
Abstract
The advent of biological therapies has been a major therapeutic advance in rheumatology. Many patients now enjoy improved quality of life through better disease control. The number of therapies continues to grow both within drug class (including biosimilar drugs) and via new mechanisms. For the first time, nonbiological drugs such as small-molecule inhibitors (Janus kinase inhibitors) have shown clinical equivalence. However, clinical unmet need remains with up to a third of patients commenced on a biologic therapy having minimal or no response: (a) Generally, the first biologic used secures the best response, with likelihood of remission falling thereafter with successive therapies; (b) the success of strategy trials using biological therapies can be difficult to replicate in clinical practice due to a combination of patient factors and service limitations. Accordingly, ensuring optimization of initial treatment is an important consideration before switching to alternatives. Therapeutic drug monitoring (TDM) is the measurement of serum levels of a biologic drug with the aim of improving patient care. It is usually combined with detection of any antidrug antibodies that could neutralize the effect of the therapy. This technology has the potential to be a form of ‘personalized medicine’ by individualizing therapy, in particular, dosing and likelihood of sustained treatment response. It requires a clear relationship between drug dose, blood concentration and therapeutic effect. This paper will outline the technology behind TDM and unpack what we can learn from our colleagues in gastroenterology, where the adoption of TDM is at a more advanced stage than in rheumatology. It will explore and set out a number of clinical scenarios where rheumatologists might find TDM helpful in day-to-day practice. Finally, an outline is given of international developments, including regulatory body appraisals and guideline development.
Introduction
The advent of biological therapies has been a major therapeutic advance in rheumatology. Many patients now enjoy improved quality of life through better disease control. The number of therapies continues to grow both within drug class (including biosimilar drugs) and via new mechanisms. For the first time, nonbiological drugs such as small-molecule inhibitors (Janus kinase inhibitors) have shown clinical equivalence. However, clinical unmet need remains; up to a third of patients commenced on a biologic therapy have minimal or no response. 1 Generally, the first biologic used secures the best response with likelihood of remission falling thereafter with successive therapies. 2 The success of strategy trials using biological therapies can be difficult to replicate in clinical practice due to a combination of patient factors and service limitations. Accordingly, ensuring optimization of initial treatment is an important consideration before switching to alternatives.
Therapeutic drug monitoring (TDM) is the measurement of serum levels of a biologic drug with the aim of improving patient care. It is usually combined with detection of any antidrug antibodies (ADAs) that could neutralize the effect of the therapy. This technology has the potential to be a form of ‘personalized medicine’ by individualizing therapy, in particular, dosing and likelihood of sustained treatment response. It requires a clear relationship between drug dose, blood concentration and therapeutic effect. This paper will outline the technology behind TDM, unpack what we can learn from our colleagues in gastroenterology where the adoption of TDM is at a more advanced stage than in rheumatology. It will explore and set out a number of clinical scenarios where rheumatologists might find TDM helpful in day-to-day practice. Finally, an outline is given of international developments, including regulatory body appraisals and guideline development.
Scientific development of TDM
The role of immunogenicity
Immunogenicity can be described as the ability of a substance to produce an immune response in the body. It is contingent on numerous factors. When caused by a drug, these triggers could include its unique structural properties, murine components, contaminants during formulation or indeed, via the production process itself by way of additives or aggregates. Individual patient characteristics, such as genetics, disease phenotype and degree of immunosuppression may be relevant. Moreover, various treatment factors such as concomitant therapies, dose, frequency, route of administration and interruptions to therapy may influence immunogenicity. 3 For example, in the latter scenario, the discontinuity theory of the immune response states that the key to the induction of an immune response is the antigenic difference in a time-dependent manner. 