
Abstract
Background:
Despite being burdened by significant adverse events, glucocorticoids (GCs) are frequently employed in managing adult onset Still’s disease (AOSD), prompting the need for GC-sparing agents. In this work, we performed a systematic review and meta-analysis to synthesize the evidence about the reduction of concomitant GCs dosage and the rate of GCs discontinuation in patients with AOSD who were treated with anakinra, a recombinant IL-1 receptor antagonist.
Methods:
A systematic review of the literature was completed to identify all available data concerning the reduction of concomitant GCs dosage following anakinra in AOSD and a meta-analysis was thus performed using a random-effects model.
Results:
A significant reduction of the GCs dosage was detected by pooled analysis with mean difference of –22.4 mg/day [95% confidence interval (CI): –28.8 to –16.1, p < 0.0001] at the last follow-up; the heterogeneity was moderate (Q = 11.67 with df = 7.00, p < 0.0001, I2 = 40.01%). Furthermore, the pooled analysis under a random effects model showed an overall rate of GCs discontinuation of 0.35 (95% CI: 0.28–0.41, p < 0.0001); the heterogeneity was low (Q = 5.99 with df = 6.00, p < 0.0001, I2 = 0.00%).
Discussion:
Taking together all these findings, the reduction of concomitant GCs dosage following anakinra could be suggested, leading to a further improvement of AOSD therapeutic strategy.
Conclusion:
In conclusion, the present systematic review and meta-analysis suggests the reduction of concomitant GCs dosage following treatment with anakinra. A percentage of patients are no longer required to be treated with GCs, discontinuing these drugs without a flare of the disease.
Highlights
Glucocorticoids (GCs) are frequently employed in adult onset Still’s disease (AOSD).
Sparing strategies are necessary to minimize the risk of GCs cumulative dosages.
As per meta-analysis, anakinra induced a significant reduction of GCs in AOSD.
Anakinra induced a discontinuation of GCs in 35% of patients with AOSD.
The GC-sparing effects of anakinra could improve the management of AOSD.
Introduction
Adult-onset Still’s disease (AOSD) is a rare inflammatory disease, typically characterized by fever, arthritis, and skin rash, which requires an immunosuppressive therapeutic strategy. 1 Glucocorticoids (GCs) are frequently employed as initial therapy starting with the dosage of 0.8–1 mg/kg/day prednisone-equivalent, although higher intravenous high-dosages are administered to manage life-threatening complications.2,3 GCs commonly induce a dramatic clinical response, even within few hours and days; the higher dosages are reported as being more efficient than lower dosages leading to subsequently less relapses of the disease.3,4 After the achievement of clinical response, with the disappearance of inflammatory signs and symptoms and normalization of laboratory markers, tapering of GCs could start, reducing the dosage of GCs as clinically feasible. However, dependence on GCs is reported, due to the possibility of a disease flare following the reduction of dosage or discontinuation of these drugs, thus requiring long-term therapy. 5 Concerning possible predictors, patients characterized by splenomegaly, low levels of glycosylated ferritin, increased values of erythrocyte sedimentation rate, and young age at onset of the disease could have an increased risk of dependency on GCs. 6 Furthermore, the long-term therapy with GCs is associated with a number of adverse events. In fact, in immunosuppressive therapeutic strategies, the concomitant use of GCs is a significant predictor of infections. 7 Besides the increased risk for infections, GCs are associated with further adverse events, such as osteoporosis, glaucoma, and glucose metabolism derangements, which contribute to the development of cardiovascular disease. 8 Consequently, different therapies have been proposed as GC-sparing agents in AOSD, including methotrexate, intravenous immunoglobulins, and tumor necrosis factor inhibitors, with controversial results.9,10 In this context, taking into account the pathogenic role of interleukin (IL-1), 11 anakinra, a recombinant IL-1 receptor antagonist, has been successfully employed in AOSD.12,13 However, lacking evidence based data, the administration of biologic drugs nowadays relies mainly on clinical judgement, 14 suggesting the need of a systematic analysis of evidence in order to retrieve relevant indications to manage AOSD. On these bases, we performed a systematic review of literature and meta-analysis to synthesize the evidence about the reduction of concomitant GCs dosage and the rate of GCs discontinuation in patients with AOSD who were treated with anakinra.
