
Abstract
Periodontitis is an inflammatory disease of dental supporting tissues (gingiva, periodontal ligament, and bone) and it has been suggested as a possible etiology for rheumatoid arthritis (RA). In this systematic review, we aim to verify if periodontitis represents a risk factor for RA. Electronic databases were consulted until March 2018 considering eligibility criteria focusing on: (P, participants) adults; (E, exposure) with periodontitis; (C, comparison) without periodontitis; and (O, outcome) development of RA. Quality assessment of studies and risk-of-bias evaluation were also performed. To undertake a quantitative analysis, the number of persons with RA and a total number of participants for the case group (with periodontitis) and control group (without periodontitis) were used to calculate the odds ratio (OR) with a 95% confidence interval (CI). A total of 3888 articles were identified, and nine studies were considered eligible. Seven of 9 articles suggested an association among diseases by the common pro-inflammatory profiles. The pooled analysis of 3 articles showed a higher RA prevalence for persons with periodontitis (n = 1177) than controls (n = 254) (OR 1.97; CI 1.68–2.31; p < 0.00001). However, considerable heterogeneity among studies was verified (I2 = 96%, p < 0.00001). Periodontitis may represent a risk factor for RA by heredity, bacterial infection, and the pro-inflammatory profile shared between both diseases. Although most of the elective studies report an association between periodontitis and RA, the quantitative analysis showed a high heterogeneity, leading to the need for further studies.
Introduction
Among the inflammatory diseases, periodontitis is one of the most common oral conditions with an inflammatory profile.1,2 This disease is an inflammatory impairment that may mildly affect gingiva, resulting in bleeding, halitosis, and edema, or result in severe damage of dental supporting tissues, promoting damage of the gingiva, periodontal ligament, loss of attachment of alveolar bone and tooth loss.3,4
The pathogenesis of periodontitis is a result of complex interactions between the periodontal pathogens and immune response. 5 Some studies have reported the activity of periodontal pathogens and the presence of inflammatory cytokines [interleukin-1 beta (IL-1β), tumor necrosis factor alpha (TNF-α), and others] in systemic inflammatory diseases. 6 Cardiovascular diseases, such as atherosclerosis, showed associations with periodontitis through inflammatory markers; immune markers also presented in rheumatoid arthritis (RA), 6 especially C-reactive protein and IL-1β.
RA is an inflammatory disease of joints involving an autoimmune attack of periarticular tissues, which may compromise synovial fluids, joints cartilage, and bone integrity. 7 The etiology of RA remains unclear, but the activity of periodontal pathogens has been related to the production of RA autoantibodies. 8 Citrullination of neutrophils and joint tissue proteins performed by Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans is possibly responsible for triggering autoimmune responses and autoantibody production.5,8 This way, the inflammatory pattern of both diseases may possibly trigger events that establish the RA disease in periodontitis patients. 9
In this systematic review and meta-analysis, we aimed to verify whether periodontitis represents a risk factor for the development of RA.
Material and methods
Protocol and registration
This systematic review was registered at PROSPERO under the code CRD42018085004. This study was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines (Supplementary Table 1), 10 adapted by Penoni et al. 11 and Almeida et al. 12
Eligibility criteria, search strategy and data extraction
The PECO strategy was used in this systematic review. Observational studies in humans (P, participants) presenting with periodontitis (E, exposure) and the absence of periodontitis (C, comparison), in which the primary outcome (O) was the development of RA in this population, were considered eligible. The null hypothesis of the study was ‘there is no association between periodontitis and the development of RA.’
The searches were conducted in the following electronic databases, without language restriction, until March 2018: PubMed, Scopus, Web of Science, The Cochrane Library, and LILACS. The gray literature was also searched through OpenGrey and Google Scholar. All publications presented in the databases and gray literature contained a combination of controlled predefined Medical Subjects Headings (MeSH) and free terms relating to periodontitis and RA. Boolean operators (or, and) were used to combine searches (Supplementary Table 2).
All relevant citations were saved in a bibliographic reference manager (Endnote x7 version, Thomson Reuters, Philadelphia, PA, USA). Duplicated results were considered only once. Titles and abstracts were analyzed according to inclusion and exclusion criteria. Additional citations were sought from the analysis of the reference list of all articles previously selected. The selection process was conducted by two examiners (ROF and NCFF) and checked by a third examiner (RRL), in case of disagreements.
