
Abstract
Rheumatoid arthritis (RA), a chronic autoimmune inflammatory disease of synovial joints, can lead to chronic pain and structural joint damage, as well as other organ involvement, especially if not adequately controlled. Because it can affect women in their reproductive years, care of pregnant women with RA requires a delicate balance of maintaining disease control while limiting potential toxicity to the fetus and neonate. While most women experience a substantial improvement in disease activity during pregnancy, for some women their RA remains active. It can even manifest itself for the first time during pregnancy or early in the post-partum period. Optimizing disease control prior to conception is key, but utilizing disease-modifying treatments effectively and safely throughout pregnancy and lactation requires open dialogue and shared decision making. This review provides evidence-based recommendations for use of disease-modifying antirheumatic drugs (DMARDs) and biologic response modifiers to guide rheumatologists in their care of pregnant and lactating women with RA and serves as a guide to counsel male patients with RA on family planning decisions.
Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disorder that can affect women in their reproductive years. With the expanded armamentarium of disease-modifying therapies available in the ‘biologic era’ and targeted approach to therapy, there is increasing ability to achieve adequate control of disease activity. However, the desire to start a family adds additional complexity to management decisions preconception, during pregnancy and following delivery given the lack of safety data and potential teratogenicity of available therapies. Male patients anticipating family planning often desire appropriate guidance in view of the potential effects on fertility and conception. Well-established data supporting the safe use of medications in pregnancy and lactation are available for a few medications, while for many others the safety profile is much less certain and guidance is based on the manufacturer’s recommendations. Based on the evidence available from animal and human data, the US Food and Drug Administration (FDA) has established pregnancy risk categories of drugs (Table 1). This provides a broad guideline, which supports but does not take the place of open dialogue and shared decision making which is critical in discussing the risks and benefits of the treatment approach that may be unique to each individual patient. In this review, we seek to provide the rheumatologist with an overview on the safety profile of drugs used for RA preconception, during pregnancy (Table 1) and lactation (Table 2). Preconception recommendations for men using RA medications are also discussed.
Summary of recommendations for safety of therapies for rheumatoid arthritis during pregnancy.

US Food and Drug Administration pregnancy category (see http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=201.57): A, controlled human studies show no risk; B, no evidence of risk in studies; C, risk cannot be ruled out; D, positive evidence of risk; X, contraindicated in pregnancy.
NSAID, nonsteroidal anti-inflammatory drug; TNF, tumor necrosis factor; VACTERL, vertebral anomalies, anal atresia, cardiac defects, tracheoesophageal, renal, and limb abnormalities.
Summary of recommendations for safety of therapies for rheumatoid arthritis during lactation.
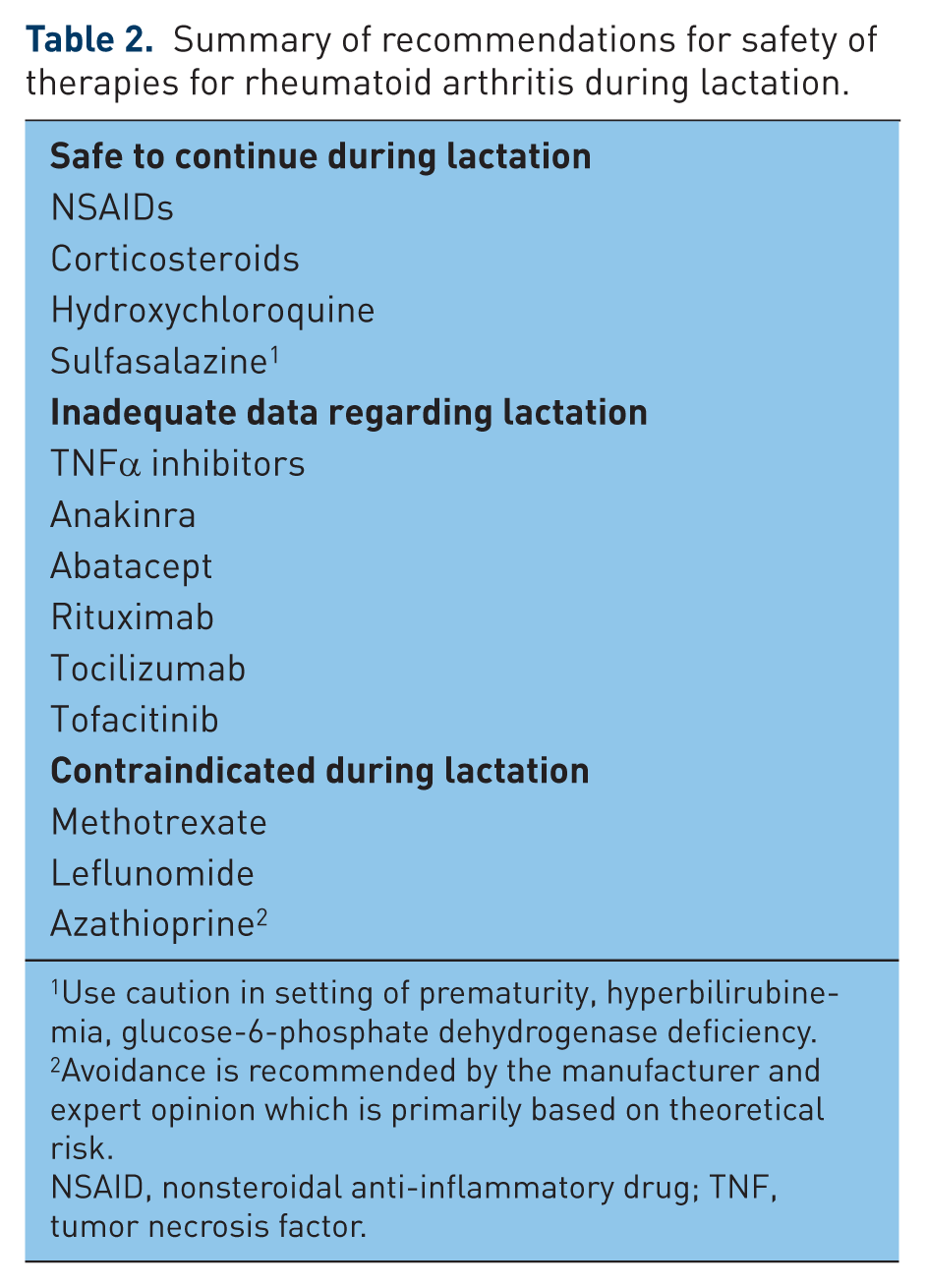
Use caution in setting of prematurity, hyperbilirubinemia, glucose-6-phosphate dehydrogenase deficiency.
