
Abstract
Background:
The aim of this study was to verify socioeconomic differences, nutrition, body balance and quality of life (QoL) in postmenopausal women with low bone mineral density (BMD) in two Amazonian communities.
Methods:
A total of 42 female volunteers participated in the study. The volunteers were separated into two groups: Villa (n = 20; 53 ± 5.5 years) and City (n = 22; 56 ± 7.9 years). The following evaluation instruments were used: dual energy X-ray absorptiometry (DXA); a socioeconomic questionnaire; a QoL questionnaire; a dietary habits questionnaire; and a balance test. Parametric and nonparametric tests were used.
Results:
The data showed significant differences in socioeconomic level (Δ%=+15.9%, p = 0.000), lumbar spine L2-L4 (Δ% = +0.10%, p = 0.007), balance (Δ% = +4.3%, p = 0.03) and some important aspects of nutrition, such as the consumption of milk (Δ%=+34%, p = 0.01) and alcohol (+14.8%, p = 0.0001). These significant differences also contributed to the total QoL score (Δ%=+76.2%, p = 0.000) and the majority of the QoL-related functions.
Conclusion:
This study verified that socioeconomic level, nutritional status, physical activity levels and QoL can influence the BMD of postmenopausal women. The study suggests new strategies for official health organizations to use in order to prevent and treat osteoporosis. In addition, this study can provide an orientation to physical activity, nutrition and medical professionals.
Introduction
According to the World Health Organization (WHO) definition, osteoporosis is a chronic disease of the skeletal system that leads to bone fragility and is associated with fracture risks and serious consequences for mobility [National Institute of Health, 2001]. In the elderly, bone fragility, the risk of falls and the frequency of falls are the decisive factors [Sambrook et al. 2007] that considerably affect the quality of life (QoL) [Bener et al. 2007]; moreover, these factors also affect the ability of the elderly to participate in daily activities, which consequently affects their functional autonomy [Navega and Oishi, 2007].
Women are more likely than men to have the disease, owing to the endogenous release of sex hormones and the absorption of the mineral calcium (Ca) [Montilla et al. 2004]. In addition to gender, other risk factors associated with osteoporosis include genetic inheritance, European descent, age, calcium deficiency, physical inactivity, excessive consumption of tobacco and alcohol, and diseases and medications related to low bone mineral density (BMD) [Borba-Pinheiro et al. 2008].
Considering all of the risk factors, special attention should be given to physical inactivity and inadequate nutrition, especially if Caconsumption is low [Montilla et al. 2004]. An appropriate diet and regular physical activity are recommended for their beneficial effects on BMD and for the maintenance of balance [Borba-Pinheiro et al. 2010b; Jessup et al. 2003], which is directly related to falls [Swanenburg et al. 2007].
Another important factor to be considered is socioeconomic differences, because they are variable determinants of human behavior. Socioeconomic differences have an important influence on the risk factors for osteoporosis, including the possibility for an active lifestyle and a Ca-rich diet [Sanchez-Villegas et al. 2003].
To reduce the prevalence of osteoporosis, scientific research is necessary to orient the actions of official health organizations, especially in countries where socioeconomical imbalance is higher such as the northeastern and northern regions of Brazil. For example, one study determined the discharge prevalence of osteoporosis and osteopenia in the lumbar spine and femurs of 473 women, and lower education, older age, precocious menopause and low body mass index (BMI) were identified as risk factors for low BMD [Costa-Paiva et al. 2003].
In northern Brazil, this public health problem may be similar to or worse than that described in the above-mentioned study; however, few studies have examined the variables that have an influence on low BMD in the women in this region. In addition, this lack of studies adds to the difficulty of creating public policies to address the problem.
Therefore, the objective of this study was to verify differences in socioeconomics, nutrition, body balance and QoL in postmenopausal women with low BMD in two Amazonian communities.
Methods
Subjects
In this cross-sectional study, 42 female volunteers with low BMD diagnosed between January and March 2009 participated. Volunteers who were included in the study had a diagnosis of osteopenia and/or osteoporosis in agreement with the WHO criteria [National Institute of Health, 2001] and were postmenopausal. The volunteers were residents of the Tucuruí municipal district in the State of Pará, Brazil, and were participants in the municipal government's health program. Of the 42 volunteers, 20 (53 ± 5.5 years) belonged to an economically high-class neighborhood (Group from Villa [GV]) located 5 miles from the city, which was built in the 1980s for the employees of a large federal government project. The remaining 22 participants (56 ± 7.9 years) lived in the city (Group from City [GC]), an area that suffered from a disordered occupation causing irregular growth when the construction of a dam started.
