more robust evidence for CTX-II.63,70,72,73
Osteocalcin is a small molecule of the mineralized bone matrix. Previous studies have shown that osteocalcin serum levels in AS are lower than in controls; 151 however, recent studies have reported high serum levels in AS, associated with radiographic progression, especially for the development of new syndesmophytes.14,19,74,75 Osteocalcin was also found to increase early following TNFi treatment, 19 which is intriguing because recent data showed a retardation of radiographic progression under TNFi.
Serum human cartilage glycoprotein-39 (YKL-40), a secretory protein of human articular chondrocytes and synoviocytes, is a marker of cartilage remodeling and is associated with disease activity in AS. 18 YKL-40 serum levels are significantly higher in patients with SpA with respect to healthy controls but YKL-40 does not seem to perform as well as other inflammatory biomarkers, such as CRP and MMP-3, in the disease assessment. 111 Aggrecan is the central component of cartilage extracellular matrix. The replacement of the glycosaminoglycan side chain with aggrecan with charge density modification determines osmotic processes, which are fundamental for the biomechanical properties of cartilage. Patients with AxSpA have been found to have decreased levels of total aggrecan compared with healthy subjects and aggrecan seems to increase following TNFi treatment. 18
Miscellaneous
Vascular endothelial growth factor (VEGF) is a driver of angiogenesis and seems to be implicated in the initial phase of bone remodeling, which is characterized by inflammation and leads to bone formation. VEGF serum levels were reported to be higher in patients with AS and axSpA than in controls.18,70,76,77,123 High VEGF serum levels are associated with active disease and worse radiographic progression according to mSASSS.59,76–78
The fetuin family encompasses a series of proteins that have been implicated in numerous biological functions. Particularly, fetuin proteins seem to play a role in inflammatory processes and are implicated in bone remodeling, osteogenesis and bone resorption. 152 Fetuin-A was found to be higher in patients with AS with syndesmophytes compared with patients with AS without syndesmophytes or controls. 153
Adipokines are cytokines secreted by adipose tissue, which also have a role in mediating immune responses and regulating bone mass. Leptin, visfatin and high-molecular-weight adiponectin (HMW-ADN) are those mostly investigated in axSpA; however, inconsistent results have been reported. Leptin serum levels in AS have been reported to be either higher154,155 or lower compared with controls.78,81 A negative association of leptin with BASMI 79 has been found and with radiographic progression independently of CRP and baseline structural damage,80,81 but other authors did not confirm this association. 45 HMW-ADN serum levels were also found to be reduced in AS compared with controls and they were associated with syndesmophyte formation. 78 Visfatin is reported to be increased compared with controls and seems to be associated with radiographic spinal progression, like resistin. 156
Cytotoxic T lymphocyte-associated molecule (CTLA-4) is an inhibitor of immune response. CTLA-4 serum levels were lower in healthy controls compared with patients with axSpA, where they were correlated with CRP and BASDAI. 157
Recently, anti-CD74 antibodies (or anti-CLIP antibodies) directed against CD74, a class II-associated invariant chain peptide, were found in patients with axSpA. 158 Binding of CLIP antibodies to CD74 may lead to activation of cells and production of proinflammatory cytokines such as TNF-α. Baraliakos et al. 159 found anti-CLIP antibodies are mostly present in patients with early axSpA compared with controls, but the frequency of such antibodies decreases overtime 158 and further studies did not confirm a significant diagnostic value in patients suffering with inflammatory low back pain. 160
Some researchers considered the possible role of p40 subunit, common to IL-12 and IL-23, as a biomarker of disease activity, as higher levels of synovial p40 IL12/23 were found higher in 27 patients with SpA versus patients with osteoarthritis and versus paired serum SpA levels. 161 Ivanova et al. reported that serum IL-12 and IL-23p40 were raised among patients with AS and correlated with CRP and ASDAS; 82 however, the findings warrant further confirmation in larger cohort studies.
Two reports have also recently described the hepatocyte growth factor (HGF) as a promising biomarker.60,83 HGF is secreted by mesenchymal cells and has pleiotropic effects, including suppression of inflammation and enhanced osteoblastic differentiation of mesenchymal cells. HGF appears to be involved in the osteoproliferation and osteoporosis in AS. 84 Consistent associations between HGF and parameters of bone remodeling and lesions on imaging, especially on MRI, have yet to emerge.
