
Abstract
Osteoporosis and resulting osteoporotic fractures are responsible for significant morbidity, excess mortality, and health care costs in the developed world. Medical therapy for osteoporosis has been shown in multiple randomized controlled trials to reduce the risk of vertebral and non-vertebral fractures and hip fractures, and in some studies bisphosphonate medications have been associated with improved survival. Although the overall benefit to risk ratio of osteoporosis medications remains favorable, there have been concerns raised about the long-term safety of these treatments. Atypical femur fracture, which is a rare type of fracture that has been associated with the long-term use of potent antiresorptive bone medications, is a potentially devastating consequence of osteoporosis treatment. This paper reviews our current understanding of atypical femur fractures, their relationship to antiresorptive osteoporosis medications, and proposed strategies for management, in order to inform clinical decision making about the optimal use and duration of medical therapy for the treatment of patients with osteoporosis or at high risk for osteoporotic fractures.
Antiresorptive osteoporosis medications
Antiresorptive medications, specifically the aminobisphosphonates (alendronate, risedronate, zoledronic acid) and the RANK ligand inhibitor denosumab, are potent inhibitors of osteoclast activity. They are the most commonly used first line therapies worldwide for the treatment of osteoporosis and the reduction of fracture risk. 1 These medications are widely prescribed and are generally well tolerated. Although the initial randomized controlled trials of oral and intravenous (IV) bisphosphonates and denosumab indicated a favorable safety profile, once they were in widespread use, reports of rare risks associated with long-term use began to appear. 2
The potent bisphosphonates have been approved to treat osteoporosis and to reduce the risk of low trauma fractures since 1995, when alendronate was first approved for use. They remain first-line therapies in all major clinical practice guidelines for the treatment of osteoporosis, as randomized controlled trials have demonstrated reduction in risk for vertebral, non-vertebral, and hip fractures in postmenopausal women, men, and in glucocorticoid induced osteoporosis. Initial studies documented adverse effects including gastrointestinal upset, musculoskeletal pain, acute phase reaction, and esophagitis. 2 Subsequent to their widespread adoption for the treatment of osteoporosis, rare but serious adverse events were reported, specifically atypical femur fracture (AFF) and osteonecrosis of the jaw (ONJ).3,4 ONJ is more common in those taking high dose IV bisphosphonates in the context of cancer treatment, but it remains extremely rare in patients who are treated with standard osteoporosis dosing of bisphosphonates. AFFs, although still rare, are increasingly recognized as occurring far more frequently than ONJ, both in those treated with high dose bisphosphonates for malignancy, and in those treated with bisphosphonates for osteoporosis.
Denosumab, an inhibitor of RANK ligand, is a highly potent antiresorptive medication which has been shown in randomized controlled trials to be effective in improving bone mineral density and reducing the risk of vertebral, hip and non-vertebral fractures women with osteoporosis 5 and in glucocorticoid users. 6 Denosumab, given as a 60 mg injection once every 6 months, is generally well tolerated. In the FREEDOM study, where denosumab used for 3 years was compared with placebo, and in the subsequent extension, where denosumab was continued for up to 10 years, the risk of serious adverse events was similar between the placebo group and treated patients,7–9 although hypocalcemia remains an important risk with denosumab, particularly when used at high doses (for malignancies) and in patients who are at risk for hypocalcemia, such as in chronic kidney disease. Although there were no initial reports of ONJ or AFF, these complications have been seen, although infrequently, in denosumab extension studies. 8 Subsequent case reports have documented AFF and ONJ with denosumab treatment, in those who have and who have not had prior bisphosphonate treatment. 10
AFF and ONJ have received widespread attention in the medical literature and in the lay media and have led physicians and patients to question and even discontinue osteoporosis medications, leading to an increasing care gap in osteoporosis management. To address this, there have been task force reports and guidelines published which address safety concerns and propose an approach to the use of bisphosphonate and denosumab therapy, and the optimal duration of treatment, in those at high risk for fracture.3,11
Definition of AFF
AFFs are stress type fractures originating in the lateral shaft of the femur. They occur with minimal or no trauma and have specific radiographic findings. This type of fractures can occur in those who are taking antiresorptive osteoporosis medications, as well as in those who are not. After initial case reports about AFFs associated with long-term bisphosphonate use were published, the American Society for Bone and Mineral Research (ASBMR) convened a task force. The first task force report, published in 2010, developed a case definition for AFF 3 for use clinically and in research. The authors of this first report concluded that AFFs are fundamentally different from common osteoporotic femur fractures, and this strongly suggests a distinct pathogenesis.