Methods
Analysis of literature
The evidence about the reduction of concomitant GCs dosage and the rate of GCs discontinuation in patients with AOSD who were treated with anakinra were retrieved by a systematic review of the literature. One author (PR) designed the research by assessment of international databases, PubMed to evaluate MedLine, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science (WOS). The databases were examined up to 30th September 2019. The following research terms were used in Pubmed: (“adult onset Still’s disease” OR “adult onset stills disease” OR “adult onset Still disease” OR “Still’s disease” or “stills disease” or “still disease” or “Still’s Disease, Adult-Onset” OR “adult onset Still*”) AND (“anakinra” OR “Interleukin 1 Receptor Antagonist Protein”). Furthermore, different combinations of more relevant keywords were employed to increase the accuracy of the research. Finally, a hand-search of relevant articles bibliography was performed to possibly identify additional manuscripts.
Inclusion criteria and study selection
The research question was about the ability of anakinra to lead to a reduction or a discontinuation of concomitant therapy with GCs in patients with AOSD. Because of its rarity, the majority of clinical research on AOSD is characterized by an observational design without a comparator. The population intervention comparison outcome (PICO) strategy was used for the research question construction: (a) population: patients with AOSD; (b) intervention: treatment with anakinra and concomitant therapy with GCs; (c) comparison: lacking an active comparator, studies were considered if the concomitant therapy with GCs was analyzed before and after anakinra following a minimum follow-up of 4 weeks; (d) outcome: the reduction of concomitant GCs dosage and the rate of GCs discontinuation. Concerning the study design, clinical trial, observational cohort studies, and case series recruiting at least six patients were considered, as performed in a previous meta-analysis. 15 Thus, the inclusion criteria were studies enrolling patients with AOSD (either clinical trial, observational cohort studies, or case series recruiting at least six patients) with a minimum follow-up of 4 weeks, treatment with anakinra and concomitant therapy with GCs, data about the reduction of GCs dosage following anakinra, data about the discontinuation of GCs following anakinra, and full-text versions published in English. The exclusion criteria were lack of data about concomitant therapy with GCs, analysis of the same cohort of patients from previous studies, data from preclinical studies, data reported on congress abstracts, and full-texts not available in English. Inclusion and exclusion criteria are summarized in Table 1. Two authors (PR and FU) independently assessed titles and abstracts of manuscripts, and, after that, they evaluated full texts of selected abstracts for inclusion in the systematic reviews according to the previously mentioned criteria. A discussion with the senior author (RG) resolved any disagreements to reach a consensus.
Inclusion and exclusion criteria to include manuscript in the systematic literature review.

AOSD, adult onset Still’s disease; GCs, glucocorticoids.
Data extraction
Two independent authors (PR and FU) extracted the data by selected manuscripts, a senior reviewer (RG) verified this process. During this process, the following variables were recorded: first author name, study year, study design, duration of follow-up, reduction of concomitant GCs dosage, and rate of GCs discontinuation in patients with AOSD at the end of study-period. In case of data concerning the use of sequential biologic drugs, the data about the last drug was extracted for purposes of analysis. If data about different time-points were available, the longest follow-up values were assessed.
Quality and risk of bias assessment
Two independent authors (PR and FU) assessed the quality of the selected manuscripts assigning a score of good, fair, or poor. The Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group proposed by the National Heart, Lung, and Blood Institute - US Department of Health & Human Services was employed. A discussion with a third senior author (RG) resolved disagreements in order to reach a consensus on these features.