Anti-drug antibodies and drug through levels
Immunogenicity has been implicated as a cause of treatment failure of bDMARDs, as all biological drugs have immunogenic potential85,162,163 and may induce formation of ADAbs. ADAb development is well known in RA and IBD, and it is described in all patients treated with monoclonal antibodies. 164 ADAbs are associated with reduced effectiveness of treatments and adverse events and correlated negatively with drug serum levels. 165 A considerable proportion of patients with axSpA treated with TNFi fail to respond ab initio (primary failure), or lose response over time despite an initial good response (secondary failure).164,166 Some patients may also discontinue TNFi treatment due to significant adverse events.86,167 ADAbs reduce drug blood levels by neutralizing the binding sites of the target molecules, or by forming immune complexes with the biological drugs and enhancing their clearance.168–171 ADAbs are described during treatment with all five TNFi to varying degrees, depending on the specific TNFi, 171 and also following secukinumab and ustekinumab treatments.172,173 A comprehensive literature search using three databases (PubMed, Web of Science, and the Cochrane Library) on immunogenicity of TNFi in autoimmune diseases between 1966 and 2017, showed that ADAbs are present in 10% of patients with SpA treated with a TNFi. 86 In these patients, lower drug through levels are also found, which are usually associated with poorer clinical response.85–89
ADAbs are often found in patients presenting secondary failure to the treatment and their detection predicted treatment failure over time.85,87,88,174 Overall, these observations led to the use of such biomarkers to drive treatment decisions, firstly in IBD, due to limited biological drug choice, and then in RA and SpA. Algorithms have been developed to identify TNFi poor responders and to drive treatment decisions, especially after the failure of a TNFi.90,91 In some studies, in patients with ADAbs and suboptimal treatment response the drug dosage was increased successfully to achieve a better treatment effectiveness. 88 More recently, the detection of ADAbs was used to identify patients more prone to successfully taper the biological treatment. 92 In patients with insufficient response, detectable ADAbs and low TNFi levels, we can assume that the drug effect is impaired by ADAbs (Figure 1). Thus, switching to another TNFi may be beneficial as it restores the TNF-α blockade. Nonetheless, if ADAbs are absent or low and the adequate therapeutic levels of the TNFi are achieved, inefficacy is not due to the neutralization of the therapeutic effect, but due to the fact that probably in that patient, TNF-α is not the main pathogenetic cytokine. 90 Therefore, in the latter, patients switching to another mode of action might be the best treatment choice. The large experience in RA confirms these observations, and also suggests that testing drug levels might be sufficient.91,175,176 One study on a small cohort of patients with SpA also found that in patients starting a second TNFi, those who had developed ADAbs on the first TNFi showed a better ASDAS response. 93
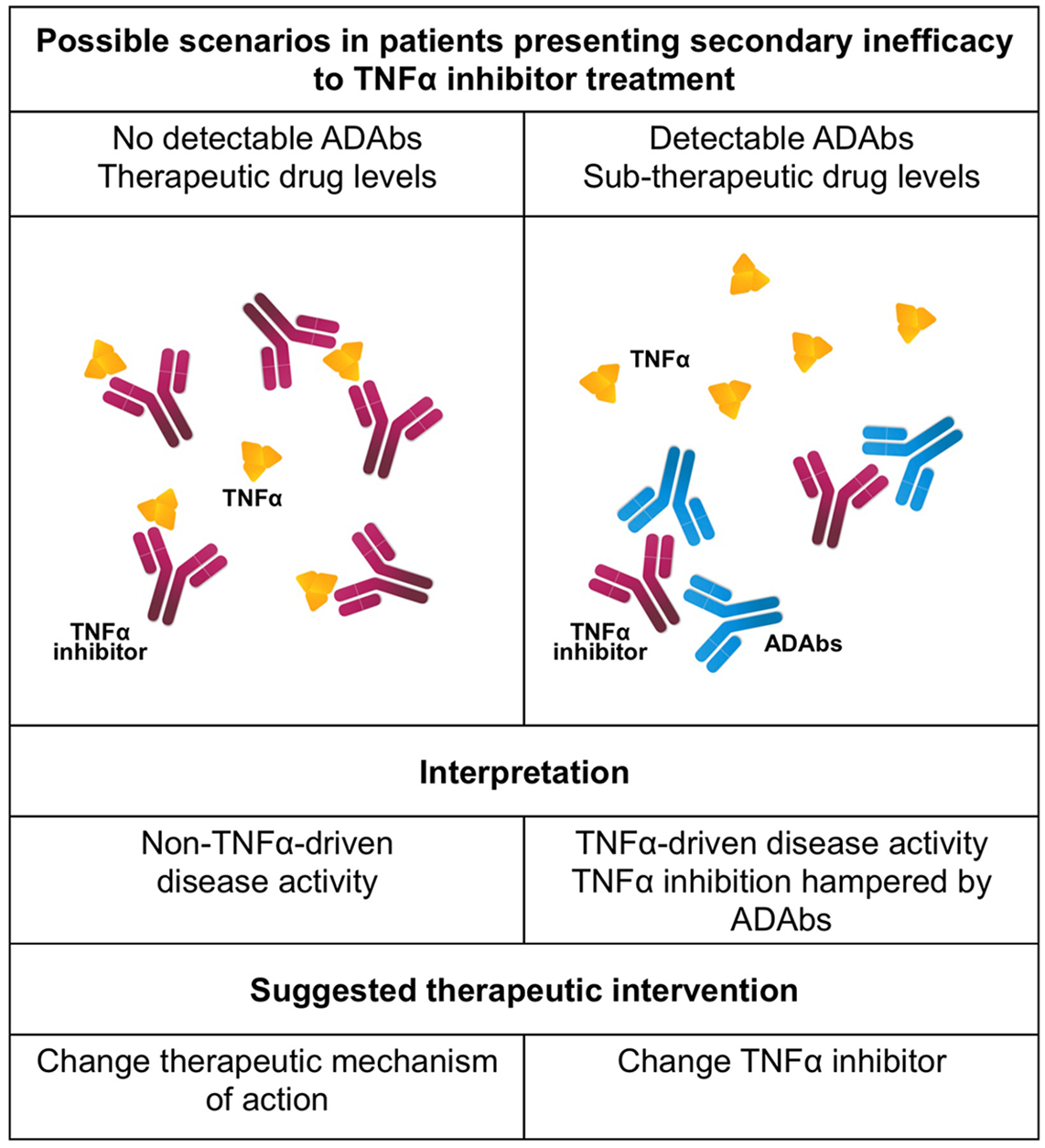
Possible pathogenetic mechanisms of secondary inefficacy to TNFα treatment. ADAbs, anti-drug antibodies; TNFα, tumor necrosis factor α