Study protocols
Measurement of BMD
BMD was measured using dual-energy X-ray absorptiometry (DXA; medium model, DPX class from Lunar®) with a 750-μA current. It was calibrated daily. The exam was conducted by a specialist, with the participant in the supine position on the examination table with her legs inclined (30°) and immobile. The right femur and lumbar spine area were scanned. The variables supplied by the DXA were body composition, the BMD measures (g/cm2), and the T-score, with positive and negative values for lumbar L2-L4 and the right femur (neck and greater trochanter).
Socioeconomic level evaluation
To evaluate the socioeconomic level (SEL) of the investigated groups, the Economic Criterion Classification Brazil (ECCB) was used [ABEP, 2008]. The ECCB classifies individuals into one of five classes: A, B, C, D or E, where class A is the highest and class E is the lowest.
Evaluation of nutritional status
To evaluate nutritional status, a dietary habits questionnaire [Phillipi et al. 1999] was used to determine the monthly consumption of various food groups according to the food pyramid adapted for the Brazilian population. The questionnaire asked about the consumption of 11 food groups: fried foods, fruits, vegetables, proteins, grains, carbohydrates, fat and oil, milk and other sources of Ca, sweets, liquids (e.g. water, juice, soft and drinks) and alcohol. In addition, 13 agree (A) or disagree (DA) questions were used to evaluate the subjects' knowledge about healthy eating and physical activity, taking the food pyramid into consideration.
Quality of life evaluation
The Osteoporosis Assessment Questionnaire (OPAQ) was used to measure the QoL associated with low BMD. In this study, the OPAQ (Brazilian—Portuguese) [Cantarelli et al. 1999] was used to determine general health, mobility, ability to walk and to lean, presence of pain in the back, flexibility, personal care, ability to perform household chores, movement, fear of falls, social activity, support of family and friends, osteoporosis-related pain, sleep, fatigue, work, tension level, humor, body image and independence.
Evaluation of body balance
Body balance was evaluated using the Static Balance with Visual Control test [Rikli and Jones, 1999]. This test assessed participants' ability to stay in a static balance position on one foot for a maximum of 30 seconds, at a distance of 2 meters from a wall while turning their heads. The results of this test were averaged over three measurements.
This study was approved by the ethics committee of the University Castelo Branco, Rio de Janeiro-Brazil/VREPGPE/COMEP/PROCIMH (protocol number 0171/2008). All participants provided informed consent [World Medical Association, 2008].
Statistical analyses
Statistical analyses were performed with a significance level of p ≤ 0.05 for all of the variables studied. PASW® for Windows 17.0 was used to analyze the data. The Student's t-test or the Mann—Whitney U-test was used along with the normality test to verify between-group differences for the following variables: BMD, socioeconomic level, balance, nutritional status and QoL. Finally, a 2 × 2 contingency table was used to evaluate the data for the A or DA questions on the dietary questionnaire (Q1-Q13), and the significant asymptotic two flow of Pearson's chi-squared test was used to calculate probability.
Results
Table 1 presents the characteristics of the studied sample, demonstrating significant differences (p < 0.05) between the two groups for T-score L2-L4 and height.
Sample characteristics.
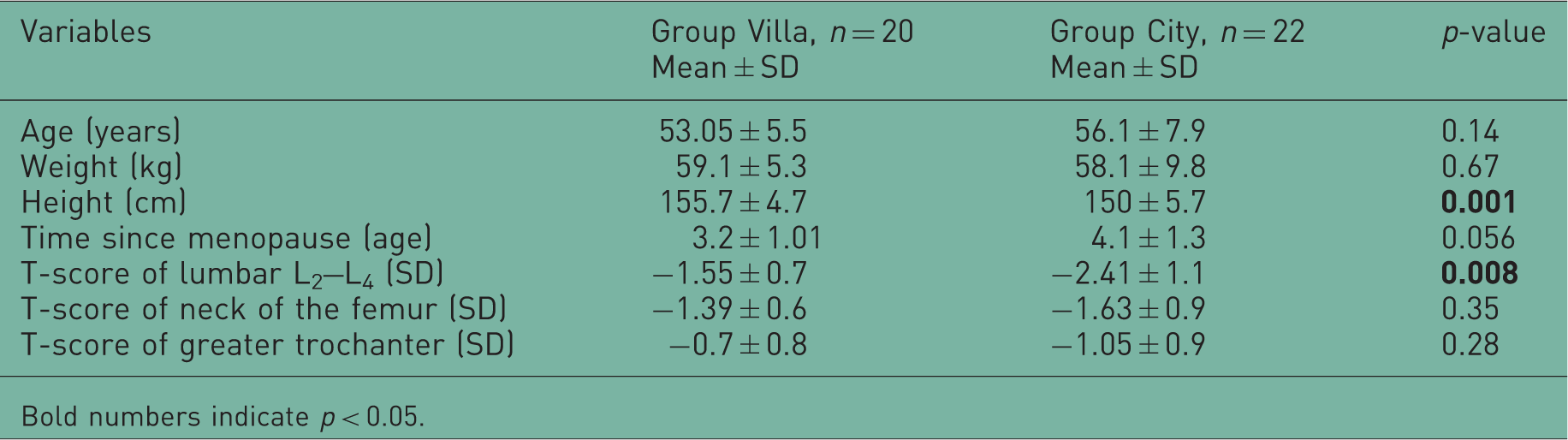
Bold numbers indicate p < 0.05.