Data analysis
For each study, dosages of GCs and rate of GC discontinuation (calculated as the number of patients discontinuing GCs) were retrieved. Crude difference in mean (before-after) with standard error and confidence interval was used to summarize the reduction in steroid dose in individual studies. Event rate with standard error and confidence interval was used to summarize the number of patients withdrawing from GCs in individual studies. Overall effect size was derived by using a random-effects model, considering the probable high level of heterogeneity. I 2 and Cochran’s Q statistic were employed to evaluate the between-study heterogeneity.16,17 After correcting for possible publication bias, the pooled estimates were calculated by the “trim and fill” method. 18 A two-tailed p-value < 0.05 was considered significant. Comprehensive Meta-Analysis software (CMA; Version 2.0, Englewood, USA) was used to perform the statistical analyses by one author (FU).
Reporting method
As detailed in Supplemental materials 1, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines was followed for reporting the data, derived from our analyses in this manuscript.
Results
Results of literature search and characteristics of the included studies
The analysis of databases retrieved 387 articles (Medline via Pubmed: n = 177; Web of Science: n = 202; Cochrane Library: n = 8); after screening titles and abstracts (removing duplicates, preclinical studies, manuscripts not written in English language, congress abstracts, case reports, reviews, manuscripts with wrong population, and manuscripts out of topic) 14 articles were assessed for eligibility by analysis of full-texts and nine manuscripts were finally selected, as shown in Figure 1. Five manuscripts were excluded after assessment of the full text due to the lack of information concerning the concomitant GCs therapy and despite data about the clinical efficacy of anakinra.19–23 Amongst the selected manuscripts, one open randomized multicenter trial with two parallel groups 24 and eight observational single-arm retrospective studies25–32 were retrieved. Concerning the randomized trial, 24 22 patients were randomized to anakinra or synthetic disease modifying anti-rheumatic drugs (DMARDs), but we