The second ASBMR task force report on atypical femur fractures was published in 2014. 11 The revised AFF case definition described AFFs as occurring below the lesser trochanter and above the supracondylar flare, and pathologic fractures were excluded. This revised definition included criteria for the diagnosis of incomplete as well as complete AFFs. Four out of five major features need to be met in order for a fracture to be classified as AFF (Figure 1). This is because, for complete AFF, X-rays are often less than optimal in the emergency setting so cortical reaction and beaking may be difficult to appreciate, and in the case of incomplete AFF, they would not be expected to extend from the lateral to the medial cortex. Minor features for AFF were also identified, but not required for the case definition. These minor features highlight the findings that prodromal symptoms, specific femur radiographic features, and bilateral fractures are commonly seen in patients with AFF. Importantly, these features may be identified prior to a complete fracture occurring, when interventions to prevent a complete fracture can be instituted.

American Society for Bone and Mineral Research case definition for atypical femur fracture. 11
Incidence of AFF
Unusual stress fractures associated with osteoporosis in premenopausal women were first described by Richardson and colleagues in a case report in 1978, 12 before highly potent bisphosphonates were in use. In 1985, Orwoll and McClung described a similar type of stress fracture in patients with low bone turnover osteoporosis. 13 After bisphosphonates were approved in the USA for the prevention and treatment of osteoporosis, there was widespread use of these medications from the mid 1990s. In 2005 Odvina and colleagues published a paper reporting on nine patients who had spontaneous non-spinal fractures while taking alendronate, and four of those were femur fractures. 14 These authors concluded that their findings raised the possibility that severe suppression of bone turnover may lead to fractures during long-term alendronate therapy. These femur stress fractures became known as AFFs.
In 2011 Wang and Bhattacharyya published an analysis of typical femur fractures and AFFs associated with bisphosphonate use in the USA in the decade after bisphosphonate medications were introduced. They estimated that with bisphosphonate therapy, for every 100 typical osteoporotic femur fractures that were prevented, there was an increase of one subtrochanteric fragility fracture. 15 In another analysis, Meier and colleagues found a 47% reduction in classic fractures, but increased risk of AFF of 10.7% per year, with long-term bisphosphonate use. 16 These authors also found that longer duration of bisphosphonate treatment was associated with a higher risk of AFF. In this study, contralateral fractures were seen in almost one-third of patients who presented with an AFF.
Subsequent large epidemiologic studies have confirmed the association between bisphosphonates and AFF and have helped to determine the incidence of these rare clinical events. A study from the Institute for Clinical Evaluative Sciences in Ontario, Canada, using administrative data, estimated that the incidence of AFF is 1–2 per 1000 patient-years after 6–7 years of continuous bisphosphonate treatment. 17 Dell and colleagues, using data from Kaiser Permanente in California, estimated a risk of AFF of 1 per 1000 patient-years after 8–9.9 years of continuous bisphosphonate use. 18 Dell also demonstrated a significant increase in risk after 8 years of continuous bisphosphonate use, as compared with a shorter duration of treatment. Subsequently, in a systematic review, Gedmintas and colleagues concluded that bisphosphonate exposure was associated with an increased risk of AFF, with an adjusted relative risk of 1.70. 19
AFFs have also been reported in patients treated with denosumab. In the FREEDOM trial extension, in which postmenopausal women had not had prior oral bisphosphonates for more than 3 years and were off of bisphosphonates for 12 months prior to enrollment, the incidence of AFF was low in those treated with long-term denosumab, with one case seen in each group in the 10 year follow up study. 8 The incidence of AFF with denosumab treatment remains uncertain, as many patients in the real world who take denosumab have previously been treated with bisphosphonates.20,21 Nonetheless, AFFs have been reported in those taking denosumab who have had no past treatment with other osteoporosis medications, both in those taking high dose denosumab for malignancy 22 and in those taking denosumab for osteoporosis.