Avoidance is recommended by the manufacturer and expert opinion which is primarily based on theoretical risk.
NSAID, nonsteroidal anti-inflammatory drug; TNF, tumor necrosis factor.
Effect of pregnancy on RA
Dr Philip S. Hench described in 1938 a remarkable improvement in the signs and symptoms of inflammatory arthritis (primarily RA) during pregnancy [Hench, 1938], an observation that led to the quest to find ‘substance X’ that resulted in the Nobel Prize-winning discovery of cortisone a decade later. Although cortisone was not the true explanation, the subsequent decades saw an upsurge in an interest to gain better understanding of the immunological and hormonal changes of pregnancy and its influence on RA disease activity [Amin et al. 2011]. The goal has been to try and induce a similar immune environment in the nonpregnant state for amelioration of RA associated symptoms.
It is now well established through large observational prospective studies that women with RA often experience a spontaneous improvement or stabilization of their disease during pregnancy [Ostensen and Villiger, 2007; De Man et al. 2008], but only to flare post-partum. Complex and well-coordinated changes in cytokine profiles, immune cell number and function (particularly regulatory T cells) and hormone levels work in conjunction to prevent maternal rejection of the developing, genetically distinct fetus [Amin et al. 2011] during pregnancy and it appears likely that this state of immune tolerance may be a key factor to understanding the improved disease activity state in RA, much about which remains to be learned.
Unfortunately, many pregnant women will require some treatment during pregnancy as only a minority achieve complete remission without medication [De Man et al. 2008]. Moreover, many women develop a flare of their RA symptoms post-partum and require rapid initiation of medical therapy [Nelson and Ostensen, 1997; Barrett et al. 1999; De Man et al. 2008] for symptomatic management. It thus becomes necessary for the treating rheumatologist to not only counsel the patient on the safe use of analgesics and immunosuppressant medications before and during pregnancy but also develop a strategic plan to optimize disease control post-delivery with a preemptive discussion of the potential risks to the neonate if breastfeeding is a consideration.
When a woman of child-bearing age is diagnosed with RA, the rheumatologist is entrusted with multiple responsibilities. A discussion of the need for contraception and safest time for conception is critical. The choice of disease-modifying antirheumatic drug (DMARD) or biologic response modifier (‘biologic’) can be influenced by the desire of the patient to start a family and must be taken into consideration, in addition to discussing the risk of the medication during preconception, pregnancy and lactation. In the case of an unplanned pregnancy while on therapy, immediate discontinuation of the medications (if considered toxic or high risk) and referral to a high-risk obstetrician for monitoring and review of options is recommended.
We will discuss below, in order, nonsteroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids (GCs), followed by safe and unsafe DMARDs and biologic response modifiers in the context of pregnancy and lactation in RA patients. Guidelines for safe use of these medications will be provided when possible, including for men.
NSAIDs
NSAIDs are often a readily available, inexpensive treatment of pain and swelling in RA. The FDA considers these agents category B (Table 1). While NSAIDs are a relatively safe option for managing pain symptoms in pregnant women with RA, they do need to be used with caution, especially early in pregnancy, and are contraindicated in the last trimester of pregnancy.
In a Danish cohort of 1462 pregnant women who used NSAIDS during pregnancy there was no association of NSAIDs with prematurity, low birth weight, or congenital abnormalities [Nielsen et al. 2001]. Yet, there are reports suggesting that these medications may be associated with an increased risk for miscarriage when used early in pregnancy. In a case-control study [Nielsen et al. 2001] 4268 Danish women with miscarriages were compared with 29,750 women with live births and found a higher risk of miscarriage with NSAID use. The risk was more with NSAID use within one week of miscarriage [Nielsen et al. 2001]. In a population-based cohort identified using Kaiser Permanente data [Li et al. 2003], 5% of 1055 women (followed for the first 20 weeks of their pregnancy) utilized NSAIDs and were reported to have higher rates of miscarriage (hazard ratio [HR] 1.8, 95% confidence interval (CI) 1.0–3.2) than those who did not use NSAIDs. This risk was higher with prolonged use (greater than 1 week) or use near conception [Li et al. 2003]. In a case-control study examining 4705 cases of spontaneous abortion, of which 7.5% were exposed to NSAIDs, it was reported that there was an increased risk with NSAID use (odds ratio [OR] 2.43, 95% CI 2.12–2.79) [Nakhai-Pour et al. 2011]. In contrast, in a cohort of 2780 women, where 43% used NSAIDs before the sixth week of gestation, there was no increased risk of spontaneous abortion associated with use of NSAIDs even when adjusted for maternal age [Edwards et al. 2012]. The disparity in results may be related to ascertainment of exposure to NSAIDs given the different prevalence rates between the cohorts. Nonetheless, NSAID use in early pregnancy warrants caution.
