
Abstract
Background:
Risk factors for sepsis have not been assessed in patients receiving tumor necrosis factor-alpha inhibitors (TNFi) for immune-mediated inflammatory diseases (IMIDs) who are vulnerable to serious/hospitalized infections.
Methods:
Data from 2003–2017 were obtained from Taiwan’s National Health Insurance Research Database to identify patients receiving TNFi, including etanercept, adalimumab, and golimumab, for IMIDs including rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriasis (PsO), psoriatic arthritis (PsA), Crohn’s disease (CD), and ulcerative colitis (UC). To investigate risk factors for sepsis, we used the Sepsis-3 definition and calculated hazard ratios (HRs) with 95% confidence intervals (CIs) using Cox regression analysis.
Results:
There were 17,764 patients (mean age 49.3 ± 14.3 years; females, 57.6%) receiving TNFi for IMIDs, including RA (58.6%), AS (19.1%), PsO (15.1%), PsA (2.5%), CD (3.0%), and UC (1.7%). The overall incidence rate of sepsis was 1088 per 100,000 person-years. After adjustment for potential confounders, recent sepsis within 3 months before TNFi initiation (HR, 2.35; 95% CI, 1.73–3.20), CD (HR, 3.36; 95% CI 2.11–5.34; reference group: AS) and glucocorticoid use (prednisolone-equivalent dose, mg/day HR, 1.05; 95% CI, 1.05–1.06) were associated with the risk of sepsis. Intriguingly, golimumab users appeared to have a lower risk of sepsis compared with etanercept users (HR, 0.56; 95% CI, 0.38–0.83). In addition, socioeconomic status, including urbanization level and insured amount, was associated with sepsis in a dose-response manner.
Conclusions:
Recent sepsis, CD, concomitant glucocorticoid use, and low socioeconomic status, which were associated with an increased risk of sepsis, are crucial for individualized risk management plans.
Keywords
Introduction
Immune-mediated inflammatory diseases (IMIDs) comprise disorders characterized by altered immune regulation leading to chronic and dysregulated inflammation.1,2 IMIDs, including rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriasis (PsO), psoriatic arthritis (PsA), and inflammatory bowel disease (IBD), are estimated to affect approximately 3–7% of the population, with an estimated incidence rate of 80/100,000.3,4 Tumor necrosis factor alpha plays an essential role in accelerating the progression of IMIDs. The successful development of tumor necrosis factor-alpha inhibitors (TNFi) such as etanercept, adalimumab, and golimumab has led to a paradigm shift in the management of IMIDs. However, the increased infection risk remains a major concern.5–8 Indeed, several studies have found an increased infection risk, including serious and opportunistic infections associated with distinct TNFi. However, the infection definition varied across studies.6,9,10 For example, serious infections can be defined as those associated with death, hospitalization, or intravenous antibiotic use. 6 Therefore, there is a crucial need for a straightforward infection definition. The Sepsis-3 definition, introduced in 2016 to characterize sepsis as a life-threatening organ dysfunction caused by a dysregulated host response to infection, is increasingly applied to define sepsis in the claim database.11,12 Therefore, we aimed to assess the sepsis risk in patients receiving TNFi for IMIDs using the Sepsis-3 definition. In the present study, we used the Taiwanese Nationwide Health Insurance (NHI) Research Database (NHIRD) to investigate the incidence of sepsis and to identify risk factors for sepsis in patients receiving TNFi for IMIDs.
Methods
Data source and identification of patients with IMIDs
Taiwan’s NHI program, launched in 1995, is a single-payer government-operated compulsory health insurance program. As of 2015, up to 99.6% of Taiwan’s population was enrolled in the NHI program. 13 The NHIRD, the database for the NHI program, contains all registration profiles and original claims data obtained for reimbursement. In the present study, we used the ambulatory and inpatient data of NHIRD from 2003 to 2017 to identify subjects with IMIDs. We used the International Classification of Diseases-Ninth Revision-Clinical Modification (ICD-9-CM) and International Classification of Diseases-Tenth Revision-Clinical Modification (ICD-10-CM) codes for the identification of patients with IMIDs, including RA (714.0, M05, M06.0–M06.3, M06.8, and M06.9), AS (720.0, M45, and M08.1), PsO (696.1, L40.0–L40.4, L40.8, and L40.9), PsA (696.0 and L40.5), Crohn’s disease (CD; 555 and K50), and ulcerative colitis (UC; 556 and K51). To avoid potential misclassification, we excluded patients (n = 341) with overlapped IMIDs diagnoses.