4 Put simply, the intermittent appearance of an antigen (such as pulsed drug dose) produces a large and sustained immune response. In rheumatic disease, immunogenicity is best understood in tumour necrosis factor (TNF) inhibitor therapy (TNFi). On initiation of treatment, free drug exists in serum. However, as time passes, up to 40% of patients develop ADAs. 5 These bind to free drug, forming immune complexes. Provided the quantity of such ADA is low, minimal clinical effect may be realized. However, the scenario can develop, whereby extensive ADA is produced, effectively removing free drug which becomes bound in immune complex, and the therapeutic effect drops. Finally, no free drug, but free ADA, can be detected. At this stage, the drug is not having any effect at the target binding site. These ADAs can be categorized as neutralizing or nonneutralizing. In the former, the ADA is binding to epitopes within the therapeutic binding site of the biological agent and prevents target binding. Non-neutralizing ADAs permit binding to target but may impact efficacy as they increase clearance of the ADA/drug complex. 5 Most ADAs are neutralizing, and available assays tend to detect small immune complexes. Those larger than dimer size are phagocytosed by macrophages. It is these large complexes that produce the infusion reactions that we associate with immunogenicity: irregular-shaped large complexes trigger the complement cascade, whereas small complexes appear unable to activate complement. 6
Assay development
Over the past decade, the number of available drug-monitoring and ADA-monitoring assays has grown almost proportionally to the number of TNF-alpha targeting agents. The main principle underlying TDM is the reliable measurement of available drug in the serum and, if this is proven uncharacteristically low, to assess if antibodies towards the drug have developed. Performance of available drug-monitoring assays are judged on their reliability, ease of use, speed with which test results are available, amount of serum sample required for the test, cost and quantitative, rather than qualitative, result that would be easily interpretable in the clinical setting. With this in mind, the three most commonly used approaches include an enzyme-linked immunosorbent assay (ELISA), a radioimmunoassay (RIA) and a homogeneous mobility shift assay (HMSA), although other methods are available (reviewed in Vande Casteele 7 and Bendtzen 8 ).
ELISA assay
For the drug measurement using ELISA, a selection of artificially raised antibodies towards TNF or specific TNFi are used, predominantly mouse or goat in origin. 9 First, the plate is coated with either a monoclonal mouse ADA or TNF-alpha protein prior to adding patient serum sample from which the drug specifically binds to the coated layer and is ‘captured’. 10 Subsequent detection of the captured drug occurs by adding antihuman immunoglobulin G (IgG) or mouse ADA linked to the colourimetric substrate, thus allowing quantitative measurement.9,11,12 Specificity of the antibodies aids the accuracy of the test and limits false-positive results, therefore underscoring the advantage of using monoclonal or monospecific polyclonal antibodies. 13
Similarly, the ELISA method can be used in detection of the ADAs. For this, drug itself is used as capture-and-detection antibody with serum-derived ADAs captured in between.14–16 Although serum predose trough sample is collected, addition of acidification step before the assay allows dissociation of endogenous drug-ADA complexes to minimize serum drug interference. 17 Other limitation of ELISA assay is its inability to detect some monovalent human antibodies, such as IgG4 as it relies on the ability of antibodies to bind two epitopes, or its ‘bivalency’, to allow the typical ‘sandwich’ structure of this assay, depicted in Figure 1. 18

Assays used in therapeutic drug monitoring.
Radioimmunoassay
To overcome these obstacles, other assays were developed. In RIA, serum sample is diluted with protein A, after which, nonbound serum components are washed off, and radiolabelled TNF-alpha or drug are added for respective measurement of the drug or ADA. After incubation, nonbound radiolabelled substrates are washed off and radioactivity is measured.19,20 Alternatively, the HMSA method involves adding fluorescently-labelled TNF-alpha to the serum sample, after which, TNF-drug complexes are separated using high-pressure liquid chromatography in combination with size-exclusion chromatography.21,22 Similarly, ADA can be measured by adding fluorescent-labelled drug and following the process above. Both these systems are better at detecting low-affinity ADA due to less washing steps than in the ELISA protocol, 23 although they are more laborious and unsustainable in the case of RIA, which uses radioisotopes.
Point-of-care testing
More recently, point-of-care testing with finger prick blood sampling is becoming available (Promonitor Quick). 24 At present this is a qualitative measurement of anti-infliximab (anti-IFX) ADA; however, future improvement of point-of-care testing will undoubtedly aid decision making at the time of the clinic appointment.
