
Abstract
The development of biological therapies has had an impact on the management of several medical conditions. Their use in systemic lupus erythematosus (SLE), however, remains very limited. This review has summarized the evidence on the clinical effect of biologicals in SLE. Biological drugs with a number of targets have been studied in several phase II and III randomized controlled trials (RCTs). Positive results have been obtained in phase III RCTs with belimumab and this led to its license for active SLE. The clinical experience with belimumab has confirmed the efficacy and safety of belimumab in SLE. Promising results have been noted in phase II trials for blisibimod, sifalimumab, anifrolumab, and ustekinumab. Despite the fact that the RCTs with rituximab did not achieve their primary endpoint, clinical experience with rituximab is extensive and shows favorable clinical response in refractory renal and non-renal SLE. It is hoped that further ongoing phase III RCTs on a number of biological agents in SLE will highlight the potential role of other biologicals in the management of this challenging and heterogeneous condition.
Keywords
Introduction
Biological therapies have revolutionized the treatment of inflammatory joint disease including rheumatoid arthritis and spondylarthritis (in particular ankylosing spondylitis and psoriatic arthritis). With the introduction of tumor necrosis factor (TNF) inhibitors two decades ago followed by other biological drugs including interleukin-6 (IL-6) inhibitors, rituximab, and abatacept, biologicals are now widely used and recommended in the management of rheumatoid arthritis. 1 Similarly, in ankylosing spondylitis, TNF inhibitors and interleukin-17 (IL-17) inhibitors are used. 2 In psoriatic arthritis, in addition to TNF inhibitors and IL-17 inhibitors, interleukin-12/23 (IL-12/23) inhibitors, and abatacept are also recommended. 3
In contrast to this, the use of biological therapies in systemic lupus erythematosus (SLE) is limited, with fewer agents available for use in this condition. SLE is clinically heterogeneous, with variable involvement of multiple organ systems including the skin, joints, kidneys, neurological and hematological involvement. 4 It is thus more challenging to measure the response to treatment not only in the clinical setting but also during research. A number of validated tools are available to assess disease activity including Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), British Isles Lupus Activity Group (BILAG), Systemic Lupus Erythematosus Activity Measure (SLAM) and European Consensus Lupus Activity Measurement (ECLAM). 5 Response criteria are composite measurements for disease activity and response and are used in clinical trials that investigate the efficacy of drugs. In SLE these include the SLE Responder Index (SRI) and BILAG-based Combined Lupus Assessment (BICLA).6,7
Traditionally, since the 1950s, corticosteroids and antimalarials have been used in the treatment of SLE. Following this other immunosuppressive drugs were introduced for the treatment of moderate to severe SLE, including azathioprine, cyclophosphamide, methotrexate, and mycophenolate. 8 In 2011, belimumab was approved as the first biological and first licensed drug for SLE. 9
The aim of this review is to summarize the available evidence on the clinical impact of biological therapies for the treatment of SLE. MEDLINE/PubMed was searched for articles published in English up to February 2019 using the MeSH terms ‘SLE’ and ‘biological therapy/therapies’, or ‘biologicals’. Additional papers were selected from the references included in these articles. This review focuses mainly on meta-analysis, phase II and III randomized clinical trials and observational cohorts. The relevant papers are included in this review.
Pathogenesis of SLE
The underlying pathogenesis in SLE consists of a complex interaction between various genetic and environmental factors. Multiple genes increase the susceptibility for the development of the disease. This susceptibility is modified by the hormonal profile. Environmental factors, including tobacco smoke, infections, and ultraviolet radiation may also trigger the disease. Apoptosis of lymphocytes and excessive neutrophil extracellular trap (NET) formation occur due to defective immune regulatory mechanisms. Abnormalities in the clearance of apoptotic cells and impaired NET degradation result in the production of autoantigens, which are bound by autoantibodies to produce immune complexes. The immune complexes stimulate the plasmacytoid dendritic cells to produce type 1 interferon (IFN) cytokines that have a leading role in the development of SLE.10–12 Type 1 IFNs promote the production of various stimulators by myeloid dendritic cells. These include the production of B lymphocyte stimulator (BLyS) and a proliferation-inducing ligand (APRIL), that are involved in the survival of autoreactive B cells, leading to the generation of pathogenic autoantibodies. In addition, type 1 IFNs induce the production of IL-6 and IL-23 that promote T helper 17 cell responses. This leads to the production of IL-17 that promotes B cell hyper-reactivity, as well as tissue inflammation and damage by recruiting neutrophils, macrophages, and lymphocytes.13,14
Biological targets in RCTs
Biological drugs are complex molecules produced by living cells, that target directly inflammatory cytokines, and immune cells. Biologic drugs that target B cells, T cells, BLyS, IFN-alpha, IL-6 and IL-12/23 have been studied in RCTs in SLE, in view of their known role in its pathogenesis. The details of the completed phase II and III RCTs have been summarized below and in Table 1 according to the drug target.