After the duplicate removal, opinion articles, technical articles, guides, and animal studies were excluded. The titles and abstracts that did not adhere to the established eligibility criteria were excluded. The resulting articles were evaluated and judged by their full text.
Data extraction
The extraction of data was conducted from the selected articles. A table was used to report year of publication, study design, participant characteristics (source and sample size), age, periodontitis assessment, RA assessment, statistical analysis, and results.
In case of absence of information that makes data extraction or risk-of-bias evaluation impracticable, we attempted to contact the authors by email. The contact consisted of sending a weekly email, for up to 5 consecutive weeks.
Quality assessment and risk of bias
For assessment of methodologic quality and the risk of bias, the Fowkes and Fulton checklist, 13 adapted by Almeida et al. 12 was applied. The checklist has domains that assess study designs and study samples, control group characteristics, quality of measurements and results, completeness, and distortion influences.
To provide valid information and feasibility of methods, the checklist was standardized by the examiners. The sign (++) was applied when the analyzed criteria had a major problem, and the sign (+) was used when the research had criteria with a minor problem. The number ‘zero’ (0) was applied when the analyzed criteria had no problems, and the sign NA was marked when the analysis of the topic was not applicable. The criteria used for quality assessment are listed in Table 1. After a detailed analysis of methods and outcomes, questions of the studies were posed to verify bias, considering: the occurrence of biased results, confusing distortions, and results occurring by chance. The summary questions were: ‘Are the results biased?’; ‘Are confusing factors present in the results?’; and ‘Is there a possibility that the results occurred by chance?’. We attributed the answers ‘Yes’ and ‘No’. If an article received ‘No’ to the three questions, it was considered having a low risk of bias.
Quality assessment and risk of bias according to Fowkes and Fulton. 13

Quantitative analysis
The Review Manager software, version 5.3 (The Cochrane Collaboration, Copenhagen, Denmark) was used in the meta-analysis to evaluate the association between periodontitis and the risk of developing RA. The number of participants with RA, the total number of participants for the case group (with periodontitis) and control group (without periodontitis) were used to calculate the odds ratio (OR) with 95% confidence interval (CI).
A fixed-effects model was applied, and heterogeneity was tested using the I2 index. Sensitivity analyses were conducted to estimate and verify the influence of studies, one by one, on the pooled result. 14 Publication bias was not quantitatively evaluated by the Egger test or funnel plot, as there were not enough studies to be grouped in a funnel plot. 15
The original authors were contacted when further results were required. If, after contact attempts, there was no response from the authors, the study was not included in the meta-analysis.
Results
Study selection and characteristics
A total of 3888 articles were identified from the searches and 793 articles were excluded because of duplication. Titles and abstracts of 3095 potentially eligible manuscripts were verified following the entry criteria resulting from the exclusion of 3079 articles, and 14 articles were selected for full-text reading.
After this step, four studies were excluded due to their evaluation of established cases of RA8,16–18 and due to the inclusion of patients with symptoms of arthralgia. 19 The reasons for exclusion and citations are presented on Supplementary Table 3.
Nine articles were included in this review and their selection process is shown in Figure 1.
