
Abstract
Background:
‘Unsafe’ movement strategies used to perform everyday activities were quantified using scores for tasks included in the Short Form Safe Functional Motion test series (SSFM). Baseline scores were independently associated with incident fractures after adjusting for factors known to effect fracture risk. The purpose of the present study is to determine whether the SSFM, a series of tests of habitual motion, is associated with incident fragility fracture at any skeletal sites.
Methods:
An osteoporosis clinic database was queried for adults with baseline SSFM scores and corresponding data for prevalent fractures, femoral neck bone mineral density (fnBMD), osteoporosis medication use, and incident fractures at 1-year and 3-year follow ups [n = 1700 (118 incident fractures) and n = 1058 (202 incident fractures), respectively]. Multiple logistic regressions, adjusted for sex, age, fnBMD, osteoporosis medication use, and any prevalent fractures at baseline, were used to determine whether baseline SSFM scores were associated with incident fragility fractures.
Results:
An Sfm-3 score was a significant independent predictor of any fracture at 1 year [adjusted odds ratio (95% CI) = 1.118 (1.025, 1.219) for each 10-point decrease in Sfm-3; p = 0.012], and 3-year follow up [adjusted odds ratio (95% CI) = 1.183 (1.098, 1.274) for each 10-point decrease in Sfm-3; p < 0.0001].
Conclusions:
Scores on the SSFM predict fracture risk such that for each 10-point drop in score the odds of fracture are increased by up to 18% independent of risk associated with age, bone mineral density, use of bone-sparing medications, and history of a fracture.
Introduction
Within the literature on predictive tools of fracture risk, gaps exist and further validation of existing measures is necessary. For example, areal bone mineral density (aBMD) measured by dual-energy X-ray absorptiometry (DXA) is an important predictor of fragility fracture, and T scores derived from these measures form the basis for the clinical diagnosis of osteoporosis.1,2 A systematic search of the literature identified 12 tools to predict fracture risk in women that were externally validated. However, only six of these were validated in a population-based setting with proper methodological quality. 3 Of the 12 externally validated tools, the most common clinical risk factors (CRFs) were age, body weight, prior fractures, and maternal history of fractures. 3 Regardless of whether aBMD was included, the predictive accuracy for fracture risk was similar for complex and simple tools. 3 The FRAX® diagnostic tool (University of Sheffield, Sheffield, South Yorkshire) integrates CRFs with femoral neck bone mineral density (fnBMD) for men and women aged 40–90 years to predict the probability of hip fracture and major osteoporotic fracture in a 10-year timeframe. 4 Using data from the Study of Osteoporotic Fractures, fracture risk assessment was similar whether using the FRAX® tool with or without aBMD. 5 FRAX® does not account for fall risk or unsafe movement behaviors. 6
Evidence suggests that habitual physical activities and associated movement patterns contribute a functional risk for fragility fracture.7–11 Movement patterns can reflect significant balance impairment for fall risk and reveal spine flexion behaviors with coinciding loading of vertebrae that may increase risk for a vertebral compression fracture (VCF). 8 Loss of strength and flexibility in the lower extremities may be compensated by use of the back muscles for lifting. In the Global Longitudinal Study of Osteoporosis in Women (GLOW) cohort more than half of vertebral fractures and 22% of other fragility fractures were unaccounted for by a fall, trip, or slip. 10
Only four externally validated CRF tools include questions about falls, three of which include questions about physical performance. 3 The Fracture and Mortality (FRAMO) Index questionnaire encourages the person to attempt the task (rise from a chair five times without using arms) before providing a ‘yes’ or ‘no’ response regarding ability. 12 Associations exist between scores on self-reported and performance-based measures of physical function in people with osteoporosis, but each of these types of measures provides unique information.13,14 The few studies that have investigated the relationship between observed physical function and fragility fractures at the spine7–9 and hip 9 suggest that assessment of functional risk adds important information. Prior research is significant for Safe Functional Motion test (SFM-10) prediction of prevalent fractures and incident vertebral fractures.8,9 The primary focus of the present study is to determine whether SSFM predicts incident fragility fracture risk at any skeletal site, and secondarily if it is consistent in its ability to predict incident vertebral fracture risk.