Outcome
The study outcome was the first diagnosis with sepsis after the initiation of TNFi. In the present study, we employed the Sepsis-3 definition to identify patients with sepsis. 11 Sepsis was identified by the ICD-9-CM and ICD-10-CM codes proposed by Angus et al., in which a diagnosis of bacterial or fungal infection and at least one acute organ dysfunction are needed to define a septic episode.14,15 The definition of acute organ dysfunction comprised: dysfunction of the respiratory, cardiovascular, hepatic, hematologic, renal, and/or central nervous system; metabolic dysfunction; and cardiovascular shock. The index date of sepsis was defined as the first day of an emergency department or hospital visit for sepsis. The censored date was defined as 31 December 2017, the last date of the data used, or the time of withdrawal from the NHI for any reason, including death or leaving Taiwan.
Covariates
Covariates in the regression model included age, sex, Charlson comorbidity index (CCI), TNFi, concomitant medication, urbanization level of the patient’s residence, and insured amount according to the payroll. The presence of comorbidity was defined as the presence of one or more inpatient visits or at least three ambulatory visits with a corresponding ICD-9/10-CM code within 1 year prior to the index date. The CCI revised by Deyo et al. was used to assess the general comorbid medical condition. 16 The goal of the study was to determine the risk of sepsis due to treatment with TNFi, including etanercept, adalimumab, and golimumab, as well as medications frequently administered for IMIDs. The concomitant medications included in the present study were non-steroidal anti-inflammatory drugs, glucocorticoids, hydroxychloroquine, sulfasalazine, methotrexate, leflunomide, and immunosuppressants, including cyclophosphamide, cyclosporin, azathioprine, and mycophenolate mofetil. The TNFi infliximab and certolizumab were approved in 2017 in Taiwan and therefore were not included in the present study. The urbanization level of the patient’s residence was classified into four clusters based on population density (people/km2), population ratio of elderly subjects aged >65 years, population ratio of subjects with educational levels of college or above, population ratio of agricultural workers, and number of physicians/100,000 subjects. 17 We used payroll-related insured amount, which was divided into quantiles, as a proxy measure of the patient’s socioeconomic status.
Statistical analysis
Descriptive results were presented as means ± standard deviation or percentages. The incidence rate of sepsis was presented as per 100,000 person-years. Patients contributed to person-years based on the length of medication exposure. The Cox proportional hazards model was used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for newly diagnosed sepsis after adjustment for age, sex, CCI, and other potential cofounders. All data were analyzed using SAS statistical software version 9.3 (SAS Institute, Cary, NC, USA). A p value < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board of Taichung Veterans General Hospital in Taiwan (approval number: CE19038A). All personal data were anonymized; therefore, informed consent was waived.
Results
Demographic data of the enrolled patients
We identified 17,764 patients with IMIDs initiating TNFi therapy, including 7891, 7538, and 2335 patients using etanercept, adalimumab, and golimumab, respectively. The most common IMID was RA (10 402, 58.6%), followed by AS (3387, 19.1%), PsO (2679, 15.1%), PsA (451, 2.5%), CD (536, 3.0%), and UC (309, 1.7%). As shown in Table 1, the mean age was 49.3 ± 14.3 years, and 57.6% of the patients were female. Notably, 2.2% of the patients receiving TNFi for IMIDs had sepsis 3 months before TNFi initiation (Table 1). The disease duration was shorter, and the proportion of those with a CCI ⩾ 1 was higher among patients treated with etanercept. The concomitant use of methotrexate, sulfasalazine, hydroxychloroquine, immunosuppressants, and glucocorticoids was also higher among patients treated with etanercept compared with those using the other two TNFi.
Demographic data of patients receiving TNFi for immune-mediated inflammatory diseases.

Data are presented as means ± standard deviations.
cyclophosphamide, cyclosporin, azathioprine, and mycophenolate mofetil.
CCI, Charlson comorbidity index; DMARD, disease-modifying antirheumatic drug; NTD, new Taiwan dollars; TNFi, tumor necrosis factor alpha inhibitors.