Pathogenesis of AFF
The pathogenesis of AFF remains poorly understood, although a number of mechanisms have been proposed. Radiologic features seen in AFF are consistent with stress fractures (Figure 2), which occur when bones are subjected to repetitive loading that overwhelms the capacity for bone repair. Antiresorptive medications, which suppress bone remodeling, may result in accumulation of micro-damage which is not repaired, thus leading to the development of stress fractures. Differences in hip and lower limb geometry may play a role in the development of AFF, and in particular may determine where in the femur stress fractures will occur. Studies have identified that variations in the shape of the femur, including varus hip angle, bowleg deformity, and small femoral shaft diameter, may determine the areas of greatest stress in the femur. This may determine where the stress changes can lead to subsequent fractures.23–26 Bisphosphonate medications also have an impact on bone material properties including collagen and advanced glycation end-products, and long-term bisphosphonate use results in increased tissue mineral density, which may enable crack propagation after development of a stress fracture. 27 Finally, there may be a genetic predisposition which makes individuals who receive antiresorptive medications more susceptible to developing stress changes in the femurs.
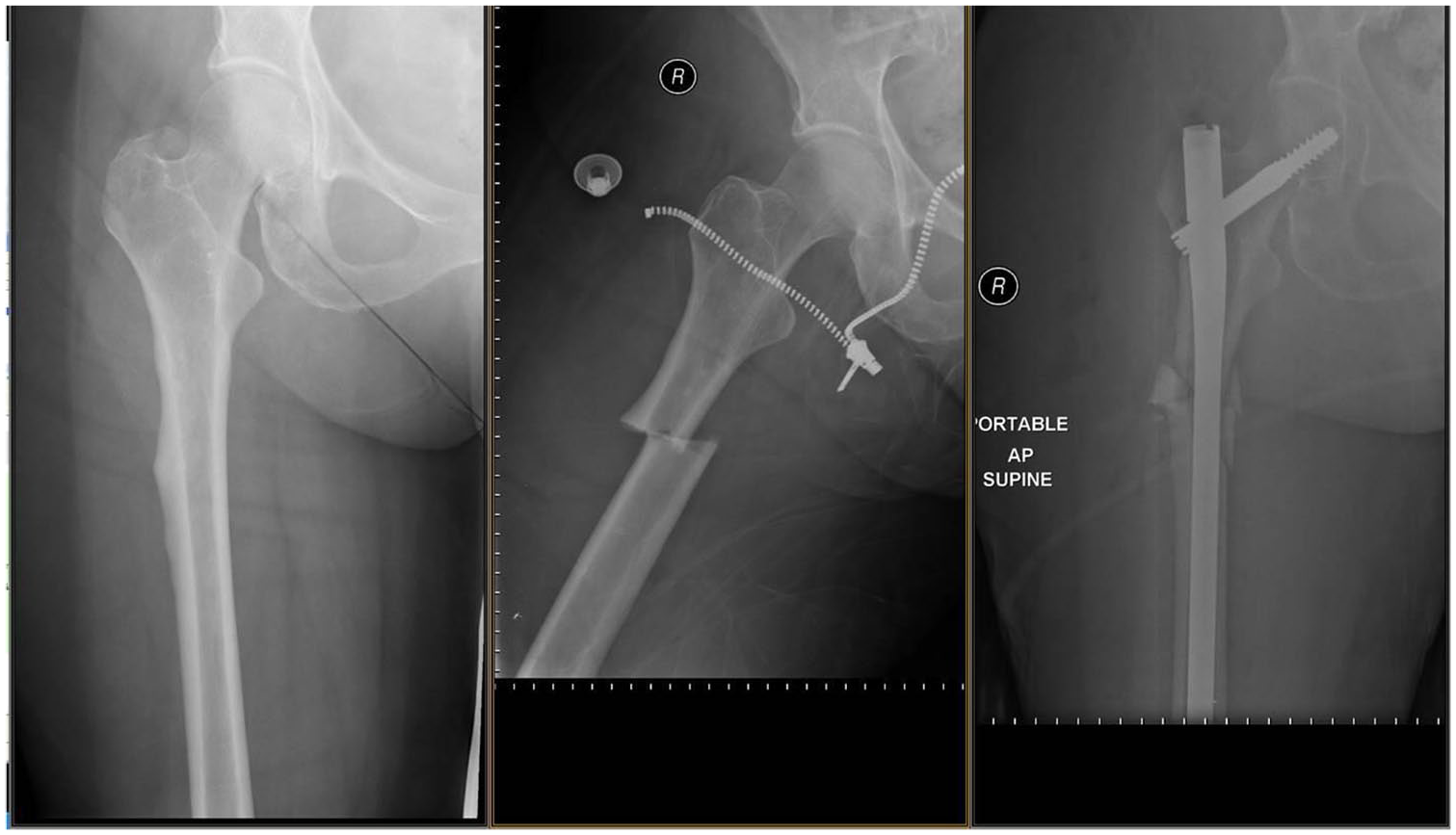
Incomplete atypical femur fracture progressing to complete atypical femur fracture.