Methods
Study design, procedures, and participants
We conducted a retrospective review of anonymized charts for adults who attended an osteoporosis specialty clinic in northeast Georgia between 2004 and 2014 for initial assessment and had 1-year and 3-year follow-up data in the clinic’s database registry. The Northeast Georgia Medical Center’s Institutional Review Board approved the protocol. Both men and women were included if they had baseline data for Sfm-3 and covariates of interest including age, sex, fnBMD, history of fragility fractures as assessed by trained medical personnel including aBMD, and X-rays, and use of osteoporosis medication. Patients must have been followed for at least 1 year (for the 1-year analyses) and 3 years (for the 3-year analyses). Patients were included only if all the variables of interest were present in our database.
Participants read and signed confidentiality and privacy forms consistent with the US Health Insurance Portability and Accountability Act and provided written informed consent allowing their de-identified data to be used for research and quality improvement purposes.
Measures
Bone mineral density
aBMD of the spine and hip neck and total was determined using GE Lunar Prodigy/Advance scanner No. 41310 DXA as the standard of care on all patients attending the osteoporosis clinic within 6 months of the initial SFM test. Data for the right hip fnBMD was used if the left hip fnBMD was unavailable. Certified radiology technicians performed all DXA testing on site. Standardized protocols recommended by the manufacturer were followed to perform clinical scans and regular quality assurance scans to confirm stable calibration over time. We selected fnBMD over spine aBMD to avoid the potential for artifacts in the spine scans and the variability in the region of interest introduced by the presence of a fracture in the lumbar spine.
Age, sex, bone-sparing medication use, and fracture history
Self-reported age, sex, history of fragility fracture sustained under low-trauma conditions prior to the baseline SFM test date, and use of bone-sparing medication use were documented. Fractures reported to occur after age 40 and prior to the baseline SFM at any skeletal site, excluding the fingers, toes, clavicle, scapulae, and/or skull and not due to trauma, were recorded as prevalent fractures. The fracture report for nonvertebral and hip fractures were self-reported and by review of electronic medical records for the corresponding hospital networks in the region. VCFs were evaluated by X-rays taken at baseline and yearly for 3 years. Use of osteoporosis medication was defined as whether or not a person started taking osteoporosis medication between 1 year prior to the baseline assessment and 1 day before an incident fragility fracture. For those who did not have an incident fragility fracture during the follow-up period, use of osteoporosis medications was defined for the period between 1 year prior to the baseline assessment and throughout the follow-up period. Participants using osteoporosis medications were taking one or a combination of the following: pamidronate, risedronate, ibandronate, etidronate, raloxifine, teriparatide, alendronate, calcitonin, and zoledonic acid.
SFM test
A trained and certified tester administered and scored the SFM according to the standardized testing procedures described previously. 9 For safety, the person being tested wears a transfer belt around the waist for the duration of testing, and the maximum weight lifted during any single task is limited to 10 pounds. A task was not performed if it was not completed within the past 6 months, as the purpose of this test is to evaluate habitual movement patterns and it asks the person to do only movements that are part of their normal life routine. The average time required to complete the SFM-10 long version is 25 minutes while the Sfm-3 version is 5 minutes. The full SFM consists of 10 tasks (pouring liquid, sweeping the floor, using a washer, using a dryer, taking on/off footwear, picking up a newspaper, reach–lift, sit-to-floor, carry–climb, night-walk) with one of the goals of the current study to reduce the number of measures while not sacrificing the predictive utility of the remaining measures.