NSAIDs are also not recommended for use in the third trimester of pregnancy. In pregnant rats, NSAIDs have been demonstrated to constrict the fetal ductus, with indomethacin having a stronger effect compared with aspirin [Momma and Takeuchi, et al. 1983; Momma et al. 1984; Koren et al. 2006]. This effect of NSAIDs on premature ductal closure was also confirmed in a meta-analysis [Koren et al. 2006]. This can result in fetal pulmonary hypertension and even death [Koren et al. 2006]. COX-2 inhibitors, considered Class C pregnancy risk category by the FDA, have also been reported to induce constriction of fetal lamb ductus arteriosus [Takahashi et al. 2000]. In addition, use of NSAIDs later in pregnancy has been demonstrated to decrease amniotic fluid levels resulting in oligohydramnios and inadequate pulmonary development via inhibition of renal prostaglandin synthesis and fetal urinary output [Hickok et al. 1989].
NSAIDs, including COX-2 inhibitors, are thus contraindicated in the third trimester, but may be used with caution prior to 24 weeks of gestation, with intermittent use of those with a short half-life preferred [Makol et al. 2011].
Glucocorticoids
GCs are frequently used for management in pregnant RA patients and are considered category B by the FDA (Table 1). They were the most commonly utilized medication during pregnancy in one cohort [Kuriya et al. 2011]. The rapidity of symptom relief and minimal transplacental transfer [Beitins et al. 1972] make prednisone, cortisone or hydrocortisone the ideal choice for management of RA flares in pregnancy. Dexamethasone and betamethasone should be avoided in pregnant women (unless required for fetal indications) as they cross the placenta with similar maternal and fetal concentrations [Ogueh and Johnson, 2000].
Unlike NSAIDs, GCs do not appear to be associated with early fetal loss. In a nested case-control study of 10,974 women with first time miscarriage, oral corticosteroids demonstrated no association with the rate of miscarriage [Bjorn et al. 2013].
There are reports suggesting that GCs use during pregnancy may increase the risk for cleft lip, but not other major congenital anomalies. In one meta-analysis, there was no difference in major congenital abnormalities [Park-Wyllie et al. 2000]. In a large Danish cohort [Bay Bjorn et al. 2014], there was no association between early GC exposure and congenital abnormalities or oral cleft. This study also compared previous studies of GC exposures and described the published range of odds ratios as 0.8–2.1 for congenital abnormalities and 0.6–5.2 for oral cleft [Bay Bjorn et al. 2014]. In an additional evaluation of a Danish cohort [Hviid and Molgaard-Nielsen, 2011], corticosteroids were not demonstrated to increase the risk for cleft lip or palate. Of note, the majority of corticosteroid exposure was in the form of topical or inhaled, only 4.2% of the steroid exposure was in an oral form [Hviid and Molgaard-Nielsen, 2011]. While there are variable reports of risk regarding oral cleft, women should be counseled about this potential risk.
There has been conflicting data regarding association between GC use and prematurity and low birth weight [Ostensen and Forger, 2009]. In a prospective study evaluating 184 women exposed to GC in pregnancy [Park-Wyllie et al. 2000], there were higher rates of prematurity and lower birth weight in comparison with 188 pregnant women without GC exposure. Greater rates of preterm delivery associated with premature rupture of membranes were identified in patients with antiphospholipid antibody syndrome treated with prednisone [Cowchock et al. 1992]. On the other hand, in a Danish cohort of 900 children born to mothers with Crohn’s disease there was no association between GC exposure and prematurity, low birth weight, or congenital abnormalities [Norgard et al. 2007].
Labor and delivery can be equated to moderate medical or surgical stress, and it has been recommended that in women on GCs through their pregnancy, a stress dose of hydrocortisone (50–75 mg) or methylprednisolone (10–15 mg) be given on the day of the procedure and quickly tapered over 1–2 days [Rosandich et al. 2004; Temprano et al. 2005].
GCs appear to be a safe option for the management of RA in pregnancy and if these are necessary, the goal is to keep the patient on the lowest dose possible to control disease activity. Counselling the mother on the low risk of fetal oral clefts with first trimester exposure is reasonable. Besides the above, counselling with regard to a close observation on blood pressure and blood glucose values may be good practice.
DMARDs safe for use in pregnancy
Hydroxychloroquine
Hydroxychloroquine is frequently used in RA as part of triple therapy in conjunction with methotrexate and sulfasalazine [Singh et al. 2012]. Much of the data regarding the safety of hydroxychloroquine in pregnancy comes from its use for malaria and connective tissue diseases, particularly systemic lupus erythematosus (SLE). Hydroxychloroquine has been reported to have transplacental passage with similar concentrations between maternal blood and cord blood at the time of delivery [Costedoat-Chalumeau et al. 2002]. In a recent prospective study evaluating 114 women with exposure to hydroxychloroquine during pregnancy for varied clinical indications compared with women without this exposure, lower birth weight, earlier gestational age, and higher preterm delivery rates were associated with hydroxychloroquine although there were no differences observed in congenital abnormalities [Diav-Citrin et al. 2013]. This may be related to maternal disease rather than hydroxychloroquine exposure. Nevertheless, several earlier studies have observed no differences in rates of adverse fetal or pregnancy outcomes, including congenital anomalies [Buchanan et al. 1996; Costedoat-Chalumeau et al. 2003; Clowse et al. 2006]. Furthermore, a meta-analysis evaluating hydroxychloroquine use in pregnancy demonstrated its safety with no association with fetal death, spontaneous abortion, rates of live births, prematurity, or congenital defect [Sperber et al. 2009]. There is data extending into childhood with a mean follow-up of 33 months demonstrating no abnormalities [Parke and West, 1996].