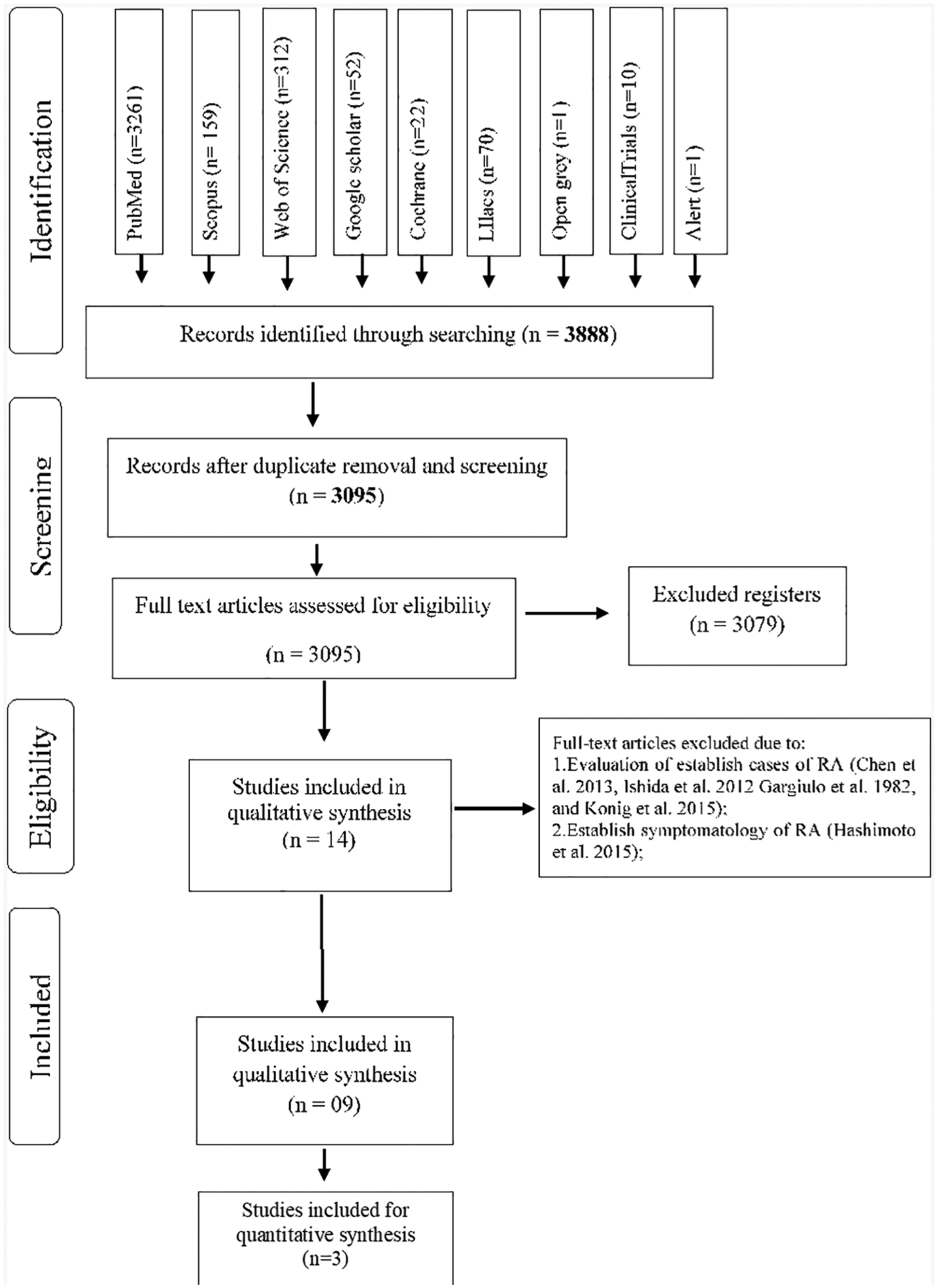
Flow diagram of databases searched according to PRISMA guidelines.
Results of individual studies
Among the nine articles included, two articles present a cohort design,20,21 while seven were cross-sectional studies22–28 (Table 2). The association between the periodontitis and development of RA were cited in seven20,22–27 of nine articles. The absence of association reported was discussed by the authors and it was agreed the reasons were related to the method of periodontitis evaluation.21,28 Dichotomous variables (yes or no/presence or absence) as tooth loss and periodontal surgery were associated with studies with higher sample sizes.20,27 The other seven articles reported relationships between periodontitis and RA, which were grouped by:
Summary of characteristics and results of the included studies.

ACPA, antibodies to citrullinated protein antigens; ADP, advanced destructive periodontitis; anti-CParg, (negative control of CCP); API, plaque index; BOP, bleeding on probing; CAL, clinical attachment level/loss; CCP, anticyclic citrullinated peptide; CEP-1, anticitrullinated α-enolase peptide-1; CI, confidence interval; cit-vim, anticitrullinated vimentin, cit-fib, anticitrullinated fibrinogen; CS, cross-sectional; CPI, Community Plaque Index; DNA, deoxyribonucleic acid; DS, dental scaling; HR, hazard ratio; ICD9-CM, International Classification of Diseases, 9th edition, Clinical Modification; IgM, immunoglobulin M; LA, loss of attachment; MCV, antimutated citrullinated vimentin; MT, missing teeth; non-PD, nonperiodontitis; OR, odds ratio; PD, periodontitis; PI, Periodontal Index; RA, rheumatoid arthritis; REP-1, antiarginine-containing α-enolase peptide-1; RF, rheumatoid factor; RR, relative risk.