Learning from gastroenterology
TDM of the TNFi infliximab (IFX) and adalimumab (ADAL) has been embraced by inflammatory bowel disease (IBD) specialists. Faced with a limited number of treatment options and a lack of robust disease activity scoring tools TDM has been adopted to support disease monitoring strategies. Guidelines published in 2017 by the American Gastroenterological Association 25 and IBD Sydney Organization and Australian Inflammatory Bowel Diseases Consensus Working Group 26 provide a useful overview and appraisal of the available evidence to support the use of TDM in IBD, as well as recommendations for implementing TDM in routine clinical practice. About one third of IBD patients treated with TNFi exhibit primary nonresponse (failure to respond to induction therapy) at 3–4 months. Among treatment responders, around 40% will experience secondary loss of response (defined by the need to intensify the TNFi dose) at 12 months. 27 The causes of TNFi treatment failure in IBD are complex and multifactorial. The development of neutralizing ADAs appears to be key. Several studies have demonstrated a link to TNFi drug levels and clinical outcomes in IBD.28–30 The much awaited personalized anti-TNF therapy in the Crohn’s disease study (PANTS) demonstrated that personalized TNFi dosing, guided by TDM, coupled with concomitant immunomodulator use, can improve clinical outcomes by optimizing trough drug levels and reducing the risk of ADA formation. 31
Two main TDM testing strategies are used in clinical practice; reactive TDM, which is performed in the face of re-emergence of clinical or laboratory markers of disease activity, and proactive TDM, in which regular testing is undertaken during clinical remission, with TNFi dosing adjustments being made to try and maintain trough drug levels within a prespecified target range. 32 To date, there are no data to support the use of one testing strategy over the other and published guidelines have tended to favour a reactive testing approach on the basis of available evidence to date. Although TDM has been implemented in diseases outwith rheumatoid arthritis (RA), it is not a given that the utility of TDM can be extrapolated across conditions. Indeed, a number of clear differences exist between the use of TDM in IBD compared with rheumatic diseases, as outlined in Table 1. One such example includes genotypic differences identified in the PANTS study, relating to patients with the HLA-DQA1*05 allele, where an increased rate of ADA occurs in Crohn’s disease treated with ADAL and IFX. 31 Pretreatment screening is being considered. The relevance in RA is unknown and remains an important research question.
Comparison of TDM use in inflammatory bowel disease and rheumatic diseases.
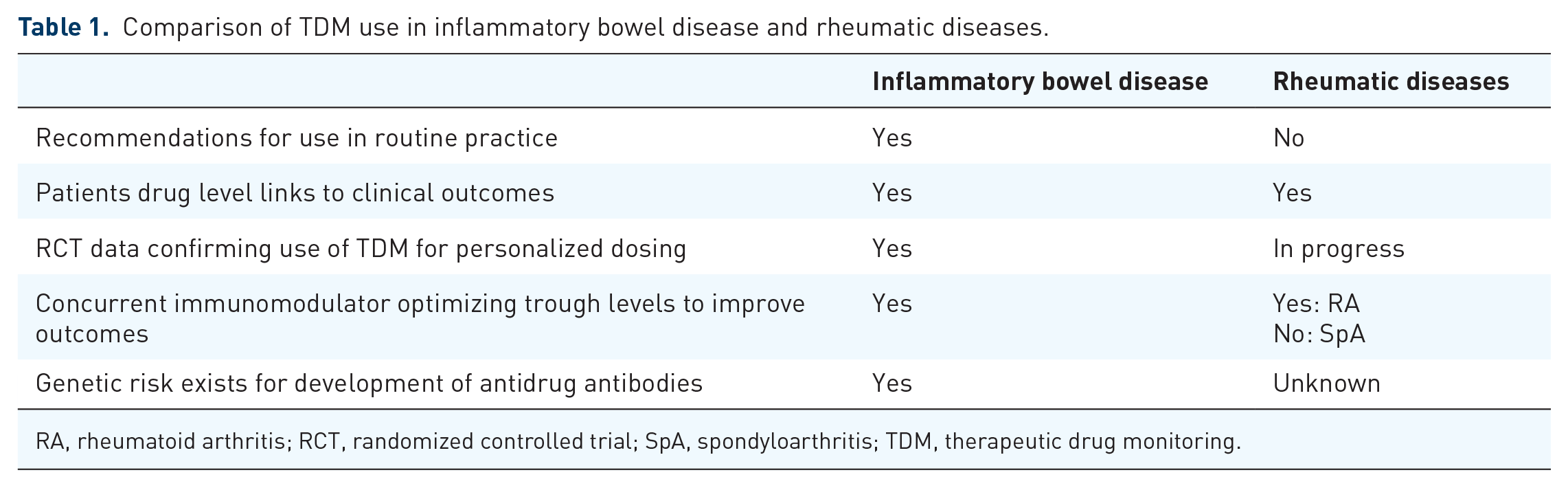
RA, rheumatoid arthritis; RCT, randomized controlled trial; SpA, spondyloarthritis; TDM, therapeutic drug monitoring.