Based on the balance of evidence available to date, hydroxychloroquine is a reasonable RA treatment option for women of childbearing age, particularly in the setting of mild disease (see the Hydroxychloroquine Prescription Insert, http://products.sanofi.ca/en/plaquenil.pdf) and can be continued safely during a pregnancy, if clinically indicated. It is labelled FDA category C (Table 1).
Sulfasalazine
Sulfasalazine is frequently used in combination therapy for treatment of RA [Singh et al. 2012]. Much of the information regarding sulfasalazine’s safety in pregnancy is from patients with inflammatory bowel disease (IBD). Its transplacental passage is demonstrated by equal maternal serum and cord blood levels [Jarnerot et al. 1981]. Nevertheless, several studies have reported safe use of sulfasalazine during pregnancy. In a Danish cohort of children born to women with Crohn’s disease, the use of sulfasalazine was not associated with low birth weight, congenital abnormalities, or prematurity [Norgard et al. 2007]. Among 287 pregnancies in a cohort of IBD patients treated with sulfasalazine and/or corticosteroids [Mogadam et al. 1981], pregnancy outcomes were similar when compared with women not on these therapies or the general population. In those exposed to sulfasalazine the risk of spontaneous abortion was less than 3% [Mogadam et al. 1981]. Although none of the infants whose mothers were exposed to sulfasalazine developed jaundice, one child of a mother treated with sulfasalazine and corticosteroids developed cleft palate and microglossia, while another infant whose mother had been treated with sulfasalazine and corticosteroids suffered congenital deafness [Mogadam et al. 1981]. On the other hand, in a case-control study comparing infants with (22,865) and without (38,151) congenital abnormalities, there was no difference in the rate of sulfasalazine exposure between the two groups (0.07% in both groups) [Norgard et al. 2001]. Furthermore, in a meta-analysis reviewing 642 women with IBD who were treated with mesalazine, sulfasalazine, or olsalazine during their pregnancy as compared with 1158 women who received no medications, there was no difference in the rates of congenital abnormalities, stillbirth, spontaneous abortion, preterm delivery, or low birth weight [Rahimi et al. 2008]. There is a report of transient neutropenia in a newborn born to a mother treated with sulfasalazine during pregnancy that resolved spontaneously in approximately 6 weeks [Levi et al. 1988].
Sulfasalazine is considered to be FDA category B (Table 1; see also the Sulfasalazine Prescription Insert at http://labeling.pfizer.com/ShowLabeling.aspx?id=524) and based on the balance of evidence available, can be used safely during pregnancy. Folate supplementation is encouraged during its use preconception and throughout pregnancy [Ostensen et al. 2006] as it is a strong inhibitor of the reduced folate carrier [Jansen et al. 2004].
Azathioprine
While not used as frequently with the availability of newer drugs, azathioprine is FDA approved for treatment of RA (see that Azathioprine Prescription Insert at http://www.tritonpharma.ca/uploads/files/pdf/imuran-tablet-en.pdf). Safety data in pregnancy is primarily derived from observational studies in the IBD and transplant patient population. A Danish cohort study [Norgard et al. 2007] reported that children born to mothers with Crohn’s disease were more likely to be born prematurely and have congenital abnormalities when their mothers were exposed to azathioprine/6-mercaptopurine. The congenital abnormalities included occipital encephalocele, sternocleidomastoid anomalies and congenital cataract [Norgard et al. 2007]. However, other reports have been very reassuring. In women with IBD, azathioprine use did not increase the risk of congenital abnormalities compared with the general population [Moskovitz et al. 2004]. In another cohort of women exposed to azathioprine versus those who were not [Goldstein et al. 2007], there was no difference in congenital abnormalities. However, there were higher rates of prematurity, lower gestational age, and low birth weight [Goldstein et al. 2007]. In another cohort evaluating women with IBD, a subset 149 (8.7%) of women were exposed to azathioprine/6-mercaptopurine, with no association noted with its use and congenital abnormalities [Ban et al. 2014].
Azathioprine is considered category D (Table 1; see also the Azathioprine Prescription Insert at http://www.tritonpharma.ca/uploads/files/pdf/imuran-tablet-en.pdf). Despite this FDA category, its demonstrated safety in human studies has made it a safer option for use in pregnancy.
DMARDs not safe for use in pregnancy
Methotrexate
Methotrexate is frequently used as the foundation drug for RA management [Singh et al. 2012]. This however poses a dilemma when initiating therapy for RA in women of childbearing age. Methotrexate is an effective abortifacient [Hausknecht, 1995] and hence considered category X for pregnancy. Even though a recent case-control study evaluating induced abortions reported a lower rate of methotrexate use in individuals who had an induced abortion versus those who did not [Vinet et al. 2013], this study does not capture the rates of spontaneous abortions or the outcomes of pregnancies. Their results may also be reflective of contraception recommendations in the setting of methotrexate.
Pregnant women exposed to methotrexate are at increased risk of the ‘aminopterin syndrome’ characterized by fetal central nervous system, skeletal and cardiac abnormalities. A patient with juvenile idiopathic arthritis who received a total of 100 mg of methotrexate over the first 8 weeks of pregnancy delivered an infant with aminopterin syndrome [Buckley et al. 1997]. Even with lower doses (5 mg weekly for 8 weeks) reports of toxicity including skull abnormalities have been noted [Powell and Ekert, 1971].