Table showing completed published phase II and III RCTs of biological drugs in SLE.
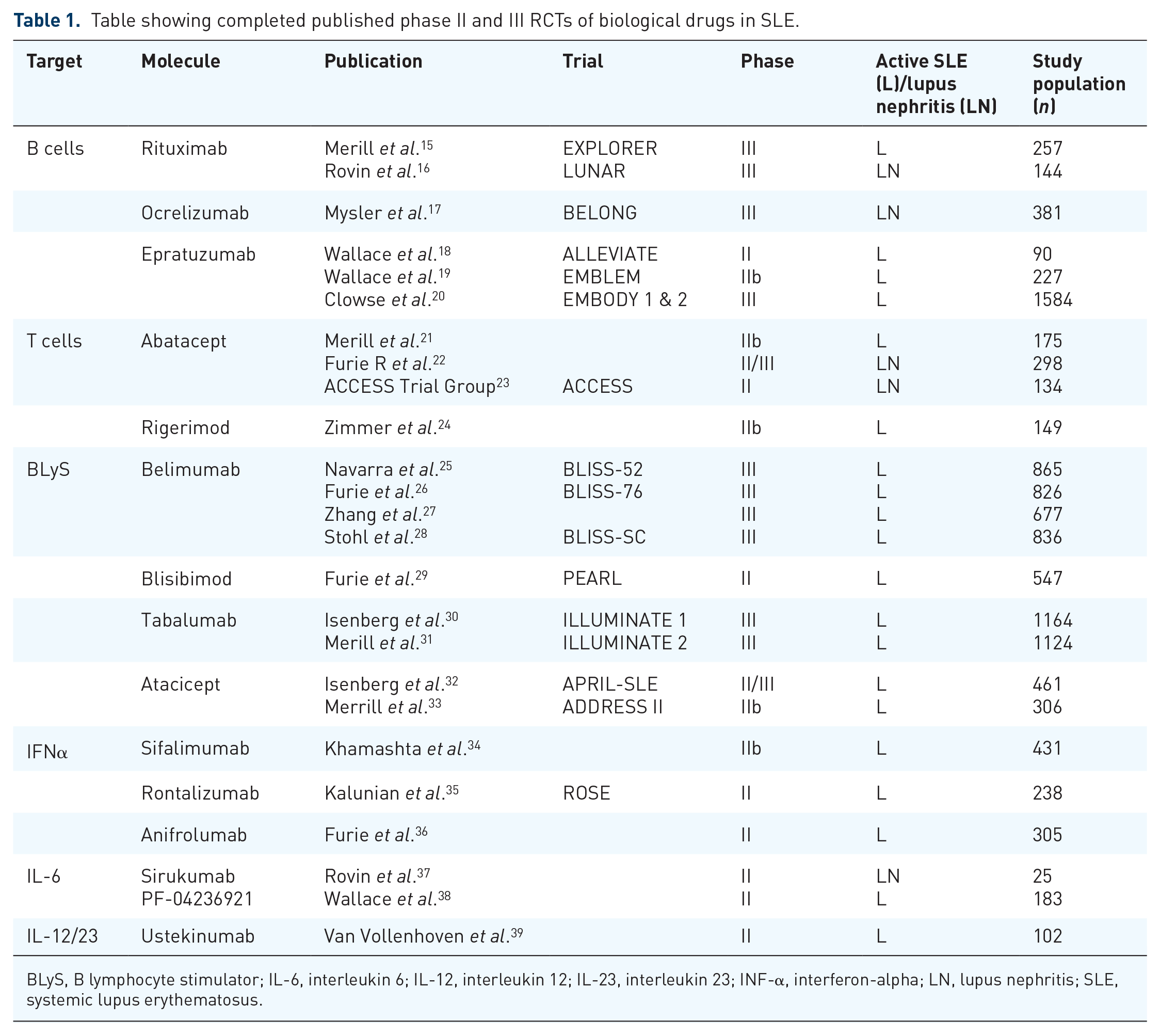
BLyS, B lymphocyte stimulator; IL-6, interleukin 6; IL-12, interleukin 12; IL-23, interleukin 23; INF-α, interferon-alpha; LN, lupus nephritis; SLE, systemic lupus erythematosus.