Challenges for TDM in rheumatology
Pharmacokinetic and pharmacodynamic rationale for TDM
Understanding the pharmacokinetics (PK) of biologic drugs is a prerequisite for interpreting serum drug levels. Models tend to emphasize compartments of drug distribution, usually a central compartment such as the bloodstream and a separate but linked compartment, for example, peripheral tissues. These compartments permit the PK parameters to be measured: volume of distribution, clearance, transfer/elimination-rate constants and half-life. Monoclonal antibody PK use first-order transfer and elimination-rate constants. 33
Early work highlighted a relationship between serum trough IFX levels, pre-treatment C-reactive protein (CRP) and clinical response to IFX in RA. Patients with high initial CRP levels had low trough IFX levels, the latter also correlating with poorer clinical response. 34 This was supported by a further small trial in RA which was able to define the receiver operator characteristics (ROC) curves for IFX treatment in RA. 35 Development of the PK modelling in other condition such as ankylosing spondylitis (AS) suggested that the development of antibody to IFX was associated with accelerated IFX clearance. 36 This was supported by data in the RA population. 37
Factors affecting pharmacokinetics of TDM
One challenge relevant across disease type is that of PK variability when interpreting TDM results for an individual patient. The modelling mentioned above can help in attempting to plan drug dosing based on a number of factors. These include disease type, degree of disease activity, weight, sex, co-prescription of immunosuppressive drugs, and presence of neutralizing ADAs.
Regarding disease type, in the PLANETRA and PLANETAS studies comparing AS with RA for patients prescribed IFX, significantly fewer AS patients developed immunogenicity by formation of ADA than those with RA. 38 At a population level, therefore, general awareness of disease type will alter threshold for suspecting immunogenicity.
Second, there are challenges in understanding if the patient is in an active phase of their disease, or quiescent. For example, enhanced drug clearance in active Crohn’s disease occurs in the gastrointestinal tract, rapidly lowering serum drug levels. 31 The disease state could therefore have a significant influence on TDM, a phenomenon explained by the ‘Antigenic sink’ theory. This suggests that at times of active disease, when inflammation is high and TNF-alpha has high expression in tissue, the anti-TNF drug will migrate from serum to tissue and bind to the effector site, thus lowering the overall free drug present in serum. 39 Conversely, in remission, when little or no TNF-alpha is expressed in tissue, a higher concentration of drug will be found in serum. This has been confirmed in a study that showed an inverse correlation of serum trough IFX levels at 14 weeks post-treatment initiation with CRP values pretreatment, in RA patients. 34
Additional challenges influencing TDM interpretation include individual patient characteristics and sampling time. Biological sex, and therefore body composition of fat and muscle mass, has long been recognized as a factor in PK interpretation and similarly applies in TDM of biologic drugs.
For instance, can TDM results from a 100 kg male aged 21 be interpreted similarly to an 80-year-old 40 kg woman? Weight is adjusted for IFX prescribing, but several subcutaneous preparations including etanercept, ADAL and certolizumab have fixed dosing. Golimumab is licensed at double dose for patients weighing over 100 kg. In a UK study of over 300 RA patients, body mass index (BMI) was the strongest predictor of low drug levels and subsequent poor response. 40 Overweight patients are recognized to be underdosed on subcutaneous anti-TNF drugs. 41
The sampling date within a 2-week drug injection interval to obtain a trough measurement in TDM could be important: is within 3 days of drug administration acceptable, or could this be extended to up to 1 week? The acceptability to patients of additional phlebotomy and the impact on service delivery needs to be considered. Adherence is variable, and interruptions to therapy common, commonly due to intercurrent infection, and both factors may therefore affect serum trough levels.
Finally, one of the principal challenges of TDM has been the relative lack of high-quality clinical evidence that could support adoption. As a developing technology, this is not altogether surprising. However, recent evidence has emerged for the PK use of TDM, including drug dose interval extension incorporating patient safety, long-term prognosis and patient-adjusted factors as outlined below.