While there is significant data regarding the risk of methotrexate both in terms of spontaneous abortions and congenital abnormalities, there are reports of pregnant women with exposure to methotrexate having no complications. One example is surveillance data from France [Lewden et al. 2004], 28 pregnancies were identified with exposure to methotrexate with 26 of 28 stopping it prior to 8 weeks gestation. Of these, 19 resulted in live births, 4 spontaneous abortions, and 5 elective abortions. One child had metatarsus varus and eyelid angioma [Lewden et al. 2004]. Other studies demonstrate the risk of spontaneous abortion but also reports of live births without congenital anomalies [Kozlowski et al. 1990; Ostensen et al. 2000, 2007; Chakravarty et al. 2003]. This should not lead to underestimation of the risk of methotrexate during pregnancy, but is data that can be used to counsel women with unintentional pregnancies in the setting of methotrexate exposure.
Methotrexate is absolutely contraindicated in pregnancy and when used in women of childbearing age, strict contraception must be advised with two different methods. It is also recommended that methotrexate be stopped at least 3 months prior to attempting conception (see the Methotrexate Prescription Insert available at http://www.rheumatrex.info/pdf/RheumatrexPackageInsert.pdf). In the case of an unplanned pregnancy while on methotrexate, methotrexate should be discontinued immediately and the patient referred to a genetic counsellor for discussion of appropriate options for observation versus intervention.
Leflunomide
Leflunomide is FDA approved for the treatment of RA and often used in cases of methotrexate intolerance [Singh et al. 2012]. Leflunomide has been demonstrated to cause significant abnormalities in animal models at pharmacokinetic doses similar to those used in humans. In mice, a wide range of abnormalities have been noted ranging from fetal death to ventricular septal defect, persistent truncus arteriosus, skeletal, and neural tube defects [Fukushima et al. 2007]. Given these reports in animals, it is considered a category X medication for pregnancy (Table 1).
The drug has a long half-life of 14–15 days but also undergoes enterohepatic circulation as a result of which it may take up to 2 years for complete elimination from the body after discontinuation [Temprano et al. 2005]. Cholestyramine wash out procedures have thus been identified to augment leflunomide elimination (see the Leflunomide Prescription Insert at http://products.sanofi.us/arava/arava.html) and are often recommended prior to conception. Cholestyramine 8 grams is given three times daily for 11 days and plasma levels, checked twice separated by 2 weeks, should be below 0.02 mg/l with additional cholestyramine administration if the level is higher than this cut-off [Brent, 2001]. Conception should be avoided for three menstrual cycles after elimination [Temprano et al. 2005]. Drug level monitoring has been recommended to help with counseling regarding the optimal timing of pregnancy [Brent, 2001].
Outcomes of inadvertent pregnancies in the setting of leflunomide exposure have been reported. In 64 women exposed to leflunomide compared with disease matched controls and healthy controls, there were no differences in the number of live born infants or spontaneous abortions. Further, there was no difference between major or minor congenital abnormalities [Chambers et al. 2010]. An additional 45 pregnancies with 16 exposed during pregnancy and 29 prior to conception were evaluated [Cassina et al. 2012]. All patients with exposure during pregnancy delivered liveborn infants while those with exposure previously, the vast majority, 93.1%, had a liveborn infant. Two infants had congenital abnormalities in the group with exposure during pregnancy including aplasia cutis congenita in one and the other with multiple including Pierre–Robin sequence, spina bifida occulta, patent ductus arteriosus, chondrodysplasia punctata, and congenital heart block. No congenital abnormalities occurred in those exposed prior to conception [Cassina et al. 2012]. Of note, the vast majority of patients with leflunomide exposure prior to conception or during pregnancy underwent the cholestyramine wash-out protocol.
Leflunomide is contraindicated in the setting of pregnancy. Caution must be used when it is prescribed to women of childbearing age, due its long half-life, even after complete cessation, and the risk during pregnancy. Women of childbearing potential should be appropriately counselled about this risk.
Biologic response modifiers
There is a relative lack of safety data in pregnancy to counsel patients with regards to the biologic response modifiers. The most is known regarding tumor necrosis factor α (TNFα) inhibitors. Much of this data is drawn from large observational studies of patients with IBD. This underscores the importance of counseling patients about potential risks.
TNFα inhibitors
TNFα inhibitors are recommended for the management of RA refractory to methotrexate alone or as first-line therapy in the setting of poor prognostic factors [Singh et al. 2012]. As a category, TNFα inhibitors are considered category B primarily due to the absence of risk in animal studies (see the Adalimumab Prescription Insert at }http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/ucm092762.pdf, Certolizumab Prescription Insert at http://www.cimzia.com/pdf/prescribing_information.pdf, Etanercept Prescription Insert at http://www.accessdata.fda.gov/drugsatfda_docs/label/2003/etanimm060503LB.pdf, Golimumab Prescription Insert at http://www.simponi.com/shared/product/simponi/prescribing-information.pdf, and Infliximab Prescription Insert at http://www.remicade.com/shared/product/remicade/prescribing-information.pdf). However, case reports of congenital anomalies following exposure to TNFα inhibitors have raised concerns about their safety profile during pregnancy. However, since these case reports, larger observational studies have become available.