Comparison of incident sepsis among distinct TNFi and IMIDs
The incidence rate of sepsis in patients receiving TNFi was highest in those with IBD (2509/100 000 patient-years in CD and 1520/100,000 patient-years in UC), followed by those with RA (1262/100,000 person-years), PsA (951/100,000 patient-years), PsO (866/100,000 patient-years), and AS (519/100,000 patient-years) (Table 2). We further determined the incident rates of sepsis in patients treated with different TNFi for distinct IMIDs. Intriguingly, among those with RA, the golimumab users appeared to have a lower risk of sepsis compared with the etanercept users [incidence rate ratio (IRR), 0.6; 95% CI, 0.4–0.9], but this finding was not found in the other IMIDs. There was a slightly higher incidence rate of sepsis in patients with RA receiving adalimumab than those receiving etanercept (IRR, 1.2; 95% CI, 1.05–1.5), and similar trends were found in patients with PsO (IRR, 1.6; 95% CI, 0.9–2.9) but not in patients with AS (IRR, 0.7; 95% CI, 0.4–1.3) and PsA (IRR, 1.0; 95% CI, 0.3–3.0).
Incidence of sepsis categorized by distinct TNFi and immune-mediated inflammatory diseases.
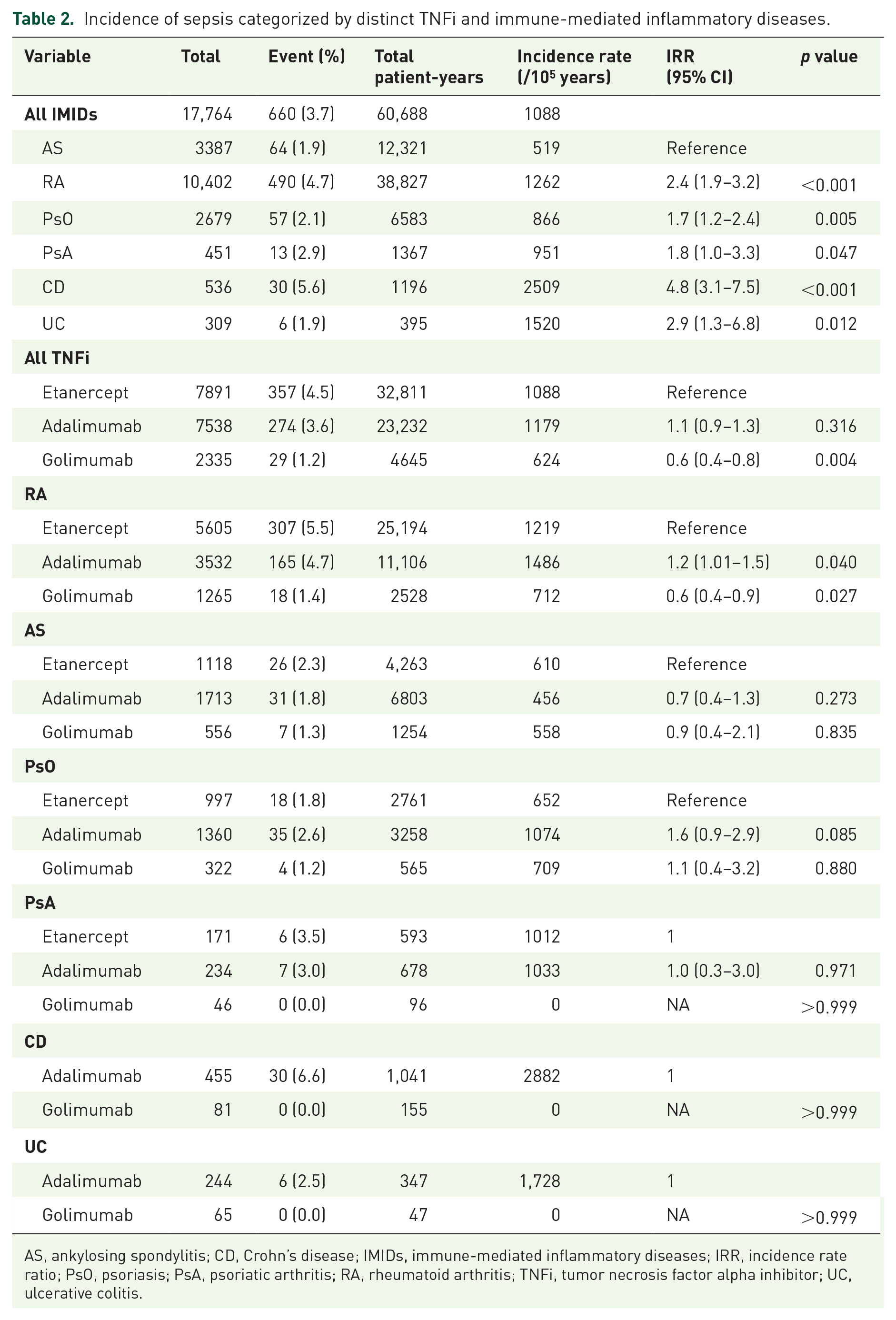
AS, ankylosing spondylitis; CD, Crohn’s disease; IMIDs, immune-mediated inflammatory diseases; IRR, incidence rate ratio; PsO, psoriasis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; TNFi, tumor necrosis factor alpha inhibitor; UC, ulcerative colitis.