B cells
Rituximab is a chimeric monoclonal antibody that targets CD20, that is primarily found on B cells. Two phase III RCTs in SLE have been performed, the EXPLORER trial in non-renal disease and the LUNAR trial in renal disease. In the EXPLORER study, patients with moderately active SLE were recruited. 1000 mg rituximab was given at weeks 1, 2, 24 and 26. Patients were allowed azathioprine, methotrexate, and mycophenolate concomitant therapy. At 52 weeks, there was no difference between the treatment and placebo group in the primary outcome measures that included the BILAG score, and in the Lupus Quality of Life (lupus QoL) score. 15 In the LUNAR trial, 144 patients with class III or IV lupus nephritis on mycophenolate were randomized to receive placebo or rituximab, also at a dose of 1000 mg at weeks 1, 2, 24 and 26. In this study, rituximab also failed to achieve the primary endpoint, and there was no significant difference between the placebo and treatment arms, in the proportion of patients who achieved complete or partial renal response. 16
The BELONG trial was a phase III trial on ocrelizumab (an anti-CD20 monoclonal antibody) in class III/IV lupus nephritis. The renal response rates with ocrelizumab were not statistically superior to those with placebo at 48 weeks. 17 The study was terminated early due to an imbalance in serious infections with ocrelizumab. A phase II trial, ALLEVIATE and a subsequent phase IIb trial EMBLEM demonstrated promising results for epratuzumab (an anti-CD22 monoclonal antibody) with significant improvement in disease activity.18,19 Two subsequent phase III trials, EMBODY 1 and EMBODY 2 were performed. These trials included patients with moderate or severe disease activity and excluded patients with active renal or central nervous system (CNS) involvement. This study demonstrated that epratuzumab did not result in improvements in response rates when compared with placebo. 20
T cells
Abatacept is a selective co-stimulation modulator that has inhibitory activity on T cells. A phase IIb trial on non-life threatening manifestations of SLE, and a phase II/III trial on active class III/IV lupus nephritis, assessed the efficacy of abatacept.21,22 Despite the fact these trials did not reach their primary endpoint, abatacept resulted in improvement in some clinical manifestations including fatigue and level of proteinuria. Another phase II trial, the ACCESS trial, assessed the efficacy of a 24 week course of abatacept in conjunction with the Euro-Lupus Nephritis Trial regimen of low dose cyclophosphamide followed by azathioprine for the treatment of active lupus nephritis. In this trial, the primary outcome (the frequency of complete renal response at 24 weeks) was not achieved. 23 A phase III trial studied the efficacy of abatacept in patients with active class III or IV lupus nephritis who had a background of mycophenolate mofetil and corticosteroids. 40 Similar to the other trials, the primary outcome (the frequency of complete renal response at day 365) was not achieved.