The SSFM allows a quick test of habitual motion tasks often conducted in daily activities and includes three of the 10 original SFM tasks. The tasks include: (1) sit-to-floor task whereby participants sit on the ground, extend their feet in front of them, and then return to a standing position; (2) carry–climb task whereby the participant must step up onto and over a block while carrying a weighted bag (no more than 10 pounds); and (3) night-walk task simulating walking in a low-light environment on compliant and noncompliant surfaces. The points for task components are summed and divided by all possible points to calculate a percentage score varying from 0 to 100, where 0 represents unsafe, impaired functional motion and 100 represents safe, optimal functional motion. The use of the SSFM items were selected as they performed as well as the full SFM long and are parsimonious in administration.
Incident fragility fracture
The occurrence of an incident fragility fracture was recorded during follow-up visits. VCF was determined by X-ray at baseline and yearly assessment as defined by a 20% or greater morphometric reduction in vertebral height. Nonvertebral fractures were self-reported and/or review of electronic medical records. Patients reporting a fracture between baseline and 1-year follow up and those with no new fracture during this period were included in the 1-year follow-up analyses. Patients reporting a fracture between baseline and 3-year follow up and those with no new fracture during this period were included in the 3-year follow-up analyses.
Statistical analyses
Associations between SFM score and incident fragility fracture at any site, and between each SFM score and incident VCF, were examined using multiple logistic regression analyses. The model for each multiple logistic regression analysis was constructed to include known predictors and control for potential confounders, specifically age, sex, fnBMD, use of osteoporosis medications, and history of a fragility fracture after age 40 but prior to the baseline SFM test. For the outcome of incident fragility fracture at any site, the history of fracture is defined as a fragility fracture at any site including VCF, whereas for the outcome of incident VCF, the history of fracture is defined as a VCF.
Participants with no incident fracture were expected a priori to have higher scores on the SSFM compared with participants who had an incident fragility fracture. 9 In addition to SSFM, other known predictors of fracture and potential confounders (age, sex, fnBMD, use of bone-sparing medications, and prevalent fractures at baseline) were included in the multiple logistic regression models for determining the odds ratio for incident fracture at any skeletal site and at the spine specifically.
Each logistic regression analysis was constructed to model the occurrence of an event (history of one or more fragility fracture or VCF, as applicable). Age, fnBMD, and SSFM score were entered as continuous data. Sex, history of fracture, and use of bone-sparing medication were entered as categorical variables with ‘Female’, ‘No history of fragility fracture’, and ‘Yes use of bone-sparing medications’ entered as the reference categories, respectively. For meaningful presentation, the odds ratios are reported using a 10-year unit (increase) for age, a 10-point unit (decrease) for SSFM score, and a 0.10 g/cm2 unit (decrease) for fnBMD. Assessment of goodness of fit of each model using the Hosmer-Lemeshow test. p values less than or equal to 0.05 were considered statistically significant. Statistical analyses were conducted using SAS Version 9.1.3 (Cary, NC).
Results
Participant characteristics
During the study period, 1700 adults attended the clinic for an initial SFM test and had data available on all outcomes and covariates of interest at 1 year, and 1058 adults were eligible for inclusion at the 3-year follow up. Full discussion of the sample may be found in MacIntyre et al. 8 The characteristics of the participants are summarized in Tables 1 and 2. By the 1-year follow up, 118 new fragility fractures were recorded as hip (n = 2), vertebral (n = 82), and other skeletal site (n = 34) and were reported by 118 fractures (6.9%) of the 1700 patients. By the 3-year follow up, 207 new fragility fractures recorded as hip (n = 7), vertebral (n = 149), and other skeletal site (n = 51) were reported by 202 (19.1%) of the 1058 patients.
Demographic characteristics for analyses of incident fracture at any site.

Includes incident and previous fractures that occurred after age 40. Adjusted for age. Fractures of digits and skull are not included. Percentages in the Incident/No Incident Any Fracture columns are based on the totals in the All column. Percentages in the All column are based on the total sample of 1700.
fnBMD, femoral neck bone mineral density; SD, standard deviation; SFM-3, Short Form of the Safe Functional Motion test.