In this study, the lumbar L2-L4 BMD measure was significantly lower in the GC. In addition, BMD measures of the neck and greater trochanter of the femur were lower in the GC, although the differences did not reach statistical significance (Figure 1).

Difference in bone mineral density (BMD) between the Villa and City groups. *p < 0.05.
In agreement with the ECCB results [ABEP, 2008], the investigated groups presented highly significant socioeconomic differences (p = 0.000), with the GV classified as wealthier (class A2) (36.8 ± 3.8 points) than the GC (class C1) (20.9 ± 6.06 points).
Figure 2 presents the differences in dietary habits, demonstrating that participants in the GV had better eating habits than those in the GC.

Differences in dietary habits between the Villa and City groups. *p < 0.05.
Another variable considered in the present study was the nutritional differences between the groups. Significant differences in several nutritional aspects were verified, including the monthly consumption of different food groups, such as fruits and vegetables, milk/other sources of Ca and alcohol, verifying that participants in the GC had less healthy diets than those in the GV (Figure 2).
The present study also showed significant differences (p < 0.05) between the groups in their answers to the A/NA questions (Q3, Q5, Q7, Q8, Q10 and Q13), reflecting that the GC had limited knowledge about healthy eating habits and the food pyramid (Table 2).
Dietary habits (knowledge of the food pyramid).

A = %Agree; DA = % Disagree; Vn = Valid numbers; Ns = Not significant; Bold numbers indicate p < 0.05.
The present study also showed significant differences (p = 0.038) in body balance between the two groups and verified that the GV (27.07 ± 3.7 seconds) performed better than the GC (22.7 ± 8.3 seconds).
Figure 3 presents the QoL differences between the GV and the GC and reflects statistical differences (p < 0.05) favorable to the GV. The GV presented the highest means for most of the OPAQ functions and for total count.

Differences in quality of life between the Villa and City groups. * p < 0.05.
Discussion
Studies have previously shown that peak bone mass occurs at about 30 years of age, and bone mass reduction begins at approximately 40 years of age [Arslantas et al. 2008]. As a result, an older person generally has lower BMD. This tendency was confirmed in the present study; specifically, the BMD (g/cm2) of the GC (56.2 ± 7.9 years) participants showed significant differences for the lumbar spine L2-L4 measurement compared with the younger GV participants (53 ± 5.5 years) (Figure 1).
In agreement with our results, Costa-Paiva and colleagues found a high prevalence of osteoporosis and osteopenia of the lumbar spine and femur and indicated that the important risk factors for low BMD in this population of women from a particular region were menopause and age [Costa-Paiva et al. 2003]. Therefore, it can be verified that the largest propensity for osteoporosis occurs in the age groups associated with menopause and postmenopause [Kanis et al. 2005].
The present study demonstrated significant SEL differences between the GV and the GC; the former was considered class A2 and the latter was class C1. Using the reference values for medium family income, in Brazilian currency, class A2 individuals earn an income of R$6564 monthly (equivalent to US$3895), while class C1 individuals earn an income of R$1195 monthly (equivalent to US$708.24) [ABEP, 2008]. This factor can have an influence on nutritional status and QoL as well as physical activity and medical treatment.
The results of this study are in agreement with previous studies in the literature. One previous study shows a relationship between SEL and cheese consumption, with the wealthiest groups consuming more cheese and consequently having a higher BMD [Sanchez-Villegas et al. 2003]. The present study verifies these results; specifically, the higher-SEL GV class consumed significantly more milk than the GC as shown in Figure 2, confirming that this variable has an influence on the nutritional conditions of the affected population.