The NOR-DRUM clinical trial, a randomized controlled trial (RCT) of TDM across indications for patients receiving IFX is due to report soon and will hopefully provide further clarity on utility. 42 Virtually all the existing evidence in TDM is for anti-TNF agents, in particular, ADAL and IFX. The immunogenicity of these agents appears greater than other anti-TNF drugs, and the assays both for ADA detection and serum drug measurement have been used for a longer period of time. 43
In further considering TDM and its role in rheumatology, this review will concentrate on the development of a therapeutic range in TDM, concomitant methotrexate (MTX) use, the potential role of TDM in reducing infection risk, and the two main clinical scenarios of ‘proactive’ and ‘reactive’ testing. Most of the evidence relates to ADAL and IFX. These drugs will therefore provide the focus of the discussion that follows.
Therapeutic range
On launch of ADAL and IFX, the detailed development PK studies were not published by the pharmaceutical industry. They have resisted calls thus far to release data, which has slowed progress. However, Pouw and colleagues 44 published a concentration-effect curve of ADAL in RA patients participating in a prospective observational cohort study. Clinical efficacy measured by Disease Activity Score (DAS-28) improved with dose, but levels exceeding 8 µg/ml had no additional benefit on disease activity. An ROC curve established a cut off of 5 µg/ml which distinguished the European League Against Rheumatism (EULAR) good response from moderate/nonresponse (sensitivity 91%, specificity 43%). This development of a ‘therapeutic range’ 5 –8 µg/ml for ADAL provided a benchmark for interpretation of other studies.
Impact of concomitant immunosuppression
An additional factor, confirmed in the Pouw et al study 44 , is the effect of MTX in significantly increasing serum ADAL levels when coprescribed. A previous landmark study 45 recognized that MTX reduced immunogenicity in a dose-dependent manner. The reduction of ADA results in fewer immune complexes comprising biologic drug bound to ADA, resulting in a higher amount of free drug available to bind to target. It has been known for some time that MTX combined with anti-TNF therapy produces better drug retention and disease control. This may provide an explanation for that effect. Other disease-modifying antirheumatic drugs (DMARDs) appear to have a similar impact on ADAL serum levels, although to a lesser extent. 46
Infection risk
The aim of careful screening of patients requiring biologic therapy is to reduce risk of serious infections. Physicians adjust doses of immunosuppressive drugs as part of routine care where infection concerns are present or develop. Could TDM be an adjunct in risk stratification? Jani recently published data from large national prospective RA cohorts where TDM occurred at 3, 6 and 12 months post biologic initiation. 47 Results were stratified as low/normal/high drug levels based on the concentration-effect curves. Infection risk during the first year was analysed. RA patients with high biologic drug levels were found to have a 50% higher risk of all infections. If replicated, the clinical implications are clear: ‘overdosing’ patients with biologic drug risks infective complications and thus potentially, treatment suspension or cessation. While this is based on population cohorts and so not directly applicable to any individual patient, it is good practice to identify high-risk patients in the same way as screening prior to biologic introduction. TDM may therefore have patient safety implications.
Testing strategies
Proactive testing
Proactive TDM testing in rheumatology occurs when a patient is in DAS remission or low disease activity (LDA) and consideration is being made for ‘drug tapering’ (interval extension or dose reduction). Using any therapy at the lowest dose to gain maximal effect for the shortest period would generally be seen as good practice. EULAR has recommended tapering of biologic DMARDs, 48 and there is good evidence that for many patients LDA is maintained on a tapered dose, in both early RA and established disease. 49 Rheumatologists use a variety of factors with patients when advising about tapering; duration of LDA, severity markers such as erosions, anticitrunillated-protein-antibody-positive status, smoking status, etc. 50 It is likely that up to 25% of patients are overtreated with drug and could be considered for dose reduction. 45 L’Ami used TDM in patients who were in LDA, with ‘supratherapeutic’ drug levels (i.e. >8 µg/mmol) to extend the dosing interval of ADAL to 3 weekly for 6 months and compared with a group who remained at standard 2-weekly dosing. 51 The primary outcome of DAS-28 scores showed a modest difference, with the dose extension group favoured. Serum drug levels for this group remained in the therapeutic range of 5–8 µg after 6 months. While the study was small, it was fully randomized and showed noninferiority. Clinicians could consider using TDM in their LDA patients with RA to increase the interval of dosing where those patients start with a ‘supratherapeutic’ level and be confident of noninferiority of care. Chen and coworkers 52 showed ADAL dose halving is feasible for RA remission patients with high trough levels. These findings are supported by another study by Bouman 53 where high ADAL trough levels appeared a successful marker for tapering. However, this study tapered until discontinuation, and did not find a predictive value of TDM at baseline.