Demographic characteristics for analyses of incident vertebral fracture.
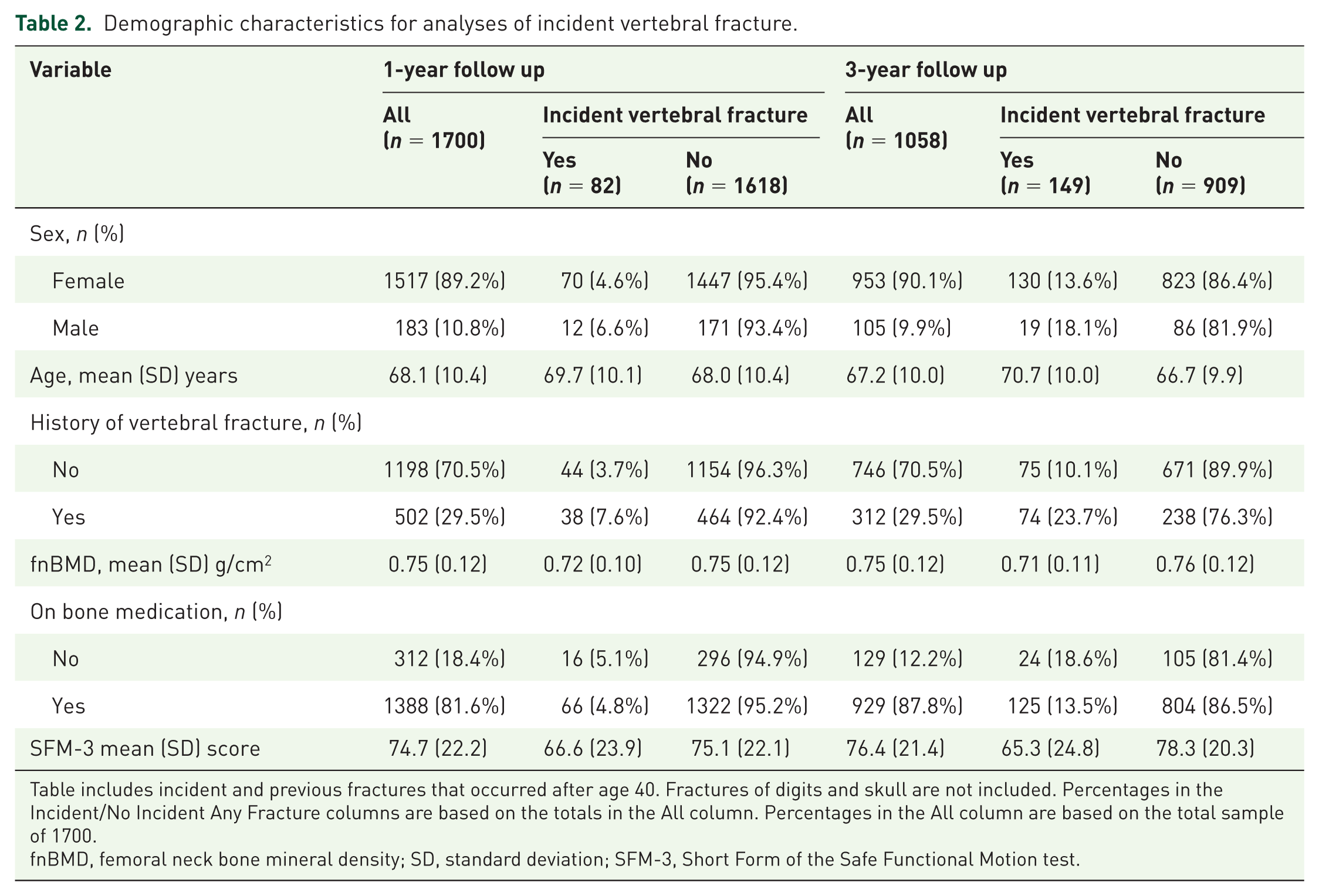
Table includes incident and previous fractures that occurred after age 40. Fractures of digits and skull are not included. Percentages in the Incident/No Incident Any Fracture columns are based on the totals in the All column. Percentages in the All column are based on the total sample of 1700.
fnBMD, femoral neck bone mineral density; SD, standard deviation; SFM-3, Short Form of the Safe Functional Motion test.