Rigerimod modulates the activation of autoreactive T cells by inducing apoptosis. A phase IIb clinical trial evaluated the efficacy of rigerimod in SLE. The results were promising because SRI was significantly higher in the treatment group compared with placebo at 12 weeks. 24 However, no statistically significant improvement was noted in SRI at 52 weeks (primary outcome) in a phase III clinical trial. 41
BLyS
Belimumab is a fully humanized monoclonal antibody that inhibits BLyS. Two phase III trials, BLISS-52 and BLISS-76 have studied the efficacy of intravenous belimumab on active SLE. Both trials excluded patients with severe active lupus nephritis and severe CNS manifestations. Belimumab at a dose of 10 mg/kg resulted in a significantly higher SRI compared with placebo at 52 weeks, thus meeting the primary endpoint of the trials.25,26 Belimumab also resulted in a reduction of flares, reduction of steroid use, and an improvement in the health-related quality of life and level of fatigue. 42 This led to the approval for use of belimumab in SLE. Similar results were obtained in another phase III RCT of intravenous belimumab in patients with active SLE in China, Japan, and South Korea. 27 A further RCT showed a significant improvement in SRI-4 response in patients with moderate to severe SLE at 52 weeks with subcutaneous belimumab. 28 The efficacy and safety of subcutaneous belimumab were confirmed in a 6 month open-label extension study. 43
A phase II randomized controlled trial on the use of blisibimod (a selective inhibitor of BLyS) in moderate to severe SLE, did not reach its primary endpoint at week 24. 29 However, patients receiving the highest dose of blisibimod (200 mg weekly) achieved statistically significant SRI-5 response rates compared with placebo at week 20. Two phase III trials, ILLUMINATE 1 and 2, evaluated the efficacy of tabalumab (an anti-BLyS human monoclonal antibody) in SLE.30,31 The primary endpoint of SRI-5 improvement at week 52 was achieved in ILLUMINATE-2 with 120 mg every 2 weeks after an initial loading dose of 240 mg. A meta-analysis including phase III RCTs of biological agents in SLE showed that belimumab, tabalumab, and epratuzumab had a significant steroid-sparing effect compared with placebo. 44
Atacicept is a recombinant fusion protein that inhibits BLyS and APRIL. A phase II/III trial on the use of atacicept in moderate to severe SLE indicated some benefits with atacicept 150 mg. 32 In this trial, enrolment in the atacicept 150 mg arm was stopped early due to two deaths that were due to infections. In addition, atacicept 75 mg and 150 mg were both associated with reductions in total immunoglobulin levels. Another phase IIb study in active SLE patients, with high disease activity at baseline, showed a statistically significant improvement in SRI response rates at week 24 compared with placebo. 33 However, the primary endpoint of the SRI-4 response at week 24 was not met in the intention-to-treat population.
Interferon-alpha (IFNα)
A phase IIb trial on sifalimumab (an anti-interferon-α monoclonal antibody) in moderate to severely active SLE, demonstrated that SRI response at week 52 (primary endpoint) was higher in the treatment groups compared with placebo. 34 This was statistically significant with the 1200 mg dosage. The efficacy of another anti-interferon-α monoclonal antibody, rontalizumab, in inactive SLE was studied in a phase II study, the ROSE trial. 35 The primary and secondary endpoints of this trial were not met.
Anifrolumab (an anti-interferon-α receptor monoclonal antibody) showed promising results in moderate to severe SLE in a phase IIb trial since the primary endpoint of SRI-4 response and a sustained reduction of oral corticosteroids at week 24 was achieved in the anifrolumab group. 36 Similarly, at week 52 anifrolumab treatment led to significantly higher response rates across multiple endpoints. This was significantly higher in patients with a high interferon signature at baseline. Despite positive results in phase II trials with both sifalimumab and anifrolumab, only the latter was chosen by the pharmaceutical company studying both, to undergo phase III trials. A press release on the results of TULIP 1 phase III trial for anifrolumab indicated that the primary endpoint of SRI4 response at 12 months was not reached. 45 Results from another phase III trial on anifrolumab, TULIP 2 have not yet been published. 46
Interleukin-6 (IL-6)
The efficacy of sirukumab (an anti-IL-6 monoclonal antibody) in active class III or IV lupus nephritis was assessed in a multicenter randomized controlled trial. 37 The treatment did not result in a reduction in proteinuria at week 24 (the primary endpoint). Another phase II RCT evaluated an IL-6 monoclonal antibody, in patients with active SLE. The primary endpoint of SRI-4 at 24 weeks was not achieved. However, a significant improvement in BILAG-BICLA response rate and severe flare reduction was noted. 38
A phase I open-label study assessed the clinical and immunological efficacy of tocilizumab in 16 patients with moderately active SLE. 47 There was a significant improvement in disease activity measured by SLEDAI and SLAM (p = 0.001, p = 0.002) after 14 weeks. A decrease in the neutrophil count was noted particularly with the higher dosage and one patient was withdrawn due to neutropenia. Despite the promising preliminary results in terms of efficacy no further phase II randomized trials have been reported to date to the best of the authors’ knowledge.