considered only the 12 patients randomized to anakinra according to the general design of this work. The overall rate of evidence retrieved was poor; the open randomized multicenter trial was codified as “fair”, whereas the other retrospective studies were codified as “poor”. Collectively, 417 patients were included in the final analysis, as summarized in Table 2. These patients, aged 36.85 ± 4.42 [mean ± standard deviation (SD)] years, showed a disease duration of 6.75 ± 3.39 (mean ± SD) years.
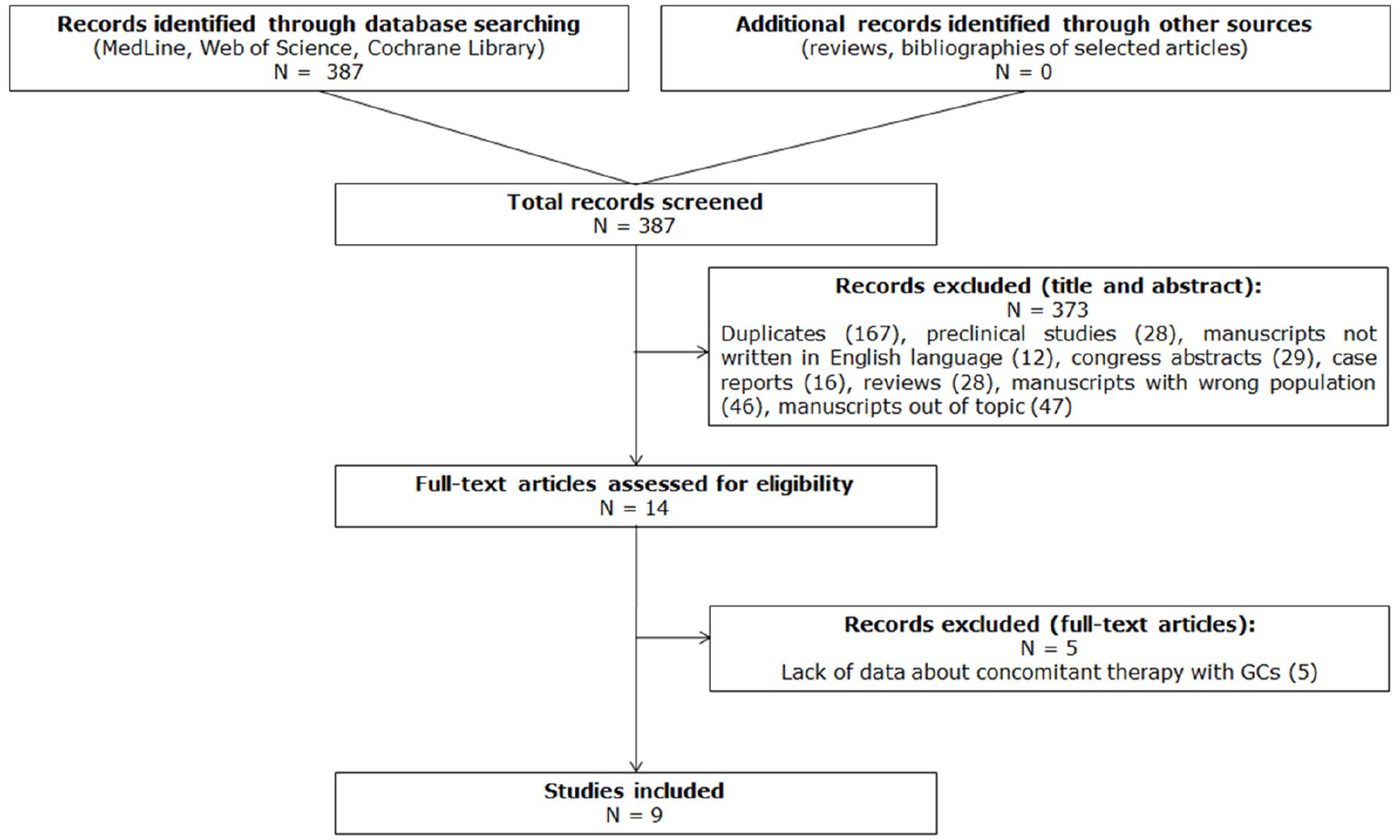
Flow chart of study selection. The studies selection is shown, finally retrieving 9 manuscripts to be included.
The reduction of concomitant GCs dosage and the rate of GCs discontinuation following treatment with anakinra in AOSD.

data are reported as mean ± SD or median (range) according to the results reported in each study of daily intake of CCSs.
AOSD, Adult onset Still’s disease; CCSs, corticosteroids; GCs, glucocorticoids; NR, not reported; SD, standard deviation.
The reduction of concomitant GCs dosage following treatment with anakinra in patients with AOSD
The reduction of concomitant GC dosage following treatment with anakinra was investigated in eight studies including 288 patients, which reported dosages of GCs at the beginning of the study and at the last follow-up. As shown in Figure 2, the pooled analysis estimated a significant reduction of the GCs dosage with mean difference of –22.4 mg/day [95% confidence interval (CI): –28.8 to –16.1, p < 0.0001] at the last follow-up. The heterogeneity across studies was moderate, Q = 11.67 with df = 7.00, p < 0.0001, I 2 = 40.01%. Following visual inspection of the funnel plot, no asymmetry was retrieved, as reported in Figure 3. Consequently, the assessment of the funnel plot with the “trim and fill” method retrieved no study to be trimmed, without any recalculation of point estimate under random effects (–22.4 mg/day, 95% CI: –28.8 to –16.1, p < 0.0001).

Pooled analysis of the reduction of concomitant GC dosage following treatment with anakinra. This figure shows a significant reduction of the concomitant GC dosage, a mean difference of –22.4 mg/day (95% CI: –28.8 to –16.1, p < 0.0001) is retrieved at the last follow-up, following treatment with anakinra.