The health economic considerations of drug tapering are also significant from a societal perspective. Two studies have assessed the cost effectiveness of TDM in RA. Laine used Markov modelling and found TDM to be cost effective when the TDM results affected treatment decision in at least 2–5 per 100 patients. 54 Krieckaert and colleagues also found TDM to be cost effective, using a real-life large cohort of ADAL patients, concluding that in 72% of simulations, TDM cohorts saved costs and resulted in more quality-adjusted life years. 55
Reactive testing
‘Reactive testing’, where loss of response to TNFi has occurred, is the second scenario where TDM can be helpful. Failure to respond to biologic treatment can be categorized as either primary or secondary. Primary failure occurs when a patient does not respond to a newly prescribed anti-TNF drug or fails to respond within first 16 weeks of therapy. 56 Secondary treatment failure is when an initial good response is lost over a period of time, and is the common reason for discontinuation of therapy, 57 reaching 48% in one large series, compared with other causes such as infection or drug side effects. 58 Predictors of response at an individual level are difficult to determine, but population predictors do exist. For example, longer disease duration and high disease activity at disease onset are associated with treatment failure. 59 In a large population study, Jani and coworkers identified that low ADAL levels and ADAs tested 3 months from drug initiation were significant predictors of no response according to the EULAR criteria at 12 months. 60 Moreover, high BMI has been linked to reduced response to anti-TNF therapies. Klaassen and colleagues studied effect of BMI on clinical response to IFX in RA. 41 Patients were divided into three categories based on BMI. The percentage of responders significantly decreased in the groups with a higher BMI (84%, 75%, and 50% for BMI groups < 20 kg/m2, 20–30 kg/m2, and >30 kg/m2, respectively).
Secondary failure, due to immunogenicity, can occur after an initial therapeutic response and is associated with increased drug reactions and adverse effects. 61 Current data suggest that ADAL-treated patients develop antibodies within the first 6 months of treatment. This has also been observed with natalizumab, a humanized monoclonal antibody used in treatment of Crohn’s disease and multiple sclerosis. 62 The development of ADA appears to be the main reason for reduced drug concentration. In a seminal paper, Bartelds and coworkers published results of a prospective cohort study of ADAL-treated RA patients over 3 years and found that the 28% of patients who developed ADA had lower serum drug levels and lower likelihood of minimal disease state or remission. 45 In the REASON study, 20% of the study population tested positive for ADA. Of these, 81% had no detectable serum drug concentrations. 63 The ATTRACT study was one of the first randomized, double-blind placebo-controlled trials where a majority of patients with undetectable serum drug concentrations showed poor clinical response. 64 Similarly, Chen and colleagues demonstrated that the presence of ADA was associated with lower EULAR response and lower drug levels compared with those without ADA. 65
Approaches in primary and secondary failure
Currently, therapeutic decision making after primary or secondary failure of anti-TNF therapy does not include routine monitoring of ADA or drug concentrations in patient serum. Thus, therapeutic adjustments with or without drug switching is carried out blindly, without appreciation of immunogenicity. When patients show lack of response to a first anti-TNF drug, therapeutic options may include switching to a biologic agent with a different mechanism of action, switching to an alternative anti-TNF drug, or increasing the dose. Mulleman and coworkers demonstrated in a cohort of 24 anti-TNF RA nonresponders that when serum anti-TNF levels were checked, therapeutic decisions were changed for almost half of the patients. 66 Nonresponders with low serum IFX concentrations benefited from dose escalation, whereas patients with high IFX concentrations responded by switching to another biologic. Therefore, the checking of drug serum concentration and drug antibodies can be helpful in optimizing decision making. Vincent and colleagues proposed an algorithm to guide common clinical scenarios in a systemic review of clinical nonresponders. 67 Where suboptimal drug levels and absence of ADA occur, compliance and weight adjustment should be reviewed. Where dose adjustment is required, increasing the frequency has been found to be more effective than increasing the dose, as the latter is more likely to be associated with increased side effects. 68 Optimal drug serum concentration in the absence of ADA suggests mechanistic failure. In this situation switching to a drug with different mechanism of action is the next logical step. Association of ADA and low/absent drug concentration occurs in secondary failure where the treatment decision should be to switch to a less immunogenic drug. A summary of the different approaches is outlined in Tables 2 and 3. Most of the data available suggest etanercept as being less immunogenic, with detection of anti-etanercept antibodies reported at around 3%. 69 With increasing use of biosimilars, prescribers should be aware that that ADAs against the originator drug can cross-react with the respective biosimilar and possibly lead to further treatment failure. 70
Proactive testing: stable patients in remission or LDA considered for dose interval extension.