The literature also shows that women over the age of 50 with higher SELs have better BMDs. The relationship between lower income and poorer BMD in this age group may be the result of the high costs of examinations and doctor visits as well as the difficulty in accessing information, receiving the necessary medicine and understanding appropriate nutrition and physical activity [Bass et al. 2006]. This theory is confirmed in the present study (Figures 1 and 2).
The present study also shows between-group differences in several aspects of diet that favor the GV. Therefore, it is probable that differences in the consumption of fruits, vegetables and fried foods had an influence on the lower BMD of the GC (Figure 2). Moreover, the Brazilian Scale of Alimentary Insecurity shows that when compared with the elderly in low-income families, the elderly in wealthier families consume more vegetables (92% vs. 61.8%), protein (74.2% vs. 43.1%) and fruit (77.4% vs. 49%) [León et al. 2005].
Another study considered nutrition over a 5-year period and found that the high consumption of greasy foods, acids and saturated fats facilitated the loss of BMD in the neck of the femur (p = 0.01). It also showed that the appropriate consumption of fruits and vegetables containing magnesium, potassium and vitamin C, as well as Ca, can protect against BMD loss in the neck of the femur in premenopausal women [Macdonald et al. 2004].
Among the different food groups investigated in these studies, protein deserves special attention, although it did not present significant differences between the groups. The consumption of a high-protein and low-Ca diet may cause damage to the balance of osteoblast activity [Montilla et al. 2004]. Therefore, if we compare the average consumption of protein and Ca in the GC (45.3 ± 16.5 and 46.3 ± 34.7, respectively) and the GV (42.7 ± 26.8 and 75.4 ± 35.01, respectively) groups, it appears that the less-wealthy group had a higher consumption of protein in proportion to Ca compared with the wealthier group, which may have contributed to the lower BMD of the GC (Figure 2). However, controversies exist in the literature with the relationship of the high protein consumption and the low BMD.
There is evidence in the literature that the risk of osteoporosis increases with low Ca consumption. The decrease in BMD may be due to the poor Ca consumption; the WHO recommends the consumption of between 1000 and 1500 mg/day [Arana et al. 2007]. This is in agreement with our results, which showed a significant difference in the groups' monthly consumption of Ca-rich foods, with the GC consuming fewer (p = 0.01). In addition, the GC had a lower BMD in the lumbar spine L2-L4 and a tendency for a lower BMD in the femur. Therefore, these results suggest a relationship between inadequate Ca consumption and lower BMD in the GC. Knowledge about healthy habits and the food pyramid has a direct relationship with SEL [Bass et al. 2006], and the GC had less knowledge than the GV participants.
Reinforcing our results, several other studies have shown that milk supplements provide significant benefit to the BMD of the whole body (p < 0.001). In one study that examined BMD loss in the lumbar spine, the control group (non-milk drinkers) had a BMD loss of 0.90%, while BMD loss among milk drinkers was only 0.13% (p < 0.05).
The present investigation also showed significant differences (p < 0.05) in alcohol consumption, with higher consumption by the GV participants (Figure 2). However, the GV had a higher BMD than the GC; this finding contradicts the literature, which shows that excessive consumption of alcohol is linked with a decrease in BMD [Bass et al. 2006]. However, despite significant differences between the groups, it is possible that the average monthly consumption of alcohol in the GV was moderate, rather than excessive (5.7 ± 8.6 drinks/month), and the average monthly consumption of alcohol in the GC was almost nonexistent (0.14 ± 0.4 drinks/month). These results suggest a good relationship between moderate alcohol consumption and the balance of osteoblast activity [Mukamal et al. 2007]. The moderate consumption of alcohol may actually promote higher BMD in the GV, in agreement with the results of Wosje and Kalkwarf [Wosje and Kalkwarf, 2007]; more specifically, the moderate consumption of 5 to 29 drinks per month (beer, wine or distilled liquor) may be beneficial to the bone health of postmenopausal women.
The GC participants exhibited worse balance (22.7 ± 8.3 seconds) than the GV participants (27.07 ± 3.7 seconds; p = 0.038), which may be related to the fact that the GC participants were older (56.2 ± 7.9 years). Balance is one of the systems most affected by aging, and it leads to the appearance of instability and the occurrence of falls among the elderly [Baloh et al. 2003].
Balance deficits and walking problems are common in the elderly and are more frequent in women and in those with vision difficulties, according to the Performance-Oriented Mobility Assessment scale, because the majority of people in these groups do not exercise; in addition, there is a significant relationship between visual ability and low performance on this evaluation [Lojudice et al. 2008].