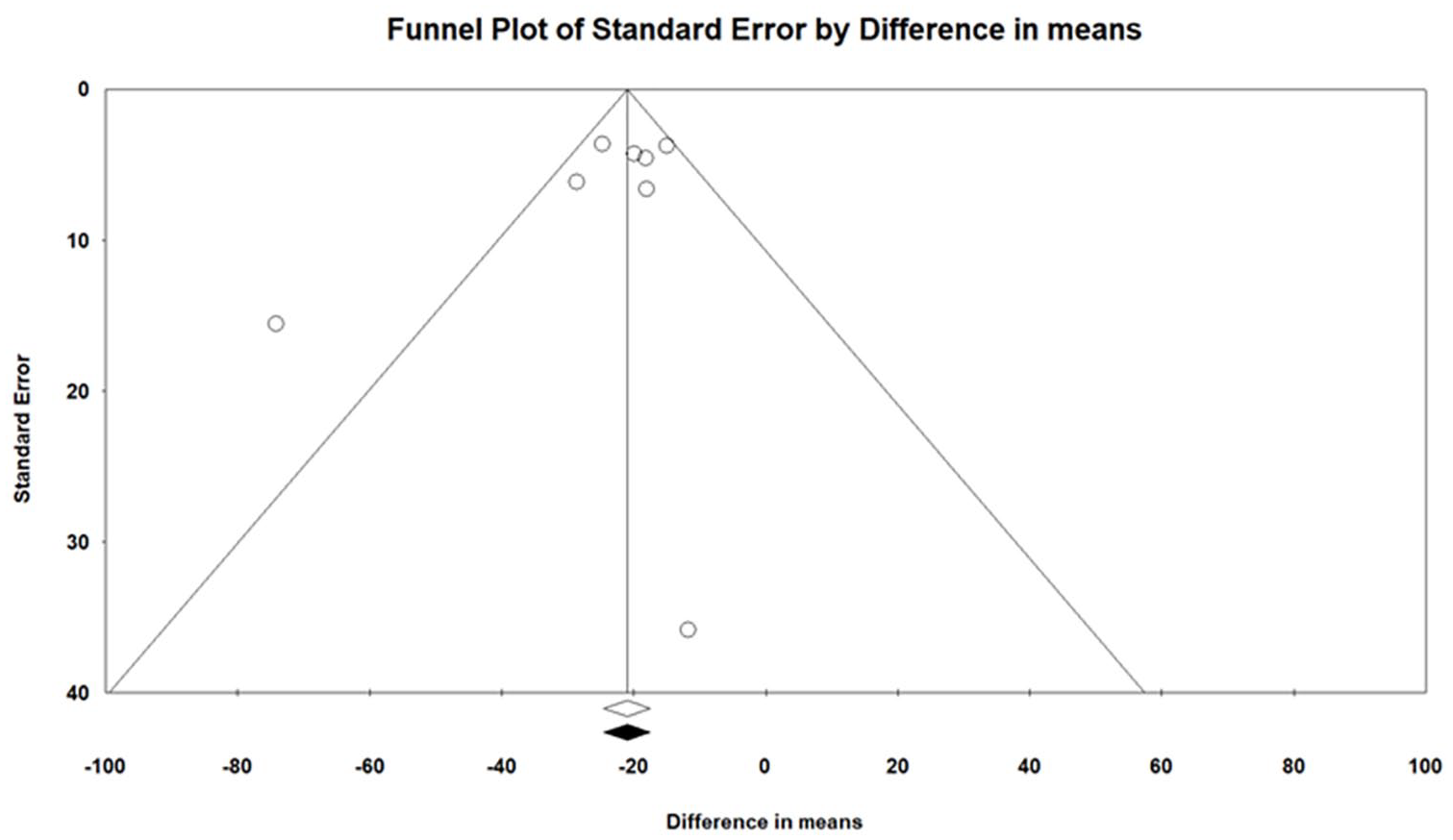
Funnel plot of the reduction of concomitant GC dosage following treatment with anakinra. Following visual inspection of the funnel plot, no asymmetry was retrieved, with no study to be trimmed.
GCs discontinuation following treatment with anakinra in patients with AOSD
The rate of GCs discontinuation after treatment with anakinra was investigated in seven studies including 234 patients with AOSD. A discontinuation rate of 0.35 (95% CI: 0.28–0.41, p < 0.0001) was estimated by the pooled analysis under a random effects model, as reported in Figure 4. The heterogeneity across studies was low, Q = 5.99 with df = 6.00, p < 0.0001, I 2 = 0.00%). Following visual inspection of the funnel plot, no asymmetry was retrieved, as shown in Figure 5. Consequently, the assessment of funnel plot with the “trim and fill” method retrieved no study to be trimmed, without any recalculation of point estimate under random effects (0.35, 95% CI: 0.28–0.41, p < 0.0001).