SSFM score and incident fragility fracture at any skeletal site
Table 3 summarizes the results for the multiple logistic regression models, adjusted for covariates known to predict osteoporotic fracture, demonstrating the association between SSFM score and incident fracture at 1- and 3-year follow up. For each 10-point decrease in SSFM score (less ‘safe’ motion), the odds of having a fracture increased by 12% (p = 0.012) at 1-year follow up. At the 3-year follow up, the odds of having a fracture increased by 18% for each 10-point decrease in SSFM score (less ‘safe’ motion, p < 0.0001). This risk was adjusted for the increased odds of fracture associated with fnBMD (odds of fracture increased by 31% for each 0.1 gm/cm2 decrease; p < 0.001) and age (odds of fracture increased by 22% for each 10-year increase in age; p < 0.03) at the 3-year follow up. For this cohort, sex, history of prevalent fracture at baseline, and use of bone-sparing medication were not significantly associated with incident fragility fracture at any skeletal site at either 1- or 3-year follow up (Table 4). This compares favorably with a 10-point increase in SFM-10 score association with VCF of 18% decrease at 1 year and 27% decrease at 3 years found in past research using these data. 8
Logistic regression model analyzing the association between baseline score on the Short Form of the Safe Functional Motion test (SFM-3) and incident fracture at any skeletal site at 1-year and 3-year follow up adjusted for factors known to influence fracture risk assessment.

Hosmer-Lemeshow goodness of fit χ2 = 4.443, p = 0.815 (n = 1700).
Odds ratio reported is for each 10-year increase in age.
Odds ratio reported is for each 0.10g/cm2 decrease in femoral neck bone mineral density (fnBMD).
Odds ratio reported is for each 10-point decrease in SFM-3 score.
Hosmer-Lemeshow goodness of fit χ2 = 7.474, p = 0.486 (n = 1058).
Logistic regression model analyzing the association between baseline score on the Short Form of the Safe Functional Motion test (SFM-3) and incident vertebral compression fracture (VCF) at 1-year and 3-year follow up adjusted for factors known to influence fracture risk assessment.

Hosmer-Lemeshow goodness of fit χ2 = 9.424, p = 0.308 (n = 1700).
Odds ratio reported is for each 10-year decrease in age.
Odds ratio reported is for each 0.10 g/cm2 decrease in femoral neck bone mineral density (fnBMD).
Odds ratio reported is for each 10-point decrease in SFM-3 score.
Hosmer-Lemeshow goodness of fit χ2 = 5.245, p = 0.731 (n = 1058).
Note: The odds ratios and 95% confidence intervals (CIs) were the same; however, the CIs were different. 1.183 (1.098, 1.274) for any fractures at year 3, and 1.183 (1.090, 1.285) for vertebral fractures at year 3.
SSFM score and incident VCF
Table 4 summarizes the results for the multiple logistic regression models, adjusted for covariates known to predict osteoporotic fracture (all patients in this study were osteoporotic), demonstrating the association between SSFM score and incident VCF at 1- and 3-year follow up. At the 1-year follow up, the odds of incident VCF increased by 12% for each 10-point decrease in SSFM score (less ‘safe’ motion). This risk was adjusted for the increased odds of fracture associated with prevalent VCF at baseline (odds of fracture increased by 72%; p < 0.05). At the 3-year follow up, the odds of having a fracture increased by 18% for each 10-point decrease in SSFM score (less ‘safe’ motion, p < 0.0001). This risk was adjusted for the increased odds of fracture associated with prevalent VCF (odds of fracture increased by 97%; p < 0.001), fnBMD (odds of fracture increased by 29% for each 0.1 g/cm2 decrease; p < 0.01) at baseline and medication use (94% increase in odds; p = 0.01). For this cohort, sex, and age were not significantly associated with incident VCF at either 1- or 3-year follow up (Table 4).