(1) Associations provided by regression analysis, relative risk, and odds ratio (OR) of periodontitis diagnosis parameters and occurrence of RA; 20
(2) Associations supplied by laboratory association of periodontitis pathogens and the pro-inflammatory profile of RA;22–24,26
(3) Associations provided by periodontitis diagnosis parameters and pro-inflammatory profile of RA. 27
The periodontal parameters used by the selected studies were tooth loss/missing teeth (MT), probing depth, clinical attachment loss (CAL), bleeding on probing BOP, tooth mobility (TM), radiographic evaluation of periodontitis (PD), recent periodontal surgery, periodontal index (PEI), community periodontal index (CPI), and plaque index (PI). Between those parameters, only four of the selected studies described the evaluated parameters.21,24,25,28
Laboratory parameters of periodontitis consist of immunoglobulin pathogens of P. gingivalis and deoxyribonucleic acid (DNA) assessment of periodontal pathogens. To correlate pro-inflammatory parameters of RA with periodontitis, the studies evaluate the anticitrullinated autoantibodies (Table 2),22,23,27 rheumatoid-factor-immunoglobulin M,23,27 and IL gene polymorphisms 25 related to RA and clinical signs of RA classified by American College of Rheumatologists, 1987.
Risk of bias
The quality of measurements depicted in the articles is shown in Table 3. Among the nine studies, six were classified as a low risk of bias,20,22–25,27 and three as a high risk.21,26,28 The high risk of bias was considered due to lack of information regarding the sampling method and statistical analysis in one study. 26 The other two articles with an increased risk of bias reported a poor periodontal disease, which may result in outcomes possibly converging to a specific direction.21,28
Quality assessment of studies included, according to Fowkes and Fulton. 13
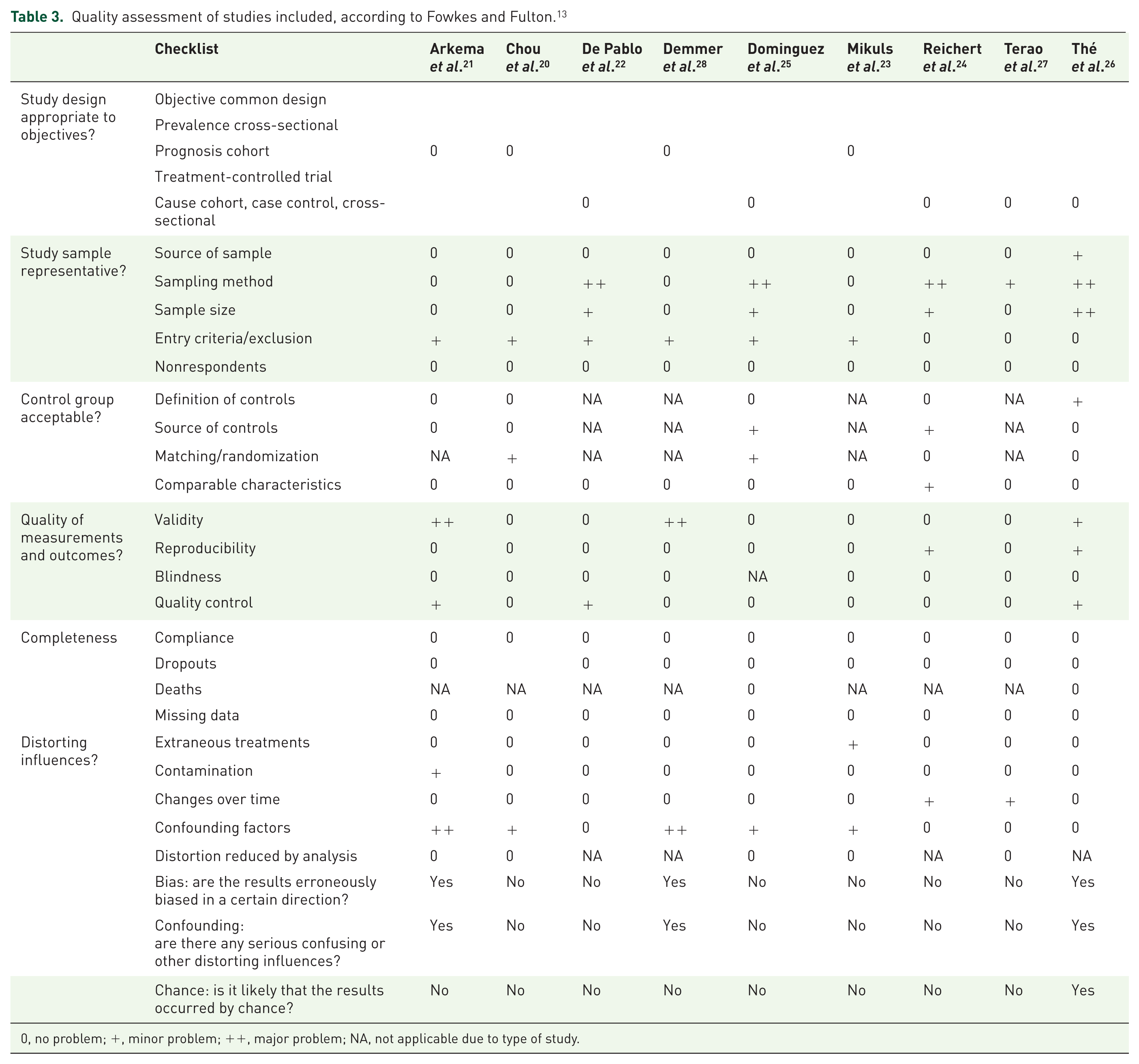
0, no problem; +, minor problem; ++, major problem; NA, not applicable due to type of study.
Qualitative synthesis of studies
Five of nine studies evaluated subsamples of national cohorts.20,21,23,27,28 The countries approached in these studies were Sweden, 21 Denmark, 28 Japan, 27 Taiwan, 20 and the United States. 23 Some studies evaluated the clinical parameters of periodontitis (CAL, BOP, etc.) only for diagnosis, but description of values in text was absent. The other studies evaluated samples using biochemical analysis of rheumatoid factors,22,24,26 and genetic polymorphisms of cytokines associated with RA. 25