LDA, low disease activity.
Reactive testing: treatment failure/flare patients.

MOA, mechanism of action.
In summary, the ability to predict non-response at an early stage of treatment with a biologic agent could help optimize patient care and potentially have a significant health economic impact. Physicians should take into account individual patient factors such as weight, disease duration, disease activity and coprescription of DMARD therapy with biologic agents. In cases of treatment failure, immunogenicity should be considered. Greater understanding of immunogenicity and genetic factors should enable early identification of nonresponders and optimize therapeutic drug selection.
National and international developments
The National Institute for Clinical Excellence (NICE) has undertaken a technology appraisal of TDM in RA. 71 It has published a consultation document following the assessment that states, ‘Enzyme-linked immunosorbent assay (ELISA) tests for therapeutic monitoring of tumour necrosis factor (TNF)-alpha inhibitors (drug serum levels and antidrug antibodies) show promise but there is currently insufficient evidence to recommend their routine adoption in rheumatoid arthritis’. Moreover, ‘Laboratories currently using ELISA tests for therapeutic monitoring of TNF-alpha inhibitors in rheumatoid arthritis should do so as part of research and further data collection’, and ‘Further research is recommended on the clinical effectiveness of using ELISA tests for therapeutic monitoring of TNF-alpha inhibitors in rheumatoid arthritis’. The UK therefore has the paradoxical situation of NICE not recommending routine use of TDM, but service developments are expanding to accommodate clinical interest.
Scotland, for example, has introduced a National TDM service, accessible to all specialties and offering testing for ADAL and IFX. This development followed a business case supported by clinicians from Gastroenterology and Rheumatology. To our knowledge, this is the first nationally accessible service, and within the first year, turned over more than 3000 individual samples, rising to 9000 by year 2. The relatively small costs of staffing, training, ELISA kit purchase and infrastructure are anticipated to be offset by efficiencies of drug use.
In an effort to provide clarity to clinicians, given the disparity between NICE recommendations and the clinical interest at ‘grassroots’ level, a EULAR study group was formed in 2018, which successfully applied to be a EULAR Task Force in 2019. This group has been charged with undertaking a review of the evidence in TDM and either making recommendations or ‘points of interest’ to advise clinicians when considering TDM. It is hoped that the evidence will be significantly enhanced by the NOR-DRUM study, an RCT of TDM in patients with IFX treatment across a number of disease types [ClinicalTrials.gov identifier: NCT03074656].
Conclusion
TDM in rheumatology has not yet been adopted into routine care. However, it is a technology providing insight into why a patient is failing treatment and provides the opportunity for personalized dosing, with potential positive health economic implications. In rheumatology, there remain research questions which require robust RCT data before TDM is likely to have universal adoption. It is hoped that the NOR-DRUM study will begin to fill that gap.
However, it is our opinion that selective use for ADAL and IFX should be considered in the following scenarios: (a) when advising patients to extend interval dosing/reduce dose; (b) in patients with drug loss of clinical response (LOR) where weight or adherence may be reducing the serum drug level; (c) in patients with secondary LOR (especially if not taking MTX) to understand if treatment failure is mechanistic or immunogenic. In each of these scenarios, the addition of TDM to the existing clinical/biomarker information is likely to affect the treatment decision.
Biosimilar drugs have been a welcome addition to originator molecules in creating downward pressure on drug cost, easing the societal burden of biologic therapies. However, reducing waste is equally important. TDM has been shown within large populations to identify patients with ‘supra-therapeutic’ levels where we know there are no additional clinical benefits; and yet these patients are exposed to an increased risk of infection. Researchers, policymakers, clinicians and patients should give careful consideration to investigating further if TDM could improve patient safety and reduction of drug wastage. As we move towards personalized medicine, TDM could be a valuable tool in understanding dose optimization and therapy selection for patients with rheumatic disease.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
MP has honoraria for speaker’s fees from Sandoz. Advisory boards: Abbvie, Gilead, Celltrion. Conference fees, hospitality and travel: Roche, Lilly and Celgene. Educational grants: Grifols, Abbvie, Sandoz.