Factors associated with the risk of sepsis among TNFi-treated patients with IMIDs
The multivariable Cox regression analysis revealed that the risk of sepsis was positively associated with age (HR, 1.06; 95% CI, 1.05–1.07), male sex (HR, 1.24; 95% CI, 1.04–1.48), CCI (HR, 1.30; 95% CI, 1.23–1.39), CD (reference, AS; HR, 3.36; 95% CI, 2.11–5.34), recent sepsis within 3 months before TNFi initiation (HR, 2.35; 95% CI, 1.73–3.20), and corticosteroid use (prednisolone-equivalent dose, mg/day; HR, 1.05; 95% CI, 1.05–1.06) (Table 3). Intriguingly, golimumab use (reference, etanercept; HR, 0.56; 95% CI, 0.38–0.83) and concomitant use of sulfasalazine (HR, 0.81; 95% CI, 0.67–0.99) appeared to be associated with a decreased risk of sepsis. Notably, the risk of sepsis was also associated with lower levels of urbanization and payroll-related insured amount in a dose-response manner. The sepsis risk was greatest in patients with the lowest level (IV) of urbanization (HR, 1.69; 95% CI, 1.35–2.12), followed by those with level III (HR, 1.41; 95% CI, 1.09–1.82) and level II (HR, 1.21; 95% CI, 0.96–1.52) urbanization compared with those with level I urbanization. Similarly, the sepsis risk was lowest in patients with the highest insured amount (level IV; HR, 0.32; 95% CI, 0.19–0.52), followed by those with level III (HR, 0.59; 95% CI, 0.46–0.76) and level II (HR, 0.82; 95% CI, 0.68–0.99) insured amount compared with those with level I insurance premium.
Unadjusted and adjusted hazard ratios of association between variables and risk of sepsis.

cyclophosphamide, cyclosporin, azathioprine, and mycophenolate mofetil.
AS, ankylosing spondylitis; CCI, Charlson comorbidity index; CD, Crohn’s disease;
CI, confidence interval; DMARD, disease-modifying antirheumatic drug; HR, hazard ratio;
NTD, new Taiwan dollars; PsA, psoriatic arthritis; PsO, psoriasis; RA, rheumatoid arthritis; TNFi, tumor necrosis factor alpha inhibitor; UC, ulcerative colitis.
Discussion
In this nationwide population-based study, we investigated the risk of sepsis in patients receiving distinct TNFi for IMIDs. We found that old age, recent sepsis, TNFi therapy for CD, concomitant glucocorticoid use, a low urbanization level, and a low insurance premium were independently associated with an increased sepsis risk. These data provide real-world evidence of sepsis risk in patients treated with distinct TNFi for IMIDs and highlight the need for individualized risk management strategies.