Most problems relating to the articles were lack of sampling methods,22,24–26 the entry criteria/exclusion (participants with smoking habits or systemic diseases),20–23,25,28 and small sample size.22–26
The association of periodontitis and RA was found in seven of nine articles.20,22–27 The link was established by comparison of levels of antibodies to citrullinated protein antigens/protein peptides (ACPA)/rheumatoid factor between groups,22–24,26,27 the presence of bacterial DNA on synovial joints,24,26 and the association of the prevalence of two diseases after regression analysis of public health data. 20
Quantitative analysis of studies
Five studies presented their results only in graphics,22–24,26,27 and one study did not provide the total number of patients in case and control groups. 21 Unfortunately, these authors have not returned the contact attempts and were excluded from the meta-analysis. Only three studies were included in quantitative synthesis.20,25,28 Two of these studies were classified as having a low risk of bias,20,25 and one as a high risk of bias. 28
The first meta-analysis of the three studies,20,25,28 indicated a considerable heterogeneity (I2 = 96%, p < 0.00001, Figure 2). The periodontitis group had 630,502 participants, and the control group (without periodontitis) had 172,438 participants. The results showed greater RA prevalence for periodontitis (n = 1177) than controls (n = 254), demonstrating positive association (p < 0.00001) between them (OR 1.97; CI 1.68–2.31).

Forest plot of meta-analysis for three studies (I2 = 96%).
In an attempt to reduce heterogeneity, a sensitivity analysis was performed. Removing studies, one by one, the heterogeneity ranges from 97% to 69%. Therefore, the study of Chou et al. 20 was excluded, and the I2 = 69% was considered.
The second meta-analysis shows two studies.25,28 The periodontitis group had 1874 participants, and the control group had 3596 participants. A result contrary to the first meta-analysis was observed. The results showed lower RA prevalence for person with periodontitis (n = 67) than for controls (n = 137), demonstrating negative association (p = 0.03) between these variables (OR 0.69; CI 0.49–0.97; Figure 3).