One case report described a woman treated with etanercept who delivered an infant with vertebral anomalies, anal atresia, cardiac defects, tracheoesophageal fistula and/or esophageal atresia, renal anomalies and limb defects (VATER/VACTERL) association [Carter et al. 2006]. In review of the FDA database up until December 2005 [Carter et al. 2009], there were 40 children with 54 congenital abnormalities born to mothers exposed to TNFα inhibitors. VACTERL anomalies occurred at a statistically significantly higher rate in women exposed to TNFα inhibitors. Anomalies were only seen in mothers exposed to etanercept and infliximab. No abnormalities were reported with exposure to adalimumab [Carter et al. 2009]. Utilizing the British Society for Rheumatology Biologics Register (BSRBR) [Hyrich et al. 2006], information is available about 32 pregnancies with the majority having RA. A total of 23 were receiving therapy at the time of conception. Two patients continued therapy past the first trimester with one continuing for the entire pregnancy. There were 14 live births while there were 6 first trimester miscarriages and 3 elective first trimester terminations. Nine other patients stopped TNFα inhibitors before conception (mean time 5 months); and there was 1 first trimester miscarriage and 8 live births [Hyrich et al. 2006]. In a cohort created by the infliximab manufacturer’s data base of 131 women exposed to infliximab with either RA or Crohn’s disease, there was no difference in rates of live births, miscarriages, or therapeutic abortions as compared with the general population or patients with Crohn’s disease not exposed to infliximab [Katz et al. 2004]. In the TREAT registry of patients with Crohn’s disease including 142 pregnancies involving women and treated male partners, infliximab as compared with other therapies for IBD did not have any difference in rates of live births or congenital abnormalities [Lichtenstein et al. 2012]. In a prospective study of 83 women exposed to TNFα inhibitors, there was no difference in the rate of major congenital anomalies compared with those both disease-matched and those without any exposures. VACTERL cases did not occur [Diav-Citrin et al. 2014]. In a systematic review evaluating IBD and pregnancy, there was no association with congenital abnormalities, prematurity, low birth weight, or spontaneous abortions when evaluating infliximab, adalimumab, and certolizumab [Nielsen et al. 2013]. In one systematic review of 472 pregnancies (194 infliximab, 261 adalimumab, 17 certolizumab), the rates of spontaneous abortions and congenital anomalies were similar to the US general population [Marchioni and Lichtenstein, 2013].
There is little data available on continuation of TNFα inhibitor therapy through pregnancy. Much of the data is isolated to exposures within the first trimester. As of 2009, there were 29 reports of women continuing TNFα inhibitor therapy throughout their pregnancy making it difficult to draw conclusions about use throughout pregnancy [Berthelot et al. 2009].
Due to different composition of TNFα inhibitors, some risk may depend on the individual agent rather than just the drug class. At birth, both infant and cord blood demonstrated higher concentrations of infliximab and adalimumab as compared with the mother whereas certolizumab in contrast had very low concentrations in infant and cord blood. This is attributed to the absence of an Fc portion on certolizumab such that it cannot be bound by the neonatal Fc receptor [Mahadevan et al. 2013]. A patient who received two doses of certolizumab during pregnancy had a full-term pregnancy with the infant suffering no consequences [Oussalah et al. 2009].
In conclusion, although initial reports raised concerns for VACTERL abnormalities with use of TNFα inhibitors, recent large meta-analyses do not seem to suggest an increased risk for this or other congenital anomalies. Overall, these agents are rated as FDA category B (Table 1; see also the Adalimumab, Certolizumab, Etanercept, Golimumab, and Infliximab Prescription Inserts). However, most of the safety data available is based on women discontinuing TNFα therapy in the first trimester; little data exists about exposure throughout the pregnancy.
Rituximab
Rituximab is frequently reserved for patients who have failed to have their disease controlled by combination DMARDs or TNFα inhibitors [Singh et al. 2012]. Rituximab depletes B cells via its mechanism of a monoclonal antibody against CD20. Animal studies are limited; no teratogen effect has been noted but B cells have been demonstrated to be reduced in offspring (see the Rituximab Prescription Insert at http://www.gene.com/download/pdf/rituxan_prescribing.pdf). A total of 231 pregnancies were identified from the rituximab global drug safety database with wide-ranging maternal indications [Chakravarty et al. 2011] with known outcomes available in 153 pregnancies. Live births occurred in 90 (58.8%), spontaneous abortions in 33 (21.6%), and therapeutic abortions in 28 (18.3%). Premature births occurred in 22 with one death at 5 weeks. Congenital abnormalities occurred in two with one infant suffering a clubfoot and another infant with ventral septal defect, patent foramen ovale, and patent ductus arteriosus. In addition, 11 infants had hematologic abnormalities and 4 different infants suffered complications of infection [Chakravarty et al. 2011]. In one case series, two patients received rituximab during their pregnancy with normal resulting pregnancies [Ojeda-Uribe et al. 2013]. In a case series of six patients [Sangle et al. 2013], one with GPA and five with SLE, all treated with rituximab, four had normal pregnancies. One baby was born prematurely and had esophageal atresia in one woman with lupus nephritis. Another woman with lupus nephritis had premature delivery. The time range from rituximab to conception was 8–22 months [Sangle et al. 2013]. Six women experienced eight pregnancies following treatment with rituximab for anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis [Pendergraft et al. 2013]. One patient had a miscarriage at 15 weeks with findings demonstrating Beckwith–Wiedemann syndrome. The remaining seven pregnancies resulted in live births. Fetal cord blood was tested in three infants and B cells were present in all [Pendergraft et al. 2013]. Concern has been raised about hematologic side effects for infants as well as infection.
Rituximab is considered to be category C (Table 1) with limited data available. It is ideally recommended that at least 12 months should elapse between rituximab discontinuation and conception (see the Rituximab Prescription Insert).
Abatacept
Abatacept inhibits T-cell activation by blocking interactions between antigen-presenting cells and T cells via binding to CD80/CD86 on antigen-presenting cells. Abatacept is FDA class C in terms of risk for pregnancy. Animal studies saw no increased risk when exposed to the maximum recommended human dose; however, at extremely elevated doses there were alterations in immune function noted (see the Abatacept Prescription Insert http://packageinserts.bms.com/pi/pi_orencia.pdf). In one case report, a woman with RA being treated with abatacept and methotrexate became pregnant. Both medications were stopped in the first trimester. A full-term infant was born without health issues [Ojeda-Uribe et al. 2013]. There is inadequate data to fully comment on the safety of abatacept during pregnancy.