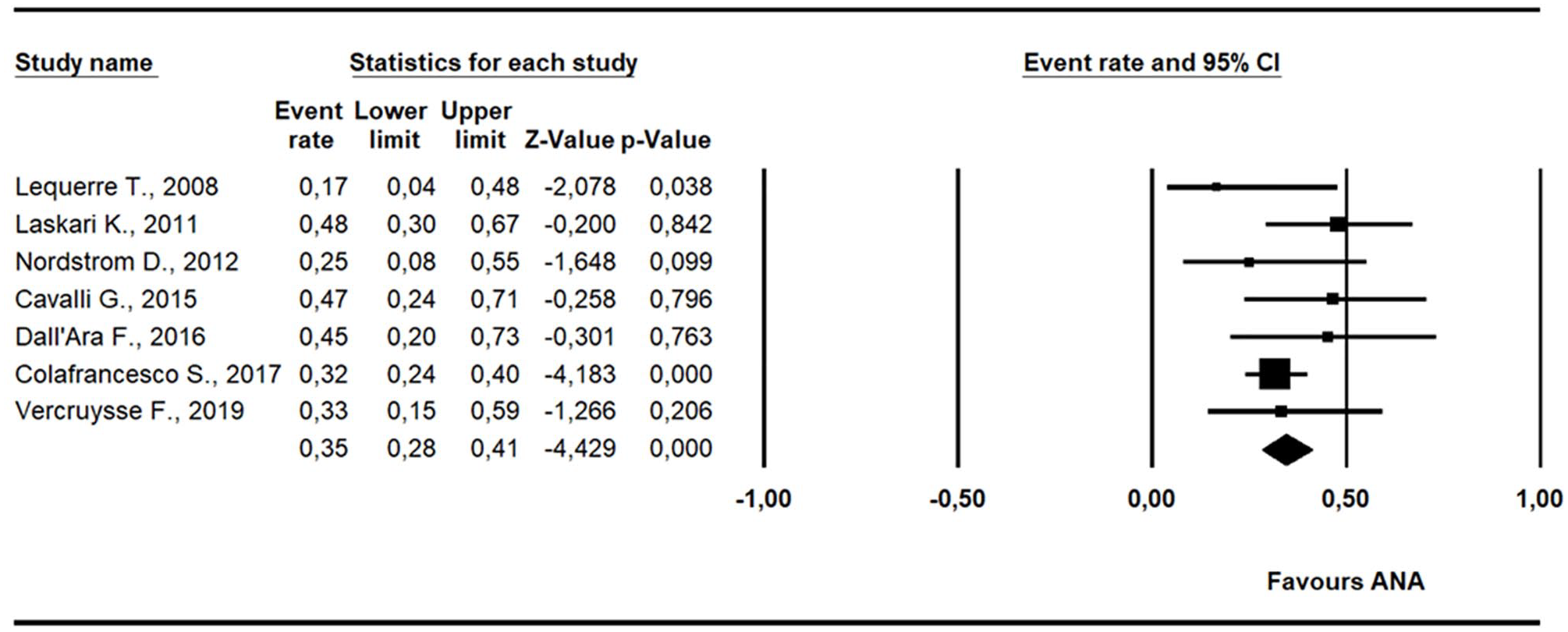
Pooled analysis of GC discontinuation following treatment with anakinra. A significant percentage of patients discontinued GCs 0.35 (95% CI: 0.28–0.41, p < 0.0001) is retrieved at the last follow-up, following treatment with anakinra.

Funnel plot of GCs discontinuation following treatment with anakinra. Following visual inspection of the funnel plot, no asymmetry was retrieved, with no study to be trimmed.