Forest plot of meta-analysis for two studies (I2 = 69%).
Discussion
The objective of this review was to identify risk factors related to the association of periodontitis exposure and RA. The qualitative synthesis of nine studies indicates relationships among the diseases (seven of nine studies), but the methodological heterogeneity of our meta-analysis means there is inconclusivity about the association of RA and periodontitis.
Systematic reviews can synthesize and critically evaluate the primary outcomes of investigations through specific strategies to limit bias and random errors. Thus, those reviews can produce supporting information for clinical decisions based on research evidence. In addition to defining key interventions, systematic reviews can also demonstrate ways to achieve decision making where knowledge is lacking. 30
According to the epidemiological aspects of the included studies, four of the chosen studies showed a comparable prevalence of RA in patients with periodontitis. About 3% incidence and a proportion of 3:1 women:men cases were shown. 31 Periodontitis cases have shown an elevated ratio/relative risk for RA development, as demonstrated in other studies. 32
However, some of the selected studies found no correlation between periodontitis parameters and the occurrence of RA.21,28 The evaluation parameters are related to tooth loss, the number of teeth, and recent periodontal surgery. It is well known that periodontitis diagnosis is a criterion correlated with related symptoms (gingival bleeding, halitosis, TM, others), natural heritage, medical history, and clinical signs (gingival recession, root exposure, TM, periodontal pockets with bleeding).3,4 Tooth loss is one of the measurements that demonstrated sensitivity to show a periodontal compromising of dental tissue. 33 Nevertheless, tooth loss can be associated with dental caries and other diseases. So, associations of tooth loss may generate false-negative errors, mainly when previous infections of periodontal tissue is not present in patients. 28
Although, other studies promote synthesis of many related signs of periodontitis using few indices. Hence, the gold standard index, CAL,1,34,35 in a full mouth examination is difficult to execute, time consuming, and unfeasible in larger-sample studies. 36 Therefore, analyzing indices with low specificity may generate misclassifications and weak associations between periodontitis and arthritis. 37
Among the six articles classified as having low risk of bias, the critical aspects to qualify with low risk of bias were: (a) periodontal characterization of the patient’s condition; periodontal conditions are mainly verified through clinical examination, being CAL, BOP, and PD, the most sensitive indices to periodontal evaluation;4,38 and (b) reduction of distortion influences. Matching/randomization and statistical reduction of distortions are essential tools that allow the assessment of study groups with equal probabilities. 39 Mathematical models that simplify the analysis only for chosen evaluated outcomes may reduce other influences like personal habits, systemic diseases, and environmental impacts.
Our meta-analysis shows an important heterogeneity (I2 = 96%, p < 0.00001). One of the articles 20 significantly demonstrates the association of periodontitis with RA development. The sensitivity analysis changed the results of the association between periodontitis and RA in the meta-analysis. This suggests that methodological inconsistencies (as suggested by Demmer et al. 28 ) regarding definition of periodontitis, and fewer proportions of RA/periodontitis patients analyzed (as suggested by Dominguez et al. 25 ), are still present among the studies included in this meta-analysis.
In our analysis, the misclassification of both diseases may lead to errors in outcomes. Therefore, more methodologically similar studies with numerical data and full periodontal analysis are necessary to clarify the real association between these two factors.
Analyzing the topics presented by articles with a positive association, IL-1β and TNF-α were responsible for many immune signaling pathways and protection of infection injuries. 40 Some of these functions are related to the bone remodeling pathway through combination with functions of receptor activator of nuclear-kappa-B ligand and its receptors. In periodontitis, TNF-α and IL-1β are actively present and are secreted by monocytes and macrophages, resulting in effects on the bone remodeling pathway. In cases of inflammatory response against bacterial infection, imbalance of bone remodeling may occur, resulting in the alveolar bone loss. 41
In RA, a systemic increase of TNF-α and IL-1β on gingival crevicular fluid and injured joints was reported, as well as an increase in the periodontal pathogens.40–42 Since then, theories about the developing relationship between RA and periodontitis have been discussed; mainly the two-hit model (periodontitis as a first hit, occasioning inflammation, leading to RA, the second hit). 9 The articles assessed in this review show a critical relationship relating to shared genetic risks involving the cytokine polymorphisms and the human leukocytes antigen–DRB1 allele23,28 as well as the activity of periodontal pathogens.