Anakinra
Anakinra is a recombinant interleukin-1 receptor antagonist. It was a FDA-approved therapy for RA in 2001. In animal studies of anakinra, no harm has been demonstrated to the fetus. Per the prescription insert, anakinra should only be used in pregnancy if clearly required (see the Anakinra Prescription Insert at http://www.accessdata.fda.gov/drugsatfda_docs/label/2003/anakamg062703LB.pdf). In a single woman with adult onset Still’s disease, anakinra was continued throughout pregnancy. She did experience retention of the placenta necessitating manual abruption but there were no other abnormalities [Berger et al. 2009]. Anakinra is considered category B (Table 1) but little has been reported about its safety in this setting (see the Anakinra Prescription Insert).
Tocilizumab
Tocilizumab is a monoclonal antibody directed against interleukin-6 receptors blocking downstream signaling. It was approved for RA in 2010 either alone or in combination with methotrexate or other DMARDs. According to the manufacturers’ package insert, no teratogenicity has been demonstrated in animal models but at high dose there was increased risk of abortion (see that Tocilizumab Prescription Insert at http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/125276lbl.pdf). In an abstract describing 32 patients, the majority of which were receiving methotrexate and tocilizumab, 13 had an elective abortion, with 7 experiencing a spontaneous abortion. One child died 3 days after birth due to acute respiratory distress syndrome (ARDS) following hemorrhage secondary to placenta previa [Rubbert-Roth et al. 2010]. There is limited information about tocilizumab and it is considered category C (Table 1) by FDA (see the Tocilizumab Prescription Insert).
New therapy options: Janus kinase inhibitor
Tofacitinib
Tofacitinib is a Janus kinase (JAK) inhibitor recently approved by FDA in 2012 for RA. Tofacitinib is a category C medication. Animal studies have demonstrated teratogenicity and feticidal effect at much higher levels than the maximum recommended human dose. A registry has been created by Pfizer®, the manufacturer of tofacitinib, to monitor safety of tofacitinib in the setting of pregnancy and breast feeding (see the Tofacitinib Prescription Insert at http://www.xeljanz.com/).
Use of DMARDs and biologics for RA during lactation
Little data is available about the safety of RA medications during breastfeeding (Table 2). Certain NSAIDs are considered compatible with breastfeeding by the American Academy of Pediatrics including flufenamic acid, ibuprofen, indomethacin, diclofenac, mefenamic acid, naproxen, piroxicam, and tolmetin [Committee on Drugs, American Academy of Pediatrics, 2001]. It is recommended to time the breastfeeding immediately before the NSAID dose to reduce the risk of exposure [Ostensen et al. 2006].
When evaluating mother’s serum and milk concentrations while taking oral GCs, the milk concentrations were found to be 5–25% of the serum levels [Ost et al. 1985]. Even on high-dose prednisolone 80 mg daily, the absorption for an infant is felt to represent less than 10% of their daily cortisol production [Ost et al. 1985]. Although exposure is minimal, it can be further reduced by nursing immediately before or more than 4 hours after the GC dose [Ost et al. 1985].
In evaluating DMARDs, only case reports and case series are available to help guide decisions. Hydroxychloroquine is secreted in breast milk but no visual or other abnormalities have been reported in neonates thus far as a result of exposure through breastfeeding [Committee on Drugs, American Academy of Pediatrics, 2001; Costedoat-Chalumeau et al. 2002]. Among eight women treated with sulfasalazine through lactation, metabolites were detectable in infants’ serum as well as breast milk. However, the concentration in infants was not high enough to displace bilirubin from albumin and no episodes of kernicterus were reported [Esbjorner et al. 1987]. One case report identified an infant who experienced bloody diarrhea between ages of 2 and 3 months in the setting of his mother taking sulfasalazine during pregnancy with resolution within 72 hours of his mother discontinuing sulfasalazine [Branski et al. 1986]. It is recommended that sulfasalazine be used with caution particularly with premature or ill infants or in the setting of hyperbilirubinemia and glucose-6-phosphate dehydrogenase deficiency [Committee on Drugs, American Academy of Pediatrics, 2001; Ostensen et al. 2006]. From among 10 women treated with azathioprine, 31 samples of breast milk were obtained of which only 2 samples from the same woman demonstrated low levels of azathioprine metabolites. There were no findings to suggest neonatal immunosuppression [Sau et al. 2007]. The use of azathioprine in breastfeeding has been conflicting. The prescription insert and expert opinion recommend against its use due to the theoretical risk [Ostensen et al. 2006] and must be addressed with the patient.
A woman treated with methotrexate for choriocarcinoma did have evidence of its secretion in breast milk with the highest milk to plasma ratio of 0.08 [Johns et al. 1972]. Methotrexate is not recommended in the setting of breastfeeding due to concern for accumulation in neonatal tissue [Lloyd et al. 1999; Committee on Drugs, American Academy of Pediatrics, 2001]. Given the absence of safety data on leflunomide and breastfeeding, its use is discouraged (see the Leflunomide Prescription Insert at http://products.sanofi.us/arava/arava.html).
In terms of biologic therapy, most information available is for TNFα inhibitor therapy. In one women receiving etanercept while breastfeeding, etanercept was undetectable in the infant (12 weeks of age), despite it being present in breast milk suggesting transplacental transfer but not transfer via breast milk [Murashima et al. 2009]. In three women who utilized infliximab during pregnancy, infliximab was undetectable in breast milk samples and serum of infants [Kane et al. 2009]. Infliximab was detectable in the serum of an infant whose mother was treated throughout her pregnancy with infliximab but it was not detected in the breast milk [Vasiliauskas et al. 2006]. For adalimumab, breast milk levels only reached 1/100 concentration as compared with the mother’s serum [Ben-Horin et al. 2010]. A single woman continued anakinra during breastfeeding with no abnormalities identified with regard to neonatal growth [Berger et al. 2009]. There is no safety information to guide the use of abatacept, tocilizumab, or tofacitinib during lactation (see the Abatacept, Tocilizumab, and Tofacitinib Prescription Inserts).