Discussion
Functional status is a component of fracture risk independent of bone mineral density and historical risk factors. SFM scores stratify safety of movement patterns involving spine flexion, muscle strength and flexibility, and balance to provide information on functional risk for fracture. Prior studies have shown a strong relation of SFM for predicting fragility fractures based on history profiles at any site and for predicting incident VCF. The current study is a parsimonious reduction of the original 10-item SFM tasks into a three-item measure used to predict the odds of incident fracture across 12 and 36 months. See MacIntyre et al . 8 for full information on the SFM-10.
The SSFM allows clinicians and therapists quick determination of functional risk for fracture by observing standard movement patterns as classified by safe or unsafe. In the present study, higher scores on the SFM test indicate safer movement and a reduced risk of fracture at 1- and 3-year time points.
Patients having an incident fracture at any site was remarkable for only 6.9% at 1 year and 19.1% at year 3. Age, fnBMD and SSFM were statistically significant at year 3. VCF was the most common incident fracture representing 69% of incident fractures at year 1 and 74% of incident fractures at year 3. VCF assessment was evaluated by yearly X-rays from baseline to year 3. SSFM, history of VCF, fnBMD, and use of bone-sparing medications were significant factors of incident VCF at the 3-year analyses.
It is unclear why prior incident fractures or use of bone-sparing medications were not significant factors for any fracture as was noted for VCF. However, it may be related to patient reported nonvertebral fracture versus morphometric identification for VCF. There were a lower number of fractures at year 1 versus at year 3. Furthermore, most patients were on bone-sparing medications. At year 1, 82% of patients were on bone-sparing medications, whereas 88% were on bone-sparing medications at year 3. These bone-sparing medications typically have a better fracture reduction at 3 years versus at 1 year, especially at nonvertebral sites. VCF reductions at year 1 may be more pronounced with these medications.
The assessment of functional risk for fracture by SFM testing provides additional information beyond bone density and historical risk factors to assess fracture risk. This information can allow practitioners to have additional information to assess fracture risk and design treatment and interventions to reduce fracture risk.
Conclusion
The current study used a sample of 1700 patients within a single medical practice in the Southeastern United States. Females were the majority of participants at 90% and may not be generalizable to the overall population of fracture patients. This study should be repeated among other samples, and compared and contrasted with other fracture prediction tools. Medications were given on a clinical basis in a real-world setting. The present study grouped osteoporosis medications according to current use or not, and did not include delineations for specific categories of bone medications such as antiresorptive versus anabolic. We did use self-reported fracture data for historical nonvertebral sites that may have introduced bias and misreporting of fractures. To mitigate this, we electronically verified records for fractures.15,16 Further study regarding fracture outcomes from a combined risk of aBMD, SFM, and historical risk factors would be of benefit.
Footnotes
Authors’ note
Chris P. Recknor and Stephanie L. Grant developed the Bone Safety Evaluation (US patent 7556045 - System and method for osteoporosis assessment), of which the SFM is a part. This study was presented in part at the Annual Meeting of the American Society for Bone and Mineral Research in Houston, Texas, on September 14, 2014. Please contact Chris P. Recknor for potential access to underlying research materials.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Daniel Van Dussen and Norma MacIntyre declare that they have no conflicts of interest. The other authors declare that they have no conflicts of interest.
Ethical approval
The Northeast Georgia Medical Center’s Institutional Review Board approved the protocol.