Risk factors for AFF
Despite widespread use of bisphosphonates and denosumab for the treatment of osteoporosis, AFFs remain rare. Most patients who are treated with even very long-term antiresorptive osteoporosis medications will not experience stress changes in the femur. Observational studies have documented that women treated with antiresorptive medications have a significantly increased risk of developing AFF in comparison with men, and they tend to be younger than those with typical osteoporosis related fractures. AFFs appear to be more common in Asian women compared with White women. 11 This may be related to differences in the lower limb geometry in these different populations. Other observed risk factors for the development of AFF include low serum vitamin D level, simultaneous use of multiple antiresorptive bone medications, concurrent glucocorticoid use, rheumatoid arthritis, and younger age at initiation of bisphosphonate treatment. 23
The presence of a genetic metabolic bone disorder may be an important risk factor for developing AFF. In a systematic review published in 2018, AFFs were identified in patients with a number of monogenetic bone disorders, 28 including hypophosphatasia, 19 X-linked hypophosphatemia (XLH), pycnodysostosis, osteopetrosis, X-linked osteoporosis, and osteogenesis imperfecta. Some of these patients, in particular those with osteogenesis imperfecta, also had bisphosphonate exposure, but others had not taken antiresorptive medication. It has been postulated that there may be a drug-gene interaction which can predispose at risk patients to AFF when they are exposed to prolonged bisphosphonate or denosumab use.
In order to use medications to treat osteoporosis as safely as possible, it will be important to identify individuals who are at particular risk for developing AFFs. Further research is needed to identify those at risk, so that they can be managed appropriately and followed closely for the development of stress fractures if they are being treated with antiresorptive osteoporosis medications.
Screening for AFF
AFFs can, in some cases, be identified prior to the catastrophic development of a complete subtrochanteric or midshaft femur fracture. In up to one-third of patients with an identified AFF, there is evidence for AFF or stress changes in the opposite femur. 16 This presents an opportunity to identify an AFF prior to a completed fracture, when it may be amenable to intervention.
It is recommended that all patients with AFF have imaging of the opposite femur. Plain X-ray or femur scans using a densitometer can accurately identify stress changes in the bone, including cortical thickening, and will show a stress fracture line if present.29,30 If there are concerning symptoms in the context of antiresorptive medication use, and no significant abnormalities are seen on initial plain radiograph or dual-energy x-ray absorptiometry (DXA) imaging, bone scan can be considered as a next step. If a lucent line is seen on plain radiograph or with DXA, a computed tomography or magnetic resonance imaging scan should be done to determine the depth of the lucent line through the cortex, and the extent of the fracture around the circumference of the femur (figure 3). This information can be helpful in decision making about the need for prophylactic surgery versus medical therapy alone.11,31 In any case, patients should be counseled regarding decreasing weight-bearing activities so that these stress fractures can heal.

Images of incomplete atypical femur fracture with plain radiograph, computed tomography, bone scan.
There have been several small studies examining strategies for screening patients on long-term antiresorptive medication for the presence of stress changes or incomplete AFF. These studies suggest that the incidence of incomplete AFF may be as high as 1–2 per 100 patients who have been treated with 3–5 or more years of bisphosphonate treatment. 29 Protocols for screening patients who have been taking long-term bisphosphonates who also have leg symptoms, such as thigh pain, ache or weakness, have demonstrated a similar incidence of AFF. 30 Patients taking bisphosphonates or denosumab should be monitored for thigh pain and other leg symptoms, especially with or after weight-bearing activities, and if present, imaging to look for stress fractures should be considered. Further study is needed to assess whether this is a cost-effective strategy to identify what is an infrequent complication of osteoporosis treatment.
Management of AFF
Recommended management for AFF is outlined in the 2014 ASBMR task force report. 11 All bisphosphonates should be stopped once an AFF is identified. Denosumab, because it is a potent antiresorptive medication, should also be avoided in any patient with AFF. Calcium and vitamin D should be continued. Patients with AFF should be investigated for secondary causes of osteoporosis and underlying metabolic bone disease. Evaluation for rare genetic diseases that have been associated with AFF, such as hypophosphatasia, should be considered where appropriate.
These fractures are managed jointly by internal medicine specialists and orthopedic surgeons. Complete AFFs need surgical repair with an intramedullary rod, as other methods of surgical fixation have a high rate of failure. Fracture healing is often slow and there is a high risk of non-union. 32 Patients with incomplete AFF can be considered for prophylactic IM nailing depending on leg symptoms, extent and depth of the fracture line, and patient preference.