The HLA-DRB1 allele is responsible for 25–50% of vulnerability to RA and, more recently, authors identified this allele as a mass producer of cyclic citrullinated autoantibody peptides (anti-CCP). 43 These macromolecules are the first epitopes that provoke autoimmune activity by macrophages on joints. 44 The possible association between periodontitis and RA converges to the central hypothesis of the relationship, in which the citrullinated antigens can cause changes in synovial joints. 45
Recent studies have shown the presence of periodontal bacteria DNA in synovial joints of patients with established RA.8,43 Moreover, further authors have associated the formation of immune complexes in synovial joints involving the P. gingivalis, and recently, the A. actinomycetecomitans, 8 the leading Gram-negative periodontal pathogens.
As reported in one of the included studies, 23 cases of periodontitis and presence of HLA-DRB1 expression result in aggravation and a possible development of RA. So, the treatment of RA, a complex investigation of symptomatology, 46 requires another health concern regarding oral pathology aspects. If the two-hit model theory becomes a plausible mechanism of RA development in cases of periodontitis (more studies needed), we suggest a combined treatment involving a careful periodontal evaluation considering different measures (health promotion, health prevention, and surgery interventions) to reduce the clinical signs and symptomatology of periodontitis. 46 Hence, the chance of RA development may be reduced, and the comorbidity in establishing cases of RA can be decreased as well.
The limitations of our study were the absence of research data that share methodological parameters to depict associations between periodontitis and RA. Among the selected articles, two articles that did not find associations directed our finding to inconclusivity regarding our review objective.
Conclusion
The evidence from the included articles suggests a link between RA and periodontitis genetic risks, bacterial infection, and the typical pro-inflammatory profile shared between RA and periodontitis are key to possible RA development. Our meta-analysis, due to high heterogeneity, showed inconclusive results in the association between these two pathologies. So, more studies with representative samples and defined periodontal evaluation are necessary to establish this possible association of clinical relevance of periodontal treatment in prevention of RA.
Supplemental Material
Supplementary_file_1_Table – Supplemental material for Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis
Supplemental material, Supplementary_file_1_Table for Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis by Railson de Oliveira Ferreira, Raíra de Brito Silva, Marcela Baraúna Magno, Anna Paula Costa Ponte Sousa Carvalho Almeida, Nathália Carolina Fernandes Fagundes, Lucianne Cople Maia and Rafael Rodrigues Lima in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
Supplementary_file_2_Table – Supplemental material for Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis
Supplemental material, Supplementary_file_2_Table for Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis by Railson de Oliveira Ferreira, Raíra de Brito Silva, Marcela Baraúna Magno, Anna Paula Costa Ponte Sousa Carvalho Almeida, Nathália Carolina Fernandes Fagundes, Lucianne Cople Maia and Rafael Rodrigues Lima in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
Supplementary_file_3_Table – Supplemental material for Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis
Supplemental material, Supplementary_file_3_Table for Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis by Railson de Oliveira Ferreira, Raíra de Brito Silva, Marcela Baraúna Magno, Anna Paula Costa Ponte Sousa Carvalho Almeida, Nathália Carolina Fernandes Fagundes, Lucianne Cople Maia and Rafael Rodrigues Lima in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
We would like to thank the University of Alberta, Universidade Federal do Rio de Janeiro, and Universidade Federal do Pará for scientific and technical support.
ROF and NCFF performed the searches, data extraction, quality assessment, analysis of results, and manuscript elaboration. RBS and APCPSCA performed analysis of results and manuscript elaboration. MBM and LCM performed quantitative analysis and manuscript elaboration. RRL performed analysis of results and manuscript elaboration.
Funding
This study was financed by UFPA Pro-Rectory of Research and Postgraduate (PROPESP-UFPA) and Brazilian National Council for Scientific Research and Development (CNPq) through Coordination for Improvement of Higher Education Personnel program - Finance code 001. The government funding agencies had no role in study design, manuscript elaboration, authors decisions, or manuscript approval for publication.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.