In addition to ADAbs, there are other factors that affects the pharmacokinetics of TNFi, such as concomitant use of conventional DMARDs, especially methotrexate, the degree of systemic inflammation, body weight, and sex. 174 Combination therapy with biologic agent and DMARDs is used to prevent the development of ADAbs in patients with RA and IBD,86,89,177 but there is no evidence to support their use in axSpA.178,179 Noteworthy, some studies also evaluated immunogenicity of switching from innovator to biosimilar infliximab in patients with SpA 180 and, as expected, it was not associated with any significant difference in the anti-drug antibody level. 180
Combination of biomarkers
In rheumatic diseases, the need for biomarkers has led to several attempts to identify an index including a panel of biomarkers to be used for clinical assessment. In SpA, only two studies are available to date. The first was conducted in a large cohort of 356 patients with SpA treated with golimumab. The study considered 73 molecules potentially associated with structural damage as assessed with mSASSS over a 2-year follow up, and found that only IL-6 was correlated with MRI changes. 45 Rademacher and colleagues, 77 considered 117 patients treated with nonsteroidal anti-inflammatory drugs in the ENRADAS trial. Only 10 biomarkers were investigated: VEGF, leptin and HMW-ADN were associated with mSASSS changes after 2 years (the latter two were inversely correlated with mSASSS). The combination of these three biomarkers with clinical characteristics proved to be superior than the clinical variables alone, but with a small added value in predicting structural damage.
Conclusion
Numerous studies have been conducted to seek biomarkers to guide treatment in SpA and to monitor the disease. Currently, no new biomarkers satisfy the characteristics for use in clinical practice and CRP remains the most relevant biomarker in axSpA. Grouping and understanding the role of all other potential biomarkers is challenging. Inflammatory markers, such as CPT, have been investigated but standardization is lacking and they mirror CRP. Markers of bone metabolism, such as MMP and Dkk-1, have shown diverging results on disease activity and progression. The reason could be that biomarkers implicated in the axSpA pathogenetic process are restricted to specific tissues and endothelial compartments and do not migrate to the systemic circulation and/or lymphoid organs.127,146 ADAbs and therapeutic drug monitoring are adequate tools to drive treatment decision but are not useful to characterize the patient and identify those prone to more rapid structural damage. Eventually, a combination of biomarkers may be promising, nevertheless association with clinical characteristics is necessary to increase their predictive value. Further research should focus on the most promising biomarkers in order to reduce heterogeneity of observations and better define their role and cut-offs either alone or in combination.
Footnotes
Acknowledgements
The authors would like to express their appreciation to Eric Frank Nde for his assistance in editing the English version of this manuscript.
Author contributions
RR and AD contributed to study design and critical revision. ML and FO contributed to data collection and manuscript drafting. AO, MF and MF contributed to literature revision.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.