In the present study, recent sepsis within 3 months prior to TNFi initiation was a robust predictor for incident sepsis in patients receiving TNFi. Indeed, patients with sepsis are susceptible to deteriorating health after sepsis recovery as reported by recent studies, including one from Taiwan.18–20 Using the Medicare claim database in the United States, Prescott et al. found that patients were frequently re-hospitalized within the first 90 days after severe sepsis, in agreement with our findings. 18 Prescott et al. also investigated 2617 Medicare beneficiaries who survived hospitalization for sepsis and found that 1115 (42.7%) survivors of severe sepsis were re-hospitalized within 90 days mainly because of sepsis, congestive heart failure, and pneumonia. 19 Similarly, in a study of the Taiwanese NHIRD, Shen et al. reported that patients who survived hospitalization for sepsis had a higher risk of subsequent sepsis compared with the age- and sex-matched controls (35.0% versus 4.3%). 20 These lines of evidence indicate the importance of vigilance for recurrent sepsis in patients treated with TNFi for IMIDs who have recently recovered from sepsis.
We used the Sepsis-3 definition to define sepsis in the present study. The previous sepsis definition, Sepsis-2, which is based on a requisite minimum of two systemic inflammatory response syndrome criteria, has been found to be somewhat unreliable.21,22 One in eight patients admitted to an intensive care unit with infection and new organ failure are estimated to not fulfil the sepsis definition according to Sepsis-2, and these patients exhibit a protracted clinical course with significant mortality and morbidity. 21 Therefore, there is a crucial need to define outcome-relevant sepsis based on organ dysfunction. 11 The Sepsis-3 definition, which uses the sequential organ failure assessment score to identify patients with sepsis, is increasingly used to identify patients with sepsis in large clinical databases.12,15,22,23
TNFi is associated with an increased risk of infection with varied definitions. However, the definite sepsis risk in patients receiving TNFi for IMIDs remains unclear. Singh et al. conducted a Bayesian network meta-analysis of published trials to assess the risk of serious infections in patients with RA and found that standard-dose biological drugs (odds ratio, 1.31; 95% CI 1.09–1.58) and high-dose biological drugs (odds ratio, 1.90; 95% CI 1.50–2.39) were associated with an increased risk of serious infections compared with the conventional disease-modifying antirheumatic drugs. 6 The definition of serious infections includes infections associated with death, hospitalization, or the use of intravenous antibiotics, and these definitions were in accordance with the standard protocol in the clinical trial of biologics. 6 Regarding the incidence of hospitalized infections, one recent Italian study by Quartuccio et al., including administrative data between 2006 and 2017, reported that 289 (4.2%) of the 5596 patients diagnosed with RA, AS, or PsO were hospitalized because of infection during a median follow-up period of 5.2 years and that the use of biologics, mainly TNFi, conferred an approximately two-fold increased risk of hospitalized infections. 24 Altogether, these data on the incidence of serious/hospitalized infections are largely consistent with the findings of the present study using sepsis as the outcome. We suggest that sepsis should at least be used as a more straightforward and practical definition of infectious diseases when compared with hospitalized/serious infections.
Given that the majority of patients receiving TNFi are those with RA, 6 the evidence in IMIDs other than RA, particularly IBD, is relatively sparse. The present study provided comprehensive evidence regarding the sepsis risk in patients with AS, PsO, PsA, CD and UC. We found a significantly high incidence of sepsis in patients receiving TNFi for IBD. A similarly high incidence of serious infections was also reported in the French National Health Insurance database involving nearly 200,000 patients with IBD and approximately 900,000 patient-years of follow-up. The study’s authors reported that the incidence of serious infections in patients with IBD receiving TNFi was 1890/100,000 patient-years, which was similar to the present study results (2509/100,000 patient-years in CD and 1520/100,000 patient-years in UC, Table 2). 8 In one Taiwanese study of the NHIRD, Weng et al. determined the infection risk of 249 patients who received TNFi for IBD between 2001 and 2015 and found that the incidence rates of infections requiring hospitalization were 1024/100,000 patient-years among those who received conventional dose (one-year cumulative dose of adalimumab <1280 mg) and 565.7/100,000 patient-years among those receiving higher than the conventional dose. 25 Notably, Weng et al. found that intra-abdominal infections accounted for nearly 30% of all infection-related hospitalizations. Therefore, increased susceptibility to intra-abdominal infections might account for the higher sepsis incidence in patients receiving TNFi for IBD compared those with IMIDs other than IBD.