Physical activity is a potential factor related to functional autonomy [Farinatti et al. 2008]; however, a lack physical activity is still evident in Brazil. This phenomenon is most obvious in one study that compared the active autonomy of the elderly in Brazil and Belgium, concluding that the Brazilians are less autonomous due to their reduced physical capacity; moreover, this reduced physical capacity hindered the activities of daily life for the Brazilian elderly [Farinatti et al. 2008].
The literature demonstrates that elderly people who practice physical activity can develop balance, improve walking, significantly minimize fall risks, and consequently minimize the risk of fractures [Borba-Pinheiro et al. 2010b]. Multi-exercise programs, which include weight training, walking, using stairways and performing balance exercises three times a week for 60 minutes for 32 weeks, have been shown to be effective [Arana et al. 2007]. These programs have shown a positive effect on femoral neck BMD and body balance (p < 0.05) [Swanenburg et al. 2007]. Activities that develop muscular force in the lower limbs, including resistance training with different intensities, have also shown benefits in reducing the risk of falls [Borba-Pinheiro et al. 2010a, 2010b].
The WHO recommends appropriate levels of the different types and amounts of activity needed for better health over a lifetime; these recommendations include 30 minutes of moderately intense physical activity on most days, which reduces the risk of diseases and increases muscular resistance and balance activities, which can reduce the incidence of falls and increase functional capacity [World Health Organization, 2004]. Although the physical activity variable was not considered in this study, it is possible that the GC had a lower level of physical activity than the GV because evidence has shown an association between income and education and the frequency of exercise during leisure time [Inouye and Pedrazzani, 2007].
Therefore, we recommend an intervention that helps the low-income population develop and maintain exercise habits. In addition, it is necessary to understand the factors that contribute to the initiation and maintenance of exercise and to develop effective interventions for improvement [Borba-Pinheiro et al. 2008].
The OPAQ revealed significant statistical differences (p< 0.05) in QoL between the GV and the GC, both overall and for specific areas. There were significant differences in health, mobility, walking and leaning, pain in the back, flexibility, household tasks, movement, fear of falls, pain related to osteoporosis, fatigue, tension level, body image and independence. Moreover, this scale revealed that the GC participants possess a low QoL (Figure 3). These results are in agreement with the literature, which shows a relationship between the QoL and bone health in women [Aranha et al. 2006].
Patients with vertebral fractures usually experience a significant deterioration in QoL compared with those with other fractures [Adachi et al. 2002]. However, postmenopausal women with osteoporosis who do not have fractures but are physically active can have a QoL similar to post-menopausal women without osteoporosis [Navega and Oishi, 2007].
It is worth mentioning that the inevitable increase of the elderly population requires increased government expenditure because with age, people become weaker and need more frequent medical attendance and leisure and retirement alternatives. This elderly population is a social phenomenon that necessitates positive response from the state, society and its institutions [Santin and Borowski, 2008]. Owing to the accelerated aging of the population, the public health system is at risk of becoming not only insufficient but also chaotic [Lima et al. 2005]. To guarantee longevity with a high QoL in the international and national context, it is imperative to consider the QoL of the aging by taking measures to protect future health and wellbeing.
In the present study, the GC had a lower SEL, and the GC participants exhibited significantly worse results (p< 0.05) than the GV in all of the variables studied. Although these results were expected based on the literature, which demonstrates that low SEL interferes with QoL, the nutritional status and lack of physical activity in this group could also have led to the lower BMD [Crans et al. 2004]. In any case, this study is of great value for the northern area of Brazil, as it is one of few studies that orient public policies towards these problems.
Aging as a social phenomenon requires public policies that meet the needs shown in this study [Santin and Borowski, 2008]. There must also be discussions in the international context about maintaining a focus on longevity with a high QoL, including measures that protect future health and wellbeing [Lima et al. 2005]. Moreover, health professionals concerned with aging must consider the prevention, diagnosis and treatment of osteoporosis in low-income populations. Several studies have shown that professionals who ignore official health organization guidelines for osteoporosis treatment are putting the health of this socioeconomic group in danger [Giangregorio et al. 2007].
In agreement with the literature, the present study verified that socioeconomic differences contribute to a lack of nutrition, a low QoL and impaired balance, which can decrease BMD and increase the risk of falls in the studied population. However, this study was limited by the small sample size in each group. Therefore, more studies should be performed with larger sample for to improve our understanding of those variables and close this knowledge gap.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
There are no potential conflicts of interest.