IL-12 and IL-23
Ustekinumab is an anti-IL12 and anti-IL-23 human monoclonal antibody. It showed promising results in a phase II RCT in patients with active, seropositive SLE. When compared with placebo, a significant proportion of patients achieved SRI-4 response at 24 weeks with ustekinumab. 39
Clinical experience
Significant data is available in the literature on the clinical experience on the use of rituximab in active SLE. A meta-analysis analyzed 30 open-label studies with a total of 1243 patients. 48 The complete response (CR) rate was 46.7% (95% CI 36.8–56.8%) and 56.6% (95% CI 32.4–78.1%) for studies using BILAG and SLEDAI respectively. The CR in renal lupus was 36.1% (95% CI 25.2–48.6%); partial response was 37.4% (95% CI 28.5–47.3%). This, therefore, demonstrates a discrepancy in the perceived efficacy of rituximab between the RCTs and observational studies. This result is also shown in other cohort studies including both renal and other organ manifestations.49–53 In addition, guidelines by the European League Against Rheumatism and the American College of Rheumatology on the management of lupus nephritis, have recommended the use of rituximab as add-on or monotherapy in class III/IV lupus nephritis patients that do not respond to mycophenolate or cyclophosphamide (level C evidence).54,55
A systematic review analyzed the efficacy of rituximab in non-renal SLE. 56 The review included 26 articles, and a total of 1231 patients who had active disease refractory to steroids and immunosuppressant drugs. The review concluded that the evidence suggests that rituximab can be recommended for organ-specific manifestations including thrombocytopenia and arthritis. In addition, guidelines by the British Society for Rheumatology, recommend that rituximab may be considered in the management of refractory moderate and severe SLE (grade C recommendation). 57 The different results obtained in the cohort studies and in the EXPLORER and LUNAR trials reflect the heterogeneity of SLE and the limitations in the study design of both trials. These include the strict response criteria and the high glucocorticoid doses in addition to immunosuppressive drugs allowed in the trials, potentially masking the rituximab benefit.
The observational studies with belimumab confirmed the findings of the BLISS-52 and BLISS-76 trials. An observational cohort study with an intent-to-treat population of 501 patients, showed that in this population of patients 48.7% had an overall clinical response of ⩾50% improvement from baseline to 6 months. 58 Another prospective observational multicenter cohort study on 195 patients treated with belimumab showed that over 51% of patients had a clinical response at 6 months. These responders had a variety of organ manifestations including rash, arthritis, and renal manifestations. 59 The role of belimumab in lupus nephritis and neuropsychiatric SLE is still unclear because these manifestations have been excluded from the BLISS-52 and 76 trials. Patients treated with belimumab and followed up for 2 years were noted to have a decrease in the number of flares, and damage progression was hindered. 60 Belimumab and rituximab have an acceptable safety profile for SLE treatment, as shown by a meta-analysis. 61
An observational cohort study on the use of etanercept in SLE patients with refractory arthritis followed up 43 patients for a median of 2.3 years. 62 Positive effects were observed on lupus arthritis since 83% achieved clinical remission by week 12. Etanercept was well tolerated and only two patients had significant adverse events due to infections. To the best of the authors’ knowledge RCTs on the use of TNF inhibitors in SLE have not been carried out, probably due to the known rare side effect of drug-induced lupus. 63
Conclusion
Despite the limited biological agents available for current clinical use in SLE, promising results have been obtained by a number of biological drugs in phase II RCTs. These include the drugs that inhibit INF-α; further phase III studies on anifrolumab are ongoing.46,64 Other ongoing phase III RCTs of biological agents in SLE include those on blisibimod and ustekinumab after achieving good results in phase II studies.65,66 These studies provide hope for better treatment of active disease in SLE.
While the results of these trials are anticipated, belimumab and rituximab are the current biological drugs available in the armamentarium for the treatment of SLE. Evidence for the use of belimumab in non-renal SLE is supported by convincing evidence from RCTs. It is effective and well tolerated in daily clinical practice in patients with active SLE. Belimumab decreases the number of flares and the need for glucocorticoids. The role of belimumab in lupus nephritis will become clearer when the results of the ongoing BLISS-LN phase III RCT are published. 67 Observational studies support the role of rituximab in renal and non-renal SLE. Rituximab currently plays a role in lupus nephritis refractory to first-line treatment-mycophenolate and cyclophosphamide. It may also be considered in refractory moderate to severe non-renal SLE. Another ongoing phase III RCT, BLISS-BELIEVE will evaluate the role of rituximab in combination with belimumab for patients with moderate to severe active SLE who do not have severe active lupus nephritis and severe active CNS lupus. 68
Currently, the use of biological agents in SLE is limited, with results from a number of phase II and III RCTs being discouraging. The underlying heterogeneity and multi-system involvement of SLE could explain the difficulty in demonstrating the efficacy of drugs in this condition. In the future, studies should be designed to focus on subsets of SLE patients with specific organ involvement and use appropriate primary outcome measures accordingly.