Intriguingly, we noted a slightly lower sepsis incidence in patients with RA receiving golimumab compared with those receiving etanercept (Table 2). Currently, there are no head-to-head trials comparing golimumab with other TNFi. However, the available reports and indirect comparisons of different TNFi suggest that golimumab might potentially have better tolerability compared with etanercept and adalimumab regarding the risk of serious infections.26,27 Further studies are required to validate the superiority of golimumab over other TNFi in terms of sepsis risk.
Socioeconomic status, including access to care, has a substantial impact on sepsis incidence and outcomes.28–32 In the present study, we assessed the socioeconomic status using urbanization levels, which may reflect access to care, and payroll-related insurance premium. We found that both urbanization levels and payroll-related insured amount were associated with sepsis risk in a dose-response manner. Goodwin et al. used the administrative data in South Carolina to report that residence in a medically underserved area, which was defined by a composite score of a population’s age, economic status, and access to basic medical services, was associated with higher incidence (8.6 versus 6.8 cases/1000 person-years, p < 0.01) and mortality rates (15.5 versus 11.9 deaths/10,000 person-years) of severe sepsis. 29 Similarly, using data from 30 239 participants in the Reasons for Geographic and Racial Differences in Stroke cohort, one of the largest contemporary cohorts of community-dwelling adults in the United States, Donnely et al. reported that a high neighborhood socioeconomic status was associated with a reduced risk of hospitalization for infection (HR, 0.84; 95% CI, 0.73–0.97). 30 Therefore, the association between living in less urbanized areas and the increased sepsis risk in patients receiving TNFi suggests that urban-rural disparities across Taiwan should be considered while administering TNFi in patients with IMIDs.
In addition to the aforementioned impact of urbanization, the low insurance salary was an independent predictor for the development of sepsis among patients receiving TNFi for IMIDs in the present study. Several studies have demonstrated that the association between low income and increased infection may result from the lack of insurance, increased environmental exposure to pathogens, lack of vaccination, or unhealthy behaviors.28,33–35 However, we wish to clarify that the lack of insurance was unlikely a key factor in the present study given the nationwide health insurance coverage in Taiwan. 13 Collectively, these pieces of evidence indicate the need for particular vigilance for sepsis during TNFi treatment of patients with a relatively low socioeconomic status.
The present study has several limitations. First, given that the study focused on the sepsis risk among patients receiving TNFi, the risk for viral infections as well as mycobacterial infections and the role of biologics other than TNFi were not assessed. Second, data on drug compliance could not be assessed in the NHIRD; however, its magnitude should be mild given that these expensive biologics are applied periodically in Taiwan. Third, the laboratory data, including disease activity and microbiological findings, could not be assessed using the claim database. The lack of data regarding disease activity in claim data is also a limitation. However, the disease activity is periodically checked by Taiwan NHI during the application for the continuous use of TNFi. In addition, the detailed information regarding concomitant medications should also reflect the disease activity of IMIDs. Despite these limitations, the use of the NHIRD claim data allowed for the assessment of sepsis risk among all patients receiving TNFi for IMIDs within the Taiwanese population without recall bias.
Conclusion
We used a nationwide population-based claim database to investigate the risk for sepsis in patients receiving TNFi for IMIDs. We identified that recent sepsis within 3 months before TNFi initiation, concomitant glucocorticoid use, a low urbanization status, and a low payroll-related insured amount were associated with increased sepsis risk. These findings provide real-world evidence of specific risk factors of sepsis in TNFi-treated patients with IMIDs, which warrant further studies to establish individualized risk management strategies in patients receiving TNFi for IMIDs.
Footnotes
Acknowledgements
This study is based on data from the NHIRD in Taiwan, but the interpretation of data and conclusions do not represent those of the NHIRD. The authors are thankful for the statistical work by the Biostatistics Task Force and Healthcare Service Research Center of Taichung Veterans General Hospital for their assistance with the statistical analyses.
Author contributions
Conceived and designed the experiments: WCC, CYW, and HHC. Acquired data: HHC and CHL. Contributed materials/analysis tools: WCC, BCH, WNH, YHC, CLW, and HHC. Wrote the paper: WCC and HHC.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by grants from Taichung Veterans General Hospital, Taiwan (TCVGH-1087325D, TCVGH-1084404D, and TCVGH-1087326D). The funders had no role in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.