Implications of DMARDs and biologics on male fertility and family planning in RA patients
Data to support the safety of DMARDs and biologics in the context of male fertility is extremely limited and available mostly in the form of case reports or series besides recommendations provided from the manufacturer. The limited available evidence is summarized and stresses the importance of discussing uncertainties with the patient.
Methotrexate
Methotrexate has been associated with temporary oligospermia which recovers after holding methotrexate [Sussman and Leonard, 1980]. In a survey of Swiss patients, three men reported methotrexate use at the time of conception. In one, an induced abortion occurred, in another a live birth, and the third had an unknown outcome [Ostensen et al. 2007]. In a survey of Swiss rheumatologists, of eight men exposed to methotrexate at conception, two neonates experienced birth defects including one with atrophy of one hand and a small fistula beneath the ear and the other anomalies of the toes [Ostensen et al. 2007]. Among 42 pregnancies occurring in 40 men with methotrexate exposure at the time of conception, no congenital abnormalities occurred. There were three cases of spontaneous abortions and three voluntary abortions. The remaining pregnancies resulted in live births [Beghin et al. 2011]. Per the manufacturer’s recommendation, pregnancy should be delayed by a minimum of 3 months after a man has been on methotrexate (see the Methotrexate Prescription Insert available at http://www.rheumatrex.info/pdf/RheumatrexPackageInsert.pdf). Appropriate discussion with all young and middle-aged males and contraception counselling as necessary is thus important.
Sulfasalazine
In comparing men with IBD who were treated with sulfasalazine with a group of men on no therapy and those who had stopped sulfasalazine over 3 months earlier, only men who were treated with sulfasalazine currently had reduction in sperm count, mobility and increased sperm morphologic abnormalities. Of the 39 men being treated with sulfasalazine, 3 were able to able to have successful pregnancies. When attempting to become pregnant, the median time from stopping sulfasalazine and having a successful pregnancy was 2.5 months [O’Morain et al. 1984].
Leflunomide
A single case reported a male patient who continued leflunomide from 6 months prior to conception through the entire length of his partner’s pregnancy with a full-term baby without any abnormalities [De Santis et al. 2005].
TNFα inhibitors
There is conflicting data regarding the effects of TNFα in in vivo models of spermatogenesis. In a rat model, TNFα improved survival of seminiferous epithelium, an effect that was blocked by infliximab [Suominen et al. 2004]. In contrast, when human spermatozoa were exposed to TNFα followed by infliximab, the quality of spermatozoa was decreased in those exposed to TNFα alone in comparison to those exposed to TNFα and infliximab [Said et al. 2005]. In a study of men with spondyloarthritis, 15 men receiving TNFα inhibitors were compared with 11 men who were not and 102 controls. There was no demonstrable difference in sperm measurements among those treated with TNFα compared with healthy controls. However, higher rates of poor motility and viability were noted in those not receiving TNFα inhibitor therapy [Villiger et al. 2010]. In the TREAT registry of patients with Crohn’s disease, there was no impact of infliximab on men in terms of live births or congenital abnormalities [Lichtenstein et al. 2012]. In 10 pregnancies of men treated with infliximab, 9 resulted in live births [Katz et al. 2004]. In a report of four men with ankylosing spondylitis treated with infliximab, six healthy pregnancies occurred [Paschou et al. 2009]. In general, the human data for exposure in men seem quite reassuring.
Rituximab
Little data is available with regard to rituximab exposure in male partners. Among 22 pregnancies, data was available on 11 of which 2 resulted in spontaneous abortions, 7 in live births and the remaining 2 pregnancies were ongoing at the time of report [Chakravarty et al. 2011].
Other biologic therapy and JAK inhibitors
Data is very limited about other biologics and JAK inhibitors and fertility in treated male partners. Male patients with RA should be counseled regarding this uncertainty.
Conclusion
Rheumatologists are a critical source of support and information for RA patients in the reproductive age group as they begin to consider raising a family. Adequate disease management with DMARDs and biologics is necessary to prevent joint damage and long-term disability, and fortunately the treatment armamentarium only continues to expand as we gain better understanding of the pathophysiology of RA. Care providers must be able to counsel the patient regarding the risks and benefits of these drugs and individualize therapeutic regimens for each patient to optimize the chances for a healthy pregnancy and healthy newborn. This can be achieved by choosing the most suitable disease-modifying therapy in accordance with the patients’ desire for pregnancy, education regarding appropriate contraception, appropriately timing the pregnancy when RA is stable, ensuring adequate follow up during pregnancy to ensure disease stability and initiating appropriate therapy post-partum to prevent severe flares from developing while taking into account the desire for breast feeding. The Organization of Teratology Information Services (OTIS) is a useful resource in helping provide women information and answers on questions related to medications taken during pregnancy (see http://www.otispregnancy.org). Men should also be appropriately educated as several drugs can cause reversible sterility, impair fertility or potentially cause embryotoxicity. Limitations of safety data on newer medications should be discussed as human experience is limited and mostly restricted to cases of accidental exposure during conception or early pregnancy besides animal and preclinical data. The importance of an early and thorough dialogue with the patient cannot be overemphasized.
Footnotes
Acknowledgements
The authors have not sought any outside assistance with regard to study design, data collection, data analysis, or manuscript preparation.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None of the authors have any relevant financial interests to disclose.