Discussion
AOSD is a rare but severe disease, with recurrent flares, multi-visceral involvement and life-threatening complications which may burden the clinical course of these patients requiring immunosuppressive therapies.33–35 GCs are frequently involved in managing AOSD, suggesting the necessity of GC-sparing agents to minimize the risks of cumulative dosages. In the present systematic review of literature and meta-analysis, we assessed the reduction of concomitant GCs dosage following treatment with anakinra in AOSD. Of interest, the pooled analyses reported a reduction of daily GCs dosages and a significant proportion of patients who discontinued GCs, suggesting the role of anakinra as a possible GC-sparing agent. Collectively, a mean reduction of 22.4 mg/day of GCs was retrieved, with 35% of patients able to discontinue the GCs, suggesting a possible subsequent reduction in occurrence of predictable side effects. In rheumatic diseases, long-term GC-treated patients are exposed to several predictable side effects, such as impaired insulin sensitivity, increased blood pressure, osteoporosis, and peptic ulcer disease. 36 The reduction of concomitant GC dosage following treatment with anakinra could consequently reduce the occurrence of these comorbidities that are related to the cumulative exposure of GCs, thus possibly improving the long-term outcomes of patients with AOSD.2,10,37 Furthermore, a well-known increased risk of infections in patients treated with immunosuppressive drugs is described, mainly in patients who were treated with GCs. 38 In this context, it has been reported that AOSD is associated with a higher risk of infection;39,40 a relevant percentage of patients treated with long-term GCs could experience pulmonary infections with a high mortality rate.41,42 Taking together all of these findings, the reduction of daily intake GCs could have the noteworthy consequence of reducing the rate of infections in patients treated with anakinra. In addition, the significant reduction of GCs would balance the high cost of therapy with anakinra compared with synthetic DMARDs. AOSD is associated with high costs, estimated around $30,000 for each hospitalization, which are also associated with the occurrence of side effects related to the chronic use of GCs. 43 On this basis, the reduction of concomitant GCs dosage following treatment with anakinra could possibly decrease the recurrence of hospitalization in AOSD.44,45
In spite of offering a synthesis of literature about concomitant GC dosage reduction and GC discontinuation on AOSD, our meta-analysis is affected by different limitations and the results should be prudently generalized. The poor methodological quality of the included articles limited our work, since mainly retrospective studies were retrieved, thus postulating less consistent findings than randomized controlled trials. However, AOSD is codified as a rare disease and it would be difficult to organize adequately powered randomized controlled trials. In addition, considering the uncontrolled nature of the evidence and missing data, we could not analyze the possible role of concomitant immunosuppressive therapies, which could influence the administration of GCs. Considering the low-quality of the included studies, relevant features, including disease duration, previous therapies, and mean duration of anakinra treatment, were reported, impairing the possibility to systematically analyze these features. Furthermore, the different lengths of follow-ups could also affect our results. Taking all these issues into consideration, future specifically designed and powered studies are necessary to entirely elucidate the role of anakinra as a GC-sparing agent.
In conclusion, the present systematic review and meta-analysis could suggest the reduction of concomitant GC dosage following treatment with anakinra. Of interest, a percentage of patients are no longer required to be treated with GCs, discontinuing these drugs without a flare of the disease. Although our meta-analysis is affected by different limitations and specifically designed studies are needed, GC-sparing effects of anakinra could be suggested in the treatment of AOSD, thus possibly improving the management of these patients.
Footnotes
Acknowledgements
The authors thank Mrs Federica Sensini for her technical assistance.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
PR received speaker honoraria and/or unrestrictive research grants from BMS, Ely Lilly, MSD, Pfizer, and SOBI. FU declared no conflict of interest. JS received speaker honoraria from SOBI. RDG declared no conflict of interest. LC received speaker honoraria from SOBI and Novartis.
RG received speaker honoraria and/or unrestrictive research grants from Abbvie, Actelion, Bristol-Myers Squibb (BMS), Ely Lilly, Merck Sharp & Dohme (MSD), Pfizer, Roche, and Swedish Orphan Biovitrum (SOBI).