For medical management, anabolic bone medications such as teriparatide and abaloparatide can be used safely in patients who have had an AFF. Teriparatide has been shown in randomized controlled trials to be effective in improving bone mineral density and reducing fracture risk in patients with osteoporosis and high fracture risk, but data showing that it promotes healing of AFF is limited.31,33–35 Nonetheless, it is recommended as first line medical therapy for those who have had an AFF, particularly in patients who are also at high risk for usual osteoporotic fractures. Teriparatide is approved for 24 months of treatment, and restarting potent antiresorptive therapy afterwards, as would otherwise be recommended, should be considered with caution. We recommend against resuming bisphosphonates or denosumab after AFF, at least in the initial 5 years. Hormone replacement therapy (HRT) and selective estrogen receptor modulators (SERMS), which have not been associated with AFF, can be considered after anabolic therapy in order to prevent subsequent bone loss in selected circumstances.
Appropriate exercise guidance is important for patients with AFF, because repetitive stress to the lower limbs can cause further bone damage and slow fracture healing. Weight-bearing exercises should be minimized, but patients AFF will benefit from muscle strengthening through low resistance type exercises.
Approach to management of osteoporosis
AFF is a rare but dreaded complication of antiresorptive medication use. This risk is increased with antiresorptive osteoporosis medication use and duration of use, and there appear to be specific patient factors that may result in increased susceptibility to developing an AFF when taking these medications. That being said, bisphosphonates and denosumab remain first line and very effective treatments for those with high fracture risk. In the 2014 ASBMR task force report, it is estimated that, overall, 162 osteoporotic fractures are prevented for every one AFF resulting from antiresorptive medication use. 36
The ASBMR task force report outlines an approach to the management of osteoporosis in patients on long-term bisphosphonate treatment, 36 and more recently Dell and colleagues have published a proposed clinical practice guideline for AFF treatment and prevention. 33 Although we do not have definitive evidence as to the optimal strategy for minimizing the risk of AFF in those being treated with potent antiresorptive medication, these authors provide practical strategies for management that can be applied to our patients.
As recommended in current clinical practice guidelines, osteoporosis drug treatment should be offered to patients according to fracture risk, with those at highest risk having the most potential benefit from medication. Ongoing need for antiresorptive drug therapies should be reassessed after 3–5 years of continuous use, and those who have risk factors for AFF and those who are at lower 10 year fracture risk may benefit from stopping osteoporosis treatment for a “drug holiday”.37,38 For patients taking denosumab, stopping abruptly has been reported to result in an increase in risk for bone loss and multiple vertebral fractures, 39 so transitioning to a bisphosphonate for 6–12 months prior to stopping treatment should be considered. 40 In those who stop antiresorptive medication after 3–5 years of use, studies have shown that reduction in osteoporotic fracture risk can persist for up to 5 years after stopping medication. It is not, however, clear for how long a “drug holiday” is needed to reduce the risk of developing an AFF.41,42 Fracture risk, and the need to restart osteoporosis medication, should be reassessed regularly while patients are on “drug holiday” from osteoporosis medication (figure 4).

Communicating risks and benefits of osteoporosis medication.
Those who are at highest risk for usual osteoporotic fractures, particularly those who have had vertebral or hip fractures, will generally benefit from continuing antiresorptive osteoporosis medication. The absolute risk of AFF is low, but it does increase with duration of therapy. As it may be possible to identify an incomplete AFF prior to a complete fracture, it is important to have an index of suspicion in patients at risk. If patients on antiresorptive therapy develop thigh pain, imaging is recommended to look for evidence of stress changes in the femur in the spectrum of AFF.
Conclusion
Despite the risk of AFF, antiresorptive medications that are currently available for the treatment of osteoporosis and reduction in fracture risk remain effective and safe. There is evidence that the care gap in the treatment of osteoporosis is growing, and it is important that patients not be denied effective treatment for fracture reduction.43,44 Appropriate use of osteoporosis medications in patients who are at high risk for fracture, if clinicians are mindful of issues around safety and duration of therapy, will minimize risk and maximize benefit. That being said, more studies are needed to determine the most appropriate treatment strategies for patients with osteoporosis, so that our patients can benefit from effective treatments, while minimizing the risk of developing an AFF. Communicating risks appropriately to both patients and physicians is critical in order to appropriately manage our high-risk osteoporosis patients.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.